
Abstract
Background:
Although targeted muscle reinnervation has been shown to be effective in enhancing prosthetic control for upper limb amputees, restored hand sensations have been variable. An understanding of possible sensory feedback channels is crucial in working toward more effective closed-loop prosthetic control.
Objectives:
To compare sensory outcomes of different targeted sensory reinnervation approaches.
Study design:
Case series, cross-sectional, and retrospective.
Methods:
Three transhumeral amputees that had undergone different sensory reinnervation approaches were recruited. Skin pressure sensitivity thresholds and anatomic sensory mapping were performed using Semmes-Weinstein monofilaments. The clinical charts of the subjects were reviewed to compare the sensory maps performed during the earlier post-reinnervation period.
Results:
While the first two subjects achieved return of hand sensations on the stump skin in early follow-up, the maps showed attenuation over time. The last subject developed discrete sensations of all digits in the recipient cutaneous nerve territories away from the reinnervated muscles.
Conclusions:
These findings confirm that it is feasible to restore hand sensation after transhumeral targeted reinnervation, but there is a significant intersubject variability. The intrafascicular approach may be particularly effective in restoring digit sensation and deserves further exploration, as do factors affecting stability of the hand maps over time.
Clinical relevance
In addition to enabling intuitive motor control of myoelectric prosthesis, targeted reinnervation can also result in sensory restoration of the hand. Documentation of sensory mapping present after reinnervation may assist with exploring future techniques for sensory enhancement, with the goal of working toward closed-loop prosthetic control.
Background
Targeted reinnervation has demonstrated success in improving motor control signals for both shoulder disarticulation and transhumeral amputation.1–3 Targeted reinnervation has also shown promising sensory outcomes in that redirected sensory afferents from the median, radial, and ulnar nerves reinnervate the skin in the residual limb, re-creating an expression of the missing hand map. 4 When these patients are touched on the reinnervated skin, they feel as if they are being touched on the missing limb.4–6 This provides a potential portal to restore sensory feedback from the prosthetic device that could be anatomically matched to the missing limb.
Restored cutaneous sensory percepts have been described in subjects with targeted reinnervation who developed hand sensations on chest skin after reinnervation, including a wide range of sensory modalities.4,7 These findings were demonstrated in subjects with local reinnervation of skin overlying the muscle after thinning of subcutaneous tissue as well as in a subject with end-to-side coaptation of the supraclavicular nerve to the ulnar nerve.1,4
In contrast, the sensory outcomes for the transhumeral targeted reinnervation procedure have not been as well reported. Dumanian et al. 3 reported on six subjects with transhumeral targeted muscle reinnervation procedures. The nerve transfers yielded four distinct electromyographic (EMG) signals from adjacent muscles controlled by four different nerves. However, they did not report any sensory outcomes. Sensinger et al. 8 described one transhumeral reinnervation subject in whom “the distal end skin was purposefully denervated.” This subject was reported to have transfer sensation of the palm and palmar aspect of digits 1–3 when touched on the medial aspect of the upper arm and was able to discriminate between gradations of force applied to these areas of skin reinnervation. Marasco et al. 9 reported on embodiment responses in two subjects with transhumeral amputation who had undergone targeted reinnervation and who had clear sensory percepts to touch projected to the missing limb. Our group recently reported a subject with transhumeral amputation who underwent a new fascicular end-to-end technique by coapting individual sensory fascicles of the median and ulnar nerves to target cutaneous areas. 10 That subject developed distinct median and ulnar hand maps in two separate cutaneous areas, separate from the motor sites in the residual limb.
Based on these reports, in a previous review article, 11 the techniques employed for sensory reinnervation were categorized into three approaches: (1) targeted reinnervation with skin denervation over the muscle site; (2) targeted reinnervation with end-to-side cutaneous nerve transfer; and (3) targeted reinnervation with fascicular end-to-end nerve transfer. Given the interest in pursuing methods of incorporating physiologically natural matched sensory feedback from prosthetic limbs, a more detailed comparison of targeted sensory reinnervation approaches is warranted. In addition, no reports have examined changes in hand maps over time. The purpose of this report is to compare the sensory outcomes of three different targeted reinnervation techniques used in our center on transhumeral amputees, and second to infer from retrospective review whether there is a change in hand mapping over time. The intent is to stimulate discussion of sensory reinnervation outcomes to inform future planning of surgical techniques to maximize sensory restoration with reinnervation.
Methods
In order to compare the outcomes of three different surgical approaches for sensory reinnervation that had been performed to date, we undertook detailed sensory testing on three subjects who had undergone different sensory reinnervation techniques. For two of the subjects who had undergone earlier procedures, we also did a retrospective review of the original noted sensory maps in the clinical chart to compare the point in time testing. The third subject had the most recent sensory reinnervation technique and therefore also had detailed mapping at an earlier time point for comparison. We also performed motor testing to confirm that the motor reinnervation procedure had been successful. Informed consent for this study was obtained with approval from the Health Research Ethics Board at our institution.
Sensory reinnervation techniques
A description of the various sensory reinnervation techniques has been previously reported: 11
Subject TH1 had standard targeted muscle reinnervation, with thinning of subcutaneous tissue overlying the muscle sites causing local skin denervation;
Subject TH2 had targeted muscle reinnervation and an end-to-side coaptation of medial brachial cutaneous (MBC) nerve to the median nerve;
Subject TH3 underwent an end-to-end fascicular sensory reinnervation technique. A sensory fascicle of the median nerve was coapted to the intercostobrachial cutaneous nerve, and a sensory fascicle of the ulnar nerve was coapted to the axillary sensory branch. Details of the intra-operative technique have been previously reported. 10
Motor testing
We used an eight-channel Bagnoli-8 EMG acquisition system (Delsys, Inc., MA, USA) to record surface EMG from the muscles of the residual limb. The subjects were asked to think of performing a specific limb movement relating to the elbow, wrist, or hand. During the visualization, electrodes were placed over the muscle belly where contraction could be felt. A graphical user interface displayed EMG signal strength where gain and thresholds could be adjusted. The process of identifying the optimal number of separable muscle signals was an iterative process consisting of exploring electrode placement and adjusting signal gain and thresholds, as per the standard approach to myoelectric signal site testing. The number of discretely separable motor signals was confirmed by matching the signal to operation of a robotic arm with 5 degrees of freedom. 12
Sensory testing
Three subjects who had undergone the targeted reinnervation procedure were recruited for detailed sensory testing including cutaneous sensory thresholds (just discernable pressure), light touch, and referred hand mapping with monofilament stimulation. A researcher with experience in sensory mapping performed the detailed sensory mapping. This testing was performed at a single time point for subjects TH1 and TH2, and at an early and late follow-up time points for TH3.
Sensory threshold for just discernable pressure was established using a Semmes-Weinstein 20 monofilament testing set. 13 The standard protocol involves choosing different weights of wire and applying pressure to the skin until the wire just bends. The sensory threshold was examined throughout the residual limb, referenced with respect to the known peripheral nerve distributions of interest: lateral outer arm (axillary nerve region), medial inner arm (intercostal brachial cutaneous (IBC)), anterior (MBC and antebrachial cutaneous), and posterior (posterior brachial cutaneous) aspect of the residual limb. Analogous locations on the intact upper arm were tested for comparison of sensory thresholds.
Referred anatomical sensory mapping was then performed on the residual limb. Light touch stimulation with a cotton ball (stroking movement over approximately 1 cm of skin) was initially used to test for any presence of hand or digit sensation. The subject was asked to report where they felt the sensation when the residual limb was touched. Light touch was exploratory in nature, as a general screen for hand percepts. Then, a 1 cm grid was marked on the residual limb being tested. A Semmes-Weinstein monofilament with sufficient weight to stimulate all areas of the skin (above the measured just discernable pressure threshold) was used to stimulate each point on the grid with the subject’s vision to the testing limb obscured. The subject reported whether the sensation was felt on the residual limb or in the phantom limb, used the intact hand to point to the location on an anatomical arm drawing, and verbally described where the stimulation was felt. They were asked to use descriptive terms such as “sharp, dull, tingling” or any descriptive word of their choice. To test reliability and consistency, each point was checked three times in random order and the subject’s sight was obscured to remove any visual cues. Results of the mapping were schematically represented such that any points on the grid with sensation referred to the missing limb consistently for all three of the randomly applied stimulations were noted, linked to the location and description of the corresponding sensation on the hand. The remainder of the limb (with no grid notation on the rendering) had native skin sensation or inconsistent reporting.
The medical records of subjects TH1 and TH2 were then retrospectively reviewed to extract the original hand maps that had been recorded during the recovery period by the clinical occupational therapist. The method used was to stroke a cotton ball over 1 cm sections of the entire residual limb, using scar and other skin markings as landmarks, and asking the subject to report where the sensation was felt. Digital palpation was also used to apply pressure over muscle bellies and soft tissue, sufficient to indent the skin but not cause discomfort. Monofilament threshold testing had not been performed on the early testing for subject TH1 or TH2. Subject TH3 had sensory threshold testing of the residual limb as part of pre-surgical planning prior to the reinnervation surgery, and at 4 months post-reinnervation had undergone the same detailed testing protocol so that data were used for comparison. Refer to Table 1 for timing of assessments for each subject.
Timing of sensory assessments.
OT = occupational therapist.
Results
Subject characteristics are listed in Table 2. All subjects were males with unilateral transhumeral amputation.
Targeted reinnervation subject characteristics.
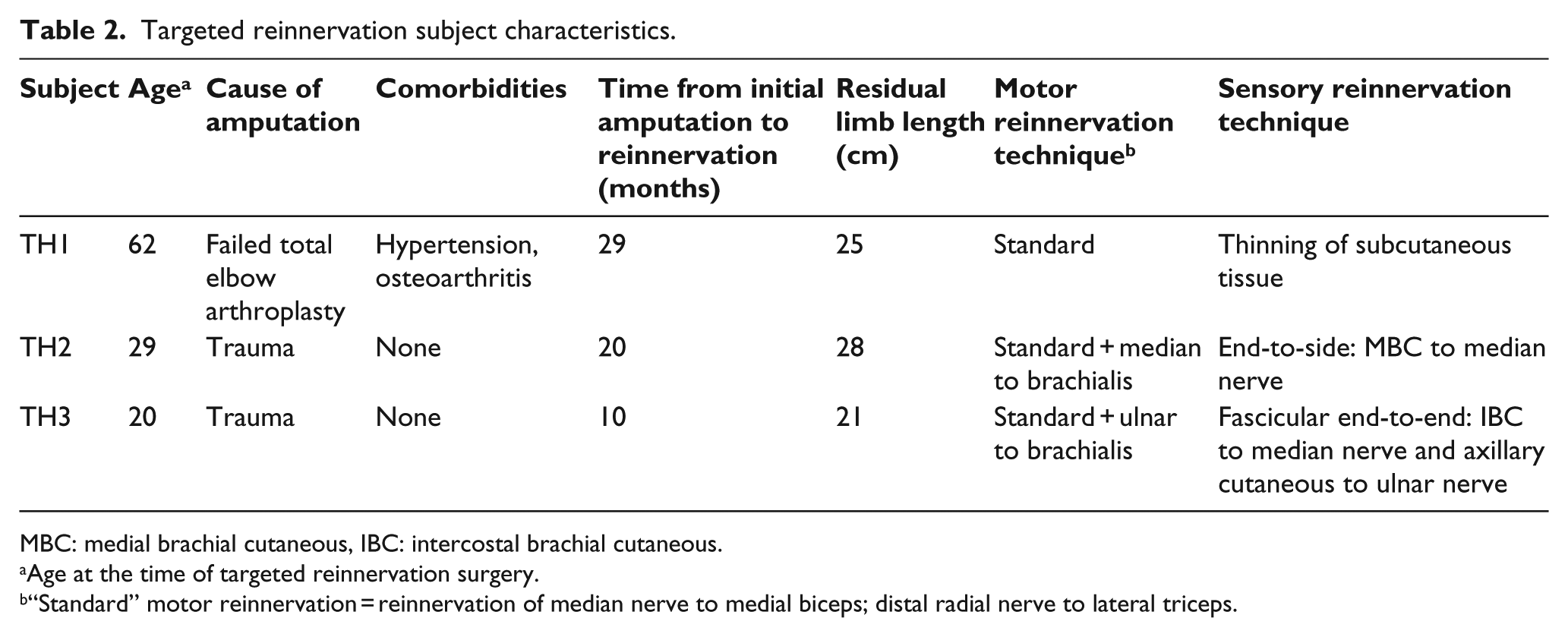
MBC: medial brachial cutaneous, IBC: intercostal brachial cutaneous.
Age at the time of targeted reinnervation surgery.
“Standard” motor reinnervation = reinnervation of median nerve to medial biceps; distal radial nerve to lateral triceps.
Motor outcomes
All subjects successfully reinnervated the target muscles, with four discretely separable motor signals for hand close (medial biceps), hand open (lateral triceps), elbow flexion (lateral biceps), and elbow extension (medial triceps). The signals could be used to simultaneously operate 2 degrees of freedom of a robotic arm. In addition, subject TH3 had a discretely separable wrist flexion signal in the brachialis muscle. TH2 had palpable muscle contraction in brachialis with imagined wrist flexion, but it could not be discretely separated from the biceps hand close signal.
Clinically, all three subjects were able to operate a myoelectric prosthesis with simultaneous motion of elbow and hand. TH1 wore a myoelectric prosthesis that included a Dynamic Arm elbow and Greifer terminal device (Ottobock, Inc., Duderstadt, Germany). TH2 operated a myoelectric prosthesis with a Boston Elbow (Liberating Technologies, Inc., Holliston, Massachusetts) and an Electric Terminal Device (ETD) hook (Motion Control, Inc., Salt Lake City, Utah). TH3 was a full-time daily myoelectric user with a Boston Elbow and BeBionic hand (RSL Steeper, Inc., Leeds, UK).
Sensory outcomes
Subject TH1
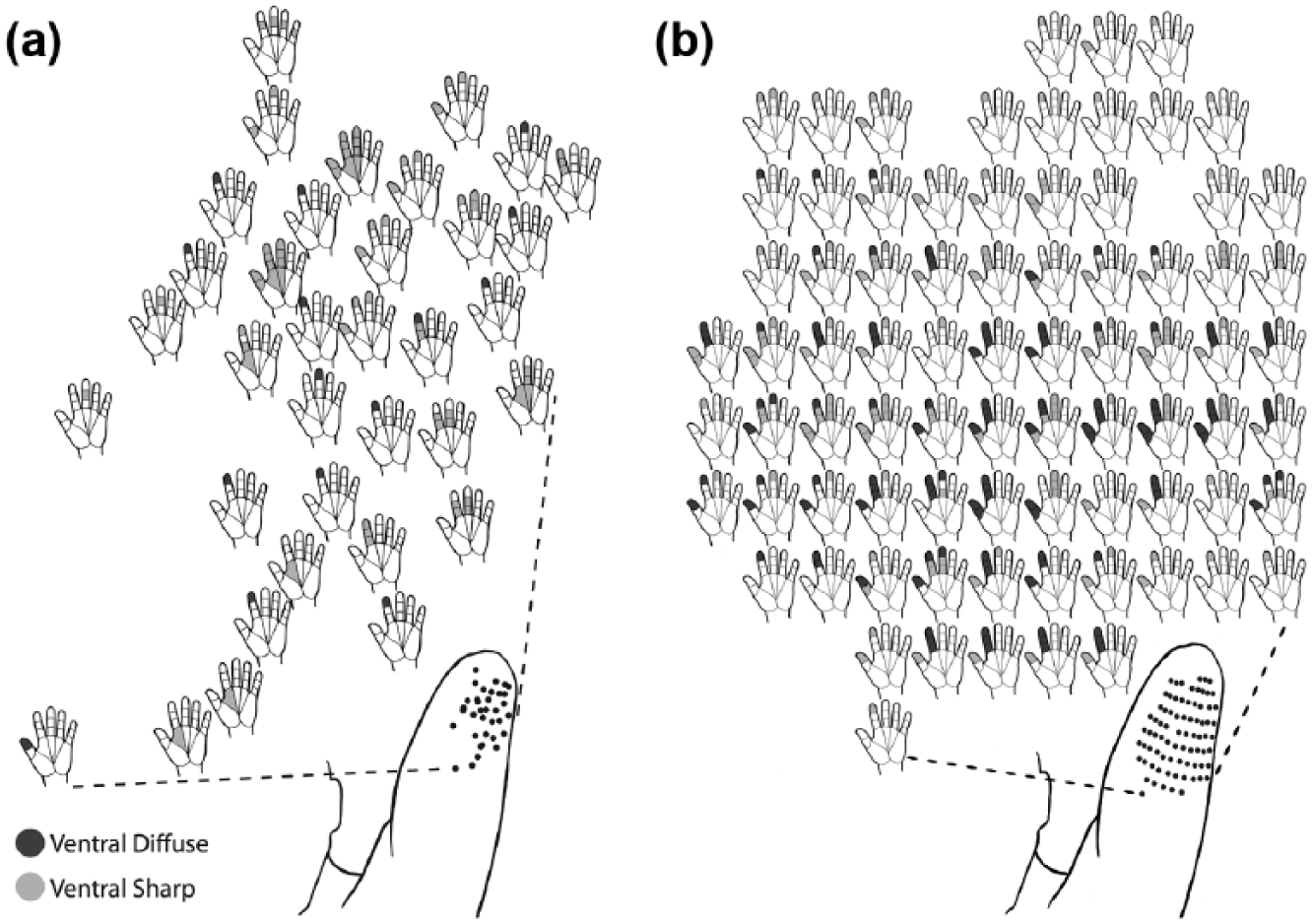
The initial sensory maps of TH1 at 8 months post-reinnervation are shown in Figure 1(a). The areas with referred sensation to the hand are shown; all other sites on the grid had native arm sensation. Light touch on the anterior distal residual limb elicited referred sensation to the volar tips of digits 1, 2, and 3. The sensation was described as a strong pins and needles sensation. With deeper pressure, the sensation would extend to multiple digits and the palm in some areas. Posteriorly on the residual limb, there were three areas along the incisional scar where the subject experienced referred sensations to the dorsal aspect of digits 2, 4, and 5. These findings were consistent with the location of the motor nerve transfers.
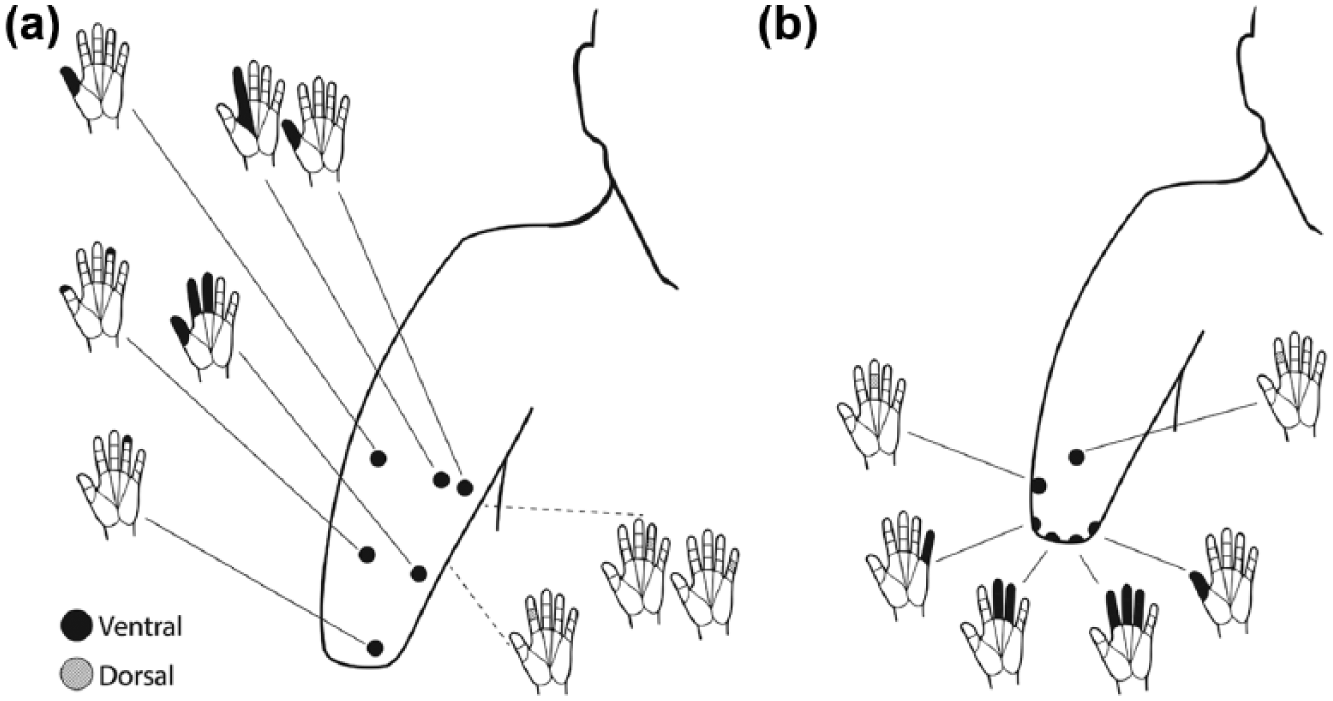
Sensory hand maps of TH1: (a) 8 months post-reinnervation surgery and (b) 5 years post-reinnervation. Solid lines connect hand map with the corresponding anatomic location on the limb, with dashed lines indicating the anatomic location is posterior (not visible) on the schematic. At 5 years, the mapping was greatly reduced, with several points clustered at the distal residual limb.
At 5.5 years post-reinnervation, sensory threshold was generally poor at 4 g pressure threshold throughout the residual limb, compared to a range of 0.02–0.6 g sensory threshold on the intact arm. The referred hand map was also greatly reduced on the residual limb (Figure 1(b)). Tactile stimulation with a 10 g monofilament to the very distal end of the residual limb at different points evoked a sense of touch to the volar aspect of the thumb, a brushing sensation across digits 2–4, and tingling in digits 3–5 (shown in Figure 1(b)). There were two locations on the anterior and lateral arm that referred to the dorsal aspects of digits 2 and 3.
Subject TH2
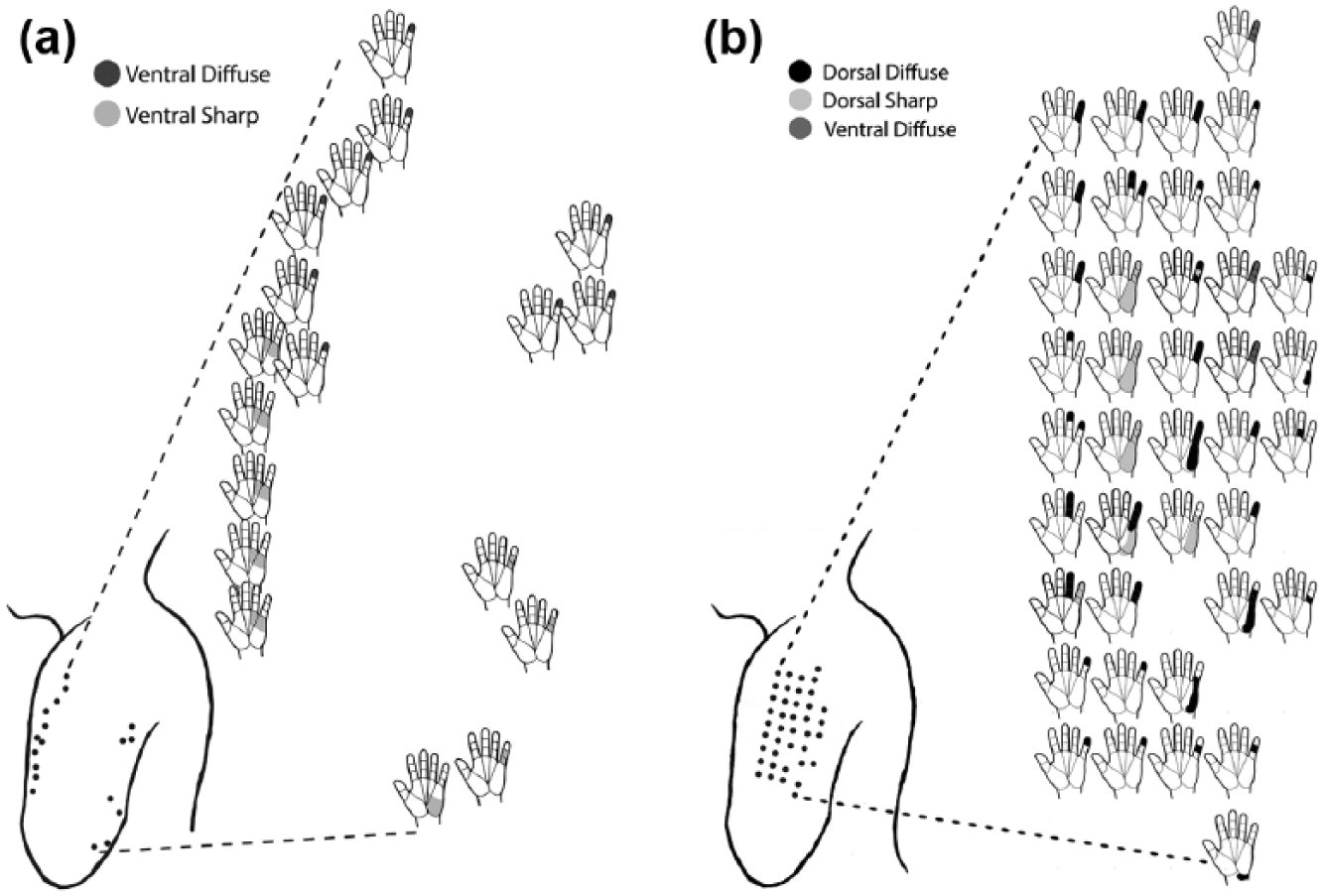
At 6 months post-reinnervation, light touch to the anteromedial distal residual limb evoked a tingling sensation to the volar aspect of digits 1–3, and localized tingling to the distal finger and base of the fingers (Figure 2(a)). The territory was consistent with the median nerve transfer. Light touch to the posterior distal limb referred sensation primarily to the hypothenar eminence and digits 4 and 5. The percept was best elicited with a stroking movement across 1 cm of the skin.
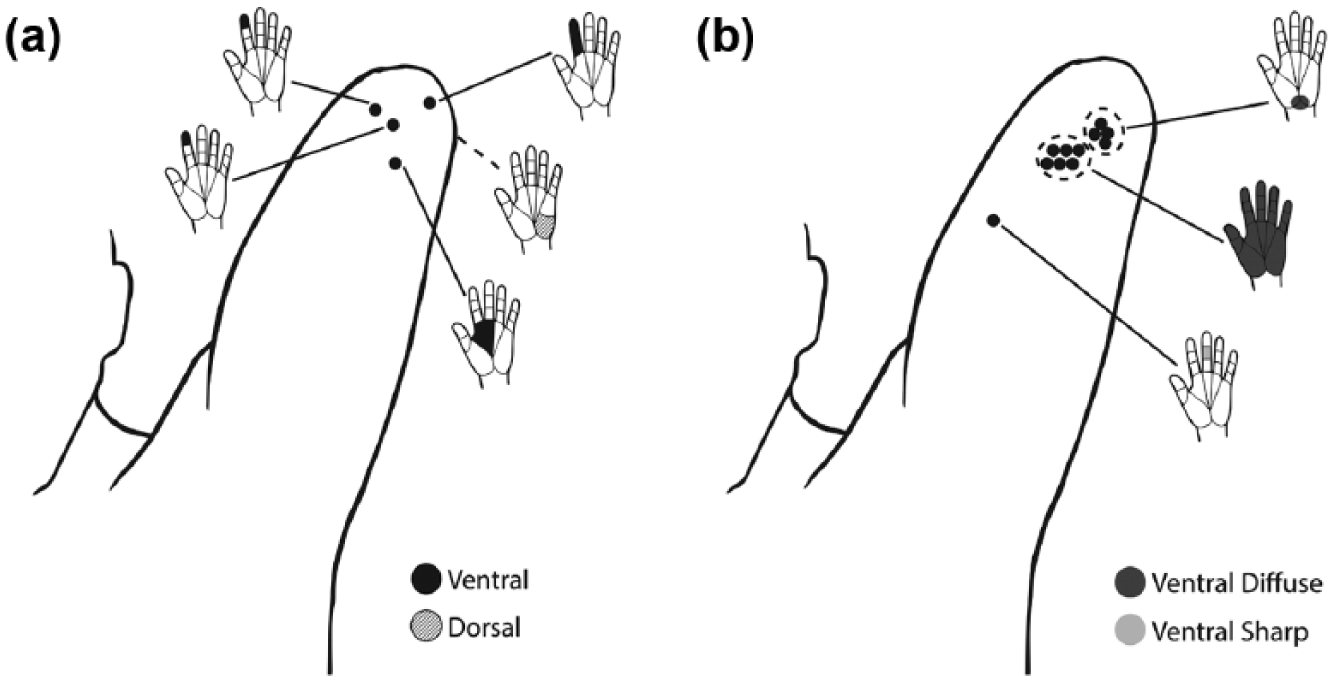
Sensory hand maps of TH2: (a) 6 months post-reinnervation surgery and (b) 6 years post-reinnervation surgery. There were several areas tested on the anteromedial limb that referred sensation to the palm and heel of the hand, illustrated as a circled cluster of dots.
At 6 years post-reinnervation, subject TH2 had poor pressure sensibility threshold in the residual limb, in comparison to normal thresholds of 0.07–0.4 g in the intact limb. Just discernable pressure using Semmes-Weinstein monofilaments was 2 g in the lateral deltoid region, 4 g in the medial arm area (MBC), and 1.4 g in the other areas of the residual limb. Precise localization of stimulation was poor, and the subject often mislocalized the sensation several inches proximal to the actual applied area on the arm. He also reported the sensation of “telescoping” of his phantom limb, with the hand position immediately at the end of the distal limb. Hand mapping with a 10 g monofilament identified a number of locations where the stimulation referred sensation to the palm of the hand, and/or radiated throughout the hand (Figure 2(b)), mostly described as “pressure” or sharp tingling sensation.
Subject TH3
At 4 months post-reinnervation, pressure threshold was impaired at 6 g in the cutaneous denervated territories, compared to 0.008 g prior to surgery. Mapping of hand sensation was consistent with the nerve transfers. Specifically, all median nerve digit sensation corresponded with the intercostobrachial cutaneous nerve territory (Figure 3(a)), and all ulnar nerve sensation corresponded with the axillary cutaneous nerve branch territory (Figure 4(a)).
Sensory hand maps of the medial residual limb of TH3: (a) 4 months post-reinnervation and (b) 15 months post-reinnervation. Each hand map shown is spatially located relative to the corresponding anatomic spot on the limb. The hand map reflected reinnervation of solely median nerve digit sensation in the intercostobrachial cutaneous nerve territory, and became more widespread and detailed at 15 months.
Sensory hand maps of the lateral residual limb of TH3: (a) 4 months post-reinnervation and (b) 15 months post-reinnervation. The hand map reflected reinnervation of solely ulnar nerve sensation in the axillary cutaneous nerve distribution.
Sensory threshold at 15 months post-reinnervation improved to 0.4 g. The analogous intact arm sensory threshold remained at 0.008 g. Mapping of the digit sensations, performed with a 2 g monofilament, was widely spread with multiple locations for each digit within the cutaneous territories (Figures 3(b) and 4(b)). The subject reported that in areas where single digit was felt, the intensity increased when higher force was applied. In areas where 2 or 3 digits were felt simultaneously, the sensation was reported as “brushing” in quality. The remainder of the arm (with no referred hand mapping) was reported as feeling normal skin sensation. There were no painful sensations reported to any of the sensory testing.
Discussion
The first two sensory reinnervation techniques initially restored areas of cutaneous sensory percepts corresponding to the hand map. The percepts found within the first 6–8 months were located in the skin overlying the muscle, and particularly the territory of the median nerve transfer, as expected. In contrast, the third subject with the fascicular end-to-end technique developed widespread topographic representation of the digits with discrete separation of the median and ulnar hand maps in the defined target cutaneous areas. The types of sensation restored were less discrete for the initial two subjects compared to the subject with the specific fascicular technique. We postulate that the direct end-to-end fascicular technique, which selected a specific nerve fascicle with high sensory content for direct coaptation to the cutaneous nerve branch, 10 likely resulted in preserved somatotopy of the digits. The sensory nerve fibers within a single fascicle are more likely to represent contiguous digits 14 and would therefore have an advantage compared to the resulting competitive reinnervation with skin denervation in TH1, where the reinnervating median nerve would have to compete with native cutaneous nerves to reinnervated the denervated skin. Similarly, the end-to-side technique used in TH2 10 attaches the target cutaneous nerve to the side of the entire median trunk, along its mid-course, and does not direct a specific fascicle to the target. We believe this resulted in overlap in innervation from competing cutaneous afferents, which may have contributed to the sensation of paresthesia or less discrete touch.
Comparing our results to those presented in the literature, detailed sensory mapping results have only been reported for reinnervation subjects at shoulder disarticulation and short transhumeral amputation levels. The end-to-side technique in subjects with sensory reinnervation over the chest has demonstrated discrete transferred sensation of the hand map with excellent sensibility, 4 comparable to our end-to-end fascicular sensory reinnervation subject. However, the somatotopic organization of the hand map in that end-to-side sensory reinnervation subject was intermixed with both median and ulnar afferents in the same regions. 1 In contrast, in our subject TH3, there was a clear exclusive separation of median and ulnar hand maps in two separate cutaneous areas. In the literature, no other detailed hand maps for subjects with the transhumeral reinnervation procedure have been reported.
It should be noted that detailed sensory threshold testing was not performed prior to the reinnervation surgeries in the first two subjects, as the focus was on the muscle reinnervation procedure, and this limits comparability of the results. Those subjects may have had impaired sensation on the residual limb prior to reinnervation, accounting for the poorer post-operative sensory recovery. One participant was also older, which might influence the results as tactile sensitivity is known to decrease with age, 15 although his sensitivity at the later time period was comparable to the younger TH2 subject. For our most recent case (TH3), detailed sensory testing assured us that he had normal sensitivity thresholds prior to the planned sensory reinnervation, which likely influenced the success of the restored sensory percepts. Nonetheless, the discrete hand maps of the median and ulnar nerves in separate cutaneous areas, not overlying the muscle sites, confirmed that surgical control over the cutaneous sensory restoration was possible.
An interesting observation was found in the fact that the first two subjects showed attenuation in the hand maps over time. The maps were not stable after 5 years of follow-up. A technical limitation could be that the early sensory mapping was done by a clinician only examining light touch and pressure at the initial examination versus the more rigorous testing with monofilaments at the follow-up time points. Also, the anatomy of the residual limb may change over time, so the 1 cm coordinates might not be identical, although the landmarks (such as scar location) were likely the same. The differences over time could therefore be an artifact due to variability of the mapping techniques. In addition, the newly regenerated sensory fibers in the early stages of recovery may not have fully reinnervated the skin in the early stages, and the map may have evolved in the interim between the initial and later testing periods. The different time points of the mapping, therefore, limit comparison between subjects. Another possible factor affecting within subject changes is that reduced skin sensitivity may occur with full-time prosthetic use, as patients using a prosthesis have been shown to have significantly poorer touch–pressure sensitivity in the residual limb compared to non-users. 16 It is also known that the cortical representation of the hand shrinks in size after amputation.17,18 The lack of functional use of the hand sensory percepts may contribute to changes in mapping and sensitivity over time. Prospective study of sensory recovery and of factors influencing the strength and maintenance of sensory percepts will need to be examined in future study. For example, sensory training and the use of relevant sensory feedback within a functional prosthesis may have an impact on sensory thresholds by strengthening cortical representation of the missing limb.
Conclusion
Based on the findings in our three cases, we have suggestions for future consideration. First, detailed sensory testing should routinely be performed preoperatively prior to reinnervation surgery and throughout recovery to gain an understanding of the evolution of the sensory maps over time. Second, to optimize sensory outcomes, handling of the sensory nerves and the sensory approach should be as carefully and deliberately planned as the motor nerve transfers. The specific fascicular end-to-end technique may be particularly promising for controlling the sensory reinnervation. Finally, the effects of sensory training on strengthening sensory percepts after reinnervation should be further investigated.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.