
Abstract
Background:
The liner is an integral part of a transtibial prosthesis designed to protect the residual limb, enhance comfort and provide suspension. Literature is difficult to interpret and use given the variety of interventions, outcome measures and method designs. Critical appraisal and synthesis of the evidence is needed to help inform decisions about liner prescription based on the user experience.
Objectives:
To critically appraise and synthesise research describing the user experience of transtibial prosthetic liners.
Study design:
Systematic review.
Methods:
A comprehensive suite of databases were searched using terms related to amputation level, liner type and user experience. Included studies were in English and measured the first-person experience of using a transtibial liner. Studies were appraised using the McMaster University Critical Review Forms.
Results:
A total of 18 articles met the inclusion criteria. While the quality of the evidence has improved over time, a number of common issues (e.g. sampling bias, validity of outcome measures, incorrect inferential analysis) reduce our ability to differentiate between the user experience of different transtibial liners.
Conclusion:
There is insufficient research to differentiate between the user experience of different transtibial liners. High-quality research is needed to inform decisions about liner prescription based on the user experience.
Clinical relevance
The available evidence suggests that the user experience of commonly reported problems (e.g. sweating) may be very similar between different liners. Aspects of the user experience that differ most between liners (e.g. unwanted noises, rotation within the socket) can help focus attention on what matters most when discussing prescription.
Introduction
Transtibial amputation (TTA) is most often the result of peripheral vascular disease affecting between 3 and 6 per 100,000 people.1,2 A prosthesis is usually provided to restore mobility and facilitate participation in work, recreation and self-care among other facets of life.
For people with TTA, the most important part of the prosthesis is arguably the interface between the residual limb and socket. 3 Typically, a prosthetic liner is used at this interface to help protect soft tissue from localised pressure, shear and trauma.4–6 Depending on the design of the prosthetic liner and socket, it is often used to suspend the prosthesis as well.4–8
To fulfil these functions for people with varying residual limb characteristics, prosthetic liners use different materials and suspension mechanisms. Liners are often categorised in terms of their material type (e.g. silicone), profile (e.g. conical), thickness and features (e.g. distal matrix). Some suspension mechanisms are integral to the design of the liner (e.g. Iceross Seal-In) while others are not (e.g. polyethylene foam liner in a socket with cuff suspension). 9
Given there are dozens of prosthetics liners and suspension mechanisms available, it is easy to appreciate the difficulty clinicians have providing advice to clients, or prescribing a specific intervention, 6 particularly given the limitations of the existing evidence. 5
The existing research into transtibial liners includes three published reviews.4–6 While this might indicate a well-developed body of research, closer examination shows that previous reviews have focused on the quality of the suspension (i.e. axial displacement of the socket relative to the residuum), interface pressures and characteristics of the liner materials. Unfortunately, no review has appraised evidence about the user experience of different transtibial liners.
Critical appraisal and synthesis of the literature describing the user experience is particularly important to inform discussions with clients and evidenc prescription of specific interventions.10–12 Unfortunately, the original research on transtibial liners is difficult to interpret and use given the variety of interventions, outcome measures and method design issues affecting this body of work. For example, we contend that the experience of donning the prosthetic liner may be more problematic than described in the literature given the proportion of young people included in research that have amputation due to trauma, where the effects of systemic disease and age are unlikely to have compromised hand dexterity and strength that make donning a liner more difficult.13,14
Given that the user experience has not been a focus of previous reviews and there are a number of recurrent methodological issues that affect our understanding, we believe there is a compelling need to critically appraise the research evidence to better inform our understanding of the user experience of different transtibial liners. The aim of this review was to appraise and synthesise research describing the user experience of transtibial prosthetic liners.
Methods
Search strategy
A systematic search of the literature was conducted in May 2014 using MEDLINE (Ovid, 1946–2014), CINAHL (EBSCO, 1982–2014), EMBASE (Ovid, 1980–2014), the Cochrane Library (Update Software Ltd, 1993–2014), ProQuest Nursing and Allied Health (1969–2014), AMED (Ovid, 1985–2014), and SCOPUS (Elsevier, 1823–2014).
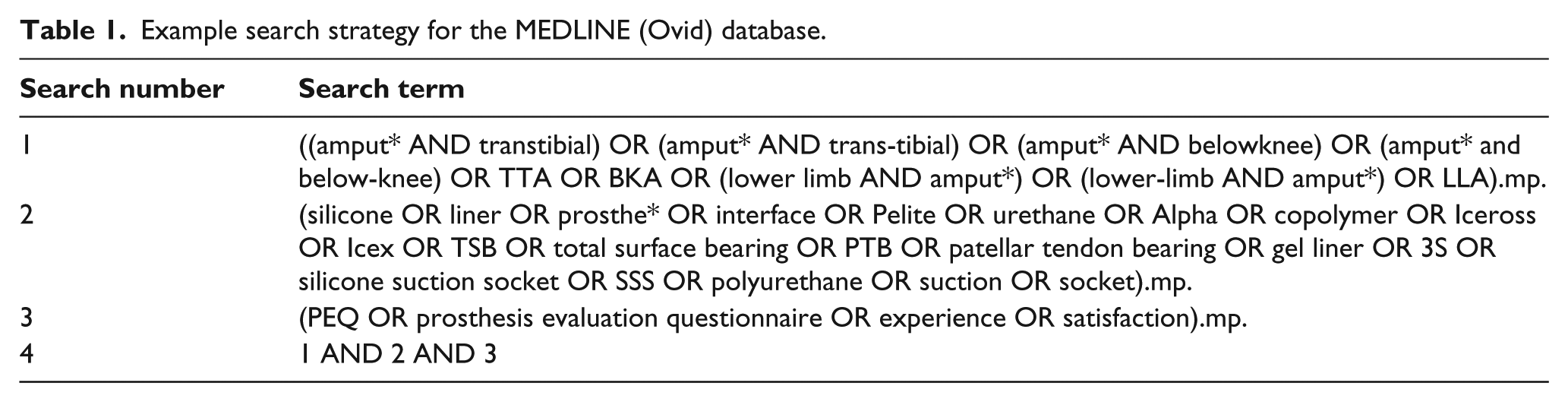
The initial search strategy was tested and refined based on the reference lists of previous systematic reviews and ad-hoc searching of the above databases. A final list of search terms related to the population, intervention and outcome, as well as their synonyms and acronyms were used with wildcards and Boolean operators as part of a title, abstract and keyword search. In keeping with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 15 an example search has been presented for the Medline database (Table 1).
Example search strategy for the MEDLINE (Ovid) database.
Study selection
Publications were included in this systematic review if they were in English and measured the first-person experience of using a transtibial liner with either quantitative or qualitative methods. Given that previous reviews have not operationally defined the intervention of interest,4–6 we defined a liner as an elastomer or foam interface worn between an individual’s residual limb and prosthetic socket. Based on this definition, and in keeping with previous reviews, a liner could consist of different materials (e.g. polyethylene closed cell foam, silicone, urethane) and suspension methods (e.g. knee sleeve, pin and ratchet lock, Iceross Seal-In). We sought to operationally define the user experience based on the development and validation of the Prosthesis Evaluation Questionnaire (PEQ), whereby rigorous efforts were undertaken to define aspects of the user experience that were important. 12 Given that a diverse range of factors may influence the user experience (e.g. appearance of the prosthesis, health of the residual limb, frustration with its use), narrow definitions would be inappropriate. As such, we were inclusive of any study that measured the first-person experience of using a transtibial liner, irrespective of the nature of the user experience.
Eligibility for inclusion was determined by the primary author (AR) based on review of the title, abstract and, as necessary, the full-text article. On occasion, a second opinion was sought from the co-author (MD) and any disagreement was resolved through discussion until consensus. As the criteria for inclusion did not require complex judgment, it was deemed unnecessary to routinely involve two authors. 16
Data collection process
A data extraction spreadsheet was developed based on the Cochrane Consumers and Communication Review Group’s data extraction, 17 that allowed demographic (e.g. age, sex, cause of amputation), methodological (e.g. study design) and quality appraisal details (e.g. check list items) to be systematically recorded.
The McMaster University Critical Review Forms 18 were used to assess methodological quality and identify sources of bias. While any number of appraisal tools could have been used given that there is no gold-standard,19,20 the McMaster tool was preferred given it is one of the few with structured guidelines to help reduce the likelihood of errors with its use.19,20 The instrument was also suitable for use in a wide variety of research designs typical of prosthetics research. Both authors independently appraised the included articles and results were subsequently compared. Any disagreements were resolved through discussion until consensus was reached. Authors of the original research were contacted for additional information as necessary.
Results
Search results
The systematic search of the databases yielded 1530 articles (Figure 1). After the removal of duplicates, 729 articles were vetted against the inclusion criteria based on title and abstract. A total of 45 full-text articles were assessed for eligibility, after which 28 were excluded because they did not meet the inclusion criteria. The references for the remaining 17 articles were hand searched, resulting in an additional five articles, of which one met the inclusion criteria. Ultimately, 18 articles were included in the systematic review.
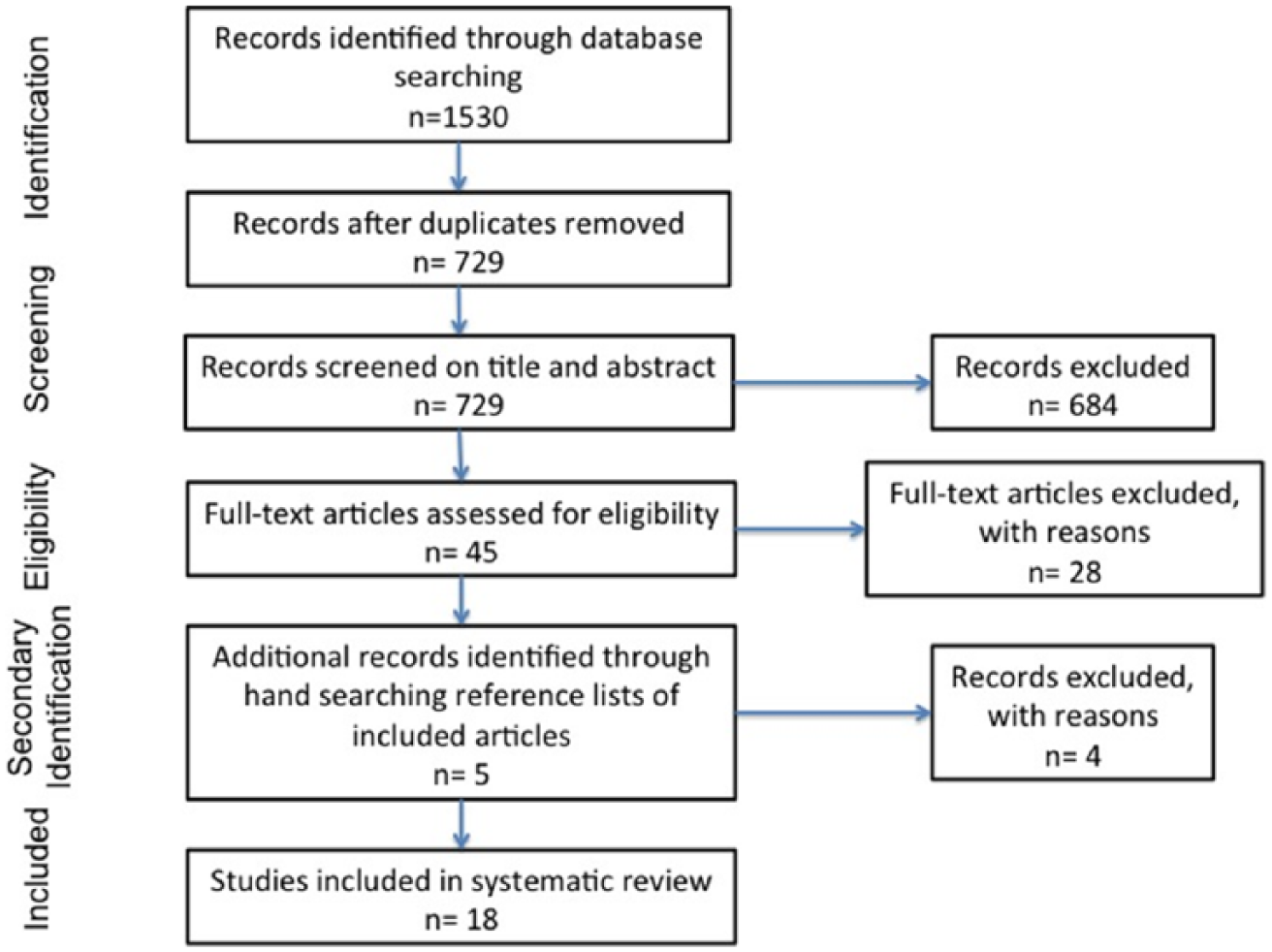
Flow of information through systematic review search process.
Characterisation of included studies
Study design
Of the included studies, 11 were before-and-after trials,7,8,21–29 one was a randomised controlled trial (RCT), 30 two were case-control studies,31,32 and the remaining 4 studies were cross-sectional surveys.33–36 The majority of these investigations were completed in a laboratory or rehabilitation facility setting7,8,21,22,27–30 using small subject numbers (e.g. <15).6,8,21–24,27,29,34 All investigations employed quantitative methods to understand the patient experience of using a prosthetic liner.
Subject characteristics
Participants included in research tended to be middle-aged, male, with amputation due to trauma many years prior to the study (Table 2).7,8,21–36 Details about common comorbidities were reported in few of the included studies.24,31,35
Population characteristics.
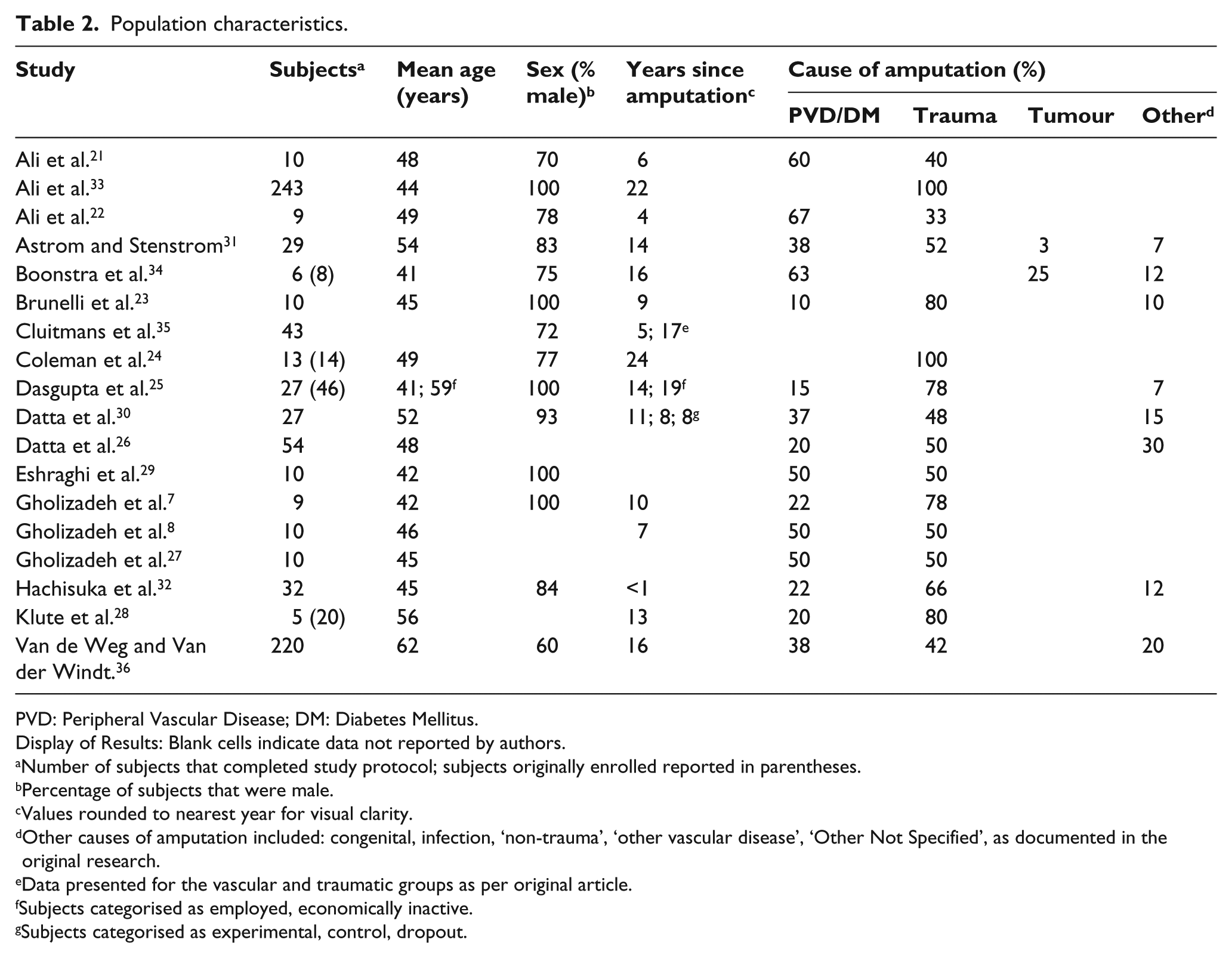
PVD: Peripheral Vascular Disease; DM: Diabetes Mellitus.
Display of Results: Blank cells indicate data not reported by authors.
Number of subjects that completed study protocol; subjects originally enrolled reported in parentheses.
Percentage of subjects that were male.
Values rounded to nearest year for visual clarity.
Other causes of amputation included: congenital, infection, ‘non-trauma’, ‘other vascular disease’, ‘Other Not Specified’, as documented in the original research.
Data presented for the vascular and traumatic groups as per original article.
Subjects categorised as employed, economically inactive.
Subjects categorised as experimental, control, dropout.
Measuring the user experience
The user experience was measured using a variety of techniques with varying degrees of rigour. Most studies used some form of author-designed questionnaire.7,8,21,22,25–27,29,31–36 A number of these author-designed questionnaires were purportedly based on the PEQ where investigators selected isolated questions or made adaptations thereby, effectively, designing their own instrument.7,8,21,22,27,29,33,36 A few studies used validated tools to measure the patient experience (i.e. PEQ, Socket Comfort Score).23,24,28 By contrast, some investigators asked research participants to provide feedback in casual conversation and unstructured interviews.26,35,36
Types of intervention
A wide variety of liners were described in the included studies (Table 3). The early literature tended to compare the standard clinical treatment of the day (e.g. Pelite® liner with sleeve suspension) to a new liner technology (e.g. Iceross silicone liner with pin suspension).24,26,30,33–36 In the very early silicone liner studies, investigators laminated their own elastomer liners.32,34 As elastomer liners became more common, experiments including a Pelite liner condition became rare. Most studies including a Pelite liner condition were conducted prior to 2005,24,26,30,34–36 with only one study published since. 33
Summary of aims, study designs, interventions, outcome measures and findings of studies included in the review.
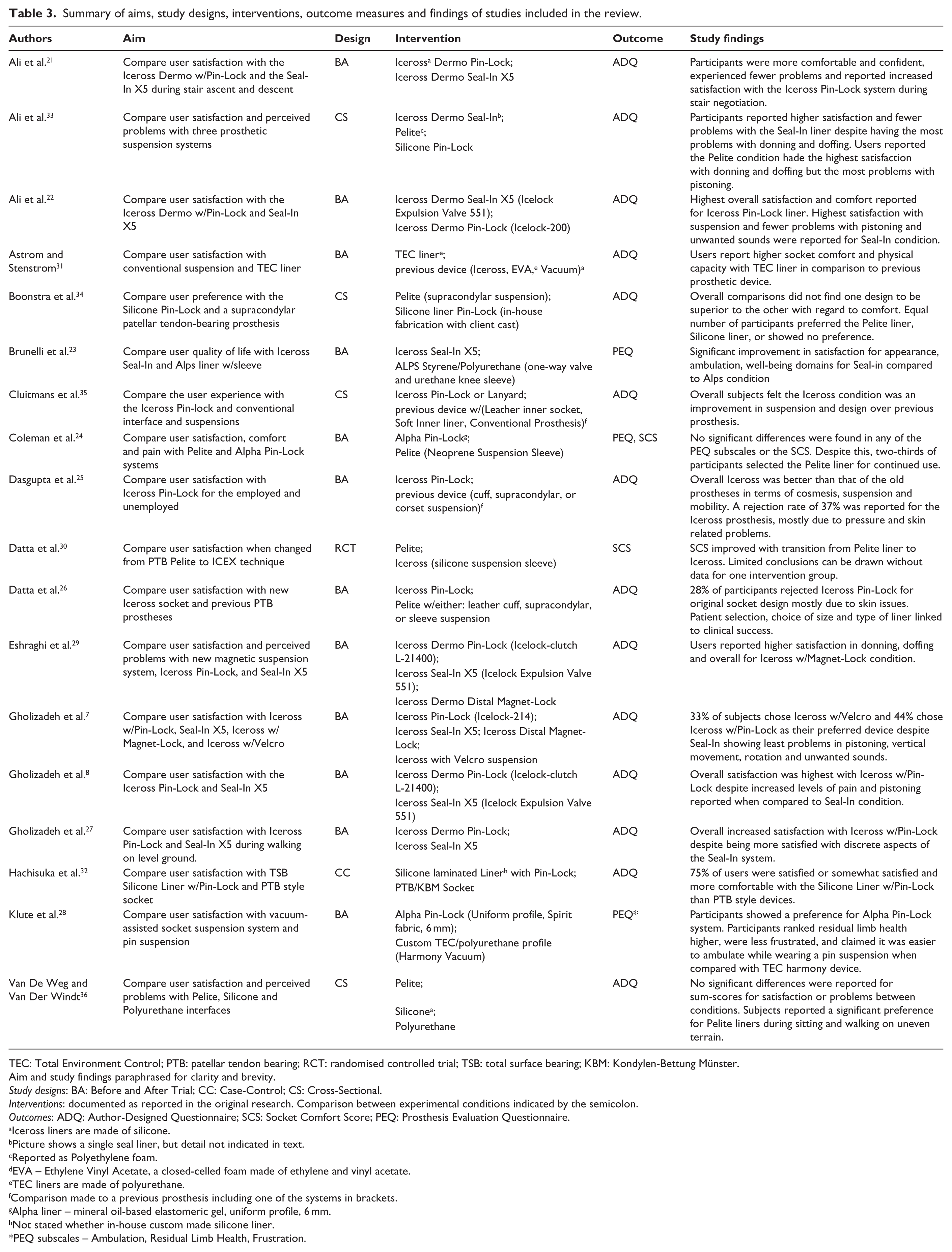
TEC: Total Environment Control; PTB: patellar tendon bearing; RCT: randomised controlled trial; TSB: total surface bearing; KBM: Kondylen-Bettung Münster.
Aim and study findings paraphrased for clarity and brevity.
Study designs: BA: Before and After Trial; CC: Case-Control; CS: Cross-Sectional.
Interventions: documented as reported in the original research. Comparison between experimental conditions indicated by the semicolon.
Outcomes: ADQ: Author-Designed Questionnaire; SCS: Socket Comfort Score; PEQ: Prosthesis Evaluation Questionnaire.
Iceross liners are made of silicone.
Picture shows a single seal liner, but detail not indicated in text.
Reported as Polyethylene foam.
EVA – Ethylene Vinyl Acetate, a closed-celled foam made of ethylene and vinyl acetate.
TEC liners are made of polyurethane.
Comparison made to a previous prosthesis including one of the systems in brackets.
Alpha liner – mineral oil-based elastomeric gel, uniform profile, 6 mm.
Not stated whether in-house custom made silicone liner.
PEQ subscales – Ambulation, Residual Limb Health, Frustration.
Over the last decade, studies have sought to understand the user experience of wearing elastomer liners of different materials (e.g. silicone, urethane),7,8,21–23,27–29 in conjunction with different socket suspension mechanisms including clutch/ratchet lock,7,8,21,22,24,27–29,33 magnetic lock,7,29 lanyard, 35 passive suction (i.e. Iceross Seal-In),7,8,21–23,27,29,33 suspension sleeve,23,24,26,30 elevated vacuum, 28 and Velcro. 7 Given that the liner and suspension mechanism are often combined into a single experimental condition, it was often impossible to examine the effect of changes to the liner or suspension mechanism independently.
Research quality
Based on the McMaster University Critical Review Form, 18 there were a number of recurrent issues affecting both the external and internal validity of studies included in the review. A detailed analysis of included studies is included as an Appendix (supplementary material). A summary of issues affecting study validity is included below.
Representativeness of the sample
Participants included in research were not representative of the broader population of people with TTA. While most studies stipulated their recruitment method7,8,21–28,30–34 none used random sampling. Participants in early liner research tended to be purposively sampled because transitioning from a conventional socket with polyethylene or Pelite® liner to a new prosthesis with a silicone liner was thought to resolve recurrent socket fit problems such as skin breakdown, rashes and blisters.25,26,34,35 Many studies excluded people that were unable to walk: without gait aids,8,22,27,30 on uneven ground, 23 on stairs, 21 or for 30 continuous minutes on a treadmill; 28 thereby reducing the representativeness of the sample.
Intervention
It was difficult to know exactly what interventions were tested in many studies because limited details were provided (Table 3).7,25–27,30–36 While, details about the brand of liner were often reported (e.g. Alpha), additional information such as liner covering (e.g. Alpha liner with either original, spirit or max covering) were not.
Appropriateness of the comparisons
A number of the studies utilised the subject’s existing prosthesis as one of the test conditions and drew comparison to a newly made device with a different liner system.23,25,26,30,31,35 Unfortunately, this experimental design introduced a number of sources of bias. For example, participants may have a better experience with the new liner simply because the new prosthesis fitted better than the old one. Many studies required participants to recall their experience of a previous device after transitioning to a new one, often after many weeks or months.8,22,23,25,26,31,32,34,35
Acclimatisation
There were a wide variety of acclimatisation periods reported from weeks7,8,21–23,26–30,33,34 to several months24,26,31,34 and potentially even years in studies that used the subjects existing prosthesis as one of the test conditions.23,25,26,30,31,35 Participants were also given different lengths of time to acclimatise to test conditions (e.g. many months or years in an existing device and a few weeks in a new one).23,25,26,30,31,35
Validity and reliability of outcome measures
The early literature tended to use author-designed questionnaires to describe the user experience without demonstrating validity of the instrument.25,32,34,35 With the introduction of the PEQ in the late 1990s, investigators had access to a valid, reliable and population specific outcome measure of the user experience.11,12 While most of the literature on this topic has been published since the development of the PEQ, only a few studies have used the complete measure23,24 or its discrete subscales. 28 A number of recent studies described using questionnaires based on the PEQ7,21,22,27,29,33 without providing sufficient detail to assess the claim that the instrument was based on the PEQ or make a determination about its psychometric properties. Only two studies using author-designed questionnaires provided this level of detail8,36 and it seems that isolated questions were taken from some PEQ subscales without justification for focusing on discrete aspects of the user experience.8,36 While these author-designed surveys may have been based on the PEQ, it was not reasonable to assert their validity and reliability given the use of isolated questions about the user experience, different anchors, and inclusion of a numerical scale, which have each been shown to influence responses on a Visual Analogue Scale (VAS). 11 All but one of these studies 36 reported data on seemingly identical outcomes and were authored by many of the same investigators. Therefore, contact was made with the primary authors to determine whether the questionnaire used by Gholizadeh et al. 8 was also used in other articles by this group.7,21,22,27,29,33 We were able to confirm that the same questionnaire was used in all of these investigations (H Gholizadeh, 4 September 2014, personal communication).
No studies included in the review used qualitative research methods to systematically gather and analyse information about the user experience. Instead, researchers loosely use the term ‘qualitative’ to describe their recording of user opinion or comment.26,35,36
Inferential analysis
Most investigations did not use appropriate statistical methods to compare the user experience of different liners.7,8,21–31,33,35 Authors often used simple inferential analysis techniques (e.g. paired t-tests) to make multiple comparisons without controlling for the likelihood of type I error.7,8,21–25,27,29,33 While a number of authors used more sophisticated inferential techniques suited to multiple group comparisons,7,29,36 a number of common mistakes compromised the results. For example, results for main-effects or post-hoc tests were often not reported or were incorrectly reported.7,36 In some studies, post-hoc analyses were conducted using a series of t-tests without controlling for the risk of type I error.7,29
Results narrative
A chronological narrative has been presented to contextualise results and show how our understanding about the user experience of different transtibial liners has evolved over time.
We grouped a number of studies into the category of ‘early literature’ because they compared similar interventions, had similar method design issues and therefore, informed our understanding in a similar way. By contrast, studies included in the category of ‘contemporary literature’ compared a broader range of interventions and tended to use more appropriate research designs.
Early literature
Literature describing the user experience of different transtibial liners dates to the time when elastomer liners were first introduced. The early literature sought to compare the new elastomer liner technology (e.g. silicone liner) with the standard treatment of the day, most commonly a polyethylene foam liner (i.e. Pelite® liner) with either supracondylar, cuff, knee sleeve or thigh corset suspension.25,26,30–32,34,35 A number of investigators seemed to purposively sample participants whom they thought would benefit from the new liner technology given a history of chronic skin and socket fitting problems25,26,34,35 or because the participants’ existing prosthesis was considered suitable for one of the test conditions.30,31 The sampling method partly explains why participants were not representative of the broader population of people living with TTA (Table 2); that is, mostly middle-aged men with traumatic amputation many years prior.25,26,30–32,34,35 A number of these studies compared an existing prosthesis (often worn for many months or years) to a new device,25,26,30,31,35 thereby introducing bias given differences in acclimatisation between the test conditions and differences in the quality of the socket fit between an old and new prosthesis. Recall bias was an issue given the difficulties of accurately recalling the experience of the first liner condition after having transitioned to the second.25,26,31,34,35
Although not exhaustive, these method design issues serve to illustrate the most significant limitations of the early literature which makes it difficult to vest confidence in the findings. By way of example, a number of these studies describe greater comfort and fewer socket fit problems with the new elastomer liner technology when compared to the previous interface.25,26,30,31,35 Unfortunately, given the limitations of the research designs used, we have no way of knowing whether the improvements observed were due to the new elastomer liner or simply the result of having a new and better fitting prosthesis. Similarly, a number of investigators noted ongoing skin problems after transitioning to the elastomer liner condition,25,26,31,32,35 some with large numbers of drop-outs.25,34 Given the research designs that were used, we cannot determine whether these problems were due to the elastomer liner or a reflection of having purposively sampled people with chronic skin and socket fitting problems. There may also be a confounding influence of developing familiarity and expertise with the new liner technology.
Contemporary literature
Over time, a wider variety of elastomer liners became available including silicone materials of different durometers and thicknesses (e.g. Iceross Dermo), alternative materials (e.g. urethane or mineral-based oils), various liner coverings (e.g. Alpha liner with Spirit fabric) and alternative suspension methods (e.g. Iceross Seal-In, magnetic pin-locks). Not surprisingly, the increased options were also reflected in research studies as investigators sought to understand their benefits (Table 3).
While the wider range of interventions delineated the early and contemporary research, so too did improvements in research quality. Two studies in particular characterise this shift in research quality.24,36 Both of these studies used outcome measures that were reliable and took care to minimise common forms of bias in the design of the method.24,36 Coleman et al., 24 for example, designed a prospective study whereby participants were randomly allocated to receive a new prosthesis with either a Pelite or Alpha liner as part of a cross-over design. Outcomes were measured following lengthy acclimatisation and the potential confounding influence of wear-time was monitored using a Step-Activity-Monitor. While both studies24,36 had their limitations (see Appendix), the improved research quality provides more compelling evidence that elastomer liner technology may not improve satisfaction and the user experience, a finding contrary to the prevailing view. Van de Weg and Van der Windt 36 found small and insignificant differences in satisfaction and perceived problems between polyethylene foam, silicone- and urethane-liner conditions in a cross-sectional survey of more than 200 participants (Table 3). Similarly, Coleman et al. 24 found no difference in any of the PEQ subscales scores (Table 4) or the SCS, between the polyethylene foam and Alpha liner conditions. This finding is interesting given that two-thirds of people selected the polyethylene foam liner for continued use. 24 This dichotomy between the PEQ results and preference for the Pelite liner may reflect a range of considerations: previous prosthetic experience, sensitivity of the PEQ to identify differences between liner conditions or the need to control for covariants (e.g. differences in wear-time) between the experimental conditions as part of the inferential analysis. 24
Results of studies that utilised the PEQ.
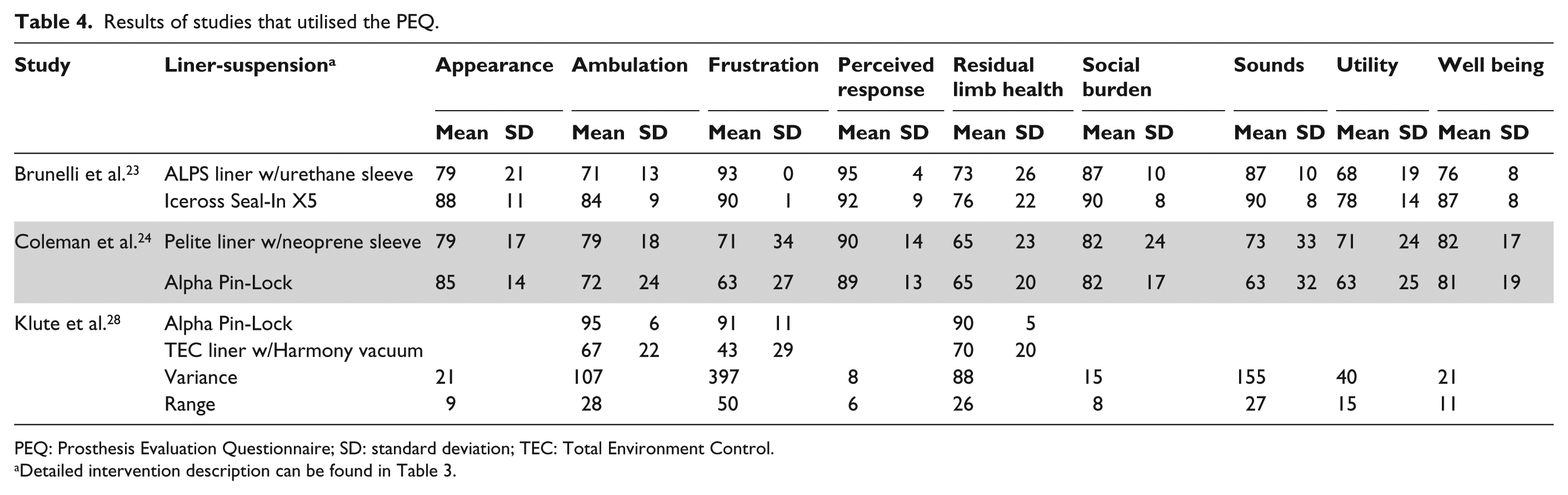
PEQ: Prosthesis Evaluation Questionnaire; SD: standard deviation; TEC: Total Environment Control.
Detailed intervention description can be found in Table 3.
In addition to this work by Coleman et al., 24 only two other studies used the PEQ to evaluate the user experience.23,28 Unfortunately, substantive issues were identified in both studies that reduce confidence in the conclusions drawn (Table 3). Reminiscent of the early literature, Brunelli et al. 23 compared an existing device (i.e. at least 18 months old) to a new prosthesis with a different liner system (see Appendix). Klute et al. 28 had a much more robust design in many respects (i.e. prospective study, randomised cross-over design), but 75% of participants dropped out (see Appendix). While large differences in the three PEQ subscales between the experimental conditions (Table 4) would suggest a real difference – something we are unable to confirm without an inferential analysis – the data reflect a biased sample of those that completed and, in all likelihood, did not experience problems with the TEC liner and Harmony vacuum system.
Unfortunately, no two investigations that used the PEQ compared the same interventions, or even the same family of interventions (e.g. some form of liner with distal pin vs. liner with suspension sleeve), which made it impossible to synthesise results across these studies (Table 4).
While we were unable to synthesise results for studies using the PEQ, the usual process of gathering data as part of a systematic review highlighted that a number of subscales of the PEQ – Perceived Response, Social Burden and Utility – had very similar scores across studies with different populations and liner conditions (Table 4). Bearing in mind the methodological limitations, this might suggest subscales of the PEQ that are not sensitive to differences in liner conditions (Table 4). By contrast, the PEQ subscales of Frustration, Sounds and Ambulation showed large variability and may therefore be better indicators of differences in the user experience between liner conditions (Table 4).
To attribute this large variability in some of the PEQ subscales scores to differences between various liners, research has to be designed to control for the confounding influence of other factors. This is perhaps best illustrated by comparing two studies that both used an Alpha liner with pin-suspension condition (Table 3).24,28 The three PEQ subscales in common – Ambulation, Frustration and Residual Limb Health – each differed by more than 20 points (Table 4). While the populations were similar in terms of age, and cause of and time since amputation, there were significant differences in terms of acclimatisation (4 weeks 28 vs. 12 weeks 24 ) and familiarisation with the test conditions prior to the experiment. All participants in the study by Klute et al. 28 used a liner and pin-suspension system prior to the study whereas only 23% of people used such a system in the study by Coleman et al. 24 It seems reasonable to hypothesise that individuals who were more familiar with the intervention prior to the study would have lower levels of frustration with its use during the investigation.
The majority of studies included in the contemporary literature were published by the same research group over a 2-year period.7,8,21,22,27,29,33 These investigations were funded by the same grant, and may include many of the same participants given the similarity of the population characteristics reported (Table 2). Certainly two of these studies included the same participants as evidenced by the identical subject characteristics.8,27
These investigations drew comparison between some form of Iceross Seal-In and Iceross Dermo with distal pin-lock.7,8,22,27,29,33 Two of these studies also drew comparison to a Pelite 33 or silicone liner with Velcro suspension condition. 7
As part of the quality evaluation, we were critical of these studies given their adaptation of the PEQ and limitations of the inferential analysis.7,8,22,27,29,33 A number of these studies are at high risk of type I error given their use of multiple paired-comparisons. These studies often reported small differences in the satisfaction and problems scores between the experimental conditions that were highly significant. For example, Eshraghi et al. 29 reported that mean scores for ‘problems with rotation of the socket’ differed very little between the silicone liner with magnetic lock (81.65) and pin-lock (80.18) conditions despite the very significant p-value of 0.017. We contend that these sorts of significant findings are likely to be spurious, a reflection of conducting post-hoc tests using a series of 54 paired t-tests without controlling for the family-wise error rate. 29 While this example may seem extreme, it is not in isolation7,8,21,22,29 Gholizadeh et al. 7 conducted 42 paired t-tests in their study with similarly problematic outcomes. Even in studies with more sophisticated multiple group comparisons, post-hoc analyses were not reported which made it impossible to determine which interventions were different.29,33 None of these studies included measures of variability which also made it difficult to use the descriptive statistics to draw comparisons between the experimental conditions.
While the range of methodological problems reduce confidence that these studies report real differences in the user experience between specific liner conditions,7,8,21,22,27,29,33 it would be disingenuous to disregard what might be learnt through cautious exploration of these descriptive data, particularly given that these studies all used the same outcome measure and compared some form of liner with pin suspension to a Seal-In system (Table 5).
Results of studies that utilised the same author-designed questionnaire.
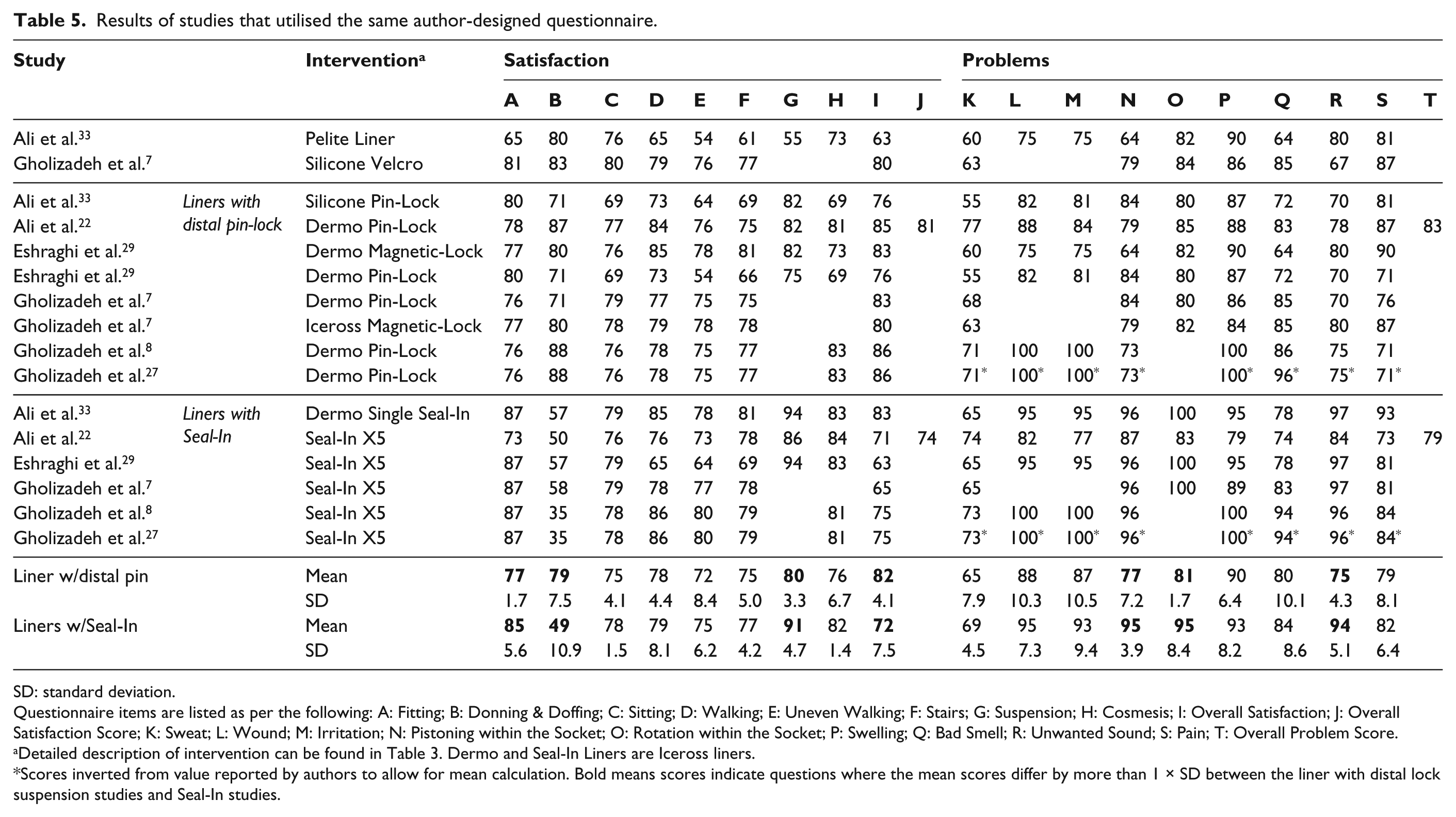
SD: standard deviation.
Questionnaire items are listed as per the following: A: Fitting; B: Donning & Doffing; C: Sitting; D: Walking; E: Uneven Walking; F: Stairs; G: Suspension; H: Cosmesis; I: Overall Satisfaction; J: Overall Satisfaction Score; K: Sweat; L: Wound; M: Irritation; N: Pistoning within the Socket; O: Rotation within the Socket; P: Swelling; Q: Bad Smell; R: Unwanted Sound; S: Pain; T: Overall Problem Score.
Detailed description of intervention can be found in Table 3. Dermo and Seal-In Liners are Iceross liners.
Scores inverted from value reported by authors to allow for mean calculation. Bold means scores indicate questions where the mean scores differ by more than 1 × SD between the liner with distal lock suspension studies and Seal-In studies.
These descriptive data (Table 5) suggest that ‘overall satisfaction with the prosthesis’ was higher with a liner and pin-suspension system (82 ± 4) compared to the Iceross Seal-In (72 ± 8), consistent with the conclusions reported in these studies.7,8,22,27,29,33 Differences in overall satisfaction seem to reflect that participants were more satisfied with their ‘ability to donn and doff the prosthesis’ with the liner and pin-suspension system (79 ± 8) compared to the Iceross Seal-In (49 ± 11) (Table 5). The similarity in mean scores might suggest that users were similarly satisfied with walking and the appearance of the liner with pin-suspension and Seal-In systems (Table 5). In terms of the user experience of problems, scores suggest users had few problems with either the Seal-In or liner with pin-lock interventions (Table 5). Users did rate being more bothered by pistoning, rotation within the socket and unwanted noise in the liner with pin-suspension system compared to the Iceross Seal-In (Table 5). Scores were very similar across the other questions (e.g. sweating) suggesting similar experience of these problems between the two families of liners (Table 5).
Discussion
Despite the number of published studies, the poor quality of research makes it difficult to be confident there are real differences in satisfaction and the user experience between various transtibial liners and suspension methods.
Clinical guidance
Although limited, the available evidence may provide some guidance to clinicians. The large variability in a number of domains of the PEQ, and specific questions in author-designed surveys, might indicate which aspects of the user experience are the most sensitive to differences between liners. This understanding could be used to focus discussions with clients about what matters most. For example, when comparing a liner with distal-pin and Seal-In system, the descriptive data suggests there may be very little difference in the experience of sweating or satisfaction with walking. As such, it may be helpful to focus on aspects of the user experience that seem to differ most between these liner options including ease of donning/doffing, the quality of the suspension, the experience of unwanted sounds or rotation within the socket. A focus on these particular aspects of the user experience may help guide the choice of intervention based on factors that matter most to a given client.
Future research
Unfortunately, our ability to draw more meaningful conclusions about the user experience of different liners was limited by a number of consistent methodological flaws. Future research could be dramatically improved with careful attention to a few key method design issues.
Researchers should include more representative samples that better reflect the age, sex, cause of amputation and comorbidity profile of the broader population of people living with TTA. This will make it possible to generalise what we learn from research to clinical practice. More representative samples could be achieved through the use of random sampling techniques and inclusion criteria that do not preclude participation by individuals with limited mobility or comorbidities typical of those living with limb loss.
More sophisticated inferential analysis techniques are required given the number of independent and dependent variables typically used in studies of different liners, and the need to control for common covariants that may influence the user experience (e.g. age, dexterity, cause of amputation). The use of more sophisticated analysis techniques (e.g. multivariate analyses of covariance, MANCOVAs) is recommended as an alternative to the simpler techniques that characterise the existing body of work. These inferential analysis techniques will require larger samples than have typically been included in research to date. Complete reporting of descriptive statistics (e.g. standard deviations) and inferential analyses (f-ratios, degrees of freedom, effect size) are important for critical analysis and to be able to conduct meta-analyses in the future.37,38
Complete reporting of the interventions and outcome measures is also required.37–39 The frequent lack of detailed reporting of the intervention limited our confidence that the same interventions were being compared or synthesised. 39 Similarly, outcome measures need to be adequately described so that it is clear what aspects of the user experience are being explored. Many reporting guidelines are available to researchers15,37–39 to ensure completeness of the information reported and we encourage their use.
Researchers could contribute to the body of work by conducting observational and qualitative studies to identify sensitive and reliable indicators of the user experience of different transtibial liners. Unfortunately, studies comparing different liners have proceeded without a solid foundation of observational and qualitative studies that first demonstrate which outcome measures are important and can differentiate between the user experience of different transtibial liners.
Many of the negative experiences reported by participants (e.g. rotation within the socket, unwanted sounds) are also common consequences of poorly fitting liners and poorly designed socket shapes. While we were unable to attribute any of these negative experiences to issues with the prostheses provided in research studies, we reiterate the need for diligence in sizing of liners and ensuring well-designed and well-fitting sockets prior to data gathering.
Limitations
A single reviewer completed the search and determined eligibility of studies for inclusion in the review. We did not utilise two reviewers given that complex judgment was not required.
While a large number of studies were included in the review and many used the same outcome measure, we adopted a narrative approach given that limitations of the existing evidence would not allow more sophisticated synthesis using statistical methods.
It may be perceived as a limitation that we have not reviewed specific interventions in the detail some may wish. This has been done deliberately given our view that the evidence does not allow definitive statements to be made about the benefits or drawbacks of specific liners. We were deliberate in not providing a paper-by-paper review or reiterating results from individual studies ad nauseum. We felt this would serve little purpose beyond reading the original research. Instead, we hope the insights presented highlight what we currently know, fairly guide clinicians given the limitations of the evidence as well as identify avenues to improve the research evidence.
Conclusion
Despite the number of published studies, there was limited evidence to determine if the user experience differed between transtibial liners. The available evidence suggests that many aspects of the user experience may be similar between transtibial liners (e.g. sweating). Focusing on aspects of the user experience that seem to differ most (e.g. ease of donning, the quality of the suspension, the experience of unwanted sounds or rotation within the socket) may help guide discussions about what is important and thereby facilitate more informed decisions about liner prescription based on the user experience.
While the literature documents the user experience of hundreds of people with TTA, a number of consistent methodological flaws limit what we can learn from these investigations. Future research should utilise valid and reliable outcomes, recruit representative samples and employ inferential analysis technique appropriate to the complexity of the research design. By focusing on these aspects of the reporting and method design, future research will be able to make a more meaningful contribution to our understanding of the user experience of different transtibial liners.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.