
Abstract
Background:
Iliocostal impingement syndrome is a rare, painful, and disabling condition associated with thoracic hyperkyphosis and kyphoscoliosis. There is little published literature regarding management of this syndrome. The purpose of this case series is to report treatment outcomes for iliocostal impingement syndrome with improving posture and back muscle strength.
Case Description and Methods:
Thirty-eight women with thoracic hyperkyphosis or kyphoscoliosis and back and/or flank pain were diagnosed with iliocostal impingement syndrome on the basis of symptoms and spine radiographs. They were instructed in weighted kypho-orthosis use and taught a home back-extensor strengthening program. Outcome measures included posture evaluation and pain level.
Findings and Outcomes:
All patients reported immediate pain reduction with weighted kypho-orthosis trial. Nineteen patients returned within 2 years, and all had continued pain relief and posture improvement.
Conclusions:
Our findings suggest that successful management of iliocostal impingement syndrome is possible with a weighted kypho-orthosis and back strengthening program focusing on posture improvement.
Clinical relevance
Iliocostal syndrome is a rare, painful, and disabling condition that severely affects quality of life. This report discusses our diagnostic and treatment approach to this syndrome, which has proven successful in our patient population.
Background
Chronic back pain and kyphotic posture can develop insidiously as a result of reduced back-extensor strength and vertebral microfractures associated with osteoporosis. The kyphotic or kyphoscoliotic deformity can cause direct contact of the lowermost ribs on the ilium, resulting in iliocostal impingement syndrome. Symptoms can include back or flank pain, which in turn can interfere with participation in daily physical activities and decrease quality of life. 1 With severe hyperkyphosis, respiratory function can even become compromised. Most commonly, iliocostal impingement syndrome results from severe spinal osteoporosis, but it can also be associated with any condition resulting in thoracic hyperkyphosis, such as trauma or congenital deformities. 1 Iliocostal impingement syndrome has also been referred to as iliocostal friction syndrome, 1 costo-iliac impingement syndrome, 2 and costo-iliac abutment.
Diagnosis and treatment of iliocostal impingement syndrome can be challenging for various reasons. The differential diagnosis of nonspecific low back and flank pain is extensive, including intrathoracic, intra-abdominal, neurologic, and musculoskeletal causes. A thorough history and physical examination are essential to determine appropriate evaluations for a patient’s symptoms. After alternative causes have been ruled out, tenderness to palpation of the iliocostal region, thoracic hyperkyphosis, and thoracic spine radiographs demonstrating contact of the lowermost ribs on the ilium can aid in the diagnosis of iliocostal impingement syndrome.
Patients with thoracic hyperkyphosis, kyphoscoliosis, and osteoporosis are regularly treated in our Rehabilitation of Osteoporosis Program Exercise (ROPE) clinic. This program includes instruction on use of a back-extension orthosis in combination with a home exercise program emphasizing back-extensor muscle strengthening and posture training. To our knowledge, this article is the first published case series regarding treatment outcomes for iliocostal impingement syndrome with use of the ROPE program.
Case description and methods
Subjects and clinical assessment
Thirty-eight women presented to our outpatient tertiary-care rehabilitation clinic with back or flank pain and kyphotic or kyphoscoliotic posture. Appropriate medical evaluations to rule out non-musculoskeletal causes for their pain were performed at either an outside facility or our clinic before presentation. Additionally, all patients had bone mineral density measurements before presentation. All patients were evaluated by the senior author (M.S.), who regularly evaluates patients with osteopenia and osteoporosis with or without spinal deformities through the ROPE program. Anteroposterior and lateral thoracolumbar spine radiographs were obtained and showed hyperkyphosis and contact of the ribs on the ilium in all subjects. Hyper-kyphosis was defined as 40° of forward flexion of the thoracic spine, diagnosed radiographically. The patients’ degree of back or flank pain was assessed and rated as mild, moderate, or severe. On the basis of their symptoms and radiographs, iliocostal impingement syndrome related to thoracic hyperkyphosis or kyphoscoliosis was diagnosed in all patients by the senior author. For the patients who returned for follow-up visits, repeat radiographs were obtained on an individual basis.
Intervention
A trial of a weighted kypho-orthosis (WKO) was performed at the initial evaluation with the senior author. On clinical evaluation, if a patient had subjective pain relief and objective posture improvement, defined as a few degrees of kyphosis reduction, with the WKO trial, she was instructed on proper use of the WKO and performance of a home exercise program. This program emphasized back-extensor muscle strengthening and proper posture and is described below. Each patient was given written instructions and pictures outlining the exercise program in addition to verbal and visual instruction.
The WKO is a fitted harness with a weighted pouch suspended below the inferior angles of the scapulae over the midline spinous processes (Figure 1). For patients with kyphoscoliosis, the WKO was placed just off midline toward the convex side of the curve, as was possible, to address the scoliotic changes in addition to the hyperkyphosis. Patients were instructed to wear the WKO for 30 min twice daily until they could perform the exercises regularly and achieve continued pain relief. Depending on the patient’s body habitus, the weight of the pouch varied between 1.75 and 2.5 lb. The exercises included back-extensor muscle strengthening and chest, back, shoulder, and hip girdle stretching to optimize posture. Patients were instructed to perform 10 repetitions of each exercise twice daily in a seated position. A follow-up visit was encouraged, but it was not always possible as some patients lived outside the state of our institution. This exercise program was previously described by Sinaki et al.1,4
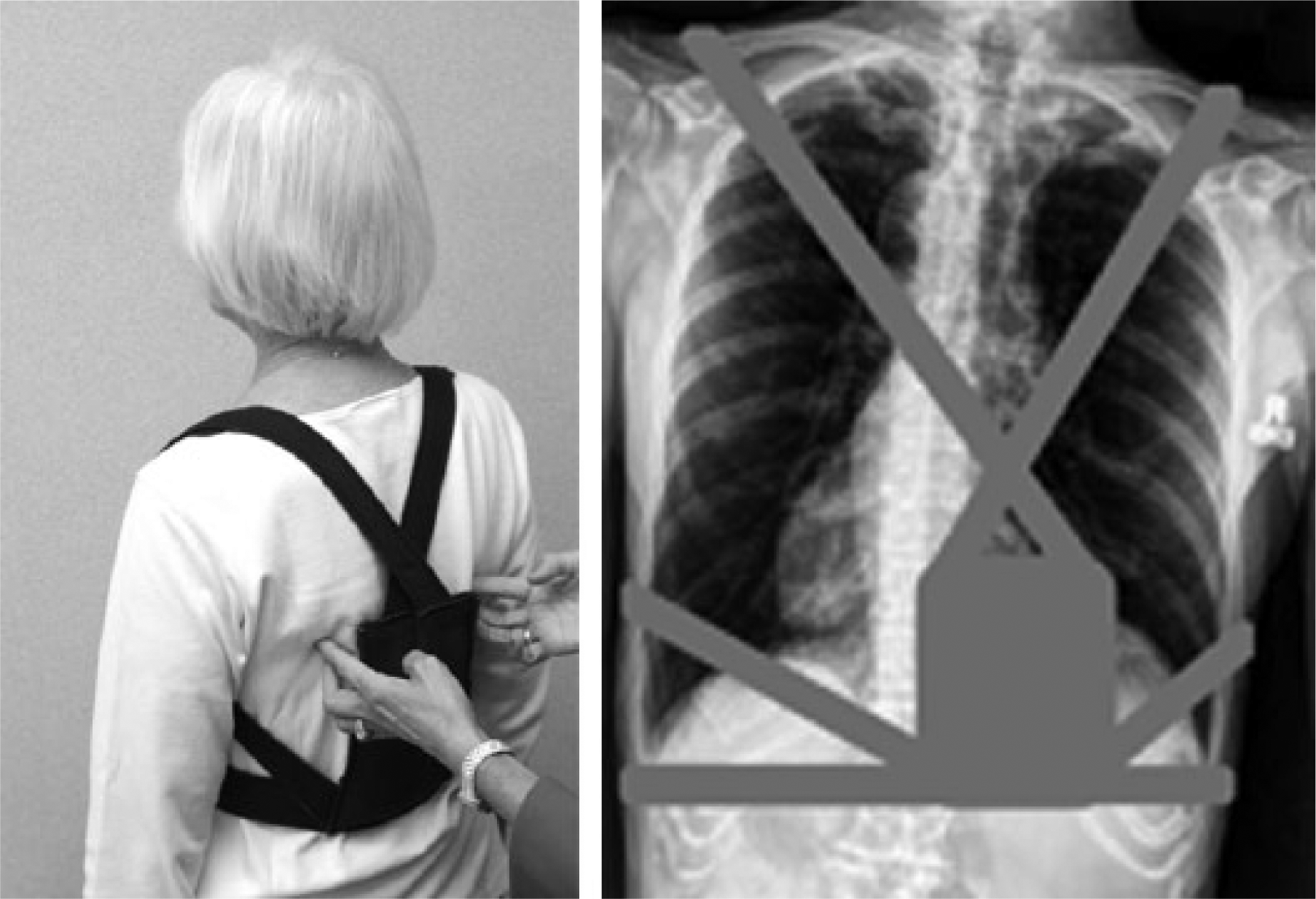
Left: Weighted kypho-orthosis positioning for kyphosis. Right: Thoracic radiograph demonstrating weighted kypho-orthosis positioning for thoracolumbar kyphoscoliosis. (Adapted from: Sinaki3)
The study was approved by the Mayo Clinic Institutional Review Board and performed in accordance with the approved protocol. All participants provided either written informed consent through the ROPE program or oral consent to the senior author during their initial medical evaluation for participation in the treatment program and publication, including publication of photographs and images of participants. They did not receive monetary compensation.
Findings and outcomes
Before their initial visit with the senior author, 10 women were diagnosed with osteopenia and 28 with osteoporosis. Patient ages ranged from 35 to 92 years (mean [standard deviation (SD)] = 74.5 [11.1] years). The youngest patient in the series was diagnosed with steroid-induced osteoporosis. The remaining 37 patients were assumed to have postmenopausal osteoporosis on the basis of their age. Height ranged from 138.8 to 188.2 cm (mean [SD] = 155.3 [10.0] cm). Weight ranged from 37.2 to 101.7 kg (mean [SD] = 61.0 [12.1] kg). All patients had thoracic hyperkyphosis and six patients had kyphoscoliosis. Most patients had failure of prior interventions, including back supports, analgesics, and other conservative pain-relieving measures such as application of heat and massage. During initial evaluations with the senior author, 20 patients had a primary complaint of unilateral flank pain and two reported bilateral flank pain. The remaining 16 patients complained of upper or lower back pain. After iliocostal impingement syndrome was diagnosed, all patients had a WKO trial resulting in clinically improved posture and immediate reduction of their primary pain symptom.
Nineteen patients returned for follow-up within 1 month to 2 years after initial evaluations, and all reported continued improvement of their primary pain symptom. Repeat thoracolumbar spine radiographs showed improvement in thoracic hyperkyphosis, defined as at least a few degree reduction in kyphosis, as compared with their initial radiographs (Figure 2). Fifteen months after achieving initial pain relief, one patient had recurrence of back pain after a fall. After she resumed WKO use and the home exercise program, her symptoms once again improved. Overall, patients who presented for follow-up reported regular use of their WKO and performance of their home exercise program. Of the 38 patients in the case series, 14 (37%) lived in Minnesota, the state of our tertiary-care center, and the remainder lived elsewhere in the United States or Canada.

Radiographic evidence of kyphosis before treatment (left) and 10 months after initiating treatment (right) with weighted kypho-orthosis and exercise program.
Discussion and conclusion
Iliocostal impingement syndrome is a rare, painful, and potentially disabling condition resulting from hyperkyphosis or kyphoscoliosis that occurs with severe spinal osteoporosis, trauma, or congenital deformities. To date, there is little published literature regarding diagnosis and management of iliocostal impingement syndrome. The studies available include individual case reports and small interventional studies, as summarized below.
To date, treatment of iliocostal impingement syndrome has included rib-compression belts, injections, and surgical resection of the lowermost ribs. The most conservative and mechanically based treatment includes the use of a 3-inch wide lower rib-compression belt. This is fitted directly above the iliac crests and adjusted tightly to provide adequate pressure on the lower ribs, shifting them away from the iliac crests. Injections have also been used under the assumption that the inserting tendons on the iliac crests or ribs are the primary pain generators. Hypertonic dextrose and lidocaine are injected at the osseotendinous junctions near the iliac crest and lower rib margins. 5 The most invasive procedure is surgical resection of the 11th or 12th rib.2,5
Hirschberg et al. 5 evaluated the pain-relieving effects of the rib-compression belt and injections in 19 patients with iliocostal impingement syndrome. After compression belt use for 3–6 weeks, 6 of 19 patients (32%) reported adequate pain relief. The remaining 13 patients underwent injection, resulting in pain relief for all but two patients over an unknown period. Of the two patients without relief following injection, one reported ongoing pain relief with use of the compression belt and one did not experience pain relief with either of the measures. Wynne et al. 2 described six patients with iliocostal impingement syndrome who underwent surgical resection of the outermost two-thirds of the 12th rib. All patients had pain relief without recurrence at 5- to 34-month follow-up.
Although these methods have been shown to provide pain relief, none have consistent long-term follow-up or aim to correct the underlying cause of poor posture, and reduced back strength. In contrast, our approach using the WKO in combination with the home exercise program targets the underlying treatable causes of malposture. Several orthotics have been designed with a similar goal in mind; however, we have had great success with use of the WKO. It is a simple orthotic that is easily donned and doffed by patients and can be worn inconspicuously underneath clothing.
Our study has several limitations. First, follow-up visits were not possible for all patients because of geographic limitations; thus, their available subsequent visits in our medical record were reviewed. Second, all patients included in this study experienced immediate pain reduction with the WKO trial; one could assume that they would likely continue to achieve pain relief with ongoing use. We did not include patients who did not experience initial pain relief with the WKO trial.
To our knowledge, this is the first case series describing diagnosis and treatment for iliocostal impingement syndrome with the goal of treating the underlying cause—hyperkyphosis or kyphoscoliosis. We are the first to describe, in detail, the treatment outcomes with the use of a WKO in combination with a home exercise program emphasizing back-extensor muscle strengthening and posture improvement. We have found that, after initial instruction, the program is convenient and easy to perform for our patients. This program has been shown to be successful for improving posture physical function, and immediate and long-term pain relief for our patients with iliocostal impingement syndrome.
Footnotes
Acknowledgements
Presented at the United Forum of the Americas, San José, Costa Rica, February 13–16, 2011. Portions of this manuscript have been published in Abstract form: Mayo Clin Proc 2005; 80(7): 849–855.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.