
Abstract
Background:
Elevated vacuum suspension systems use a pump to draw air from the socket with the intent of reducing bone–socket motion as compared to passive suction systems. However, it remains unknown if elevated vacuum suspension systems decrease limb displacement uniformly during transitions from unloaded to full–body–weight support.
Objectives:
To compare limb–socket motion between elevated vacuum and passive suction suspension sockets using a controlled loading paradigm.
Study design:
Comparative analysis.
Methods:
Persons with transtibial amputation were assessed while wearing either an elevated vacuum or passive suction suspension socket. Digital video fluoroscopy was used to measure axial bone–socket motion while the limb was loaded in 20% body-weight increments. An analysis of variance model was used to compare between suspension types.
Results:
Total axial displacement (0%–100% body weight) was significantly lower using the elevated vacuum (vacuum: 1.3 cm, passive suction: 1.8 cm; p < 0.0001). Total displacement decreased primarily due to decreased motion during initial loading (0%–20%; p < 0.0001). Other body-weight intervals were not significantly different between systems.
Conclusion:
Elevated vacuum suspension reduced axial limb–socket motion by maintaining position of the limb within the socket during unloaded conditions. Elevated vacuum provided no meaningful improvement in limb–socket motion past initial loading.
Clinical relevance
Excessive bone–socket motion contributes to poor residual limb health. Our results suggest elevated vacuum suspensions can reduce this axial displacement. Visual assessment of the images suggests that this occurs through the reduction or elimination of the air pocket between the liner and socket wall while the limb is unloaded.
Background
Properly functioning sockets are designed to distribute pressures created during ambulation to previously non-weight-bearing tissues and to keep the prosthesis affixed to the residual limb. 1 Many residual limb problems, such as skin ulceration and pain, are associated with poor fitting sockets.2,3 These problems often arise when axial limb–socket motion, or pistoning, exerts undesirable shear forces on the skin as the residual limb is repeatedly loaded and unloaded during ambulation. 4 Consequently, the ability for individuals with amputation to maintain limb health and a preferred level of activity may depend on optimizing socket fit and minimizing limb–socket motion.
A variety of methods are available to use in suspending a socket from the limb of an individual with a transtibial amputation. Previous research reported 0.5–3.6 cm of displacement with conventional methods such as patellar straps, sleeve suspension, liners with pin suspension, and seal-in liners.5–9 The majority of this displacement occurred during the initial loading of the limb instead of uniformly as load on the limb increased.5,9 Tucker et al. reported approximately 60% of the axial displacement occurred during the first 20% body weight (BW), and over 80% by 40% BW. 9 The results suggest minimizing displacement during the transitions from an unloaded to weight-bearing condition would significantly reduce total displacement of the limb within the prosthetic socket.
The use of a mechanical or electric pump to create an elevated vacuum (negative pressure relative to atmospheric pressure) at the residual limb liner and socket interface has been reported to reduce total limb displacement 0.5–0.7 cm compared to conventional suspension systems.6,10 Elevated vacuum has also provided other benefits to users including fewer residual limb skin problems, more stable limb volume, and improved step symmetry.10–15 These results suggest improved socket suspension could be maintained through the use of devices providing elevated vacuum. However, previous studies examining limb displacement have only presented comparisons of an unloaded condition to fixed static draw amounts or full weight-bearing conditions. An approach examining the effect of elevated vacuum on axial motion during progressive limb loads has not been reported. Therefore, the effects of elevated vacuum on axial limb motion during transitions from unloaded to weight-bearing, and across progressively higher amounts of loading remains unknown. Research is warranted to evaluate if elevated vacuum suspension systems decrease total axial limb displacement by limiting motion primarily during early weight-bearing, or more uniformly as full BW is loaded on the limb.
The purpose of the study was to evaluate the effect of elevated vacuum on axial limb–socket motion during incremental increases in weight bearing in persons with a transtibial amputation. We hypothesized elevated vacuum would have the greatest effect in decreasing limb–socket motion during initial loading of the limb.
Methods
Participants
Individuals with traumatic transtibial amputation(s) were recruited to participate in the study. In addition, the participants had to be between the ages of 18 and 45 years, able to walk without the use of an assistive device, and have normal range of motion in the hip and knee of the tested limb. This study was approved by the San Antonio Military Medical Center Institutional Review Board and all volunteers provided written, informed consent prior to participation.
Prosthetic setup
All participants used a modified total surface bearing socket that accommodated both passive suction and elevated vacuum suspension. The elevated vacuum within the socket was produced by either a mechanical (Harmony; Otto Bock, Minneapolis, MN) or electrical pump (LimbLogic; The Ohio Willow Wood Company, Mt Sterling, OH), and a neoprene vacuum sleeve extending proximal to the prosthetic liner to help maintain subatmospheric pressure in the socket. Switching between a passive suction and elevated vacuum was possible by powering on or off the electrical compressor or rendering the valve of the mechanical pump functional or inoperative. Alignment and all prosthetic components used in the study were provided to the participants as part of clinical care and remained identical between sessions.
Collection procedure
A cross-over design was utilized in which each participant was tested while using a passive suction and elevated vacuum suspension system. The intent was to randomize the testing order. However, a need to minimize disruption to the individual’s clinical care resulted in a non-randomized order for some participants. An acclimation period of approximately 3 weeks was provided prior to data collections with each suspension system.
During each data collection, participants repeatedly applied vertical loads of 0%, 20%, 40%, 60%, 80% and 100% BW through their prosthetic limb. Each repetition started with the limb in an unloaded position (0% BW). Bone–socket motion was assessed using digital video fluoroscopy, a method shown previously to be reliable in persons with amputation.16,17 Medial–lateral digital video fluoroscopy recordings (Dynamix Motion X-ray system; VF-Works Inc., Palm Harbor, FL) of the residual limb within the socket were collected from three trials at each of the six loading conditions. Each recording was 1 s in duration. Vertical loading of the residual limb was controlled via auditory feedback (Biofeed Trak; Motion Analysis, Santa Rosa, CA) and a real-time graphic representation of direction and magnitude of the ground reaction force vector. The feedback was generated using data obtained from a forceplate (AMTI, Inc., Watertown, MA) positioned under the prosthetic limb. For each trial, the participants were required to be within 5% of the desired vertical load with shear forces in any direction less than 5% of the total load. During processing, ground reaction force data were used to confirm the desired loading range was maintained.
Image processing
A representative single image was obtained from each 1 s digital video fluoroscopy recording. The shortest distance from the distal point of the tibia to the superior border of the pylon of the socket adapter (Figure 1) was measured using digital video analysis software (Image Pro+; Media Cybernetics, Silver Springs, MD). Distance values for the three trials at each BW load were averaged and changes in displacement between loading ranges were calculated. A radiopaque ruler secured to the participant’s socket was used to ensure consistent scaling of all image measurements.
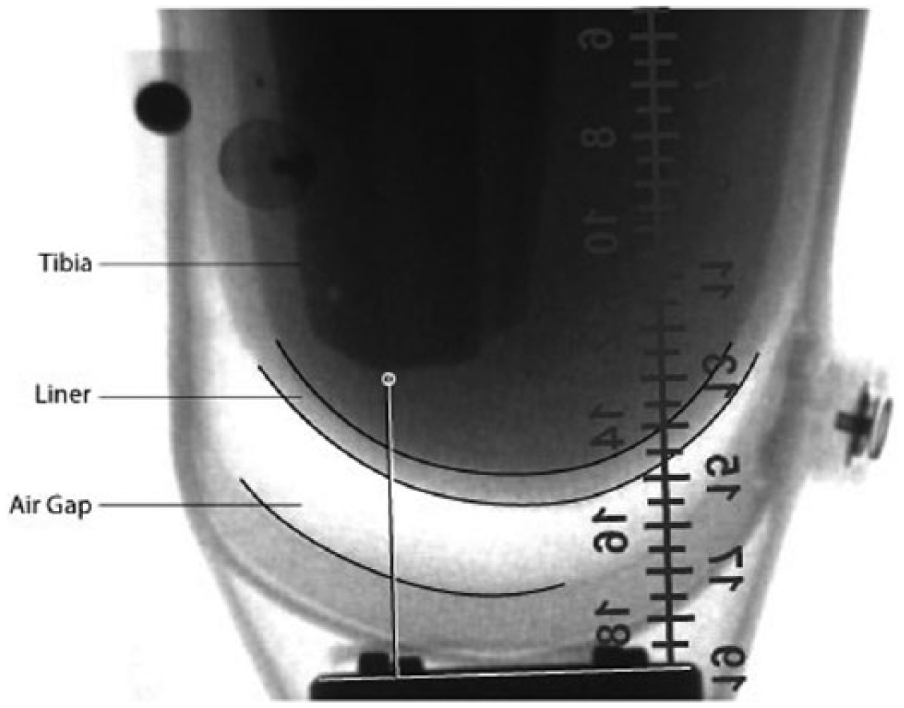
A sample medial–lateral video fluoroscopy image of a residual limb. The distal point of the tibia and superior border of the pylon socket adapter are highlighted. The displacement for a given weight condition was the measured perpendicular distance between the points.
Statistic analysis
All statistical analyses were performed using SAS v9 (SAS Institute Inc., Cary, NC). A two-factor analysis of variance (ANOVA) (suspension type, BW load, and the interaction of these variables) was used to model axial limb–socket displacement. The assumption of data normality was confirmed with a q–q plot. Significance was set at a p value less than 0.05 with a Bonferroni correction made for pairwise comparisons at each BW interval.
Results
In total, 10 male adults (mean age: 31 ± 6 years) with a traumatic transtibial amputation (6 unilateral, 4 bilateral) enrolled in the study and all participants successfully completed both testing sessions (Table 1). Eight of the enrollees wore a LimbLogic device and the remaining two wore the Harmony device. As previously noted, the order was not fully randomized. In total, 8 of the 10 participants were tested with the passive suspension method first and elevated vacuum second.
Participant demographics.
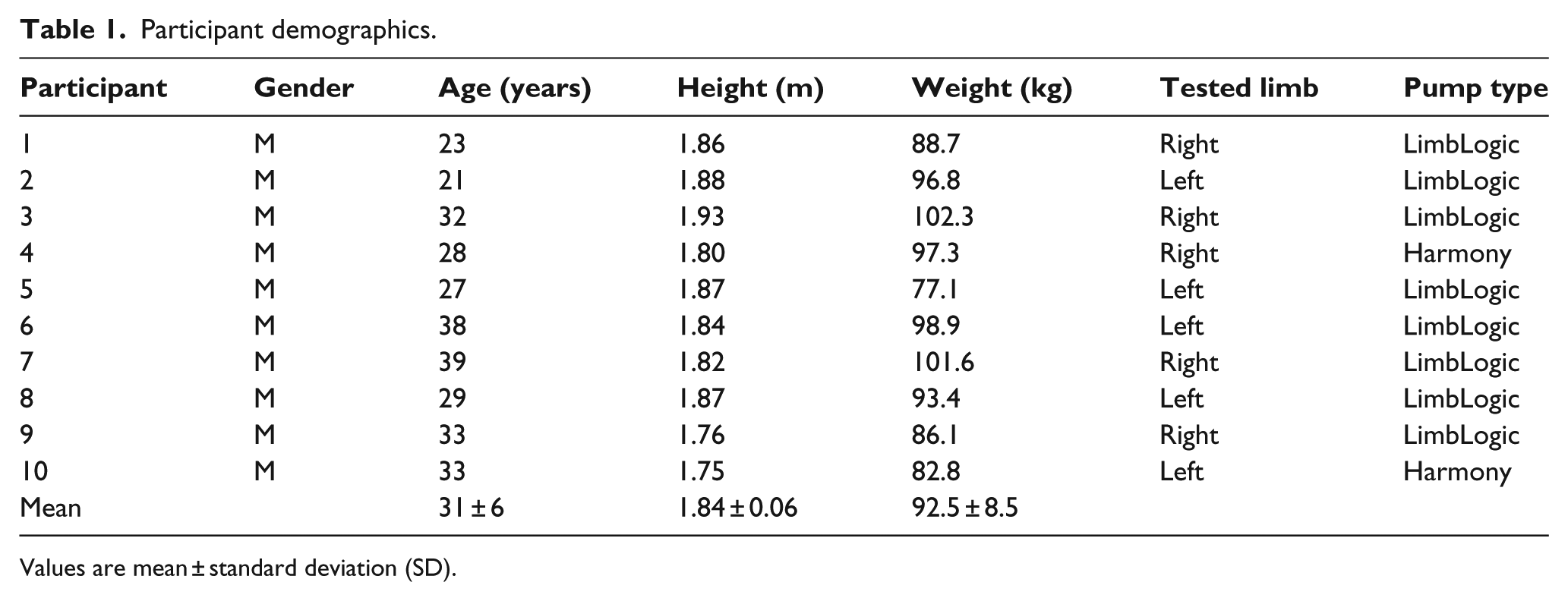
Values are mean ± standard deviation (SD).
A statistically significant interaction between socket condition and limb loading (p < 0.0001) was found as anticipated for the overall group level comparison of passive suction and elevated vacuum suspension systems. As such, planned comparisons were completed for each BW interval (Table 2).
Mean ± SD axial bone–socket displacement with each socket suspension system at BW increments between 0% (unloaded) and 100% (full-BW).
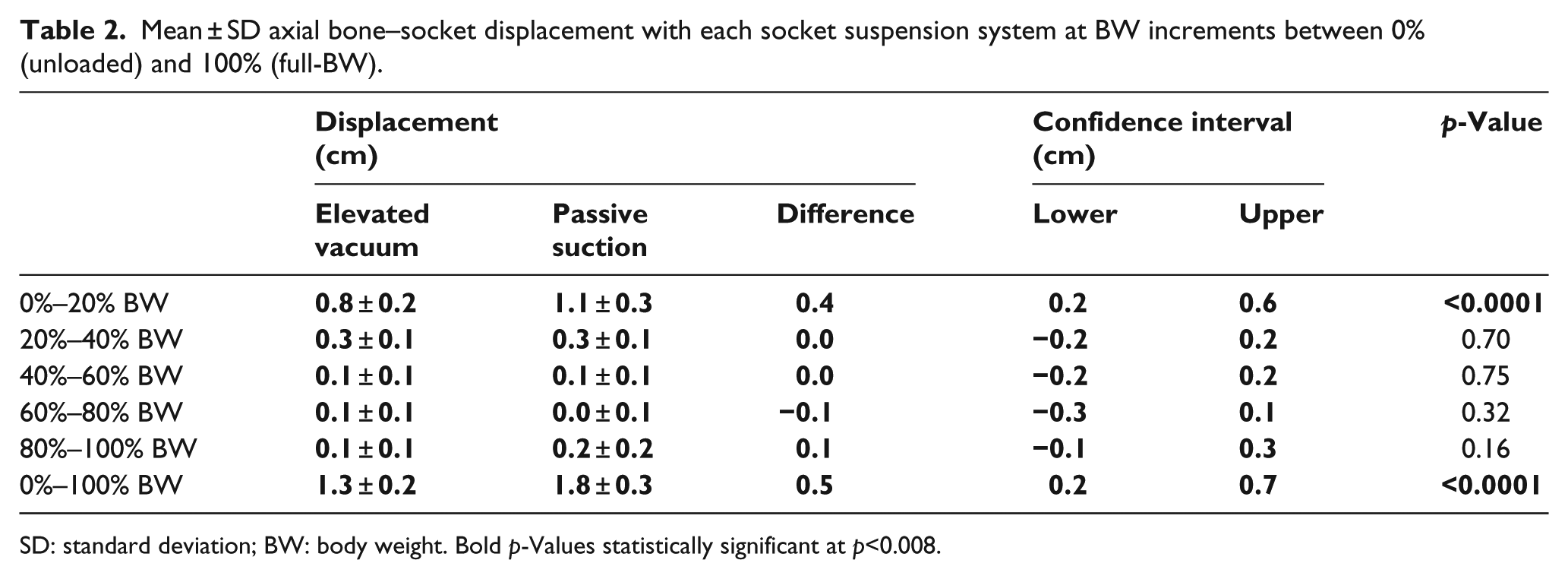
SD: standard deviation; BW: body weight. Bold p-Values statistically significant at p<0.008.
Participants experienced a total of 1.8 ± 0.3 cm displacement between 0% and 100% BW with passive suction and 1.3 ± 0.2 cm with elevated vacuum suspension (p < 0.0001). Of the total displacement, passive suction systems permitted 1.1 ± 0.3
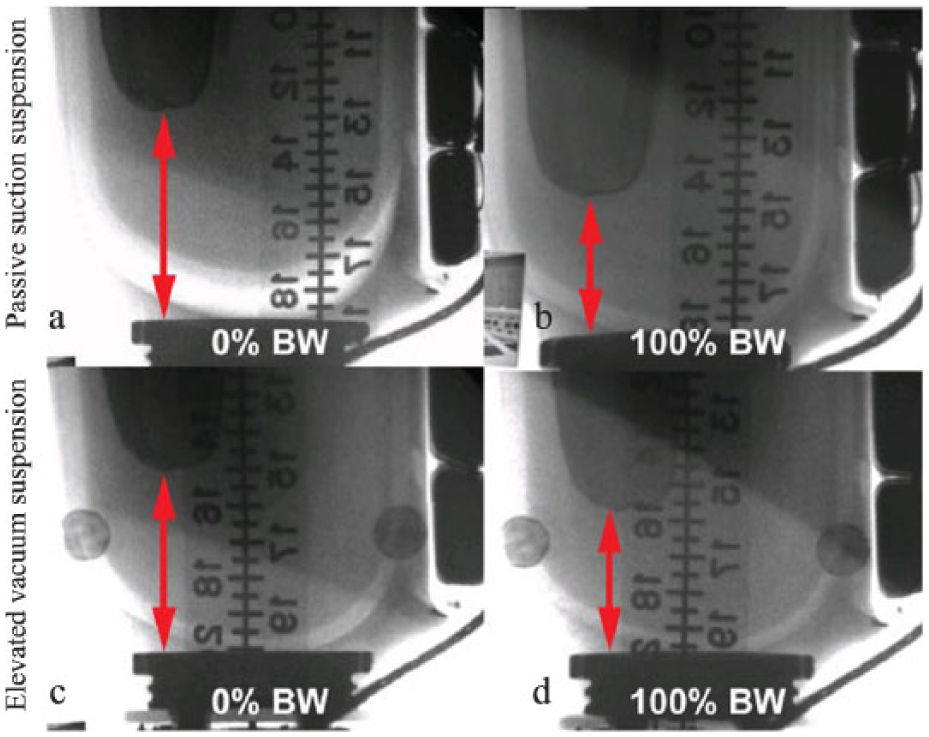
A side-by-side comparison of medial–lateral video fluoroscopy images of a residual limb. (a) and (b) Images show the axial displacement permitted by a passive suction suspension and (c) and (d) elevated vacuum when transition from unloaded to 100% body weight (BW). Note the formation of an air gap between the liner and the socket wall when using the passive suction suspension.
Discussion
In this study, digital video fluoroscopy was used to measure the tibia motion relative to the prosthetic socket for five increments of BW loading, ranging from unloaded to full BW. Our results indicate all participants experienced at least 1.3 cm of limb–socket motion regardless of the socket suspension. This finding agreed with the vertical displacements reported in other studies using radiographic based techniques,5,7,10,17,18 and highlights the ongoing limitations of current suspension techniques. Furthermore, we demonstrated elevated vacuum decreased the vertical displacement by 0.5 cm on average, similar to the 0.5–0.7 cm previously reported.6,10 However, further comparison is limited due to differences in experimental procedures. Board et al. measured bone–socket displacement due to distraction of the socket in a supine position, while we measured displacement for limb loading in a standing position. Klute et al. 6 indirectly assessed motion with limb loading using motion capture of markers attached to the socket and suspension sleeve to determine the vertical displacement.
The greater total displacement with passive suction likely resulted from the formation of a gap between the socket wall and the liner. Elevated vacuum suspension systems reduce the pressure in the space between liner and the socket. This increases the force required to separate the surfaces, effectively holding the liner to the socket wall. 10 In contrast, passive suction systems maintain a smaller pressure gradient between the liner and socket wall. The result can be, as our data suggest, a separation at the interface and an increase in axial displacement (Figure 2). Deformation of the liner material or soft tissue around underlying bony structure can also contribute to displacement of the limb within a prosthetic socket.5,10,19,20 However, these factors likely had no effect during this study as the same prosthetic liner was used by an individual for each test session.
Consistent with previous research, the majority of the vertical displacement occurred as the limb was loaded with BW simulating amounts expected early in stance phase of gait.5,17 Approximately 60% of the total vertical displacement occurred within the first 20% BW support through the prosthetic limb, and over 80% of the total displacement occurred by 40% BW. The pattern of limb displacement did not differ between the tested socket suspension systems. However, the elevated vacuum suspension did reduce displacement during initial loading of the prosthetic limb. In total, 75% of the total decrease in vertical displacement occurred by 20% BW. This result suggested elevated vacuum systems to reduce axial displacement primarily while the prosthetic limb was unloaded. It is unlikely elevated vacuum suspension systems provided additional meaningful improvement compared to passive suction systems after initial loading of the limb occurred.
The true clinical significance of the decrease in limb displacement is unknown. Nevertheless, an overall approximate 0.5 cm reduction in limb displacement has potential to help maintain skin integrity by decreasing motion of the limb and shear forces on the skin during daily activity. 10 This benefit may be particularly important for those prone to skin injury and those at higher risk for skin injury due to a cumulative volume of limb motion occurring during a physically active lifestyle.
Limitations
This study examined the benefits of elevated vacuum suspension only in comparison to passive suction. Although it is possible that our findings may not be generalizable to other suspension methods (i.e. pinlock), previous data from individuals using either pinlock or suction suspension demonstrate comparable displacement values. 9 One must also consider that most participants wore sockets which were recently fabricated as part of their standard clinical care. These sockets would be considered to have an ideal fit compared to sockets further along in their lifecycle. As a result, the sockets may have allowed less overall limb–socket motion diminishing the potential benefits of the elevated vacuum suspension system. Finally, as has been the case in previous research, a goal of the study was to approximate loading conditions experienced during the walking cycle. However, using digital video fluoroscopy during a walking trial was not technologically feasible. Forces and motions experienced within the socket during our test methods may not precisely match those experienced during walking. Furthermore, we did not evaluate other potential sources of motion within the socket, such as soft tissue elongation. 10 Future research should investigate other sources of motion within the socket, and seek novel surgical or prosthetic solutions to minimize movement at the limb–socket interface during transitions to and from an unloaded limb.
Conclusion
Maintaining residual limb position within the socket remains an important consideration with prosthetic design. The study results suggest elevated vacuum suspension improved socket fit by reducing axial limb–socket motion between non-weight-bearing and BW experienced during early stance phase of walking. However, there was no evidence elevated vacuum suspension systems differ from passive suction systems in reducing limb–socket motion past initial loading.
Footnotes
Acknowledgements
The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the US Army Medical Department, the US Army Office of the Surgeon General, the Department of the Army, Department of Defense, US Government, or the National Institutes of Health. The participants were enrolled in a study approved by the Institutional Review Board at Brooke Army Medical Center, Ft. Sam Houston, TX (C.2008.082).
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Military Amputee Research Program and by the Clinical and Translational Science Awards (CTSA) No. KL2TR000057 from the National Center for Advancing Translational Sciences.