
Abstract
A sand-casting technique for transtibial sockets was applied to 28 amputees in 2005. Although this meant an improvement in the quality of fitting as compared to historical reports with plaster of Paris casting, a total contact required three (two to five) stump socks. Continuing research leads the inventor, Dr Y. Wu, to replace the sand with micro polystyrene beads and simplify the equipment by eliminating the need for fluidization of silica sand by an air compressor during casting of the amputation stump. In a pilot series of 10 transtibial amputees, socket casting was performed with the new CIR casting technique and compared with the former sand-casting technique conducted by the same Category-I prosthetist. It was possible to obtain a good fit in eight out of 10 cases, which is an improvement from 19 out of 28 in the old series. Furthermore, there was a highly significant reduction in circumference measurements on the positive model with the new technique as compared to sand-casting.
Keywords
Introduction
In 2005 we published1 our positive experiences with the sand-casting technique2 developed at the Center for International Rehabilitation (CIR), Chicago, USA, by Dr Yeongchi Wu. We had our reservations, however, in as much as the fit was consistently and evenly larger than the amputation stump, but total contact could be achieved by applying three (2–5) one-ply wool stump socks. In the meantime Dr Wu and his group has worked on overcoming this problem and developed a system, which is simpler, faster and require less equipment,3 which we have now tested in a pilot series.
Patients and methods
The principal difference from the sand-casting system is that the original sand-container is replaced by a small light-weight casting-bag containing polystyrene beads, and an air compressor is no longer needed. However, a vacuum pump with a large surge tank is still required.
First the stump is covered with a thin nylon sheet and a thin plastic bag (40 × 80 cm, 0.5–0.75 mm thick) and the casting bag is rolled on to a level slightly above the trim line. A second plastic bag with a vacuum connector attached is applied onto the end of the casting bag and then pulled over the casting bag towards the knee. The second plastic bag is held down by a rubber band, and the first bag folded downwards to cover the second bag and secured with another rubber band distally to the former. At this time the vacuum pump is connected and air evacuated resulting in the casting bag becoming a solid negative mold of the amputation stump. By pulling and pushing on the socket comfort is checked and can even be checked for discomfort by allowing weight bearing on for instance a padded auto jack.
The negative mold is removed, but the vacuum suction maintained. A soft sponge of 1 cm is inserted onto the posterior wall to create an indentation in the popliteal area under vacuum, enhancing the build-up of the posterior trim line. The negative mold is filled with silica sand or round glass-beads normally used for road marking. A suction mandrel is inserted; a bottomless plastic cup placed on top of the sand and filled up with sand. The first plastic bag is then pulled over the bottomless cup and taped onto the mandrel to seal the sand inside the cavity of the negative mold. Vacuum is then applied to the mandrel to form the solid positive sand model. The vacuum suction is maintained through the mandrel, but released from the casting bag, which can then be removed.
The positive model can now be modified such as forming a PTB bar, a posterior trim line, or reliefs over sensitive areas (end of tibia, tibial crest, tibial tuberosity) by building up with water-based clay directly on the positive model. Another thin plastic bag is pulled over the model and taped to the suction mandrel. Eventually a nylon stocking is pulled over the model from the end to the plastic cup and an adaptor coupling plate for endoskeletal components mounted to the stump end with water-based clay.
The positive model is then ready for drape vacuum forming or bubble vacuum forming of the prosthetic socket. The prosthesis can then be finalized in the usual fashion including mounting of a foot, alignment and cosmesis.
A pilot-study on 10 transtibial amputees was performed casting sockets by both the original sand-casting method and the new CIR casting method; done by the same Category-I prosthetist.1 All subjects were given full informed consent and the opportunity to withdraw at any time without prejudice to care, and because the applied method is non-invasive and not in contact to natural orifices, circulation or central nervous system and full anonymity observed, the University for Labour and Social Affairs agreed that the study fulfilled the ethical requirements of the Helsinki declaration. There is no ethical clearance committee at the university.
An endoskeletal prosthesis was made for the CIR-Wu cast and followed for five months. All the amputees were subjected to the ISPO follow-up system.4 Further to that, the circumference of the positive cast was measured at the level of the posterior trim-line, and 4, 8, and 12 cm distally for each method of casting. The results were compared to historical data.1
Results
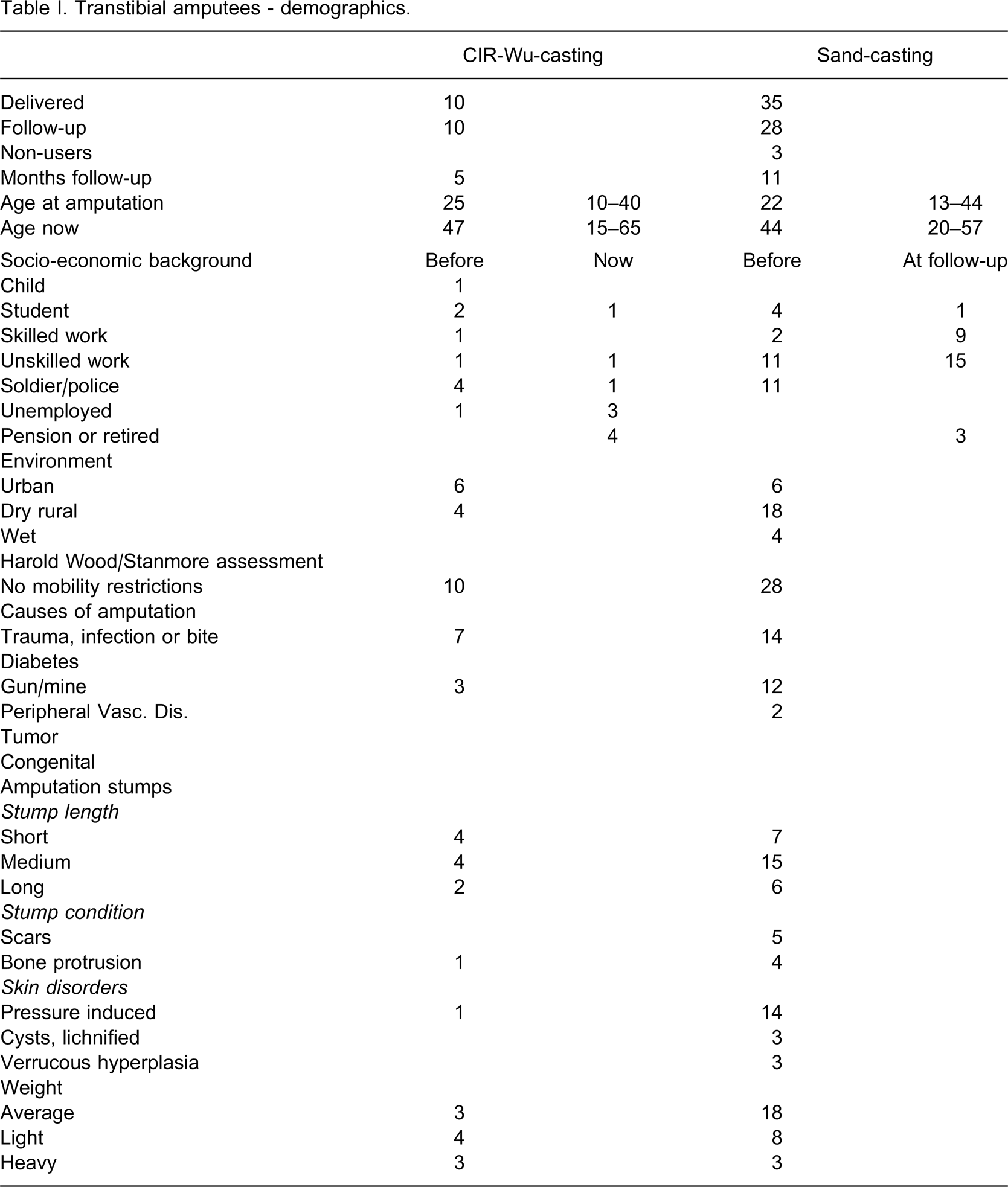
The demographics (Table I) of the pilot series and the historical series were different in as much as a higher proportion of the historical series were from rural areas and the vast majority was in work. However, none of the involved subjects had any mobility restrictions by the Harold Wood/Stanmore assessment and nearly all had sustained traumatic amputations. The stumps were all non-problematic.
Transtibial amputees - demographics.
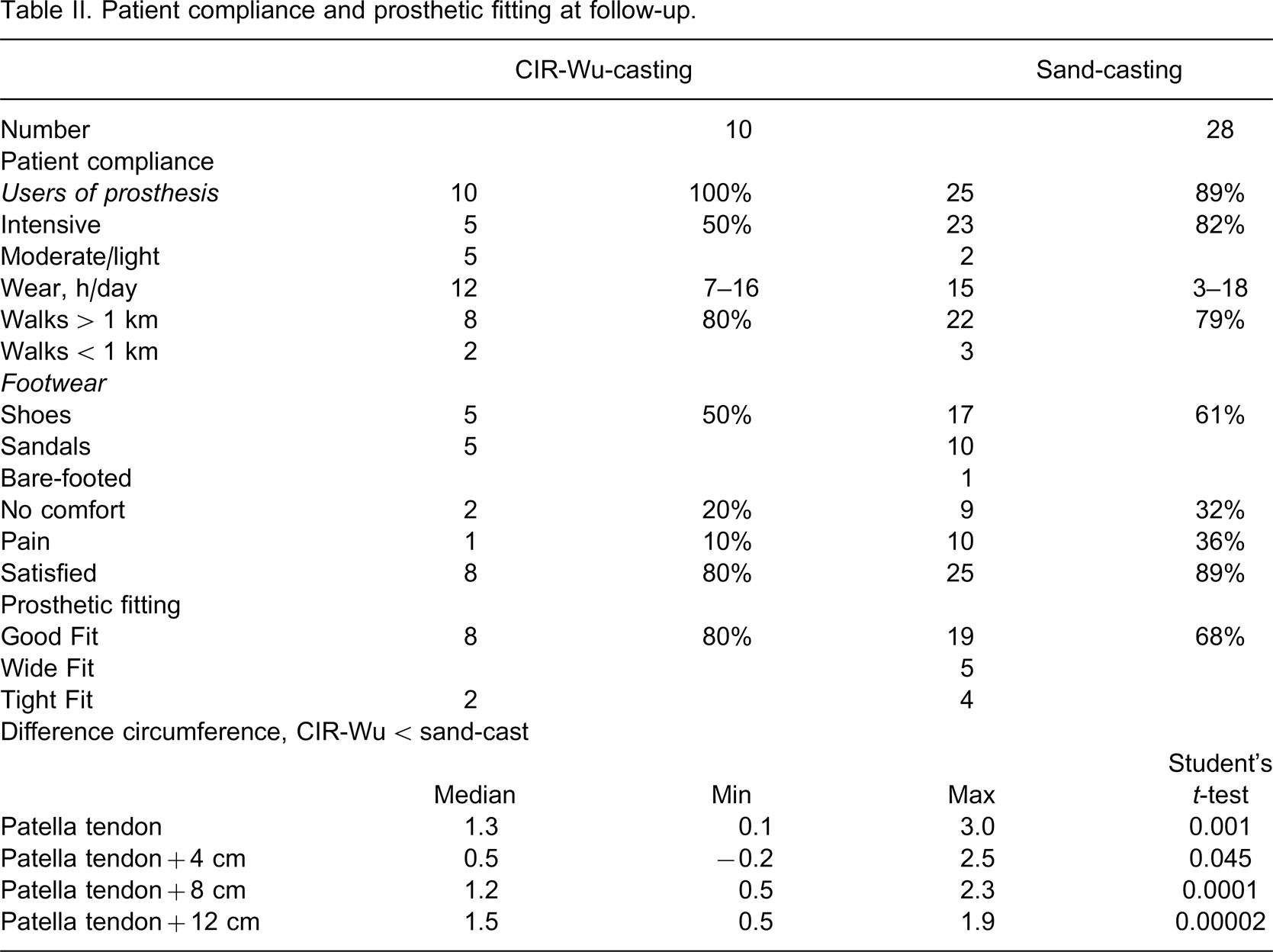
In respect of user compliance the prostheses were used slightly more intensively in the historical series with regard to walking distance and hours of daily use. However, most users walked more than 1 km. Although the satisfaction rate of 80% did not differ, it is clear that comfort complaints were less with the pilot group 20% vs. 32% and the prosthetic fits better, 80% vs. 68% with no wide fits. This was specifically reflected in the measures of circumference (Table II), that were significantly lower at all levels with the CIR casting system, and also that only one sock was required to obtain total contact as compared to three (2–5) with the old sand-casting system.
Patient compliance and prosthetic fitting at follow-up.
Discussion
The sand-casting method for socket fabrication1,2 never did come to a technical breakthrough in the developing world. It could be speculated that the demand of equipment and unreliable electrical power supply during the whole fabrication process were setting some limits, but also that the technique was not overly simple, and still required involvement of an educated and trained prosthetist.
However, a problem was recognized both in the Vietnam study1 and in clinical practice in India and in the hands of the inventor. This was in part attributed to the fact that granules inside a solid container become more compacted and reduces in volume when vacuum suction is applied, thus causing the mass of silica sand to move away from the stump. This resulted in a socket fit that was wider than full contact. Furthermore, build-up for pressure relief directly on the amputation stump, held in place by two layers of nylon sheath or stump socks, increased the cavity inside the formed negative mold and prevented total contact. However, unlike the heavy sand (specific gravity 1.64) that always sediment to the lower end of the object, the lightweight (specific gravity 0.16), micro polystyrene beads contained in a thin bag could be evenly distributed manually around a stump. This leads to a good fit with only narrow space between stump and socket, an advantage over traditional hand casting that is often subjected to wide sockets, in as many as 35% of cases.5
The present study has proved this to be correct, when performed by an educated prosthetist without laborious pre-testing training in the particular technology. The requirement of a sand container and an air compressor were eliminated. The sockets manufactured in this small pilot series only required one stump sock to achieve a total contact fit, meaning with the full stump end, no open-ended sockets. This can be difficult to obtain with plaster casting even in trained hands.
Footnotes
Acknowledgements
The study was sponsored by the Leahy War Victims Fund, United States Agency for International Development (grant no. HRN-G-00-00-00015-00). The opinions expressed in this paper are those of the authors and ISPO, and do not necessarily reflect the views of the USAID.