
Abstract
Background:
Little is known about secondary impairments and overuse problems in patient with acquired or congenital upper limb deficiency.
Objectives:
Our aim was to estimate the frequency of overuse problems in persons after unilateral upper limb deficiency and identify the factors relevant for development of these problems.
Study design:
Cross-sectional study conducted at the University Rehabilitation Institute in Ljubljana.
Methods:
In total, 65 persons after unilateral upper limb deficiency who had visited our subspecialist outpatient clinic during the 2011–2013 period (excluding those with other possible medical causes of overuse-type problems) were interviewed about the frequency, duration and severity of neck, elbow and shoulder pain and the presence of carpal tunnel syndrome and filled in the Orthotics and Prosthetics User Survey-Upper Extremity Functional Status questionnaire.
Results:
The most frequent problem was carpal tunnel syndrome, followed by shoulder pain, neck pain and elbow pain. No statistically significant association of deficiency level, cause of deficiency, time since deficiency, extent of daily prosthesis use or type of prosthesis with frequency or severity of pain or number of problems was found. The presence of carpal tunnel syndrome decreased from wearing no prosthesis through aesthetic and body-powered to myoelectric prosthesis (p = 0.014).
Conclusion:
Factors contributing to overuse problems after upper limb deficiency are not straightforward, so a large multicentric study is warranted.
Clinical relevance
Persons with acquired or congenital upper limb deficiency are under a heightened risk of developing overuse problems but the contributing factors are not clear, so regular individual follow-up is required.
Keywords
Background
After acquired (i.e. amputation) or congenital upper limb deficiency, all functions of the human hand are lost. The persons after upper limb deficiency face problems at many activities, leisure pursuits, social contacts as well as at work.1–14 The main aim of their rehabilitation is to enable them to become independent in performing meaningful activities of daily living and to reintegrate them into society in terms of being able to participate in all social roles. This can be achieved by performing the affected task in other way, by using assistive devices, by using the residual limb only or by using upper limb prosthesis. However, even the best prosthesis is used the way we usually use the non-dominant hand – the movements differ from the movements of the non-affected hand 15 and the persons perform some compensatory movements of the trunk.16,17 High-level upper limb amputations also change the normal symmetry and balance around the shoulders and upper part of the body, 18 which results in an elevated shoulder and/or deviation of the spine in the frontal plane. The consequences of this may be overuse problems and secondary impairments. Overuse problems result from the performance of repetitive and forceful hand-intensive tasks 19 and secondary impairments are impairments that occur during the life of a person with disability, in which the primary disabling condition is a risk factor for that secondary impairment. 20
When searching the PubMed database using the ‘upper limb amputation and overuse’ query, we found only four articles, and none when searching using the ‘upper limb amputation and secondary impairments’ query. An additional article was found in the references of the initially retrieved articles. In 1978, McComas et al. 21 found reduced inhibition after stimulation of the ulnar nerve of the intact limb and suggested that it may be due to overuse. The other researchers7,22–24 used postal questionnaires. Jones and Davidson 22 tried to see all those who returned the questionnaire; Østlie et al. 24 obtained a convenience sample. None of these studies clearly states whether – and if, how – other possible causes of problems were excluded. Only Hanley et al. 23 studied some factors that may be related to the patient-reported problems.
The aim of this study was to estimate the frequency of overuse problems in persons with upper limb deficiency (either congenital or due to amputation) in Slovenia and identify the factors relevant for the development of these problems. Our hypothesis was that persons with a higher level of deficiency, with congenital upper limb deficiency, who use their prosthesis fewer hours per day, have had the deficiency for a longer time and use their prosthesis for fewer activities have more (and more severe) problems. We also anticipated that the extent of problems depends on the type of prosthesis (fewer problems in persons using a myoelectric prosthesis, followed by those wearing a body-powered prosthesis) and whether they regularly use it or not.
Methods
Subjects and procedure
We included all the people who had unilateral upper limb deficiency at the wrist or higher for at least 2 years and visited our outpatient clinic for rehabilitation of persons after upper limb amputation between September 2011 and September 2013. We excluded all the people in whom any problem may have been due to another known cause (i.e. who had any injuries of the upper limbs, other neurological or rheumatological diseases or other diseases that increase risk for overuse problems 25 ). With all the participants, the first author (MD, professor and specialist in physical and rehabilitation medicine) performed a structured interview about the frequency (never, less than once per month, less than once per week, several times per week, every day), duration (in years) and severity (rated on a 11-point scale with 0 meaning no pain at all and 10 meaning pain as bad as it could be) of neck, elbow and shoulder pain and the presence of carpal tunnel syndrome (CTS) and carried out a clinical examination. We also collected demographic and clinical data (sex, age, age at the onset of deficiency, deficiency of the dominant/non-dominant side, level of deficiency, cause of deficiency, type of prosthesis, hours of prosthesis use per day) and the participants filled in the Orthotics and Prosthetics User Survey-Upper Extremity Functional Status (OPUS-UEFS) questionnaire. 26 The data from the questionnaire were used for analysis only in terms of the number of activities performed with the prosthesis (ranging from 0 to 22). 26 This study was approved by the Medical Ethics Committee of our Institute.
Statistical analysis
Before statistical inference was performed, missing data were imputed with a combination of substantial rules and statistical models. In total, 14 values (which represent only 1.8% of the data matrix of 65 × 12 = 780 values) were imputed as follows:
For the two participants not reporting the year of deficiency onset (whereby injury was the cause of amputation in both cases), the time since amputation was regression-imputed based on age, sex and amputation level within the injury-caused amputation subgroup).
For the two participants who did not have a prosthesis, the missing number of activities performed with the prosthesis was set to zero.
For the other eight participants with missing data on the number of activities performed with the prosthesis, the missing values were regression-imputed based on the number of hours of daily prosthesis use.
For the participant who only reported frequency but not severity of shoulder and elbow problems, severity was replaced by the conditional expectation (i.e. the average severity of the participants reporting the same frequency of shoulder and elbow problems).
Because the data comprised five potential predictors (including one categorical with five categories) and three covariates (sex, age and cause of deficiency), the given sample size precluded building valid regression models for predicting the studied outcomes. Therefore, only bivariate statistical test were used. Because of the ordinal nature of the data, nonparametric statistical methods were used (but it should be noted that parametric methods, that is, t-test, one-way analysis of variance and Pearson correlation instead of exact Mann–Whitney test, exact Joncheere–Terpstra test and Spearman correlation, respectively, yielded equivalent conclusions). For the binary outcome (presence of CTS), the association with categorical risk factors was tested using either Fisher’s exact test (for cause of deficiency) or exact χ2 test of linear association (for deficiency level and prosthesis type, with categories order according to our hypothesis).
To alleviate the problem of multiple statistical test caused by numerous outcomes, we calculated three summary measures of overuse problems from the patient-reported data: maximum rating of frequency of problems, maximum pain rating and the number of reported problems (0–4 among neck, shoulder, elbow and CTS). The statistical analyses were carried out using the IBM SPSS Statistics 20 software (IBM Corp., Armonk, NJ, USA, 2011).
Results
We included 65 people in the survey (49 men and 16 women), aged 23–85 years (mean and median 58 years). The characteristics of their deficiencies and prosthesis use are presented in Table 1. The average age at the onset of deficiency was about 18 years, and they had the deficiency for nearly 40 years on average. The prevailing deficiency level was trans-radial, followed by trans-humeral. Three-fourths of the participants had undergone upper limb amputation because of injury; the majority of the participants had an aesthetic prosthesis. More than half of the participants (60%) were using the prosthesis the whole day (12–16 h daily, with nearly 50% of the participants reporting 12 h of prosthesis use per day); about one-third (34%) were using it less than the whole day and three participants (5%) were not using a prosthesis. The number of activities performed with the prosthesis ranged from 0 to 20 with an average of about 8; 39% of the participants (25/65) performed 6–10 activities of those considered by the OPUS-UEFS questionnaire using the prosthesis.
Characteristics of deficiencies and prosthesis use in the 65 included participants with acquired or congenital upper limb deficiency.
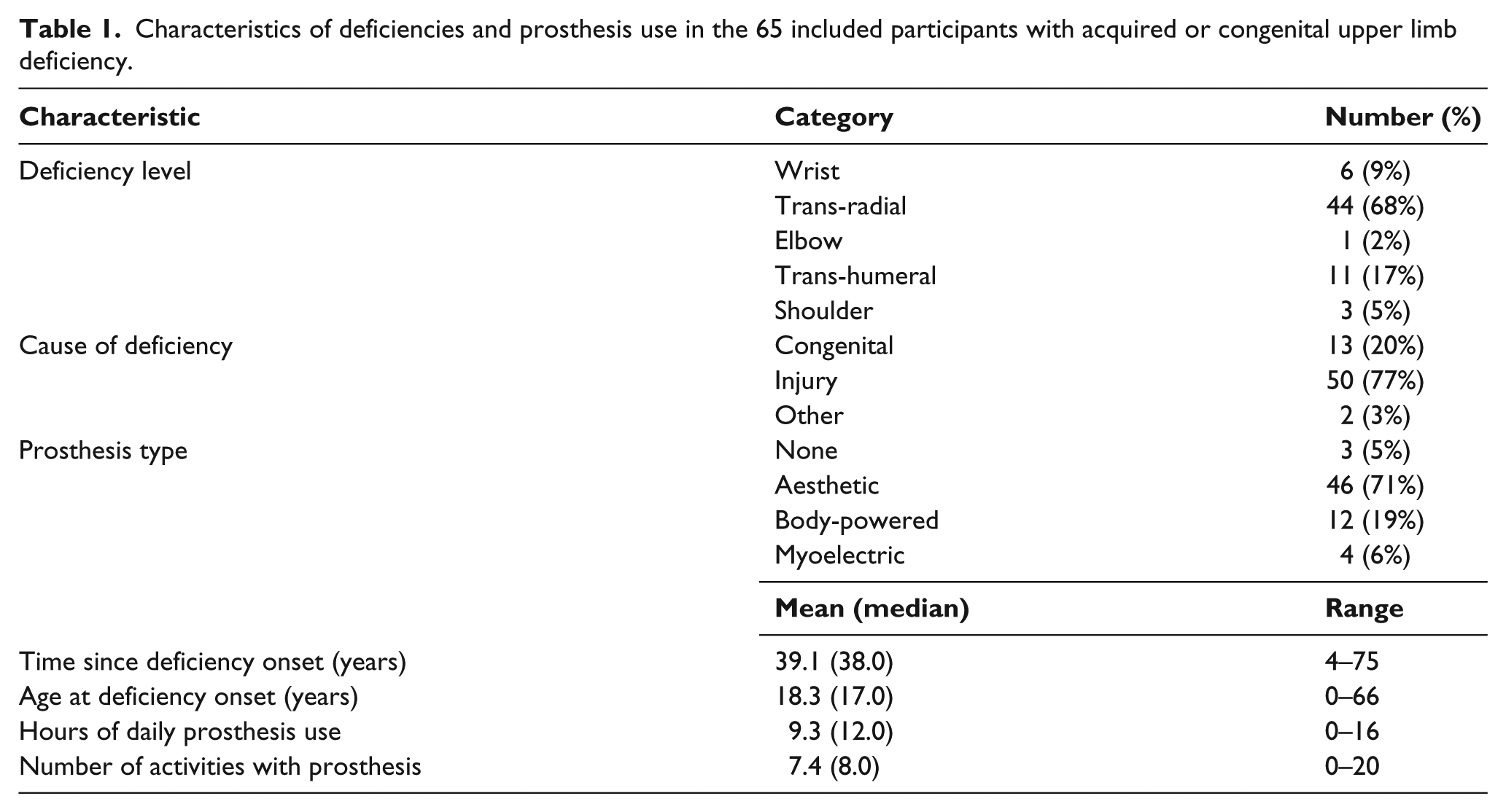
Table 2 summarises the frequency, duration and severity of the problems. Shoulder pain and CTS were much more frequent (present in about 40% of the participants) compared to neck and elbow pain (present in about 30% and 20% of the participants, respectively; p = 0.005 from exact Friedman test). Elbow pain tended to be of the longest duration (typically 6 years). Shoulder pain tended to be somewhat less severe than elbow or neck pain. The participants reported zero (28%) to four problems (3%) in total, the median being 1 (reported by 29% of the participants).
Presence, frequency and descriptive statistics for duration and severity of reported overuse problems after acquired or congenital upper limb deficiency among the 65 participants.
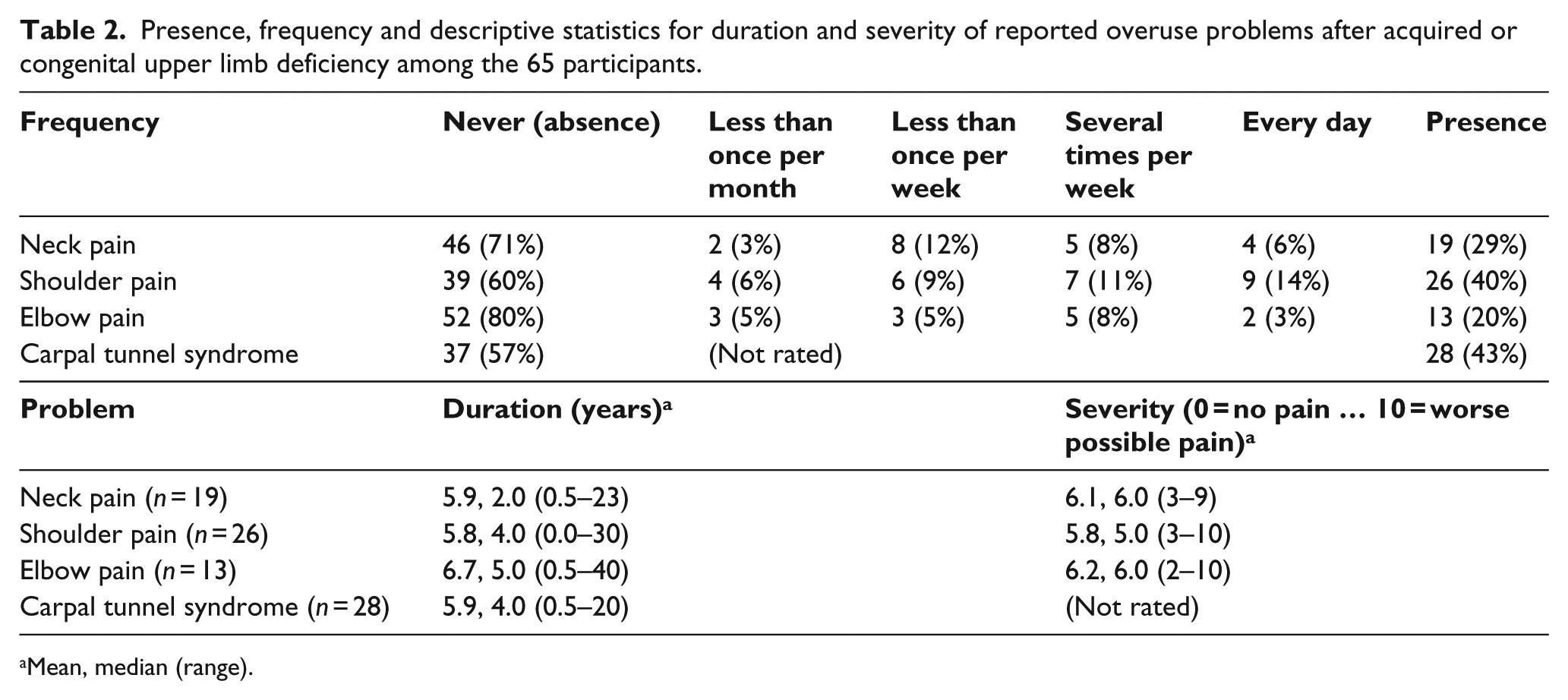
Mean, median (range).
The level of deficiency, cause of deficiency, type of prosthesis, time since deficiency onset, hours of daily use of prosthesis and number of activities for which the participants use their prosthesis were not statistically significantly associated with the summary measures (Tables 3 and 4). When the same types of analyses were performed for the original frequency and severity ratings of neck, shoulder, and elbow pain, none of the correlations or differences was statistically significant either (even without correcting for multiple tests).
Correlations of time since deficiency onset, hours of daily prosthesis use and number of activities performed with the prosthesis with the summary measures of overuse problems.
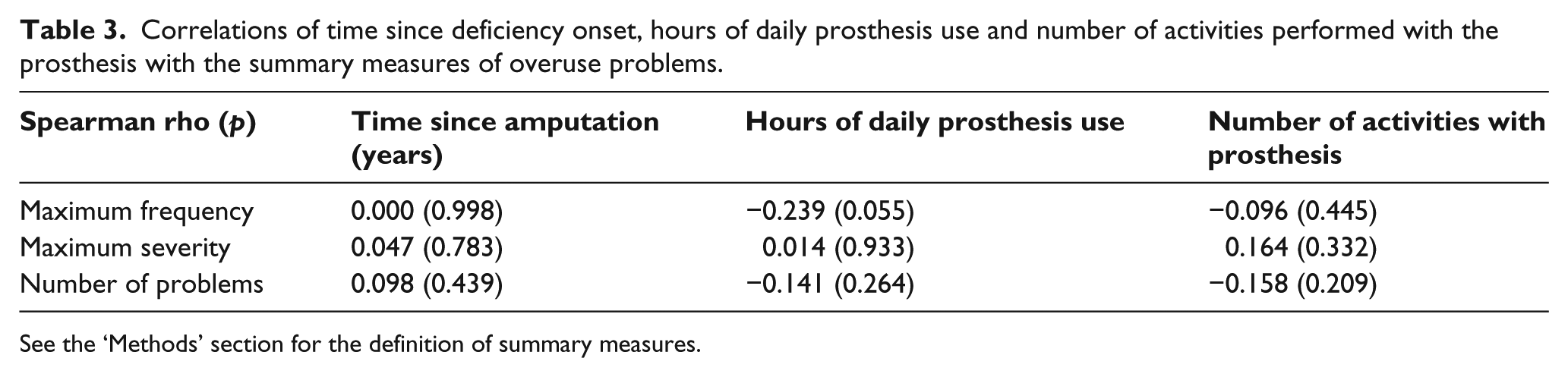
See the ‘Methods’ section for the definition of summary measures.
Descriptive statistics and results of statistical tests for comparison of summary measures of overuse problems with respect to deficiency level, cause of deficiency and prosthesis type.
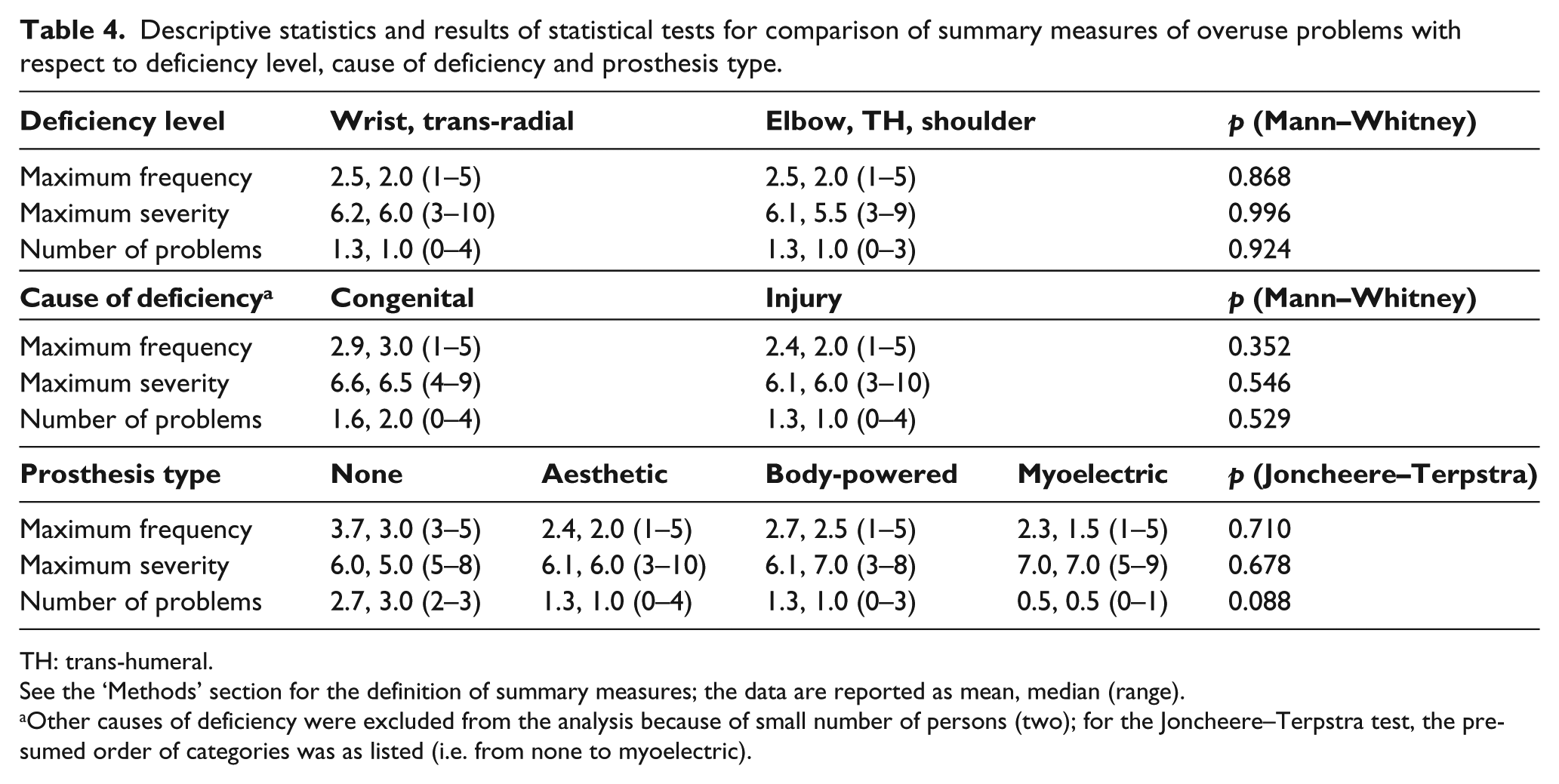
TH: trans-humeral.
See the ‘Methods’ section for the definition of summary measures; the data are reported as mean, median (range).
Other causes of deficiency were excluded from the analysis because of small number of persons (two); for the Joncheere–Terpstra test, the presumed order of categories was as listed (i.e. from none to myoelectric).
The presence of CTS was not statistically significantly associated with time since deficiency onset, hours of daily prosthesis use or the number of activities performed with the prosthesis (all p values for exact Mann–Whitney tests were above 0.05 even without correcting for multiple tests). The presence of CTS was also not statistically significantly associated either with deficiency level or cause of deficiency (p = 0.388 and 0.457 for χ2 test of linear association and Fisher’s exact test, respectively). Only the type of prosthesis was statistically significantly associated with the presence of CTS in the hypothesised way (χ2 test of linear association: exact p = 0.014). The syndrome was reported by none of the participants using a myoelectric prosthesis (0/4, 0%), one-third of those wearing a body-powered prosthesis (4/12, 33%), about one-half of those wearing an aesthetic prosthesis (21/46, 46%) and all those not using a prosthesis (3/3, 100%).
Discussion
Our survey found a much lower frequency of neck pain than previous studies7,23–26 and a slightly lower frequency of shoulder and elbow problems after upper limb deficiency than Datta et al., 7 which is most probably due to our exclusion of other possible medical causes of problems. However, we surprisingly found a higher frequency of shoulder problems on the non-amputated side than Datta et al., 7 a higher frequency of elbow problems than either Jones and Davidson 22 or Østlie et al., 24 and a higher frequency of CTS than the previous studies. These findings indicate that it is important to exclude other medical causes that may lead to the studied problems and that there may also be other factors causing the overuse problems that neither previous nor this study have addressed, such as work-related factors.
The results did not support our hypothesis that overuse problems directly depend on the level of deficiency, the cause of deficiency (amputation vs congenital), the time since the onset of deficiency, the daily amount of time during which the prosthesis is used, the number of activities it is used for and the type of prosthesis. It is a general principle that the higher the amputation, the more difficult it is to replace all the lost functions with a prosthesis. Hence, our hypothesis was that persons with a higher level of deficiency would perform more activities with the other upper limb and would thus experience more overuse problems. Persons with congenital deficiencies may experience more problems because of longer duration of impairment and the changes in their body structure. 27 However, they may experience fewer problems because they had learned to use the stump and/or the prosthesis for more activities. 3 In any case, we could not confirm a simple relationship between the extent of overuse problems and the level or cause of deficiency. The type of prosthesis appears only to be critical for developing the CTS.
The reasons for the higher frequency of overuse problems in persons with upper limb deficiency than in the general population were not exhaustively examined in this study. As already mentioned, one important factor may be work (or work-related factors); 28 another possible reason may lay in compensatory movements.15–17 If an occupational therapist observes and tries to teach a person with upper limb deficiency how to perform an activity without compensatory movements, it may be possible to prevent or at least decrease the extent of the overuse problems.
From a rehabilitation point of view, it is important to know that persons with acquired or congenital upper limb deficiency have a higher incidence of overuse problems and to use all known strategies to prevent these problems or at least delay their onset. It is also important that the problems are checked at regular follow-up so that appropriate treatment can be started immediately.
The main comparative advantage in this study is that we excluded all other medical causes that may have caused overuse problems. The main limitations are the relatively small sample size (in view of the heterogeneity of the participants and thus the small subgroups, especially the small number of participants without prosthesis and those using a myoelectric prosthesis) and not addressing other non-medical and prosthesis-related factors. In order to increase the sample size, we had collected the data for 2 years; an even longer period of data collection would not have significantly increased the number of participants because the majority of patients visit our outpatient clinic at least once every second year. However, those without a prosthesis are not visiting our outpatient clinic, and even if they have overuse problems, the physicians at the primary level will take care of them. At the same time, the national health insurance does not cover myoelectric prosthesis for adults (only for children and students), so we could not increase the number of participants with a myoelectric prosthesis. Because of this regulation, most of our participants opted for an aesthetic prosthesis and only a few found the body-powered prosthesis to be useful, which is in agreement with the findings of a previous study. 3
Another limitation in this study is that we do not have data for frequency of these problems in general population in the country and also did not include a control group. In order to increase the effective sample size in the future while considering additional factors, a multicentric study might be required.
Conclusion
Our survey of overuse problems after acquired or congenital unilateral upper limb deficiency found a much lower frequency of neck pain than previous comparable studies, which can be attributed to our exclusion of other possible medical causes of the problems. Our hypothesis that deficiency level, cause of deficiency, time since deficiency onset, extent of daily prosthesis use and the type of prosthesis bear a straightforward effect on development of overuse problems in persons with upper limb deficiency could not be confirmed. The only exception was a clear association of prosthesis type with CTS, whereby the incidence of the syndrome decreases from no prosthesis through aesthetic and body-powered to myoelectric prosthesis. Studies on larger samples, possibly multicentric and targeting a more homogeneous population while addressing other possible factors are required to gain better insight.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.