
Abstract
Background: Identifying and understanding the changes in transfer of momentum that are directly affected by orthotic intervention are significant factors related to the improvement of mobility in individuals with hemiplegia.
Objectives: The purpose of this investigation was to use a novel analysis technique to objectively measure weight transfer during double support (DS) in healthy individuals and individuals with hemiplegia secondary to stroke with and without an ankle foot orthosis.
Study design: Prospective, Repeated measures, case-controlled trial.
Methods: Participants included 25 adults with stroke-related hemiplegia >6 months using a prescribed ankle foot orthosis and 12 age-matched healthy controls. Main outcome measures included the weight transfer point timing (WTP, %DS), maximum total force timing (MTF, %DS), timing difference between WTP and MTF (MTF-WTP, %DS) and the linearity of loading (LOL, R2) during the DS phase of the gait cycle.
Results: The WTP and LOL were significantly different between conditions with and without the ankle foot orthosis for the affected and unaffected limb in post-stroke individuals, p ≤ 0.01. The MTF and difference in timing between MTF-WTP were significantly different during affected limb loading with and without the ankle foot orthosis in the stroke group, p ≤ 0.0001 and p = 0.03, respectively. MTF, MTF-WTP and LOL were significantly different between individuals with stroke (during affected limb loading) and healthy controls (during right limb loading).
Conclusions: This research established a systematic method for analysing weight transfer during walking to evaluate the effect of an ankle foot orthosis on loading during double support in hemiplegic gait. This novel method can be used to elucidate biomechanical mechanisms behind orthosis-mediated changes in gait patterns and quantify functional mobility outcomes in rehabilitation.
This novel approach to orthotic assessment will provide the clinician with needed objective evidence to select the most effective orthotic intervention to maximize functional recovery for individuals with hemiplegia secondary to stroke.
Introduction
Hemiplegia secondary to stroke causes decreased mobility and functional disturbances in healthy walking patterns, leading to limitations in activities of daily living and long-term disability. 1 – 3 Patient goals for rehabilitation after stroke are primarily functional in nature and regaining the ability to walk is a key objective. 4 – 6 Assistive technology devices such as ankle foot orthoses (AFOs) are often prescribed to individuals with motor deficits as a result of stroke to assist with ambulation. 7 – 11 While research addressing hemiplegic gait and orthotic interventions does exist, this research has consistently been limited by the research methodology. 12 – 15 Specifically, functional ambulation measures such as walking speed, step length and cadence have been used as the key determinants of orthotic effectiveness, but the mechanisms underlying these functional outcomes have not been clearly identified. 12 – 14,16 Increased walking speed is a measure of walking performance, while improved transfer of momentum during hemiplegic gait is a marker of functional recovery. 17 Past research efforts have focused on neuromuscular and biomechanical changes in acute stroke without considering their relationship to biomechanical mechanisms. 12 Evaluating the mechanism of transfer of momentum during hemiplegic gait would help explain the decrements in gait efficiency and walking speed associated with hemiplegic gait. 12,16
During gait, conservation of momentum allows for the continued forward progress of the body while the system recycles for the next power phase. 18,19 Successful transfer of momentum during gait occurs as forefoot weight bearing decreases in the trailing limb and more weight is transferred to the anterior weight acceptance limb. 20 Weight transfer in the trailing limb occurs proximal to distal in an efficient manner. 18 The ability to efficiently transfer weight during double support allows effective transfer of momentum from one limb to the other and the uninterrupted use of the kinetic energy which is created by the swing limb activity of the offloaded limb. 18,20 If weight transfer is delayed, the kinetic energy created by the swing limb is not utilized; it must be generated by added compensatory mechanisms that are less efficient and will decrease walking speed. 18 The limb-loading and propulsive phases of the gait cycle are inefficient in individuals with hemiplegia. 21 – 23 This is often due to inefficient weight bearing on the affected side causing non-linear limb load transfer. 16,24 In individuals with hemiplegia the centre of mass (CoM) is generally shifted towards the unaffected limb, creating disturbances in dynamic weight transfer during double support. 25 – 27 Stroke rehabilitation goals focus on improving load transfer onto the affected limb to facilitate more healthy movement patterns. The ability to maintain gait speed is dependent on the ability to shift body weight to the affected limb. 28,29
It is well understood in the literature that characteristics of double support are directly related to gait speed. 20 Previous research has focused primarily on the duration of double support but has failed to further evaluate the specific characteristics of weight transfer during this phase of gait. 30 – 32 As a result, this research focuses on the double support portion of the gait cycle to evaluate transfer of momentum during limb loading using a novel weight transfer analysis.
Identifying and understanding the changes in transfer of momentum that are directly affected by orthotic intervention are significant factors related to the improvement of mobility in individuals with hemiplegia. 12,16 We suggest that a more active rollover, indicated by increased linear loading and a more efficient load transfer from one limb to the other, will ultimately preserve momentum and increase gait speed.
Individual mechanisms contributing to improved walking speed in hemiplegic gait with AFO intervention will help to maximize functional recovery and, ultimately, rehabilitation outcomes. The purpose of this investigation was to use a novel analysis technique to objectively evaluate weight transfer during double support (DS) in healthy individuals and individuals with hemiplegia secondary to stroke with and without an AFO.
Methods
Participants
Individuals with hemiplegia secondary to stroke with symptoms lasting more than 6 months and age-matched healthy controls were recruited for participation. All participants with stroke were previously prescribed an AFO for functional ambulation by their treating physician. Other inclusion criteria for the stroke group included: (1) uninvolved lower limb with no history of injury or pathology; (2) able to walk independently or with supervision for 25 feet both with and without AFO; (3) wears an AFO when walking at least 50% of the time. Individuals with significant orthopaedic, neuromuscular or neurological pathologies or history unrelated to stroke that would interfere with walking or limit the range of motion of the legs were excluded from the study.
Procedures
Wireless pedobarography data was collected bilaterally using the pedar®-x (Novel Electronics, Inc., Munich, Germany) at 100 Hz for all participants during walking trials at a self-selected pace. The pedar®-x is an objective quantifiable pressure distribution measuring system for monitoring the magnitude and timing of plantar loading. The system consists of a portable data collection device attached to the subject’s hip, and two thin elastic sensor insoles inserted directly below the plantar surface of the foot. The insole sensor technology allows for bilateral analysis of multiple steps without the need to target foot placements during gait, as is needed when force platforms are used. Force is calculated by multiplying the recorded pressure by the sensor area, resulting in a force ‘normal’ to each sensor in the matrix. 33 Calculation of force using this technique may underrate the force as compared to the forces recorded from a force plate. The accuracy of the forces recorded using the pedar®-x has been deemed reliable for research and clinical applications. 33 – 35
Individuals in the stroke group completed 10 walking trials on an 8 m walkway (five with AFO, five without AFO). Healthy controls completed a 6 minute walk as part of a larger research study, and data was analysed for the first 18 seconds of the walking test. Per convention, the first two steps were omitted from the analysis for all walking tests.
During all walking tests participants were allowed to stop and rest if necessary, and members of the study team provided non-contact guarding for safety. Participants wore New Balance neutral walking shoes (style NB 575VW, last SL2) for all walking trials and no comparisons were made to a barefoot condition. Shoes were standardized to minimize shear friction and plantar pressure attenuation due to low-pass filtering effects, and the metatarsophalangeal joints were free to extend within the AFO and the confines of the toe box. All procedures performed in this investigation were approved by the Human Subject Review Board and informed consent was obtained prior to study participation.
Weight transfer analysis
All pedobarography data were exported as time processes files from Novel Multimask evaluation software (Novel Electronics, Inc., Munich, Germany) and imported into Matlab (The Mathworks, Inc., Natick, MA) for custom analysis. Time series force data were used to determine gait cycle events. Footstrike was defined as the time point at which any sensor measured a force greater than zero and toe-off was defined as the first time point subsequent to footstrike when all forces plantar to the foot were equal to zero. Double support was defined as the time period between footstrike on the loading foot and toe-off on the unloading foot. The three weight transfer analysis outcome variables of interest were the weight transfer point timing (WTP), maximum total force timing (MTF) and the linearity of loading (LOL) (Figure 1). All three variables occurred during the double support (DS) phase of the gait cycle.
Weight transfer outcome variables during initial double support (IDS) on the loading limb: a. Weight transfer point (WTP) and maximum total force (MTF); b. Linearity of loading (LOL).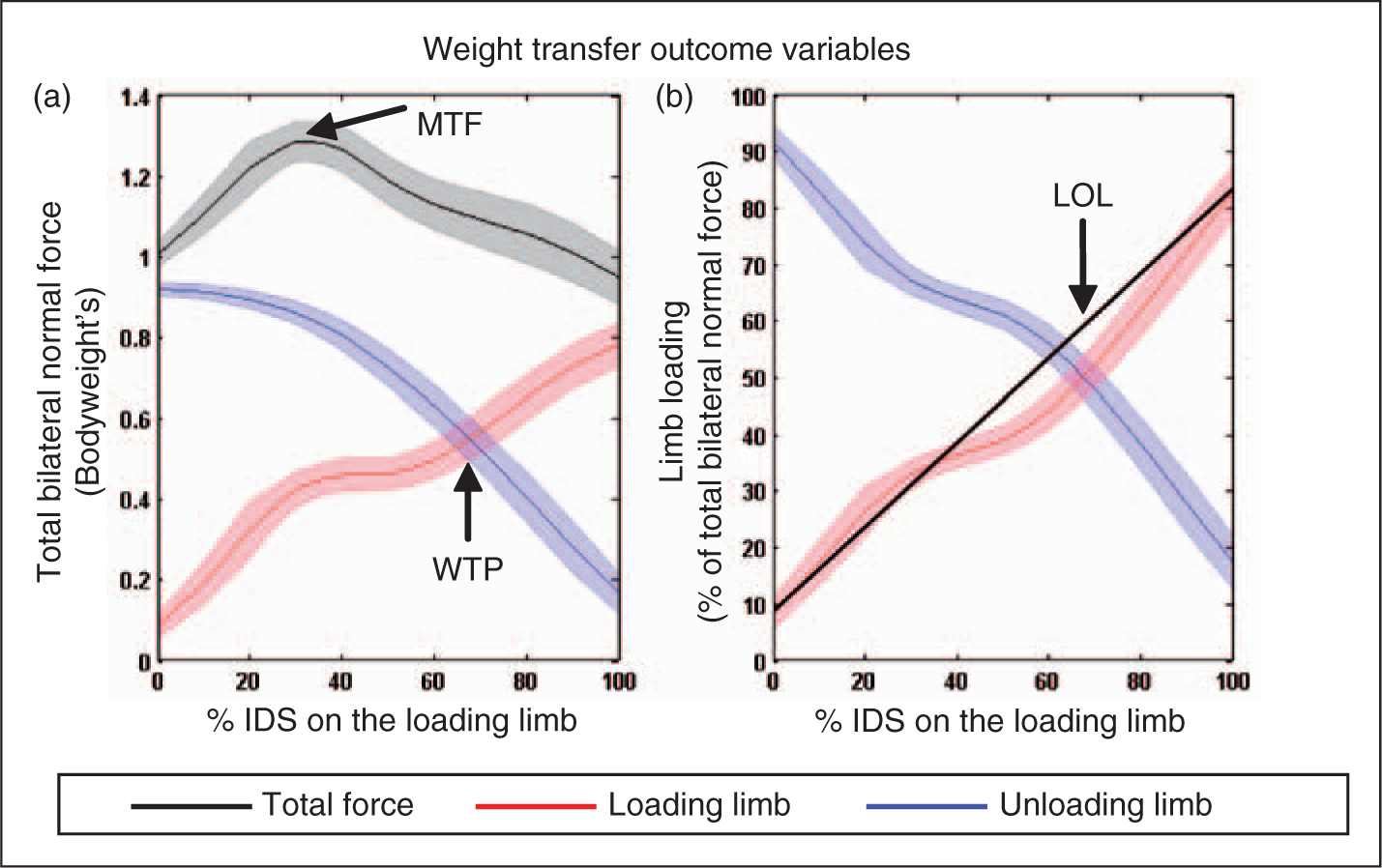
Normal force (Newtons) was collected using the pedar®-x, and time normalized to 100% of initial double support and the corresponding terminal double support on the unloading limb. The normal force under each foot was calculated as a percentage of the total loaded force in body weights. The force of the loading leg during double support was plotted against the force on the unloading leg to determine the time point when weight was equally distributed, which was defined as the weight transfer point (WTP, %DS). Maximum total force (MTF, %DS) was defined as the time point when peak bilateral force occurred during double support (bodyweights), and was calculated by adding the loading limb force and the unloading limb force to measure the force exerted bilaterally. WTP and MTF were used to measure the temporal changes in weight transfer during walking. The timing difference between the WTP and MTF was also analysed (MTF-WTP).
Loading limb force was graphed as a ratio of loading limb force to total force of both limbs during double support. A linear regression was fitted to the normalized loading limb force for which the coefficient of determination (R2) was defined as the linearity of loading (LOL).
Demographic information including age, gender, height, weight and time since stroke was collected and verified with medical records. Data from all assessments are represented as mean ± standard deviation.
Data analysis
Demographic data were analysed using descriptive statistics in PASW Statistics 18.0. Independent two sample t-tests were performed to determine if there was a significant difference in weight transfer (WTP, MTF, MTF-WTP and LOL) between the stroke group and the healthy control group. Comparisons were made while the affected limb was accepting weight (loading) and the unaffected limb was unloading (preparing for swing) for individuals in the stroke group. In the healthy control group the right limb was used as the loading limb and the left as the unloading limb throughout the analysis for comparison.
A two-way within-subject repeated measures analysis-of-variance (ANOVA) model was used to determine if there were significant differences in the weight transfer (WTP, MTF, MTF-WTP and LOL) in the stroke group between conditions, with and without AFO. Comparisons were made bilaterally during double support for affected and unaffected limb loading to examine the intralimb (within a limb) difference in weight transfer during walking trials with and without AFO in the stroke group.
Results
Participant characteristics (mean ± SD).

All participants with stroke included in this investigation used their own custom moulded plastic AFO on their affected limb during ambulation in the with-AFO condition. All AFOs were positioned below the knee just beneath the neck of the fibula and secured across the anterior aspect of the proximal tibia with a hook and loop strap. Distally, the AFO was trimmed posterior to the ankle malleoli and included a footplate that extended along the length of the plantar surface of the foot to at least the metatarsal heads. The AFO was used for ambulation inside the shoe and shoe type (style and last) was standardized.
Weight transfer outcome variables during affected and unaffected limb loading in individuals with stroke, and right limb loading in the healthy control group.
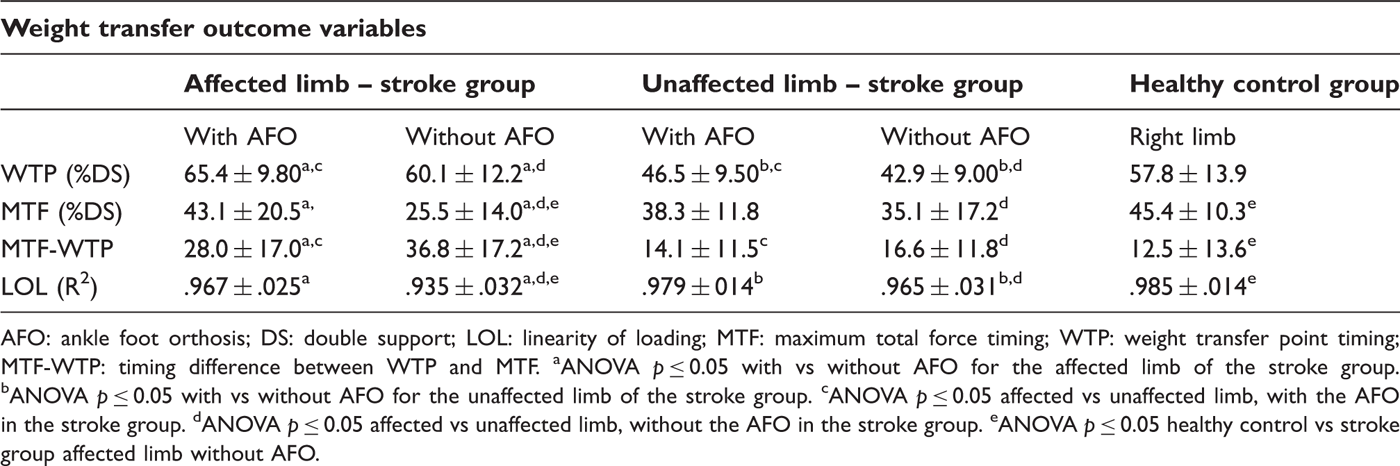
AFO: ankle foot orthosis; DS: double support; LOL: linearity of loading; MTF: maximum total force timing; WTP: weight transfer point timing; MTF-WTP: timing difference between WTP and MTF. aANOVA p ≤ 0.05 with vs without AFO for the affected limb of the stroke group. bANOVA p ≤ 0.05 with vs without AFO for the unaffected limb of the stroke group. cANOVA p ≤ 0.05 affected vs unaffected limb, with the AFO in the stroke group. dANOVA p ≤ 0.05 affected vs unaffected limb, without the AFO in the stroke group. eANOVA p ≤ 0.05 healthy control vs stroke group affected limb without AFO.
The WTP between the affected limb of the stroke and healthy control group were not statistically different, t(35) = 0.09, p = 0.929. In the stroke group for the WTP there was a significant main effect of AFO condition, F(1,72) = 20.83, p ≤ 0.0001. With the AFO, WTP occurred significantly later than without the AFO during double support for both affected limb (p = 0.0051) and unaffected limb (p = 0.0096) loading (Figure 2). The WTP for the unaffected limb of the stroke group occurred significantly earlier (∼20%) than affected limb loading in the with- and without-AFO condition, t(35) = 7.35, p ≤ 0.0001, and t(35) = 6.67, p ≤ 0.0001, respectively.
Mean weight transfer point timing (WTP) during initial double support (IDS) on the loading limb of individuals with stroke, for unaffected and affected limb with and without ankle foot orthosis (AFO), and healthy controls.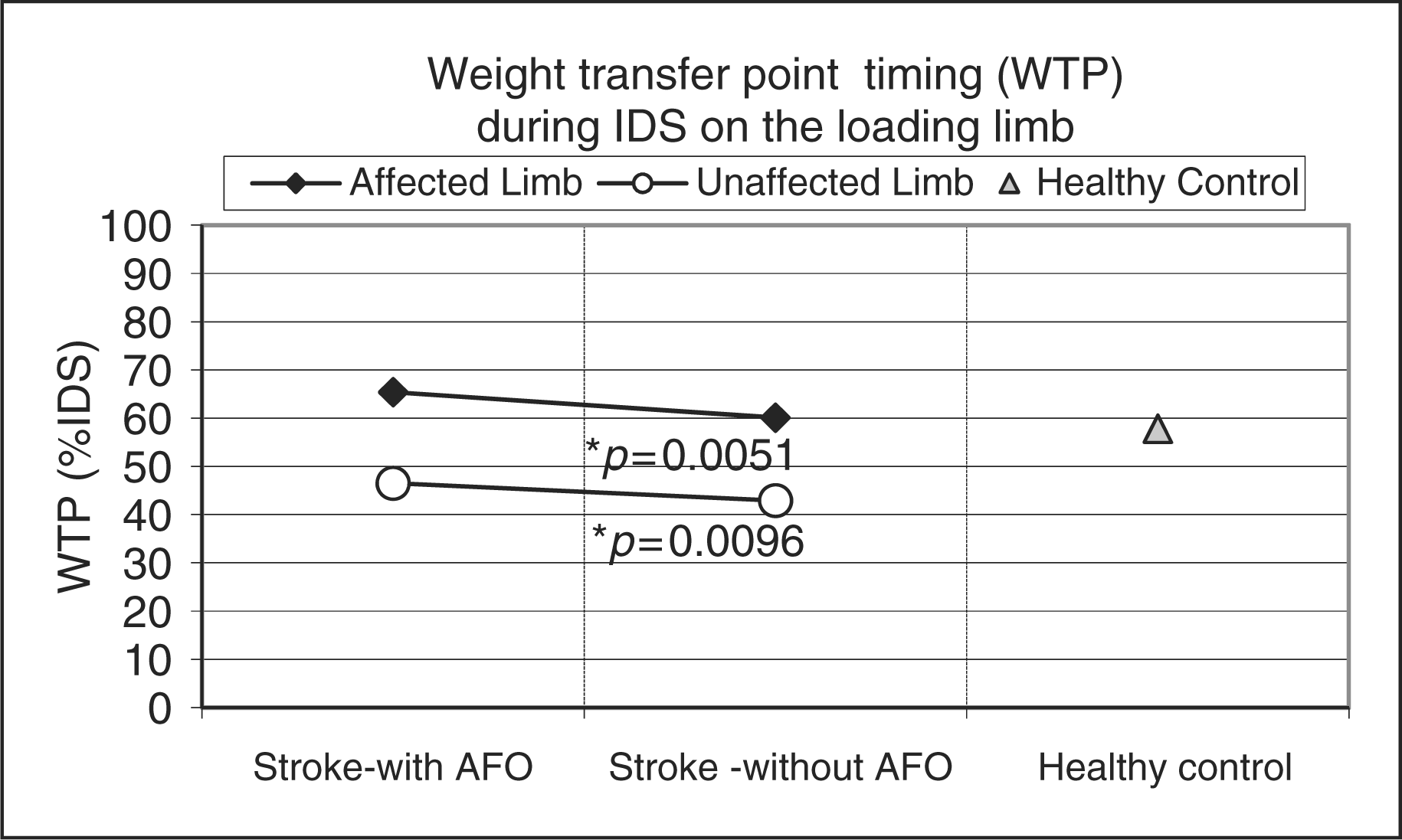
MTF occurred significantly earlier in the stroke group compared to the healthy controls, t(35) = −4.98, p ≤ 0.0001 (Figure 3). In the stroke group the repeated measures ANOVA for MTF revealed a significant main effect for the AFO condition, F(1,72) = 25.36, p ≤ 0.0001. When wearing the AFO, MTF occurred significantly later (∼17%) in double support for the affected limb (p ≤ 0.0001).
Mean maximum total force timing (MTF) during initial double support (IDS) on the loading limb of individuals with stroke, for unaffected and affected limb with and without ankle foot orthosis (AFO), and healthy controls.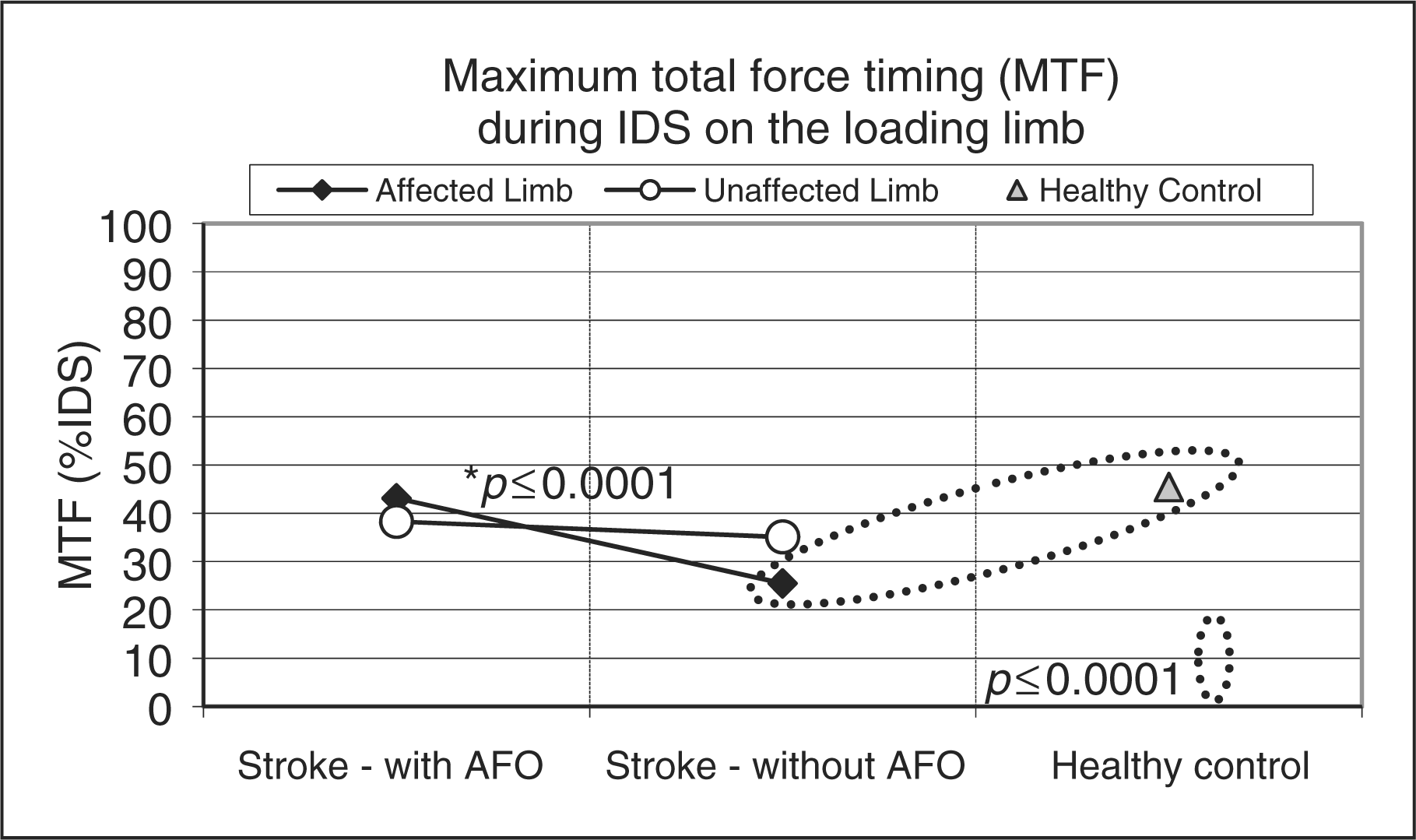
The timing difference between MTF and WTP was significantly different between the stroke group and the healthy control group, t(35) = 3.63, p = 0.0009 (Figure 4). In the stroke group for MTF-WTP there was also a significant main effect for the AFO condition, F(1,72) = 7.44, p = 0.008. When the AFO was added there was a significant convergence between MTF and WTP on the affected limb (p = 0.0309).
Mean timing difference between MTF and WTP (MTF-WTP) during initial double support (IDS) on the loading limb of individuals with stroke, for unaffected and affected limb with and without ankle foot orthosis (AFO), and healthy controls.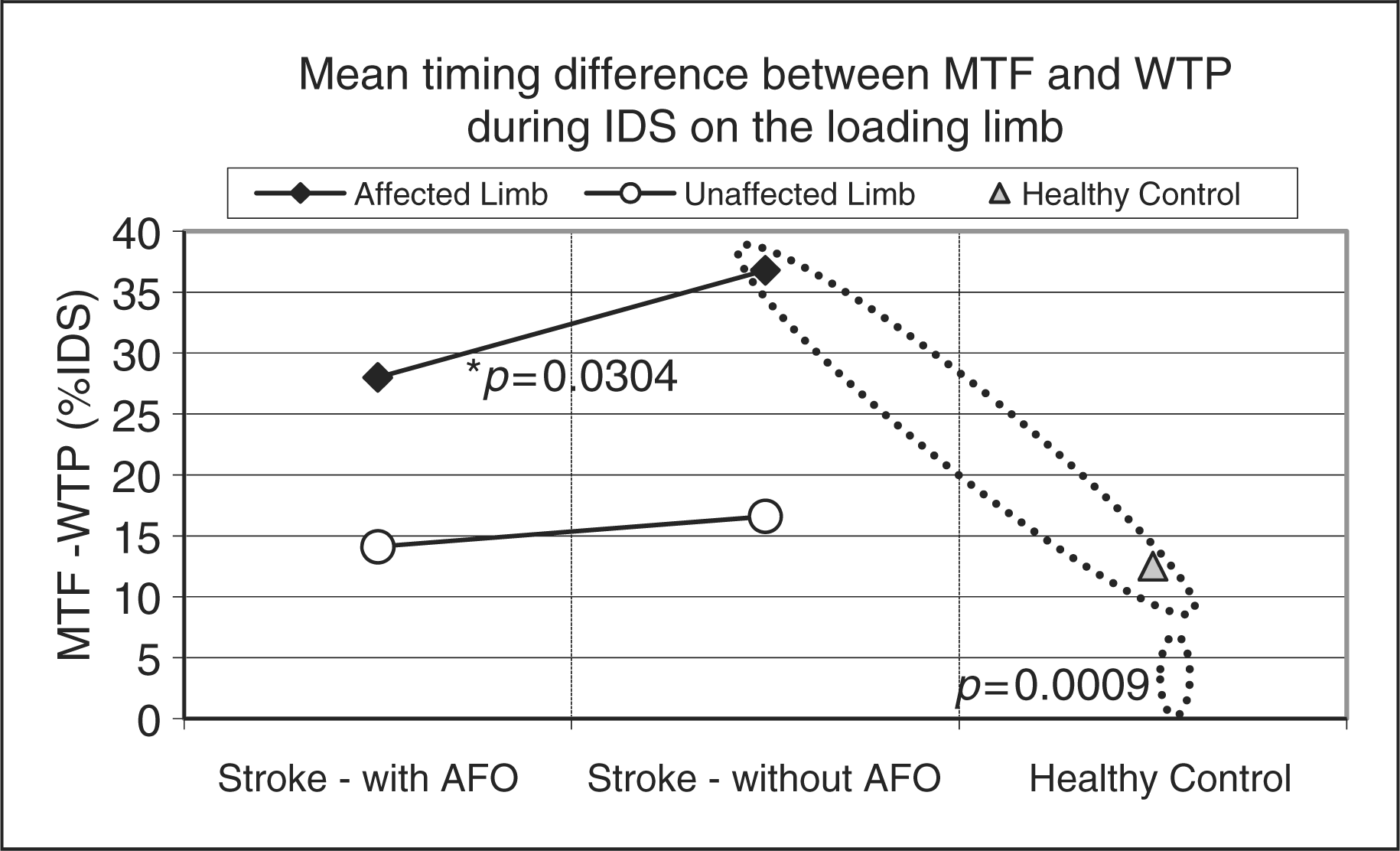
LOL was significantly more linear in healthy controls than in individuals with stroke, t(35) = −4.25, p = 0.0001 (Figure 5). The repeated measures ANOVA revealed a significant main effect for the with-AFO condition, F(1,72) = 28.34, p ≤ 0.0001. Linearity of loading (R2) significantly increased in the with-AFO condition during affected and unaffected limb loading in individuals with stroke (p ≤ 0.0001 and p = 0.014).
Mean linearity of loading (LOL, R2) during initial double support (IDS) on the loading limb of individuals with stroke, for unaffected and affected limb with and without ankle foot orthosis (AFO), and healthy controls.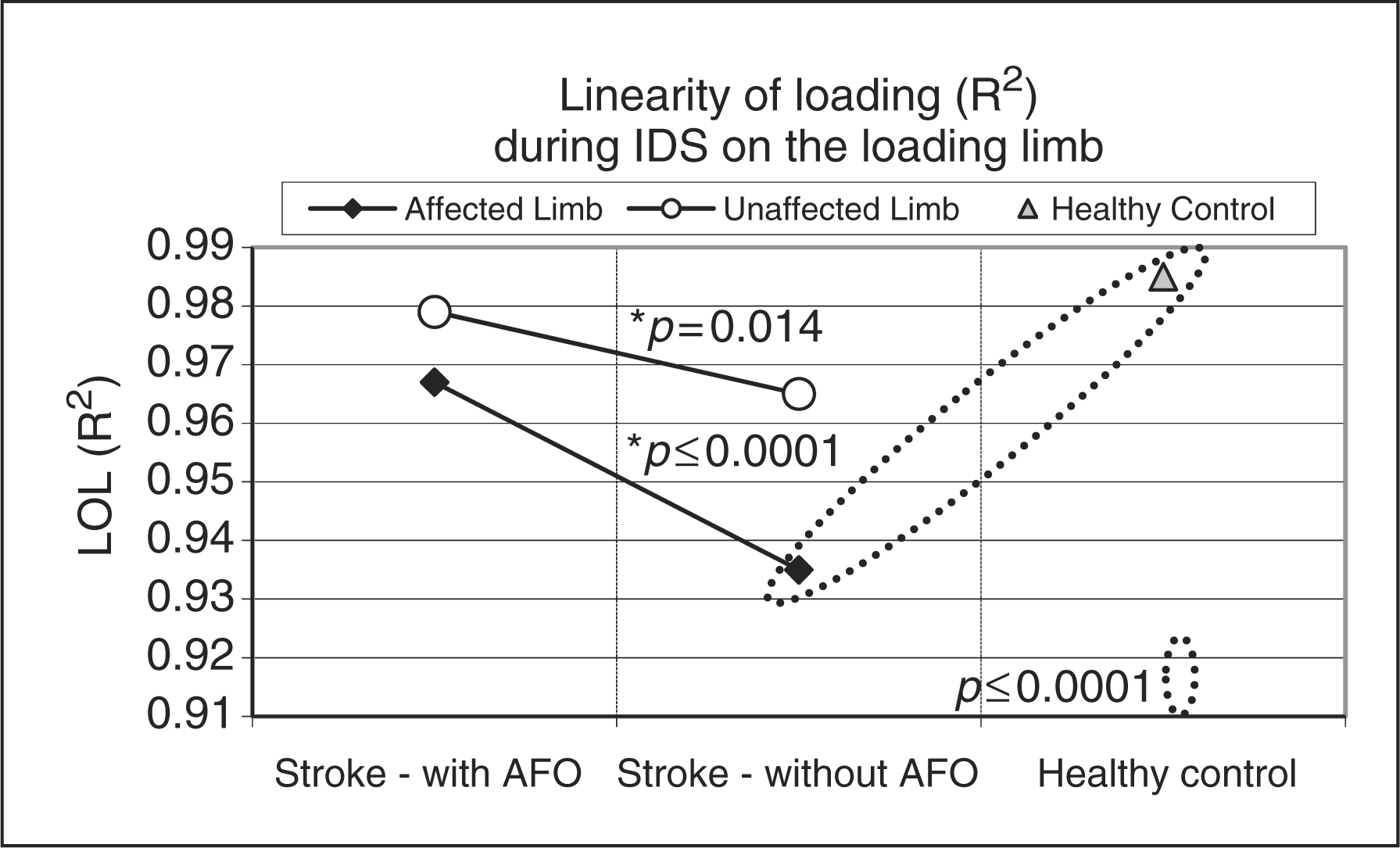
Discussion
Weight transfer analysis provides information about the transfer of momentum during gait and can offer valuable insight into changes in functional ambulation after orthotic intervention. Objectively quantifying the weight transfer mechanism after orthotic intervention is a key factor in understanding the mechanism of improving walking speed during hemiplegic gait. This study demonstrates the utility of weight transfer analysis and establishes a systematic method for analysis of orthotic interventions.
Weight transfer data analysis revealed that in healthy adults the temporal characteristics of weight transfer are more symmetrical and there are minimal interlimb loading differences. Within the stroke group WTP occurred ∼20% earlier for unaffected limb loading as compared to affected foot loading, producing an asymmetrical gait pattern. Individuals with hemiplegia delayed weight transfer when loading the affected limb, maintaining load on the unaffected limb for as long as possible (Figure 6). When loading the unaffected limb, individuals with hemiplegia unloaded the affected limb rapidly in an effort to again load the unaffected limb for as long as possible. Increased time loaded on the unaffected limb during weight transfer causes a disruption in the transfer of momentum and may negatively affect walking speed. Delayed WTP during unaffected limb loading was an anticipated positive result of orthotic intervention. Delayed weight acceptance during weight transfer onto the affected limb, resulting from orthotic intervention, was an unanticipated result. More research is needed in adults with hemiplegia after orthotic intervention to determine the relationship between delayed weight transfer and walking speed.
Weight transfer outcome variable linearity of loading (LOL) during initial double support (IDS) on the loading limb provided for two representative participants: a. stroke participant affected limb loading without AFO; b. stroke participant affected limb loading with AFO; c. healthy control right limb loading.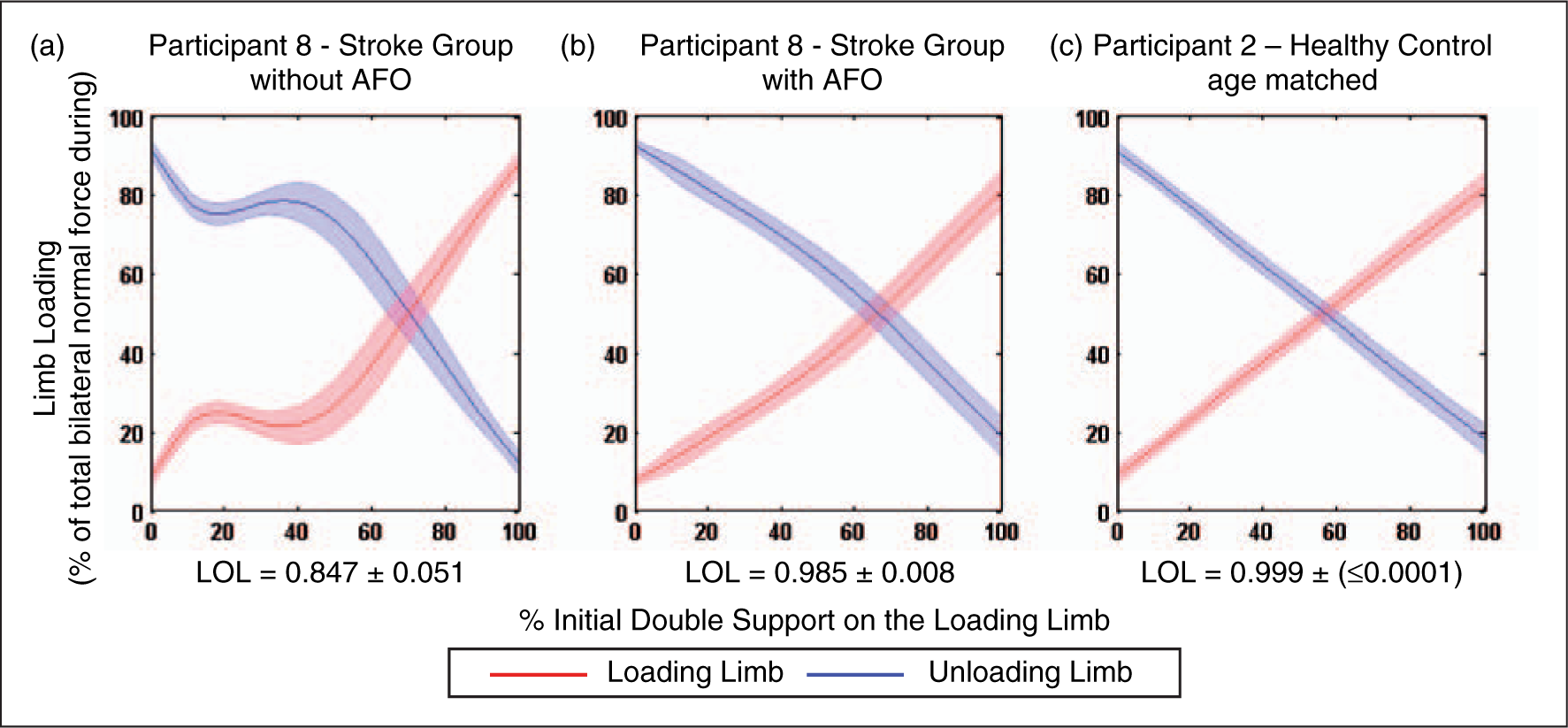
The timing of MTF is an important factor for maintaining balance during double support. Healthy controls exhibit an even distribution of weight between limbs at the point of maximal loading, producing a more balanced position. Individuals with stroke are typically asymmetrically loaded during MTF because weight transfer onto the affected limb is delayed (Figure 6). This asymmetrical load transfer during peak loading may create a necessity for compensation by other structures to maintain balance during double support. Interestingly, when the AFO is added, MTF timing shifts for the affected and unaffected limb to more closely resemble the MTF timing of healthy controls. This information could become a critical outcome in quantifying the effect of orthotic intervention.
The similarity of WTP and MTF timing in the healthy control group indicated a more balanced position as weight was transferred. In individuals with stroke the difference in timing between the MTF and WTP during affected limb loading indicated a greater weight imbalance between limbs at the point of maximum loading. This weight imbalance could cause undesired lateral forces that may lead to instabilities during gait. The convergence of the WTP and MTF during affected limb loading in the stroke group after orthotic intervention indicated a more balanced position during maximum loading that more closely resembled weight transfer in healthy controls.
Limb loading was more linear (LOL) bilaterally in the healthy controls, indicating a fluid weight transfer and effective transfer of momentum to the loading limb. In individuals with stroke, affected leg loading was characterized by oscillations in weight acceptance (loading) creating a less linear weight transfer. This non-linearity in individuals with stroke represents an inconsistent rate of loading the affected limb, which will reduce momentum and create an inefficient gait pattern. Individuals with hemiplegia delay weight transfer onto the affected limb which produces loading curves with a cubic shape. In the stroke group, orthotic intervention increased LOL bilaterally, indicating a more linear weight transfer and an improved transfer of momentum. Effective transfer of momentum can increase propulsion; the more linear the weight transfer between limbs, the more efficient the transfer of momentum and rollover progression during gait. 18 This concept of transfer of momentum is often overlooked, but is a significant factor related to the improvement of mobility of individuals and functional recovery in individuals with hemiplegia. 16 Identifying the mechanisms underlying the asymmetrical and non-linear loading provides objective outcomes to aid in rehabilitation and orthotic intervention.
This research aims to improve the clinician’s ability to create more individualized assessment options in rehabilitation. Measuring outcomes that can directly correlate to real life function will provide meaningful information about the potential effectiveness of an orthotic device. Using these novel objective analytical methods to evaluate weight transfer will help to provide the needed clinical evidence to incorporate new assessment techniques when selecting the most effective orthotic interventions to efficiently maximize functional recovery and create an improved standard of care for individuals with hemiplegia secondary to stroke. 36
A potential limitation of the current study is that the inclusion and exclusion criteria of the study may have created a sample of stroke patients that were higher functioning, especially because they were able to walk twenty-five feet without their AFO. 37,38 However, research has found that patients who receive an AFO on entry to or discharge from rehabilitation are more functionally impaired than patients who do not receive an AFO. 39 Additional research suggests that higher functioning patients may benefit from use of an AFO to increase and improve functional ambulation. 15 Another possible limitation is that only traditional plastic AFOs were used in this investigation. It is possible that different AFO designs (dynamic or hinged AFOs) could potentially provide different biomechanical advantages or disadvantages; therefore AFO type should be evaluated in future research. In addition, the AFO-footwear combinations were not tuned to optimize gait prior to data collection. The researchers did not attempt to adjust the AFOs and completed all testing procedures with the device as prescribed and fitted by the participant’s physician and orthotist. Another potential limitation is that there may be variations in weight transfer between males and females, as gender had an effect when difference scores were evaluated during preliminary data analysis. Future research should therefore evaluate the effect of gender.
Conclusion
This research established a systematic method using three easily calculated outcome variables (WTP, MTF and LOL) for analysing weight transfer during walking, to quantify functional mobility outcomes in rehabilitation. Our novel analysis technique was utilized to objectively evaluate weight transfer during double support in healthy individuals and in individuals with hemiplegia secondary to stroke with and without an AFO. The load transfer mechanism in hemiplegia is a key factor in understanding how to improve gait speed and efficiency through orthotic intervention. We also anticipate that this novel approach to orthotic assessment will expand our assessment measures to better evaluate changes in functional ambulation in order to elucidate biomechanical mechanisms behind orthosis-mediated changes in gait patterns.
Footnotes
Funding
This work was supported by the Department of Education National Institute on Disability and Rehabilitation Research (grant no. H133F070028), New Balance Athletic Shoe Inc. and the Kessler Foundation.