
Abstract
Background:
Ankle–foot orthoses could be utilized both with and without shoes. While several studies have shown that ankle–foot orthoses improve gait abilities in hemiplegic patients, it remains unclear whether they should be used with shoes or without.
Objectives:
The study purpose was to compare the effect of standard shoes and rocker shoes on functional mobility in post-stroke hemiplegic patients utilizing ankle–foot orthosis.
Study design:
Randomized clinical study.
Methods:
Thirty post-stroke hemiplegic patients participated in this study randomly assigned to two groups. Group I received standard shoes + ankle–foot orthosis and group II were provided with rocker shoes + ankle–foot orthosis. Their functional mobility and energy expenditure parameters including timed up and go, timed up stairs, timed down stairs, preferred walking speed, and oxygen (O2) cost (mL/kg/m) were measured.
Results:
In group I, no significant changes were seen in outcome measures after wearing standard shoes. While in group II, O2 cost and timed up and go time significantly decreased, and preferred walking speed increased when patients wore rocker shoes. Also, there was a significant difference between rocker shoes and standard shoes in improvement of timed up and go, preferred walking speed, and O2 cost.
Conclusion:
When patients using ankle–foot orthosis wore rocker shoes, their functional mobility improved and oxygen cost diminished. Also, rocker shoes was significantly more effective than standard shoes in improving functional mobility parameters.
Clinical relevance
This study suggests that in post-stroke hemiplegic patients using ankle–foot orthosis, wearing rocker shoes can lead to much more improved functional mobility and decreased energy expenditure compared to ankle–foot orthosis only. Thus, in stroke patients, the combination of ankle–foot orthosis-rocker shoes is recommended for both rehabilitation programs and ankle–foot orthosis efficacy investigations.
Background
Stroke is a major cause of death and disability worldwide.1–3 Hemiplegia secondary to stroke may lead to decreased mobility, 4 altered gait pattern,5,6 increased energy consumption,7,8 and un-coordinated movements. 9 Consequently, hemiplegic patients often face a lot of difficulties in their daily life activities. 10 Regaining the functional mobility is one of the most critical goals in rehabilitation of these patients. 11 Among different rehabilitation approaches, ankle–foot orthoses (AFOs) are widely prescribed to improve walking and functional mobility for patients with hemiplegia.8,12,13
Many studies have been conducted on the effect of AFOs on hemiplegic gait so far and most concluded that a suitable AFO could potentially improve function and increase gait velocity.7,14–17 Moreover, energy expenditure is reported to be an important factor which can potentially affect the activities of daily living in stroke survivors. Although due to decreased gait velocity the rate of oxygen consumption in stroke patients is similar to healthy subjects, it is generally believed that their oxygen cost per distance walked is considerably higher than able-bodied persons, which could be decreased using an AFO. 8
AFOs are usually utilized with shoes. 18 While several studies have shown that AFOs improve functional abilities in hemiplegic patients, it is still unclear that they are better to be used along with which type of shoes to have the most effect. On the other hand, normal function of the foot and ankle is described as three combined sequential rockers including heel rocker, ankle rocker, and forefoot rocker. Following hemiplegia, all three rockers are seriously damaged. 19 Previous studies conducted on the mechanism of the influence of AFOs have reported that AFOs improve heel and ankle rockers during walking; however, they did not seem to influence forefoot rocker in hemiplegic gait.10,18 Also, it was demonstrated that rocker bars in shoes could result in improving rollover function of the foot and consequently, facilitating weight progression and push off or transferring weight from one limb to another. That is, the curvature of the rocker shoes (RS) leads to a better rolling of the body over the ground and reduces the need for foot movement.19–21 Thus, it was hypothesized that wearing shoes with forefoot rocker modification while using AFO could improve walking ability and as a result functional mobility in hemiplegic patients.
The purpose of this study was to compare the effect of the standard shoes (SS) and RS on functional mobility and energy expenditure in patients with stroke utilizing AFO.
As the main objective of using various orthoses is to improve function and activities of daily living, 22 functional tests could be potentially useful indicators.23,24 On the other hand, functional tests, which are considered to be valid and reliable,23–28 seem to be cheap and easily accessible so that clinicians will easily be able to evaluate the short-term effectiveness of the prescribed orthoses, without the need for voluminous and costly equipments. Hence, in this study, functional tests along with measurement of oxygen consumption per meter were used to evaluate the efficacy of the SS and RS on functional mobility and energy cost in hemiplegic patients secondary to stroke utilizing AFO.
Methods
Participants
Considering the confidence level of 95% and power of 80%, 30 hemiplegic patients secondary to stroke (both men and women) were recruited for the purpose of this study. Patients were randomly assigned into two groups through block randomization method. Inclusion criteria were having the age between 40 and 70 years, the spasticity score of 3 according to Modified Ashworth scale, the ability to walk with or without assistive device, and suffering from stroke for a period of at least 6 months. Patients were excluded if they had deformity in their spine or lower limbs, any history of surgery in their spine and lower limbs, cardiovascular problems or were unable to perform the tasks. Table 1 demonstrates demographic characteristics of the participants.
Demographic characteristics of the patients (N = 30).

ROM: range of motion; DF: dorsi-flexion; M: male; F: female; L: left; R: right.
Interventions
A prefabricated solid ankle–foot orthosis (SAFO), which was made of polypropylene, was prepared for each patient. The foot and ankle were kept at 90° to the lower leg (neutral plantigrade position) using orthosis. A rough (anti-slipping) rubber was attached to the bottom of the SAFO foot-plate in order to prevent slipping in AFO-only condition. As the attached rubber was thin (only 3-mm thick), and exactly the same rubber was used at the bottom of the shoes, it did not seem to affect the obtained results. Also, in order to put the foot and ankle in a secured position, four straps were used to tightly hold ankle–foot complex in the orthosis. Each orthosis was selected and fitted to the patient’s limb by an expert orthotist.
Both SS and RS were custom fabricated (made of leather) based on anthropometric data obtained from the patients’ foot and ankle. They were high top (extended to lateral malleoli), in order to secure the AFO and foot properly, and had larger toe box to provide extra room for the AFO. At the sole of the SS and RS, ethylene vinyl acetate (EVA) rubber with standard hardness (shore-A 30–40) for midsole and a rough hard rubber (shore-A 50–60) were used. SS had almost flat footwear extended from heel to toe. In RS, rocker bar started at 65% of the full shoe length with respect to the posterior part of the heel with angle of 15°. The rest of the sole of the shoe was flat to provide maximum stability during standing and walking. As off-the-shelf RS are not usually high top and have heel-to-toe rockers which may potentially disturb hemiplegic patients’ balance during walking, in this study, custom-made shoes were preferred to be utilized.
Patients were randomly assigned into two groups using block style randomization scheme. Group I received SS and group II were given RS while all participants used SAFO and wore the same shoes (Figure 1).Patients in each group were examined with and without their shoes in random sequences. Figure 2 shows flow chart of the study.

Solid ankle–foot orthosis (SAFO).
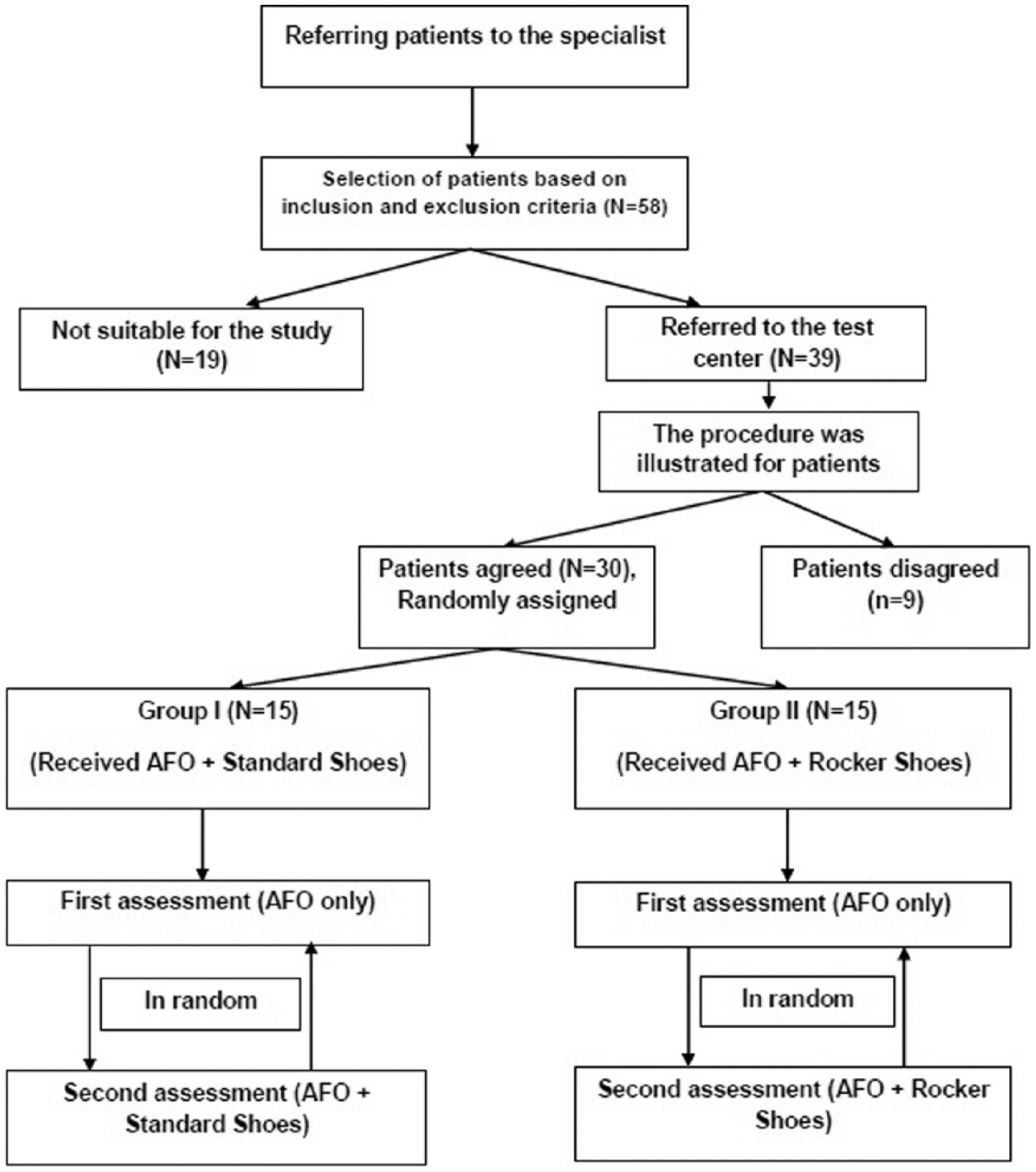
Flow chart of the study.
Outcome measures
Timed up and go (TUG) test. Patients were asked to stand up from a standard chair, walk for 3 m, turn, walk back to the chair and sit down again. The time of this task was recorded in seconds.
Timed up stairs (TUS) test. Patients were instructed to go up to 10 steps of a stair that is produced for this test. Stairs included 10 stairs totally with 16.5 cm high and 25 cm deep and 1 m wide with a rail on both sides. The total time of the task was recorded in seconds.
Timed down stairs (TDS) test. Patients were instructed to go down from the top to 10 steps, until they reached the land. The total time of the task was recorded in seconds.
Preferred walking speed (PWS). Patients were asked to walk 10 m in a straight line at self-selected speed. The time of the task was recorded in seconds and then divided to the distance (10 m).
Oxygen cost
Oxygen uptake (mL/kg/m) was measured in order to examine the effect of standard and RS on energy expenditure in post-stroke hemiplegic patients. The participants walked on a motorized treadmill at their self-selected speed,8,29 which had been determined and set before each test, and simultaneously, their oxygen cost was recorded by a breath-by-breath gas analyzer system (Cosmed Quark b2; Cosmed, Rome, Italy). It consisted of a facemask that covered mouth and nose that was tightened to the head. Participants were asked to walk for 5 min while the data of the last 3 min were recorded to be analyzed. The data of O2 consumption were measured when it reached to a stabilized (steady-state) condition. Five-minute rest in a sitting position was considered appropriate for each patient between the first and second measurements.
With regard to functional tests, at least three trials were performed for each patient, and the overall average of obtained data was used for final evaluation. Prior to each condition (AFO only, AFO + RS, and AFO + SS conditions), patients were given 5–10 min practice time to be acclimatized. Furthermore, in order to become familiar with the test procedures, all participants were asked to perform the tests at least one time before the measurements were taken.
The means and standard deviations were calculated for the performed tests. The study was approved by the local medical ethics committee at the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran and all participants signed a consent form before their participation in the study.
Data analyses
Kolmogorov–Smirnov test was used to assess the normality of the data. A paired t-test and an independent t-test were used to compare changes between wearing and not wearing SS and RS while using an AFO within each group and between two groups, respectively. The level of p < 0.05 was considered statistically significant. SPSS statistical software version 16.0 (SPSS Inc., Chicago, IL, USA) was utilized for data analysis.
Results
Table 2 gives information regarding functional mobility tests and oxygen cost recorded from participants of groups I and II while using AFO. In group I, although PWS, TUG, and oxygen cost demonstrated some improvements, no statistically significant changes were found in all outcome measures while patients wore SS (p > 0.05 in all instances). In group II, wearing RS led to significant reduction in the time of performing TUG (p < 0.05). PWS was also significantly increased after wearing RS (p < 0.05). Accordingly, oxygen cost significantly decreased when patients wore RS along with their AFO (p < 0.05). However, as for TUS and TDS, no significant differences were seen following wearing RS while utilizing AFO (p > 0.05).
Functional mobility and energy expenditure parameters of the participants in group I and group II using AFO (mean ± SD).
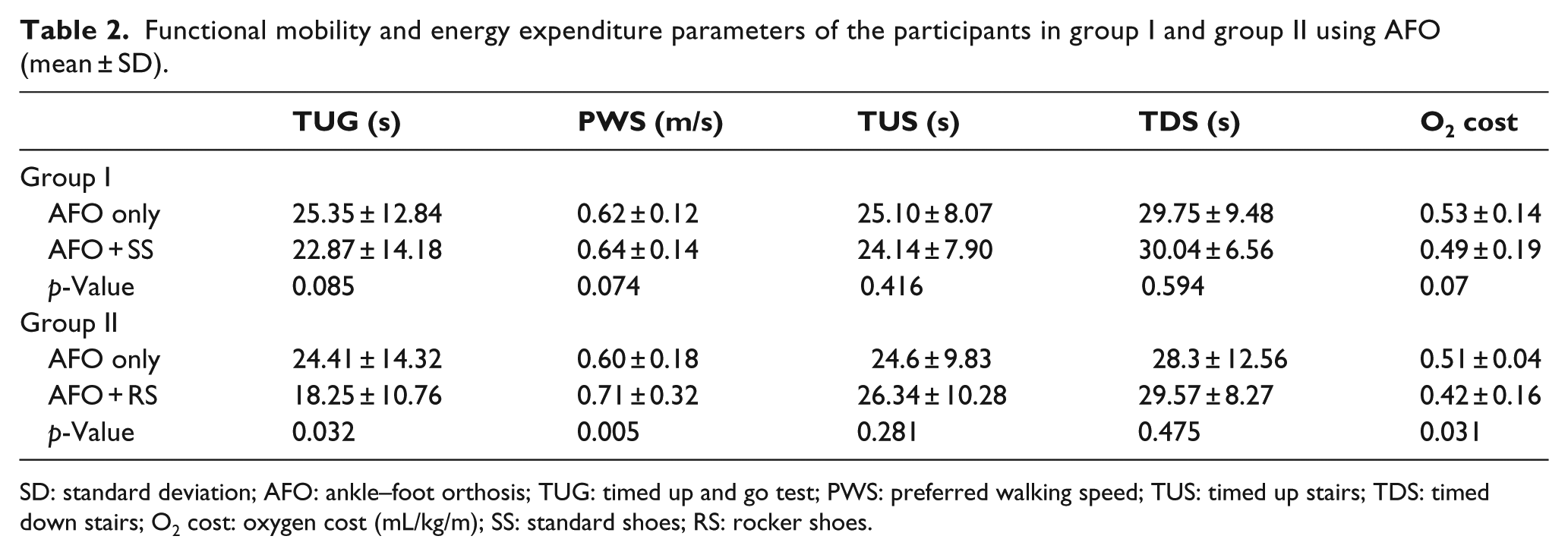
SD: standard deviation; AFO: ankle–foot orthosis; TUG: timed up and go test; PWS: preferred walking speed; TUS: timed up stairs; TDS: timed down stairs; O2 cost: oxygen cost (mL/kg/m); SS: standard shoes; RS: rocker shoes.
Table 3 provides data analysis on between-group changes. There was no significant difference in outcome measures between the two groups while using AFO only (p > 0.05). However, with RS, patients demonstrated significantly more PWS, less time of doing TUG, and less oxygen cost compared with wearing SS (p < 0.05 in all instances). No significant changes were seen regarding stairs tests (p > 0.05).
Comparison of the functional mobility and energy expenditure participants of the two groups (mean ± SD).
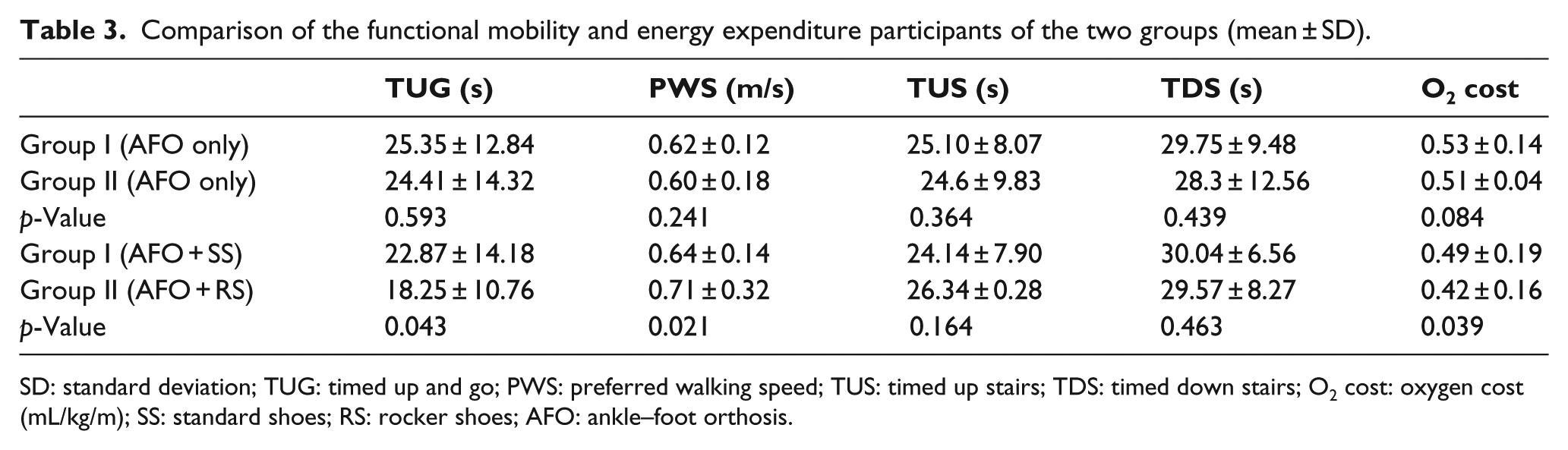
SD: standard deviation; TUG: timed up and go; PWS: preferred walking speed; TUS: timed up stairs; TDS: timed down stairs; O2 cost: oxygen cost (mL/kg/m); SS: standard shoes; RS: rocker shoes; AFO: ankle–foot orthosis.
Discussion
AFOs are commonly used by hemiplegic patients. 30 It is generally believed that AFOs improve functional mobility and increase walking velocity in patients with hemiplegia.16,17 AFOs are routinely utilized with shoes. 18 Nevertheless, limited data exist regarding the efficacy of different shoes on hemiplegic patients’ function while using AFO. Therefore, this study was designed to evaluate the effect of SS and RS on functional mobility and energy expenditure of the post-stroke hemiplegic patients.
According to the obtained data, SS with flat footwear resulted in no significant changes in functional mobility and energy cost in participants of group I. In a study conducted by Churchill et al., 31 it was concluded that shoes may improve some gait parameters in hemiplegic patients including stride-length, although other parameters such as gait velocity and cadence demonstrated no significant changes. The differences between the results of this study and those reported by Churchill et al. may be attributed to the interventions and group studied. Churchill et al. compared “shoes-only” condition with “shoes + AFO condition,” while in this study “AFO-only” condition was compared to “AFO + shoes” condition.
On the other hand, the findings of this study demonstrated a significant increase in PWS while patients wore RS. The results also indicated that the time of performing TUG was considerably reduced and oxygen cost was decreased while patients wore RS along with their AFO. It seems that these improvements may be attributed to the effect of rocker bars which were designed at the sole of the shoes. Many studies have been conducted on the effect of rocker soles on various gait characteristics.20,21,32–34 Generally, it was reported that rocker bars in addition to removing weight from special areas like metatarsal heads affect knee–ankle–foot function and, consequently, improve weight transferring and enhance anterior progressive forces during stance phase of gait.20,21,35 Arazpour et al. investigated the effect of rocker bar on gait characteristics in patients suffering from spinal cord injury. They modified the sole of the foot part of standard advanced reciprocating gait orthosis with cushion heels and forefoot rocker bars. They demonstrated that rocker bars have a positive effect on gait patterns including walking speed. 35 Accordingly, reduction in oxygen cost has most likely been due to improved gait pattern and the better and faster weight transferring from heel strike to toe off during stance phase of gait.
Various studies have demonstrated that any improvement in impaired gait pattern secondary to stroke may lead to diminished energy expenditure.8,29,36 The results of this study were consistent with previous research which reported that RS improves walking ability in healthy and neurologically disabled subjects.20,21,35
Moreover, the results of this study indicated that RS had no significant effect on the time of doing TUS and TDS. As the main effect of forefoot rocker bar is on push off and toe clearance at the late stance phase of the gait cycle, it seems that RS was not able to efficiently affect the time of going up and down stairs.
Between-group changes of this study showed that RS had significantly more positive effect on functional mobility outcome measures (except for stairs tests) and oxygen cost in hemiplegic patients in favor of RS compared with SS. These findings gave support to the previous research in which rocker bars contributed to faster weight progression and as a result better gait pattern.
One of the limitations of this study was that only the immediate effect of the interventions was assessed. Evaluation of the short-term and long-term efficacy of SS and RS in further studies is strongly suggested. Lack of kinetic and kinematic data was another limitation of this study. It is suggested that these outcome measures be included in future studies. Also, examining different kinds of RS along with using AFOs is recommended for further research.
Conclusion
This study revealed that if RS is utilized along with AFOs in post-stroke hemiplegic patients, further improvement in gait velocity and, consequently, performing TUG task as well as reduction in energy expenditure may be achieved. Finally, findings of this study can potentially provide hemiplegic patients who use AFO to walk and their care givers with valuable information regarding the effect of standard and RS on functional mobility and energy expenditure.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.