
Abstract
Background:
Ankle-foot orthoses are known to have a generally positive effect on gait in stroke, however the specifc type of AFO and the time point at which it is provided are highly variable in the currently available literature.
Objective:
The objective was to determine the immediate spatiotemporal and kinematic effect of custom-made solid ankle–foot orthoses in early stroke rehabilitation, compared to shod walking.
Methods:
Five male and three female participants were recruited to the study (n = 8), with a mean age of 57 (16) years who were 3.5 (3) weeks post-stroke. Each received a custom-made solid ankle–foot orthosis to a predefined set of design criteria and tuned using heel wedges to control the shank inclination angle during shod walking. Repeated spatiotemporal and three-dimensional gait measures were taken pre- and immediately post-intervention.
Study design:
A pre–post-test experimental study.
Results:
With the solid ankle–foot orthosis, walking velocity increased from 0.22 (0.2) to 0.36 (0.3) m/s (p < 0.05), overall average step length increased from 0.28 (0.1) to 0.37 (0.1) m (p < 0.05), cadence increased from 45 (19) to 56 (19) steps/min (p < 0.05) and step length symmetry ratio increased from 0.65 (0.2) to 0.74 (0.2) (not significant). No clear changes were observed in the joint kinematics of the hip and knee.
Conclusion:
In our small group of early stroke patients who were fitted with a solid ankle–foot orthosis, immediate significant improvements occurred in walking speed, step length and cadence, when compared to walking with shoes only.
Clinical relevance
This study provides evidence about the immediate effects of custom solid ankle–foot orthoses on gait of early stroke survivors. Ankle–foot orthosis design specifications are fully described for replication. This study suggests that observing global segment orientation may be more useful than joint angles when fitting and tuning ankle–foot orthoses for optimal ankle–foot orthosis/footwear alignment.
Background
It is widely acknowledged that stroke is the most common cause of severe adult disability in the United Kingdom, 1 with gait dysfunction being the most commonly reported post-stroke disability. 2 Gait dysfunction is highly significant for recovery from stroke, as those with low levels of ambulatory activity are more likely to suffer further health problems such as profound cardiovascular and metabolic deconditioning. 3
While quality of gait has been found to decline in the years following stroke, 4 one intervention that has proven successful in reducing that decline is the ankle–foot orthosis (AFO). 5 At a national level, in Scotland, a best practice statement (BPS) for the provision of AFO for stroke within the National Health Service (NHS) has been developed. 6 The BPS was developed by practitioners in a working group from the fields of orthotics, physiotherapy, stroke nursing and bioengineering, staff of NHS Quality Improvement Scotland and a patient representative. A systematic literature review was undertaken to evidence recommendations made. The BPS contains information on the principles behind the use of AFOs and their role in stroke rehabilitation, a referral screening tool and a fitting/review tool. 7
At an international level, several studies have been conducted on the effects of AFO use in stoke rehabilitation. Franceschini et al. 8 found increases in walking speed and cadence combined with decreases in stance time, double support time and reduced walking energy cost in patients who were a median of 39 months post-stroke (range: 2–244 months). Gok et al. 9 found that metallic and solid plastic AFOs provided an increase in walking speed, cadence and step length combined with a decrease in double support time and the authors concluded that the more rigid metallic AFO provided better outcomes than the plastic AFO tested. De Wit et al. found significant increases in walking speed, reduced time to complete timed up and go and stair ascent/descent tests. The study involved participants more than 6 months post-stroke who had already been using a rigid plastic AFO for at least 6 months. The authors found, however, that none of the improvements could be considered clinically significant. 10 Simons et al. 11 found that AFOs provided improvements in the Berg Balance Scale, timed up and go, walking speed and Functional Ambulatory Category. The use of Chignon articulated AFOs was compared with off-the-shelf AFOs, and it was concluded that the Chignon AFO provided a significantly higher level of immediate improvement in walking speed and selected kinematic parameters, and a larger reduction in spasticity measures over 90 days. 12
The studies mentioned above did not describe whether an AFO–footwear combination (AFO-FC) tuning process was used for the AFOs included in their methodology. Tuning the AFO-FC is the process of making fine adjustments to the design for biomechanical optimisation. 13 Typically, these fine adjustments include the use of rocker soles and the iterative addition of heel wedges. While a recent review outlined the potential utility of AFO-FC tuning in children with cerebral palsy, 14 the only study that mentions post-stroke AFO-FC tuning is a case study where the kinetic and kinematic changes were detailed, and knee hyperextension was successfully eliminated. 15
Published algorithms for AFO tuning suggest that with >5° thigh inclination during the mid-to-late stance (MTLS) phase, and a shank-to-vertical angle (SVA) of 10°–12°, combined with adequate control of the knee, it is possible to achieve a ground reaction force (GRF) alignment which successfully passes anterior to the knee joint centre, and posterior to the hip joint centre. 16 Without correct segment orientation at this phase of the gait cycle, GRF alignment cannot be correct, and therefore, the correct signals cannot be sent from the hip proprioceptors to the central pattern generators, which are thought to use that signal as one of the inputs for swing phase initiation.17,18 The AFO can be used to directly control the SVA at mid-stance, which if correct should increase the likelihood of achieving correct segment orientation during the MTLS phase.
Leung and Moseley 19 reviewed AFO literature, and while they found that AFO use may lead to immediate kinematic and spatiotemporal improvements in gait, they also stated that issues surrounding impact on daily functionality, clinical implications for the wider population, long-term effects and compliance have not been resolved.
Given the general consensus from the studies described above (i.e. that there are numerous positive effects from AFO use in stroke), it is surprising that the grade of recommendation in the recently published Scottish Intercollegiate Guidelines Network (SIGN) 20 clinical guidelines remains low. While the reported positive effects of AFOs are plentiful, one problem is that none of these studies can be considered directly relevant to the stroke AFO service provided in many parts of the United Kingdom. An example of how these studies may not be applicable on a local level is that in NHS Greater Glasgow and Clyde, many in-patients are prescribed and receive an AFO as early as possible (1–8 weeks post-stroke) in agreement with recommendations on early mobilisation21,22 and the finding that AFOs provide more benefit earlier in the rehabilitation process. 23 Of the studies cited above, Gok et al. 9 studied the group with the earliest mean time since stroke at 9.5 weeks (range: 1–38 weeks), whereas the others studied groups at a much later stage.8,10–12 Furthermore, the AFO studies cited above also often refer to the use of varied types of AFO which, although available to the local NHS stroke AFO service orthotists and patients, are prescribed to a lesser extent than solid AFOs, so their findings are not necessarily applicable. It was thought that a useful addition to the existing body of work would be a description of the instantaneous effects of appropriately tuned AFOs at the point of provision with people at an early stage in their stroke rehabilitation.
The aim of this study was to investigate the immediate spatiotemporal and kinematic effects of fitting and tuning solid AFOs on walking with patients who had suffered a recent hemiplegia, compared to their walking with no AFO. The AFOs provided were similar to those provided as standard within the local clinical service.
Methods
Participants
Five males and three females (Table 1) were recruited as part of an ongoing randomised controlled trial investigating the effectiveness of using biomechanical data to fit and tune AFOs. 24 Participants in this study had to be within 1–12 months after stroke, over 16 years of age, meet the criteria for AFO referral as outlined in the NHS BPS (able to walk with assistance but had difficulty flexing knee and extending hip during gait), assessed by a participating NHS orthotist and judged suitable for a custom solid AFO. Participants had a mean age of 57 (16) years and were 3.5 (3) weeks post-stroke.
Participant characteristics at baseline.
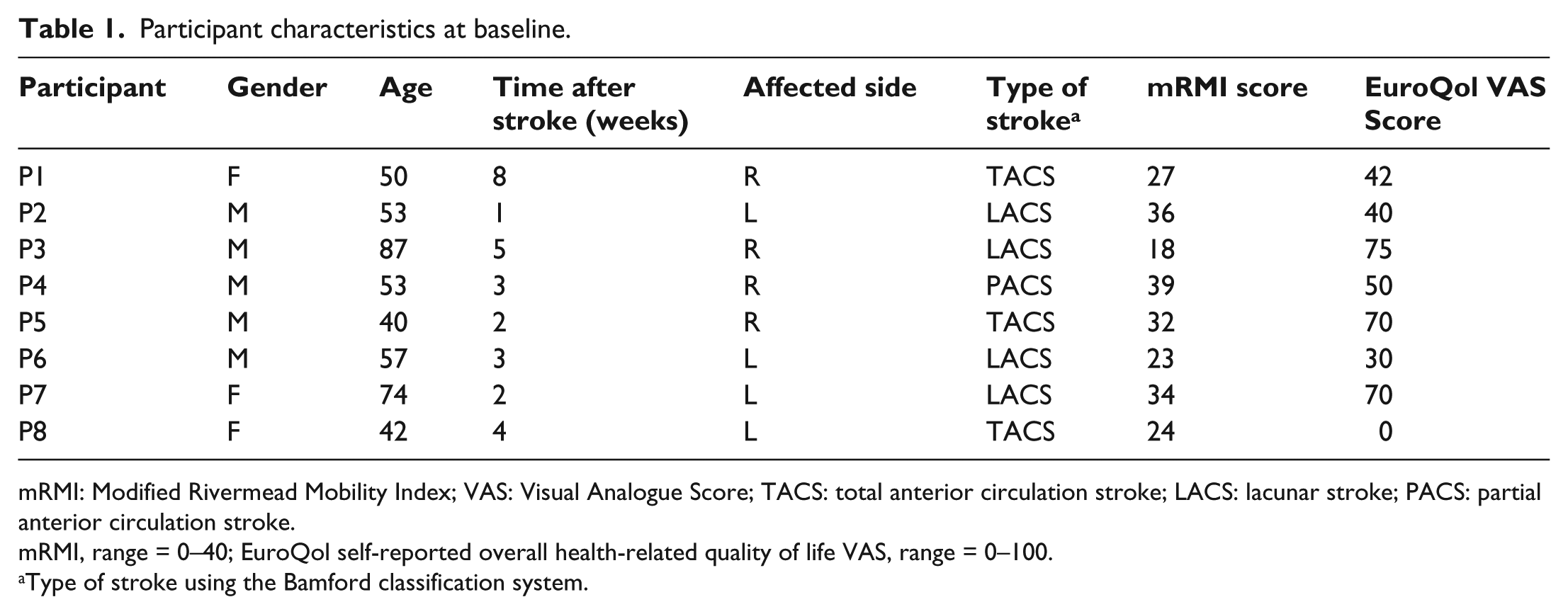
mRMI: Modified Rivermead Mobility Index; VAS: Visual Analogue Score; TACS: total anterior circulation stroke; LACS: lacunar stroke; PACS: partial anterior circulation stroke.
mRMI, range = 0–40; EuroQol self-reported overall health-related quality of life VAS, range = 0–100.
Type of stroke using the Bamford classification system.
AFO design and fabrication
All participants received a custom solid AFO (Figure 1) designed and fabricated by the participating NHS orthotists using the following design criteria:
The AFO must not position the ankle in a more dorsiflexed position than can be achieved with the knee fully extended (i.e. the gastrocnemius length). This means the AFO may in some circumstances hold the ankle in a plantar flexed position.
The AFO should give an initial SVA of 0° when placed on a flat surface without a shoe. A permanent wedge should be attached to achieve this if the AFO holds the ankle in a plantar flexed position.
5 mm homopolymer polypropylene should be used.
Carbon fibre reinforcements should be used, with their leading edge placed at the midline of each malleolus.
There should be no noticeable deflection when the AFO is forced into plantarflexion or dorsiflexion. There should be no outward bulging at the malleoli when the AFO is forced into dorsiflexion.
Trimlines should be approximately 10 mm anterior to the midline of the malleoli. At the forefoot, the medial and lateral trimlines should be close to the metatarsal heads, to allow for control of supination/pronation and forefoot adduction/abduction. The sole plate should extend at least 5 mm beyond the toes.
Straps should be made of Velcro™ (or webbing backed with Velcro™). The top strap should be no more than 10–15 mm from the top of the AFO. The lower strap should apply a force in a posterior and inferior direction, at roughly 45° to the vertical, to the dorsum of the foot.

Custom-made rigid AFO as specified by study design criteria.
Three-dimensional gait analysis
In order to implement a pre–post-test experimental design, three-dimensional (3D) gait analysis measures were taken on two occasions: one before the AFO was fitted walking with shoes only (baseline session), and another 7 days later immediately after the AFO was fitted and tuned (tuning session). During the tuning session, the AFO was fitted by one of two practising NHS orthotists, and heel wedges were added such that a suitable SVA (thought to be 10°–12°) at mid-stance 16 was judged to have been achieved. Rocker soles were not used.
The 3D gait analysis was conducted using an 8-camera Vicon 612 system (Oxford Metrics, UK) in conjunction with two AMTI BP400600 force platforms. Participants had a total of 34 reflective markers (18 single markers and 4 rigid clusters, each comprising 4 markers) attached to key anatomical landmarks. Single markers were placed on the pelvis (left and right anterior superior iliac spine (ASIS) and posterior superior iliac spine (PSIS)), the knees (medial and lateral epicondyles), the ankles (medial and lateral malleoli) and the feet (calcaneus, first and fifth metatarsal heads). Rigid clusters of four asymmetrical markers were attached to thigh and shank segments such that the eight single knee and ankle markers could be removed after a static calibration was captured, and these were reconstructed using the rigid clusters during subsequent walking trials.
All gait trials were conducted in a shod condition with feet markers attached to the outside of the shoe. Patients walked in outdoor shoes of their choosing during the baseline session, and all were given a pair of basic training shoes for the AFO fitting and tuning session. These shoes had a fairly rigid sole, a small heel-to-toe differential (9 mm) and three Velcro™ straps which allowed for easy insertion/removal of the AFO and heel wedges.
Post-capture processing was carried out on the data collected using code which derived the hip joint centres from the pelvic markers 25 and calculated 3D hip, knee and ankle joint angles using the joint coordinate system described by Cole et al. 26
Outcome measures
Spatiotemporal parameters of walking velocity, step length symmetry ratio (longest step divided by shortest step), overall average step length and cadence were calculated using the 3D motion analysis data. Average walking velocity was calculated using the differential of the displacement of the midpoint of the left and right ASIS markers on the pelvis with respect to the global horizontal direction of travel.
Both the SVA and the thigh-to-vertical angle (TVA) of the affected limb were calculated from the 3D motion data using 3D global segment orientations. An Euler angle sequence of ‘tilt–obliquity–rotation’ was used to describe the segment relative to the laboratory, whereby the tilt component represented the forward/backward inclination of the segment. The convention used was forward inclination of the segment with respect to the participant’s direction of travel and was taken to be positive. A spatial definition of mid-stance was used and was taken as the point at which the ankle joint centres were level in the horizontal direction of travel. TVAmax of the affected limb was taken at its point of maximum inclination, which usually occurred during the MTLS phase, which is described as the time between mid-stance and prior to toe-off. Knee flexion for the affected limb was taken at the same time point as TVAmax, with normal values at this point of the gait cycle being 10°–18° flexion. 27 Additional baseline measures such as the modified Rivermead Mobility Index (mRMI) 28 and the EuroQol EQ-5D-5L 29 quality of life questionnaire were also taken. Walking velocity was considered as the primary outcome measure as walking velocity gains have been shown to contribute to a higher class of ambulation category and result in increased function and quality of life. 30
Ethical approval
This study was granted ethical approval by the NHS West of Scotland Research Ethics Committee (Ref: 11/AL/0166) and the University of Strathclyde Research Ethics Committee. All participants were asked for their informed consent prior to inclusion in the study.
Statistical analysis
A non-parametric Wilcoxon Signed-Rank test was used to test for significant differences before and after AFO fitting and tuning.
Results
The mean number of gait cycles captured for each participant was 10 at baseline and 7 immediately post-AFO tuning. There were a number of changes in the spatiotemporal parameters measured between baseline and immediately after the AFO had been fitted and tuned, as shown in Table 2. All but one participant (P7) showed an increase in their walking speed. The walking speed increase across all participants was statistically significant (p = 0.021). Only one participant (P8) did not show an increase in step length symmetry, although the increases across all other participants were not statistically significant (p = 0.082). All participants had a longer step length with their paretic limb compared with their non-paretic limb, although two did not always consistently follow this pattern through all gait trials (P2 and P5). All but one participant (P7) showed an increase in overall average step length. The overall step length increase across all participants was statistically significant (p = 0.021), as was the increase in cadence (p = 0.042).
Changes in spatiotemporal parameters pre and immediately post-AFO fitting and tuning.
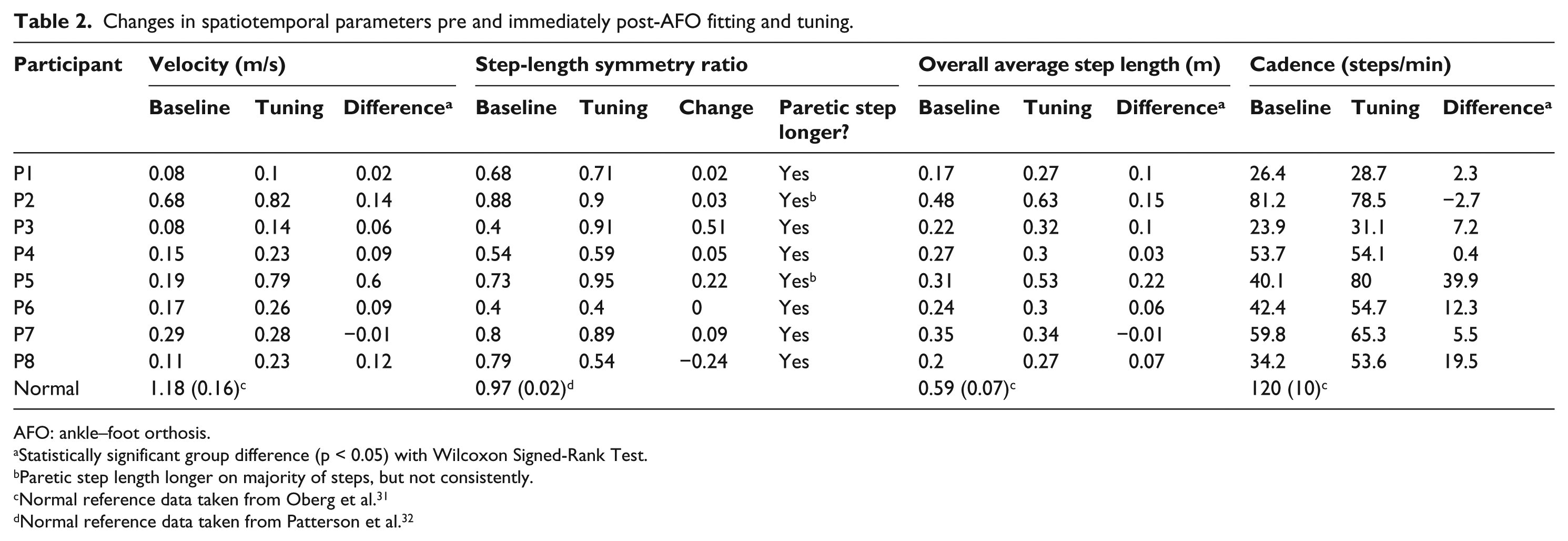
AFO: ankle–foot orthosis.
Statistically significant group difference (p < 0.05) with Wilcoxon Signed-Rank Test.
Paretic step length longer on majority of steps, but not consistently.
Normal reference data taken from Oberg et al. 31
Normal reference data taken from Patterson et al. 32
For the majority of participants, affected limb segment orientation kinematics moved closer to predefined target values (i.e. SVA = 10°–12° inclination, TVAmax > 5° inclination) as shown in Table 3, although none of these differences were statistically significant. SVA changes towards the target values were apparent in most participants, except for P3 who changed from 11.3° (6.7°) to 6.3° (6.2°), and P6 who moved marginally outside the target range from 10.4° (1.9°) to 12.4° (1.1°). Small TVAmax changes towards target values were observed in four participants: P1, P2, P5 and P7, with a large change observed in P3 (−7.7° (7.2°) to 10.3° (3.6°)). A reduction in the TVAmax for P6 was observed from −4° (2.4°) to −8.4° (2.5°), as was the case for P4 (4.9° (4.6°) to −3.8° (5.8°)).
Changes in segment kinematic parameters pre and immediately post-AFO fitting and tuning, shown as mean (SD).
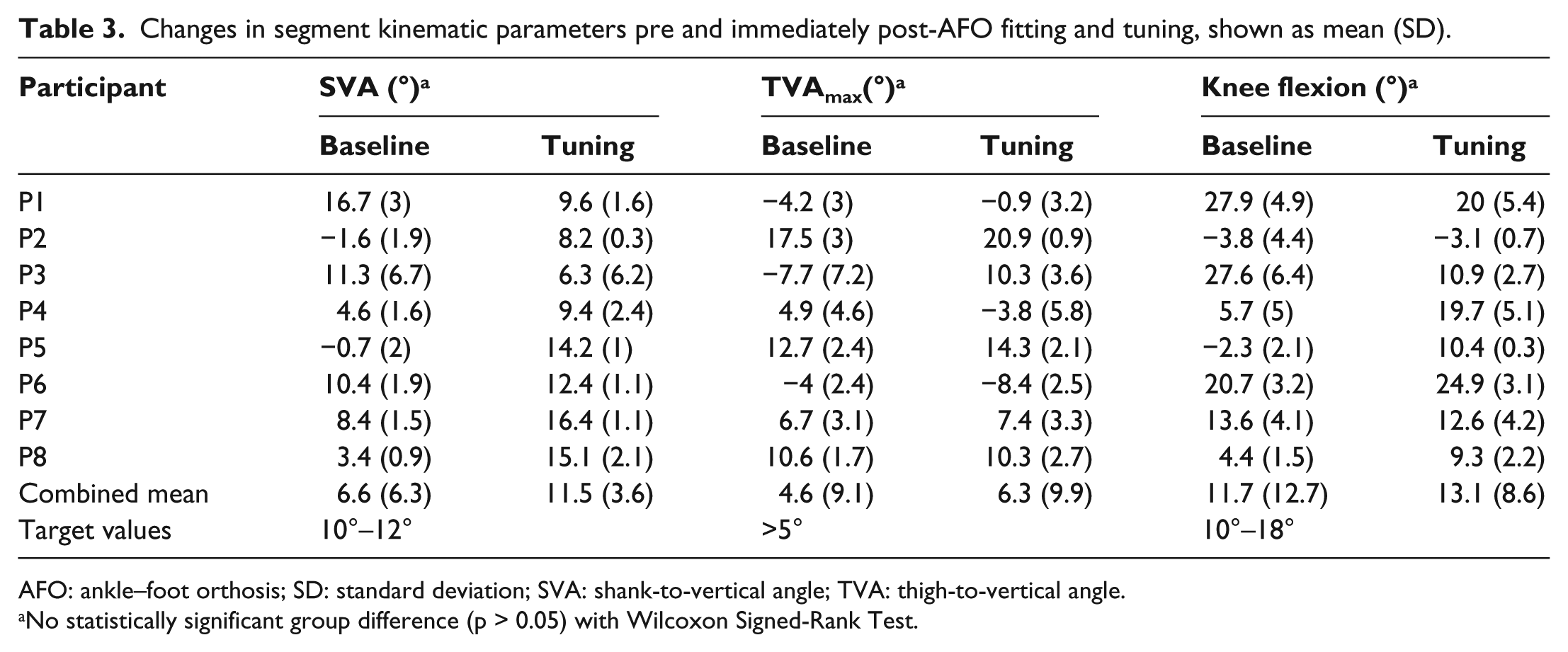
AFO: ankle–foot orthosis; SD: standard deviation; SVA: shank-to-vertical angle; TVA: thigh-to-vertical angle.
No statistically significant group difference (p > 0.05) with Wilcoxon Signed-Rank Test.
Knee flexion angles were changed for P5, with knee hyperextension eliminated (−2.3° (2.1°) to 10.4° (0.3°)). Knee hyperextension was marginally reduced in P2 (−3.8° (4.4°) to −3.1° (0.7°)). In addition to reducing hyperextension in some participants, in others, the tuned AFO reduced excessive knee flexion in P1 (27.9° (4.9°) to 20° (5.4°)) and P3 (27.6° (6.4°) to 10.9° (2.7°)). The tuned AFO changed knee flexion angles such that they deviated further from normal ranges (10°–18° flexion) in two participants, with P4 experiencing a knee flexion increase from 5.7° (5°) to 19.7° (5.1°) and P6 experiencing an increase from 20.7° (3.2°) to 24.9° (3.1°).
Sagittal knee and hip joint angles throughout the gait cycle at baseline and post-tuning are shown in Figure 2 for all participants. All participants (with the exception of P2 and P4) exhibited excessive amounts of knee flexion at initial contact during baseline sessions (see knee profiles in Figure 2: P1, P3, P5, P6, P7 and P8). Few participants achieved any hip extension at baseline (see hip profiles in Figure 2), and the AFO appeared to have an immediate positive effect on hip extension for P3 and P8, with no positive effect on the other six participants.
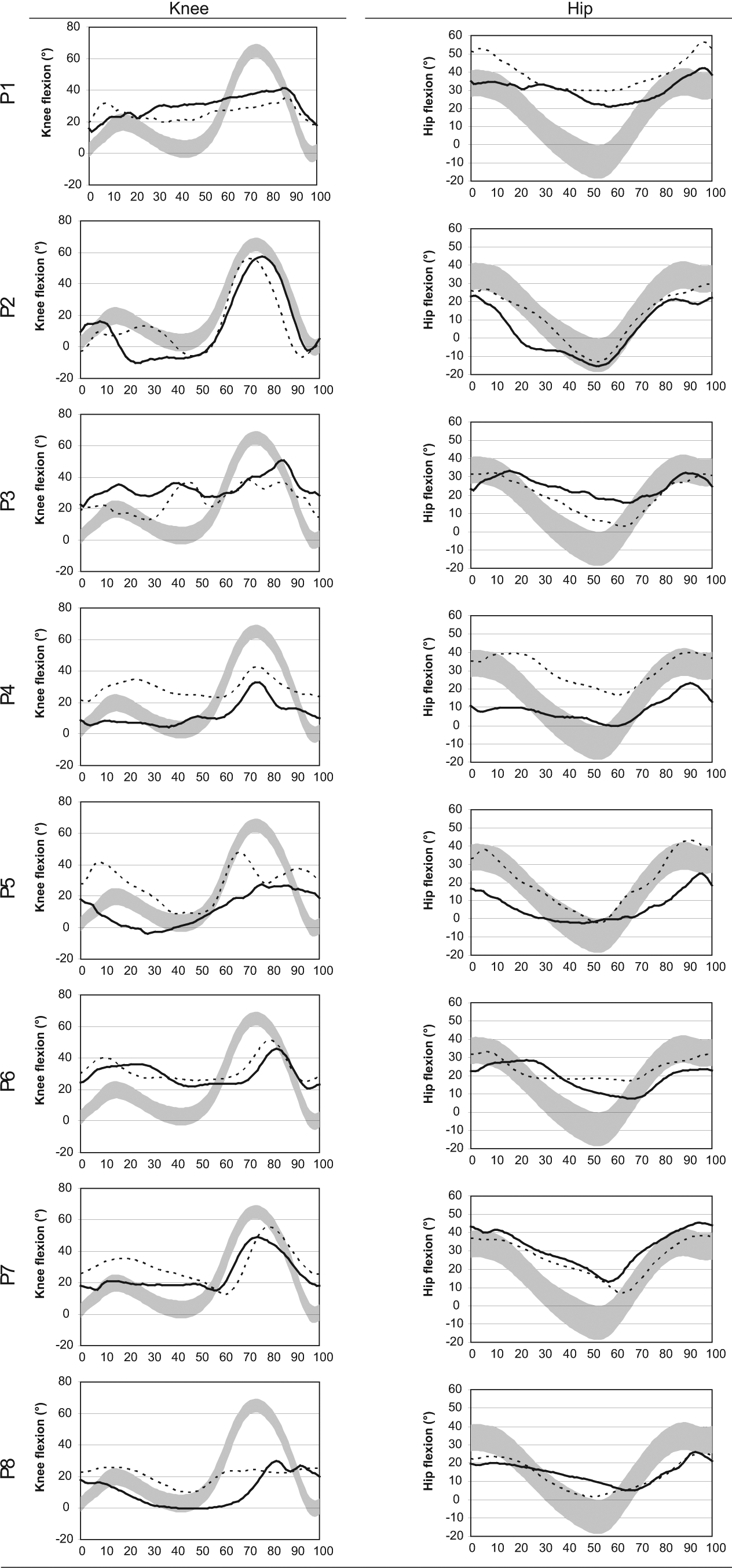
Hip and knee flexion extension profiles, showing the affected limb only. Solid line shows mean baseline measures, dotted line shows post-AFO fitting and tuning measures. Light grey shading shows normal reference data (±1 SD) from healthy older adults.
Discussion
The majority of participants experienced improvements for all spatiotemporal parameters indicated in Table 2, with only P7 and P8 showing any deterioration, although neither deteriorated with regard to all parameters. While the improvements in walking speed were statistically significant, only one participant (P5) showed an immediate clinically significant increase of >0.2 m/s. 33
The goal with the AFO intervention is to get the patient to walk as close to normal as possible.30,33 In order to achieve that, it was proposed that for the paretic limb, the SVA at mid-stance should be 10°–12° inclined, 16 and at MTLS, the thigh should be inclined (>5°) with the knee slightly flexed at approximately 10°–18°. 27 By using the AFO to directly control the SVA at mid-stance, the likelihood of achieving correct segment orientation during the MTLS phase should have been increased, thus allowing a correct GRF alignment. Intervening with segment orientations in this way is likely to influence motor control by attempting to ensure that the correct signals are sent to the central pattern generators.
Theoretically, if these three kinematic parameters were correct, the patient should have seen a significant improvement in their gait pattern, as indicated by the spatiotemporal parameters. While there was a general trend for the group towards improvement regarding these three parameters (such that they were brought closer to normal target values), the only participant who experienced clear immediate improvements in all three parameters was P5 (Table 3). This participant also had the most significant improvement in walking velocity (0.6 m/s), improved their symmetry from 0.73 to 0.95, cadence from 42.4 to 54.7 steps/min and had the largest increase in their overall step length from 0.31 m to 0.53 m (Table 2). P2 also experienced improvements in all three kinematic parameters (only marginal improvement in knee flexion from −3.8° (4.4°) to −3.1° (0.7°)) and improved walking velocity by 0.14 m/s, symmetry from 0.88 to 0.9 and step length from 0.48 to 0.63 m, although cadence was decreased from 81.2 to 78.5 steps/min (Table 2). Another participant whose data supported this theory was P6, as the participant appeared to experience the least improvement in the three kinematic parameters (Table 3) and exhibited some of the smallest improvements in spatiotemporal parameters (Table 2).
One participant who experienced mixed improvements in the three kinematic parameters was P3 as the participant achieved an improvement in TVAmax and knee flexion angle at TVAmax, although the participant’s SVA moved further away from the target values. Despite this, P3 improved with regard to spatiotemporal parameters. P3 did have a highly variable SVA values (standard deviations of 6.7° and 6.2°), whereas other participants had considerably lower SVA standard deviations (0.3° to 2.4°). This suggests that P3 walked in an inconsistent manner both before and immediately after AFO provision. While the participant’s AFO may have been tuned appropriately during standing, some unexplained lack of motor control or muscle imbalance meant the AFO could not adequately control the shank segment. This suggests that it is important to assess the SVA in both standing and at mid-stance during gait. It is unknown whether or not P3 would have achieved better immediate spatiotemporal outcomes were the AFO able to consistently keep his SVA at the target 10°–12° at mid-stance. P3 also had the lowest mRMI score, the highest EuroQol score and was the oldest participant which suggests an acceptance of his poor mobility levels, and possibly had lower expectations from his rehabilitation programme than the younger participants. Despite this, P3 did benefit from AFO fitting and tuning, which suggests that tuned AFOs can help patients who have very limited mobility and potentially low levels of motivation.
The individual cases described above only suggest a link between correct AFO fitting and tuning with respect to the three kinematic parameters and improvements in their spatiotemporal gait parameters. This study would have needed greater numbers of participants to allow a meaningful investigation of any correlations between spatiotemporal and kinematic parameters.
Ideally, every participant would have received an AFO which provided improvements for the three identified kinematic parameters, as was the case with P5. Table 3 shows that this was not achieved in this study. It could be the case that a tuned AFO cannot achieve all of these improvements with every stroke patient at once given each participant’s unique combination of gait abnormalities. Often one kinematic parameter was improved but to the detriment of another, for example, P4 experienced an improvement in SVA combined with a deterioration in TVAmax. A particular hindrance to achieving these improvements in all participants was that the AFO tuning process was not as exhaustive as it could have been. With participants ranging from 1 to 8 weeks post-stroke, they often fatigued very quickly, so only a small number of different wedge heights could be tested; therefore, the optimal solution was perhaps not obtainable in the time available.
The time point at which the maximum response to a solid AFO occurs is currently not known. It is likely the case that improvements in all kinematic parameters (except for SVA at mid-stance) do not occur immediately; therefore, it would be useful to take further 3D gait analysis measurements with these participants at 3 and 6 months, which could prove to be particularly important given the varying rates of improvement seen with different AFOs as reported by De Sèze et al. 12 The target values for SVA, TVAmax and knee flexion at TVAmax used in this study (see Table 3) were taken from different sources and were collected using different techniques, so future work in this area should also be done to clearly define the mean and standard deviation values for these three parameters in normal healthy participants. Such data could then be used for creating robust target values for AFO fitting and tuning sessions.
While it remains unclear whether segment orientation kinematic parameters are good predictors of the success of an AFO, they would appear to be more practical than the hip and knee joint kinematics profiles (which are regularly provided in gait analysis reports) shown in Figure 2. Given that much AFO fitting and tuning occurs without the use of 3D motion analysis systems, it may be pragmatic to suggest that clinicians focus on segment orientations when conducting observational gait analysis. The use of a larger sample size would allow any correlations that exist between these three kinematic parameters and spatiotemporal gait improvements to be investigated fully. In doing so, the nature of the improvements offered by solid AFOs and appropriate fitting and tuning techniques could be better understood.
Overall, this study broadly agrees with the previous studies5,8 –12,19 in that it shows a general improvement in spatiotemporal walking parameters in stroke patients with AFOs. It describes in detail how a local protocol for custom-made solid AFOs that have been tuned can be used to provide to early stroke patients with statistically significant walking improvements.
Conclusion
This study has shown that custom-made solid AFOs are likely to cause an immediate increase in gait velocity, overall step length and cadence in persons who are at an early stage stroke of stroke rehabilitation, although levels of improvement were variable. While the AFO fitting and tuning process does improve spatiotemporal parameters of walking speed, overall step length and cadence, it did not have a noticeably positive effect on hip and knee kinematic profiles. The three kinematic parameters discussed (SVA, TVAmax and knee flexion at TVAmax) were moved closer to normal ranges through the use of AFOs, and although these changes were not significant, they may ultimately prove to be useful in assisting clinicians to achieve optimal AFO tuning during routine clinical sessions.
Footnotes
Acknowledgements
The authors would also like to thank the National Health Service (NHS) Physiotherapists, Orthotists and Service Managers who made this study possible.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by The Medical Research Council, Lifelong Health and Wellbeing (Phase 2) (Ref: G0900583, Grant ID: 91021).