
Abstract
Background:
An ankle-foot orthosis with an oil damper was previously developed to assist the first rocker function during gait, but the effects of the amount of resistive moment generated on gait have not been clarified.
Objectives:
To measure the amount of resistive moment generated by the ankle-foot orthosis with an oil damper during gait and determine its effect on the gait of patients with stroke.
Study Design:
Preliminary cross-sectional study.
Methods:
The gait of four patients with stroke in the chronic phase was measured in four conditions: without an ankle-foot orthosis and with the ankle-foot orthosis with an oil damper generating three different amounts of resistive moment. Measurements were taken with a three-dimensional motion analysis system and a specially designed device to determine the resistive moment.
Results:
The resistive moment was observed in the former half in stance of the paretic limb, and its magnitude was less than 10 N m. Some gait parameters related to terminal stance and preswing were affected by the amount of resistive moment. The forward component of floor reaction force and the shank vertical angle showed peak values when the patients reported feeling most comfortable during gait.
Conclusion:
Although the resistive moment generated by the ankle-foot orthosis with an oil damper was small, it was sufficient to alter gait.
Clinical relevance
To maximize the effectiveness of ankle-foot orthoses, it is necessary to know the effects of resistive moment on the gait of patients with stroke. The ankle-foot orthosis with an oil damper assists the first rocker function in gait and also affects the gait in a later phase in stance. The peak values of some gait parameters coincided with patients reporting gait to be most comfortable. It is important to know that ankle-foot orthosis with an oil damper assistance in the first rocker alters the weight acceptance on the paretic limb and affects the gait parameters related to propulsion ability in stance.
Background
Most patients with central nervous system (CNS) disease experience some difficulties with gait, such as foot drop during the swing phase, insufficient plantar flexor activity, and mediolateral instability of the ankle joint in stance. These problems result in decreased gait speed and an asymmetrical gait pattern.1 –5 Ankle-foot orthoses (AFOs) are frequently prescribed to overcome these problems, and the mechanical properties of the AFOs should be tuned to meet the needs of individual patients.
For tuning the AFOs, the neutral ankle joint angle and the stiffness of the AFOs must be considered. The neutral ankle joint angle is the angle at which the resistance of AFOs starts to generate, and it largely affects the shank vertical angle (SVA) in the stance phase. Previous studies have shown the importance of tuning the SVA alignment of the AFO–footwear combinations of nonarticulated AFOs.6,7 With regard to the stiffness of the AFOs, two kinds of stiffness have to be considered: the resistance to plantar flexion and the resistance to dorsiflexion. Most AFOs generate resistance to plantar flexion to prevent foot drop during the swing phase; indeed, this is one of the most important functions of AFOs for patients with CNS disease. 8 However, the need for resistance to dorsiflexion, which is generated by most nonarticulated AFOs, remains controversial. Some studies reported that such resistance is necessary to assist insufficient activity of the plantar flexors in mid-stance to late stance,9 –11 and specially designed carbon fiber AFOs were shown to improve the gait of children with plantar flexor weakness 12 and children with hemiplegia. 13 On the contrary, some studies found that AFOs generating such resistance impeded smooth ankle joint movement in stance. 14 In these studies, the gait of individuals wearing different kinds of AFOs with different degrees of stiffness was compared; however, the amount of resistance generated during gait has remained unreported. The amount of resistance of AFOs is shown by the resistive moment around the ankle joint. Therefore, to know the effects of resistive moment on gait, it is necessary to know the amount of resistive moment generated by an AFO during gait. Bregman et al. 15 measured the resistive moment generated by polypropylene AFOs with a low stiffness during gait in patients with stroke and found that while the mechanical contribution of AFOs was small, the patients’ gait was benefited by their use.
Another function of AFO resistance to plantar flexion besides preventing foot drop during the swing phase is the assistance of the first rocker function during gait. 16 This function assists insufficient eccentric contraction of the dorsiflexors of patients with stroke. 17 An ankle-foot orthosis with an oil damper (AFO-OD) was developed specifically to achieve this function, 18 and gait improvement in patients with stroke was seen with the AFO-OD, 19 with further improvement of gait being shown after gait training with the device. 20 Ohata et al. 21 performed electromyography in patients with stroke and found a significant reduction of excessive gastrocnemius activity in the loading response of the paretic limb when patients used the AFO-OD.
The amount of resistive moment to plantar flexion of the AFO-OD can be altered easily to meet the specific needs of individual patients. However, it is not clear how much resistive moment the AFO-OD generates during gait and how it affects the gait of patients with stroke. To answer these questions, a device to measure the amount of resistive moment generated during gait with the AFO-OD was developed. The purpose of this pilot study was to measure the amount of the resistive moment generated by the AFO-OD during gait in patients with stroke and its effects on their gait. Moreover, the relation between the gait parameters and the patients’ evaluation of comfort level during gait was investigated. The hypothesis of this study was that resistive moment would affect the gait of patients with stroke throughout the gait cycle while also affecting patients’ evaluation of comfort.
Methods
Measurement device
An AFO-OD (GaitSolution Design, Kawamura Gishi, Japan) that contains an oil damper at the ankle joint to generate resistive moment to plantar flexion was used in this study (Figure 1). To tune its use to the needs of individual patients, the amount of the resistive moment can be changed easily by rotating a screw at the top of the oil damper. The amount of resistance can be changed continuously in the range of 1 (very flexible) to 4 (rigid). In this study, the following three levels of resistance were tested: 2, flexible (AFO-OD2); 3, moderate (AFO-OD3); and 4, rigid (AFO-OD4). Level 1 was not tested because preliminary measurements determined that the amount of resistive moment at this level is less than 1 N m, and the effect of this moment was not thought to be important. To measure the plantar flexion resistive moment during gait, a load cell was inserted above the hydraulic cylinder in the oil damper unit. As the hydraulic cylinder produces a resistive force, it pushes the load cell as a counterforce; therefore, the measurement of the counterforce reflects the resistive force at the oil damper. The resistive moment was calculated by multiplying the lever arm by the resistive force. This device was the same as that used in a previous study. 21 The ankle joint of the AFO-OD rotates to dorsiflexion freely without resistance. The neutral ankle joint angle can be adjusted to the ankle joint angle at initial contact in each patient. Dorsiflexion adjustment ranged from 0° to 10°.
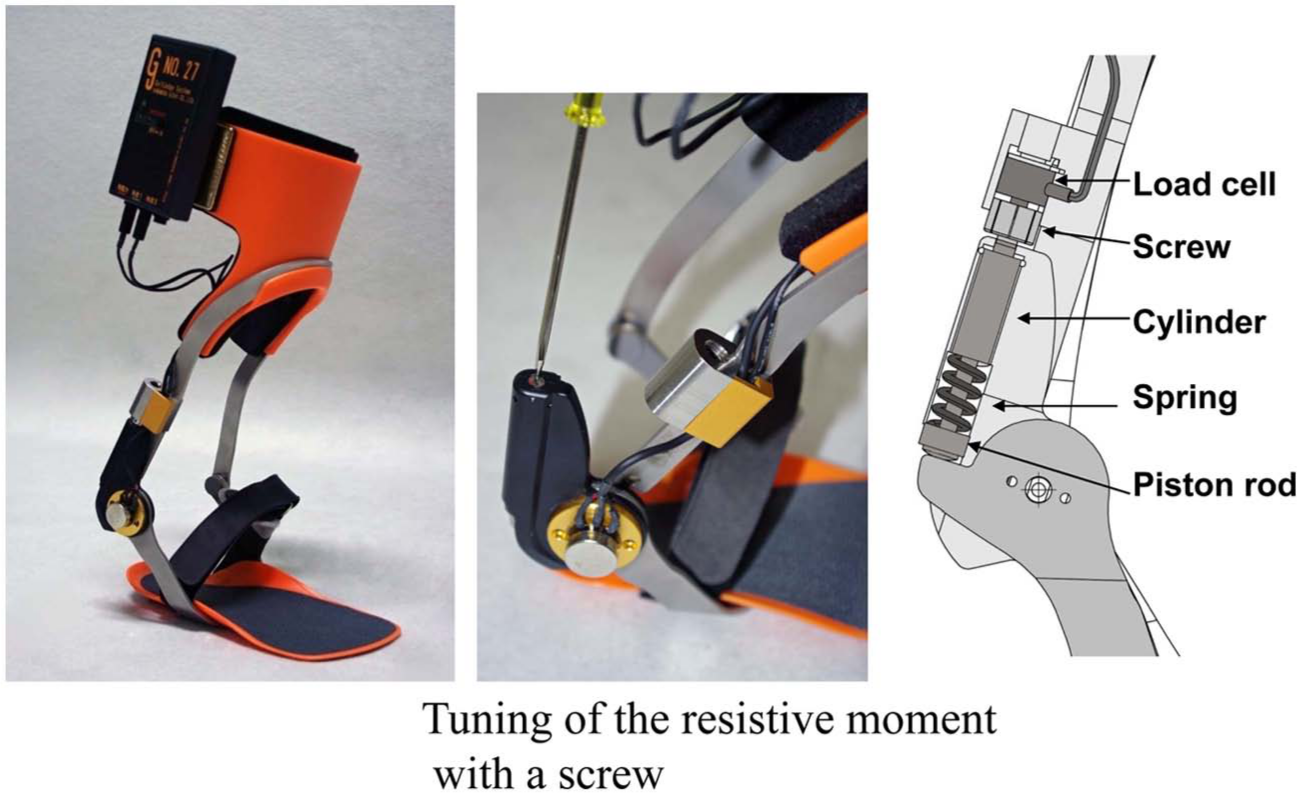
Measurement device for resistive moment generated by the AFO-OD.
A three-dimensional (3D) motion analysis system consisting of 10 cameras (VICON, Oxford, UK) and 6 force plates (AMTI, Watertown, MA, USA) was used. The trajectories of 16 reflective markers, force plate data, and resistive moment generated by the AFO-OD were measured simultaneously at a sampling frequency of 100 Hz. Markers were attached to the patients at each of the following landmarks: bilaterally on the acromion process; trochanter; and posterior aspects of the iliac spine, elbow, wrist, lateral epicondyle of the knee, lateral malleolus, and fifth metatarsophalangeal joint. Patients wore their own shoes in all measurements, and the use of canes was allowed during measurement if necessary.
Patients
Four patients with stroke in the chronic phase (more than 181 days after onset) participated in this study. The inclusion criterion was daily use of an AFO. The exclusion criteria were nonconcurrent pathologies affecting the CNS or neuromuscular system, communication problems, severe spasticity, and proprioceptive sensory impairment. The profiles of the patients are shown in Table 1. Two of the patients used the AFO-OD daily and the remaining two used other AFOs. To obtain control data, the gait of a 27 year-old healthy male subject was measured.
Profiles of patients with stroke.
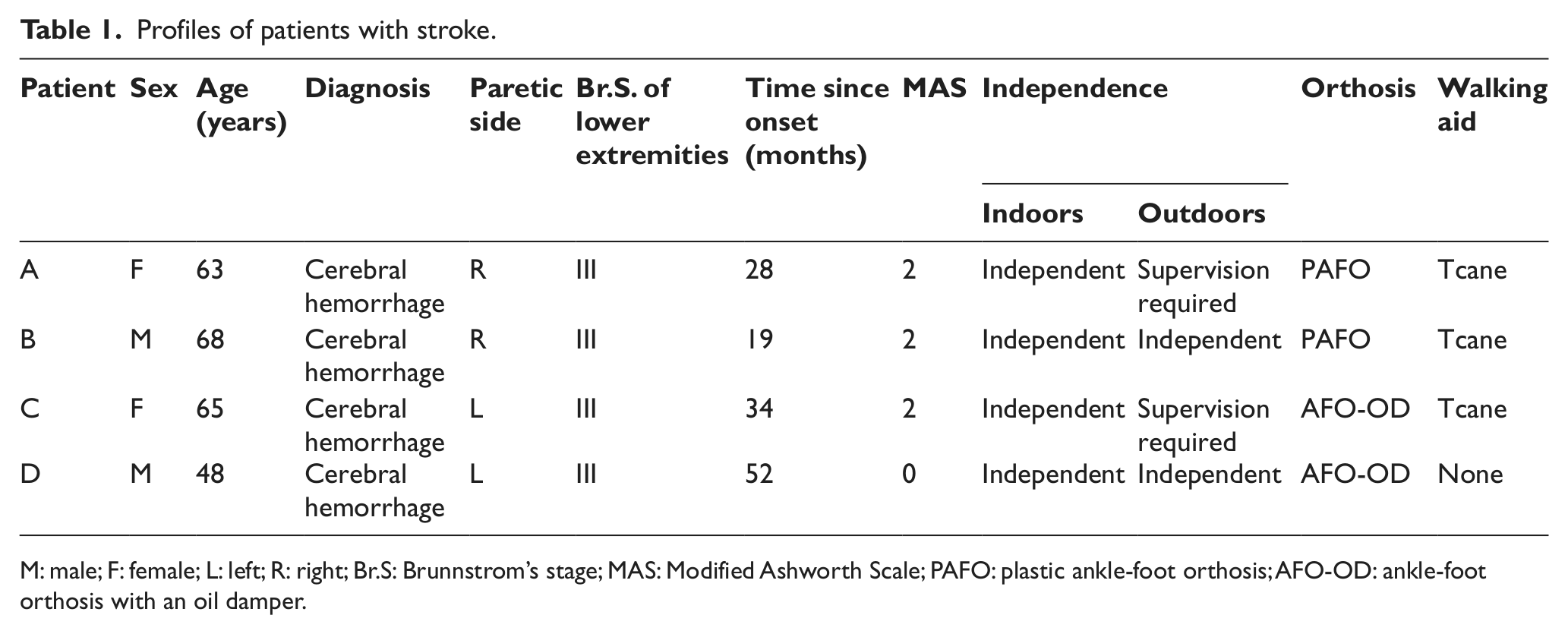
M: male; F: female; L: left; R: right; Br.S: Brunnstrom’s stage; MAS: Modified Ashworth Scale; PAFO: plastic ankle-foot orthosis; AFO-OD: ankle-foot orthosis with an oil damper.
All procedures were approved by the local ethics committee of International University of Health and Welfare and were consistent with the Declaration of Helsinki. Informed consent was obtained from all patients and the control subject prior to their participation in this study.
Measurement protocol
Gait without an AFO but with shoes was measured first, at a speed the patients determined to be comfortable. The measurements were repeated until five steps of the paretic limb on the force plates were obtained. Then, gait with the AFO-OD was measured for each of the three levels of resistive moment, AFO-OD2, AFO-OD3, and AFO-OD4. The order of resistive moment was randomized. A few minutes of practice was undertaken prior to the measurement in each condition. Patients were not informed about the value of the resistive moment. After all measurements had been taken, the patients were asked which of the three levels of resistance was the most comfortable.
Data processing
The trajectory of the markers and the force plate data were low-pass filtered by a second-order Butterworth filter with a cutoff of 6 Hz. The link segment model was defined, and the inverse dynamic model was used to calculate the joint kinematics and kinetics. 20 From these data, the spatiotemporal parameters and peak values of the joint angles and the joint moments of the paretic limb were detected in each condition. The ankle joint moment calculated by the inverse dynamic model was the sum of the internal joint moment and the resistive moment generated by the AFO-OD. The internal joint moment was obtained by subtracting the resistive moment from the net joint moment calculated by the inverse dynamic model. The maximum forward velocity of center of gravity (COG) in loading response, which meant the double support at the start of the stance phase, was also measured to show the level of weight acceptance. The SVA and anterior–posterior floor reaction force were also measured because these are the indicators of the propulsive ability of gait in patients with stroke.22,23 The maximum forward inclination of SVA in stance and the maximum forward component of the floor reaction force were detected. In total, 21 gait parameters (left column, Table 2) were used for the analysis.
Data in each condition and result of statistical analysis.
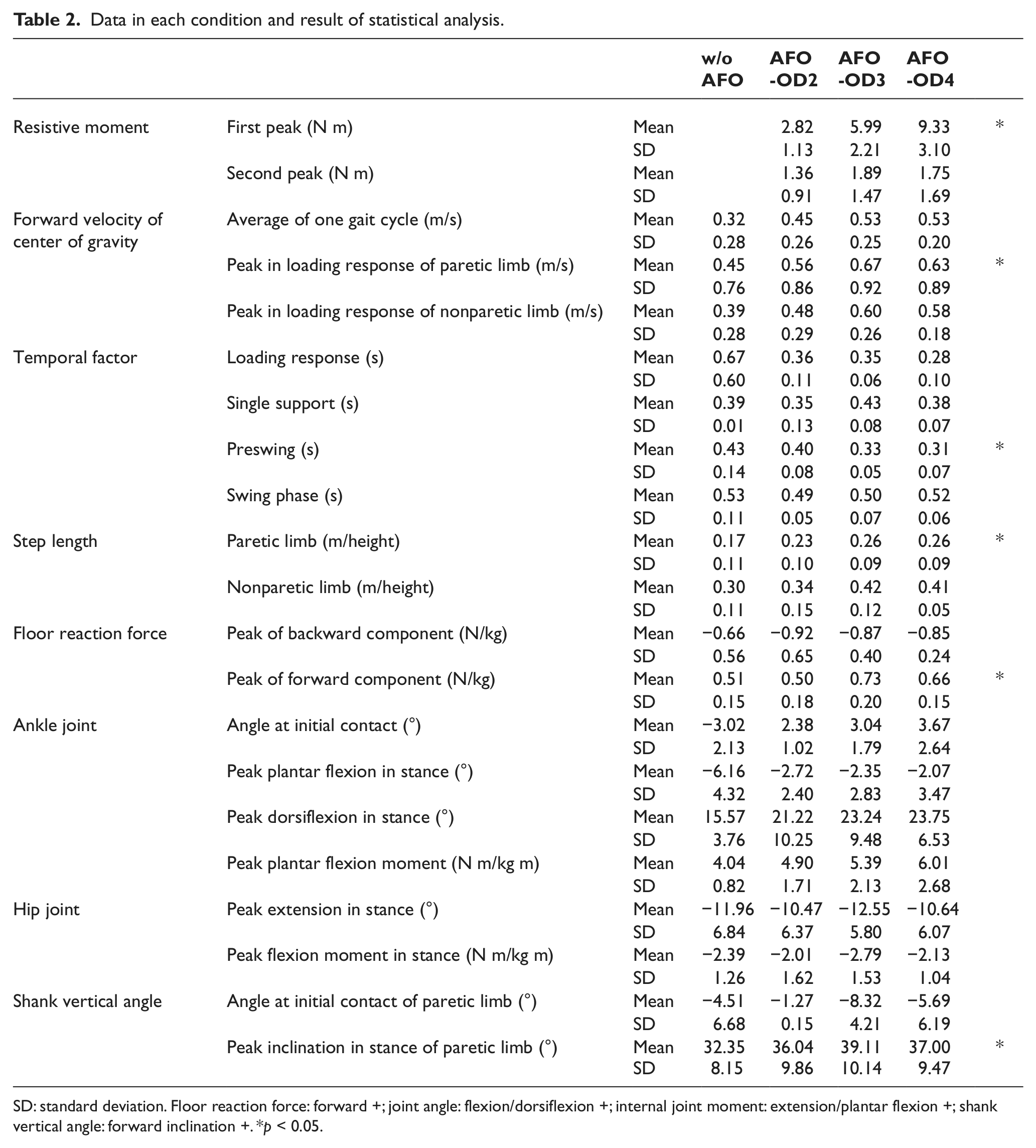
SD: standard deviation. Floor reaction force: forward +; joint angle: flexion/dorsiflexion +; internal joint moment: extension/plantar flexion +; shank vertical angle: forward inclination +. *p < 0.05.
Statistical analysis
The gait parameters were determined and averaged for at least five gait cycles in each of the four gait conditions. For the statistical analysis, step length was normalized by body height, the joint moment by body height and mass, and floor reaction force by the body mass. The peak values of the resistive moment were also averaged in the three conditions of AFO-OD2, AFO-OD3, and AFO-OD4. The number of patients was so small that nonparametrical statistical analyses were performed to exclude the effect of outliers. A Friedman analysis was used to determine which gait parameters were affected by the resistive moment of the AFO-OD. SPSS version 14 (SPSS Inc., Chicago, IL, USA) was used for all analyses, and the level of significance was set at p < 0.05.
Results
The joint moment around the ankle joint when the control subject walked in the AFO-OD3 condition at 1.0 m/s is shown in Figure 2 for one gait cycle starting at initial contact. The ankle joint shows plantar flexion twice in the cycle, so we would expect the resistive moment generated by the AFO-OD to show two peaks during the gait cycle. The first peak occurs during the loading response and the second occurs at the time of foot off. The magnitude of the first peak was less than 10 N m, and it was small compared to the internal joint moment generated by the muscle.
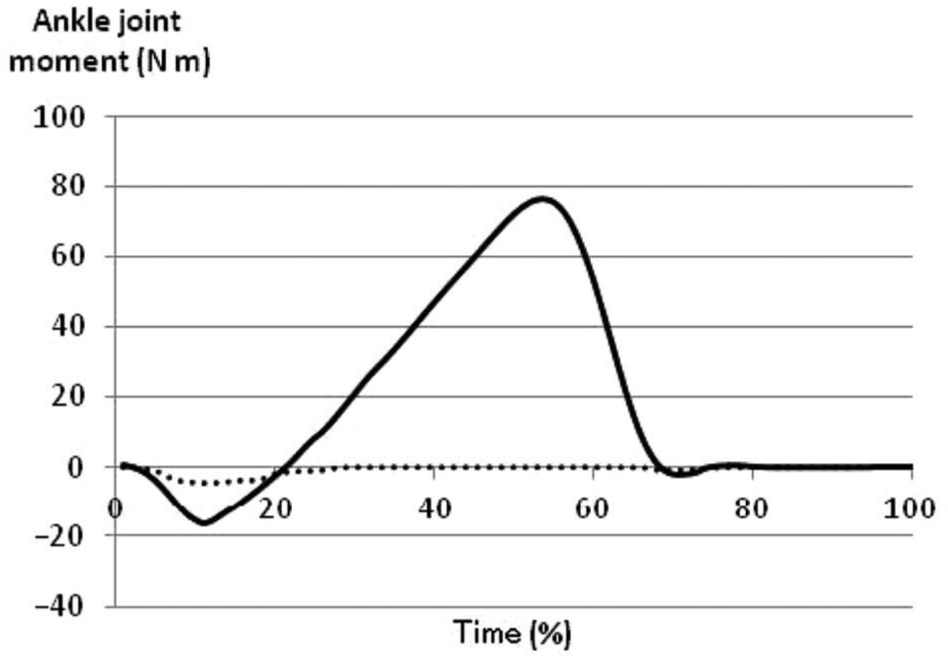
Moment around ankle joint during gait of a normal subject walking at 1.0 m/s. Plantar flexion is positive. Solid line: internal joint moment and dotted line: resistive moment by the AFO-OD.
Figure 3 shows the results of the four gait conditions in the patients with stroke. The peak values of the internal plantar flexion moment were small compared with those of the control subject. The internal dorsiflexion moment in loading response was not found in Patients A–C during the gait without AFOs. It meant that they could not make the heel contact. The AFO-OD started to generate resistive moment just after the initial contact. The first peak of the resistive moment was less than 5 N m in the AFO-OD2 condition but was slightly increased in the AFO-OD3 and AFO-OD4 conditions. The period of generating the resistive moment was longer for patients than that for the normal control.
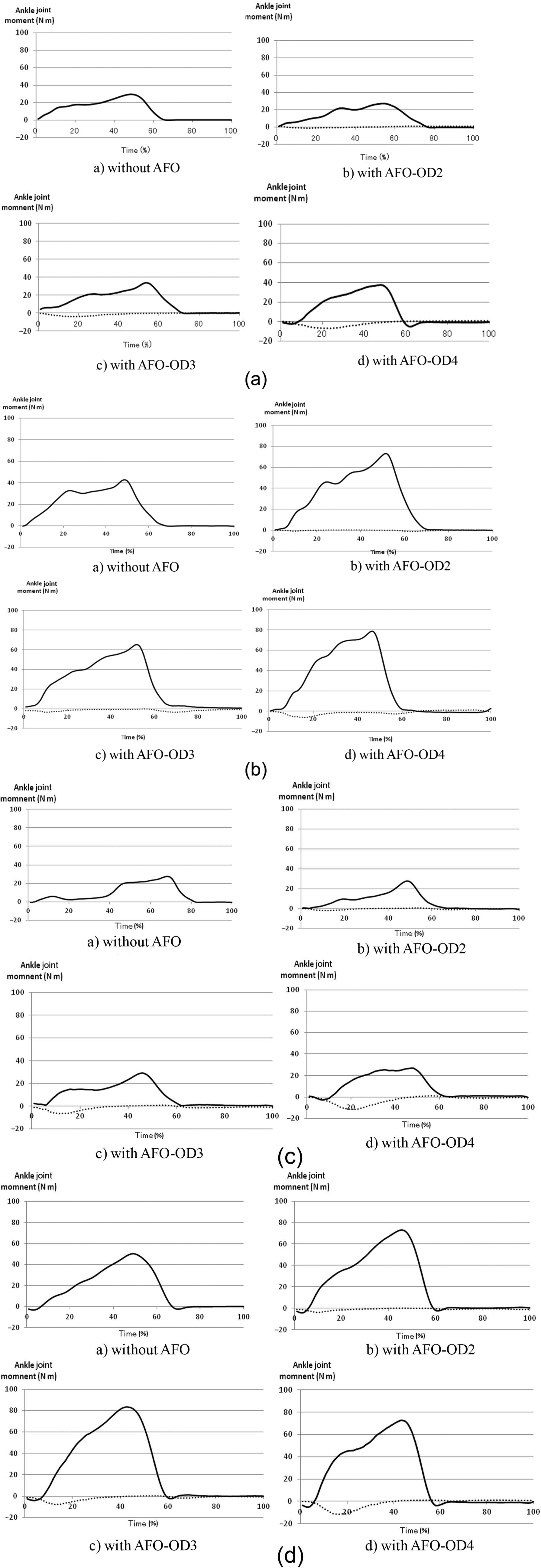
Moment around ankle joint during gait of patients with stroke. Plantar flexion is positive: (a) Patient A, (b) Patient B, (c) Patient C, and (d) Patient D. Solid line: internal joint moment and dotted line: resistive moment generated by the AFO-OD. AFO: ankle-foot orthosis; AFO-OD: ankle-foot orthosis with an oil damper.
All patients selected the AFO-OD3 condition as that with the most comfortable resistance. In the AFO-OD2 condition, stiffness was reported to be insufficient (i.e. too flexible), whereas it was too rigid in the AFO-OD4 condition. Averaged results and the result of the Friedman analysis are shown in Table 2. The number of patients was so small that no pairwise comparison was made. Figure 4 shows the changes in these gait parameters that showed a significant difference between the four gait conditions. The first peak of resistive moment increased in the order of the AFO-OD2, AFO-OD3, and AFO-OD4 conditions in all patients. Both the peak forward velocity of the COG in the loading response and the step length of the paretic limb increased when patients walked with the AFO-OD, while preswing time decreased. Regarding the forward component of floor reaction force and the SVA, three of the four patients showed a peak value when walking in the AFO-OD3 condition, which they reported as providing the most comfortable resistance. The present findings showed that the present hypothesis is valid.
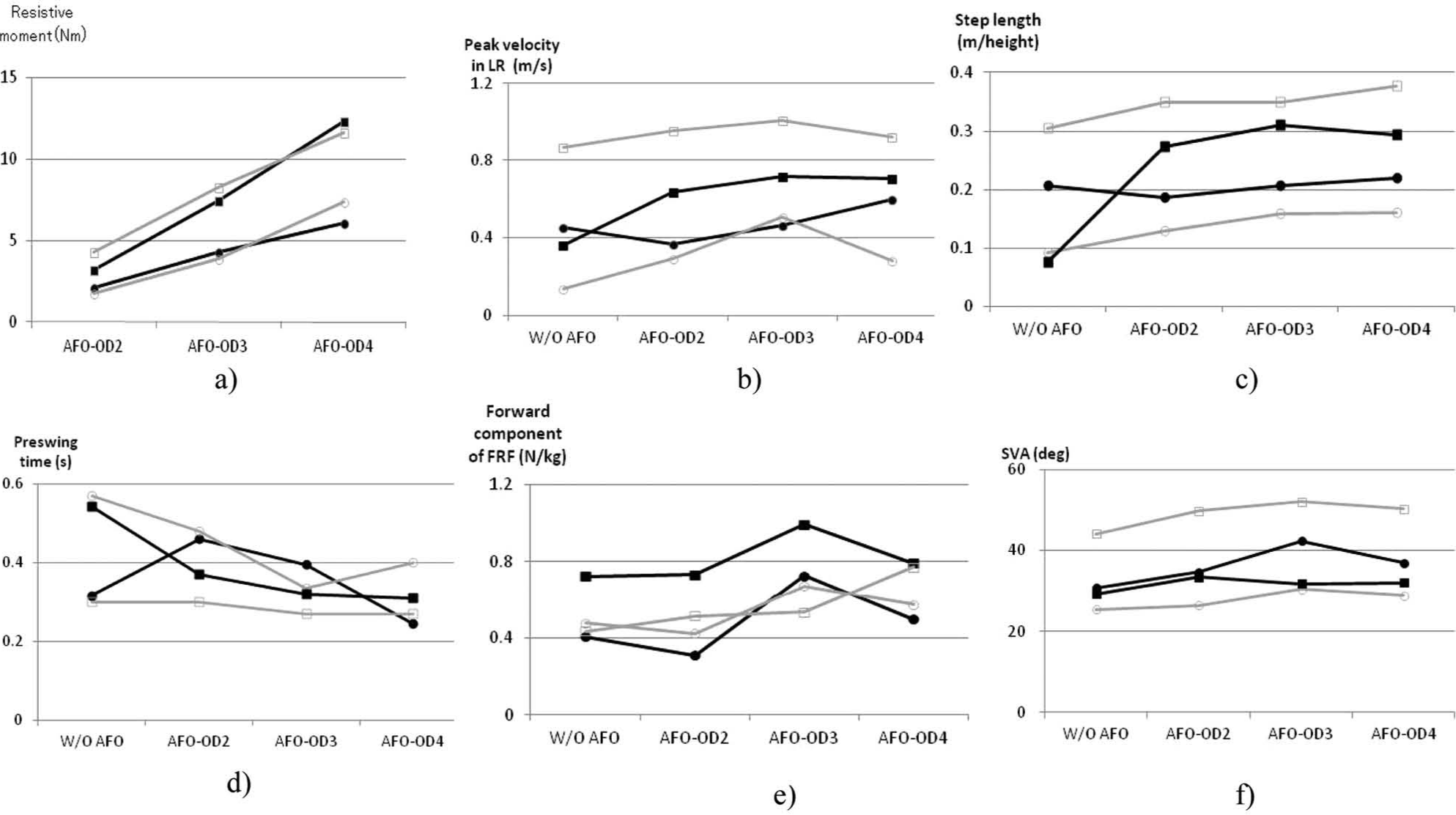
Gait parameter changes caused by the resistive moment generated by the AFO-OD in four patients: (a) resistive moment (p = 0.018), (b) peak velocity in LR (p = 0.049); (c) step length of paretic limb (p = 0.017), (d) preswing time (p = 0.045), (e) forward component of floor reaction force (FRF) (p = 0.019), and (f) shank vertical angle (SVA) in stance (p = 0.038). Patient A: •; Patient B: ○; Patient C: ■; Patient D: □ LR: loading response; AFO: ankle-foot orthosis; AFO-OD: ankle-foot orthosis with an oil damper.
Discussion
The resistive moment generated by the AFO-OD was measured using a specially developed device in this study. Blanchette et al. 24 measured the resistive moment of an electrohydraulic AFO directly during gait in normal subjects, and other studies indirectly measured the resistive moment of AFOs during gait in patients with stroke.15,17 The stiffness characteristics of AFOs have been measured previously, and the resistive moment was estimated using the ankle joint angle of the AFO during gait. This method could not be used for the AFO-OD, however, because the resistive moment of the AFO-OD, which uses an oil damper, depended on not only the ankle joint angle but also the angular velocity. Therefore, direct measurement of the resistive moment was necessary. The measured resistive moment was less than 10 N m, which is in accord with the findings of previous studies.15,17
The Friedman analysis revealed that gait change involved peak forward velocity of COG in loading response, step length of the paretic limb, preswing time, the forward component of floor reaction force, and SVA in stance. The first two are parameters related to initial contact and loading response of the paretic limb, indicating that patients might change their acceptance of the loading by the paretic limb in accordance with the resistive moment of the AFO-OD. The last three parameters are related to terminal stance and preswing of the paretic limb. The AFO-OD was initially designed to assist the first rocker function, but the change was actually found to occur in a later phase in stance. Both the forward component of floor reaction force and SVA showed peak values when the patients reported feeling most comfortable during gait. As shown in Table 2, the SVA angle at initial contact of paretic limb was changed, but it was not significant. It implied that the patients changed the alignment at initial contact in accordance with the resistive moment of the AFO-OD, and it could be related to the comfortable gait. Moreover, the alignment change had the possibility to alter the ankle rocker function and the propulsion ability in stance. Further research will be necessary to clarify the relation between the gait improvement and the patients’ feeling.
An electromyographic analysis using the AFO-OD previously showed that excessive gastrocnemius activity in loading response was inhibited when using the AFO-OD. 21 The present results imply that the resistive moment generated by the AFO-OD affects weight acceptance on the paretic limb and has the possibility to change muscle activity. Although previous studies have shown the effect of the resistive moment of the AFO-OD on the ankle joint angle,18,25 the present study did not show these results significantly. Such a discrepancy could be due to the limited number of patients as well as patient variety, namely, AFO-OD users and nonusers. As shown in Figure 4(a), the first peak values of the resistive moment were different between AFO-OD users and nonusers. This difference had the possibility to affect the ankle joint angle during gait.
There are a number of limitations to this pilot study, which should be addressed in the future full-scale studies. First, the number of patients was small, and thus, there can be no generalization of the results. Second, two of the four patients used the AFO-OD on a daily basis and the remaining two did not, and a previous study showed the importance of being accustomed to the AFO-OD for gait improvement. 20 Consequently, the inclusion of both AFO-OD users and nonusers might have affected the results. Further study including the electromyographic analysis is necessary to determine the general effects of the AFO-OD, and specifically the amount of resistive moment it generates, on the gait of patients with stroke.
Conclusion
A specially designed device to measure the resistive moment generated by the AFO-OD during gait revealed that the resistive moment during gait occurs in the former half in stance and increases in accordance with the resistance of the oil damper. The AFO-OD was designed to generate the resistive moment to assist the first rocker function, but gait analysis results showed that the amount of resistive moment affected gait parameters related to the later phase in stance. Some parameters, such as the forward component of floor reaction force and SVA, showed peak values in the AFO-OD gait condition that patients reported to be the most comfortable. These findings show that although the resistive moment of the AFO-OD is less than 10 N m and smaller than internal joint moment, it still affects weight acceptance on the paretic limb and alters gait in the later stance phase.
Footnotes
Conflict of interest
The authors declare no potential conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.