
Abstract
Background:
Little research has been undertaken into occupational health and safety in the Prosthetics and Orthotics profession.
Objectives:
To identify physical, psychosocial and environmental workplace experiences of Prosthetists and Orthotists in organisational settings.
Study design:
Qualitative methodology, cross-sectional design, using thematically analysed data collected from focus groups.
Methods:
Focus groups explored workplace and work experiences across varied Prosthetic and Orthotic settings. Data were thematically analysed to identify physical, psychosocial and environmental workplace experiences.
Results:
Three major themes, Demands of Work Practice, Impacts on the Individual and Job Design, were identified as problematic. A latent theme Perceptions of Others of P&O highlighted a lack of understanding of the Prosthetics and Orthotics job role outside the profession.
Conclusion:
This first study of occupational health and safety in the Prosthetics and Orthotics profession identifies a number of important physical and psychosocial issues, including characteristics that have been previously identified as risk factors for work-related musculoskeletal disorders. Findings from the study indicate that some Australian organisations lack understanding of the Prosthetics and Orthotics job role, which results in inappropriate expectations of Prosthetics and Orthotics professionals. Preventing injuries and retaining experienced Prosthetists and Orthotists in the workplace is vital for the profession, and as a result, issues raised in this study require further exploration and then development of appropriate management strategies.
Clinical relevance
This is the first study characterising the experiences of work and risk of injuries in Prosthetists and Orthotists. Preventing injuries and retaining experienced Prosthetists and Orthotists in the workplace is vital for the international profession. Issues raised in this study require further exploration and then development of appropriate management strategies.
Background
Occupational health and safety (OHS) for the Prosthetics and Orthotics (P&O) profession has not been well explored, despite anecdotal evidence from clinicians suggesting that they are exposed to a range of hazards, 1 particularly manual handling hazards and others previously linked to the development of work-related musculoskeletal disorders (WMSDs).
Injuries and claims for health-care workers
Research has shown that health-care workers are likely to both under-report injuries and only claim compensation when seriously injured.2–4 Physical and psychosocial risk factors have both been identified for the health-care sector in Australia and internationally, and increasingly in relation to WMSDs with a resultant focus on prevention activities. 5 This ongoing increase in injuries and failure of risk management has been hypothesised as resulting from a narrow focus on only the physical or ‘manual handling aspects’ of tasks,6,7 despite the substantial body of evidence supporting the importance of a systematic risk management approach to address both physical and psychosocial hazards.8–12
Health workers’ musculoskeletal disorder risk factors
Macdonald 6 describes the broader relationship between physical and psychosocial workplace risk factors and workers (see Figure 1). Of central importance to this framework and risk management approach is the potential imbalance between the demands of work and an individual’s coping resources, with a subsequent increased risk of WMSD development. The risk factors related to relationships between physical and psychosocial factors, and WMSD development, have been identified and characterised within a range of occupational groups including health professionals.8,13
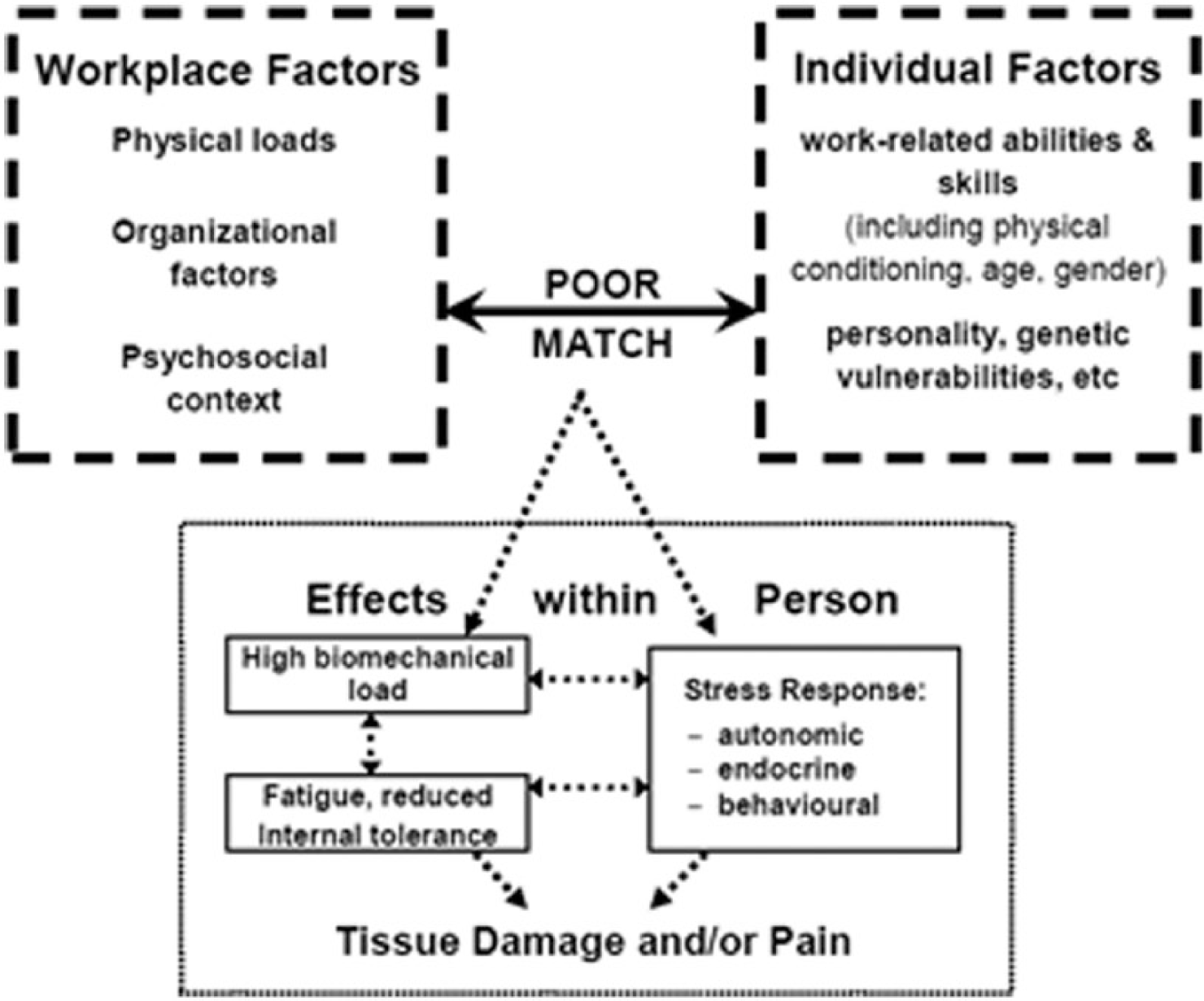
Model of causation for MSD: 30 the relationship between physical and psychosocial workplace risk factors and workers.
Research focussed on paramedical and allied health professions including nurses and physiotherapists 14 has reported rates of WMSD ranging from 57% to 91% of clinicians in United States and Australia, respectively.14–17 In physiotherapists, high rates of WMSD have been linked to both physical and cognitive workplace demands. 18 Among nurses, the WMSD risk management focus has been on reducing patient-handling manual handling risks, a strategy which post intervention research suggests has limited success. 19
P&O workplace risk factors
Neither OHS risks more generally nor those related to WMSDs have been explored in the P&O profession. While P&Os share many risk exposures with other Allied Health professionals such as Occupational Therapists and Physiotherapists, a key difference in the role of a P&O compared to other Allied Health professionals is their exposure to the combination of clinical and manufacturing environments, and exposures to a range of hazards during the fabrication of orthoses and prostheses. Tools used to assess more traditional aspects of health-care work-risk need modification to ensure that issues specific to both the technical and clinical aspects of the P&O profession are included, particularly if P&Os identify unique experiences when characterising their work demands.
P&O development as an allied health profession
The development of the P&O profession in Australia provides important context to OHS issues for contemporary clinicians. P&O is a relatively new allied health profession, which has developed over the past 40 years from an apprenticed trade to a tertiary undergraduate Diploma, Degree and now Masters qualification. 20 While the professional status has developed significantly over this time, practitioners continue to work in clinical, technical and workshop-based environments.
Characterising P&O workplace risks
The combination of previously identified allied health practitioner risks, exposures to manufacturing-related hazards, and the dearth of research into health and safety issues related to P&Os underlines the necessity for detailed characterisation of the P&O work environment to inform the development of effective and appropriately targeted risk management interventions. This study aims to identify the physical, psychosocial and environmental workplace experiences of P&Os in organisational settings to address this knowledge gap.
Method
Participants
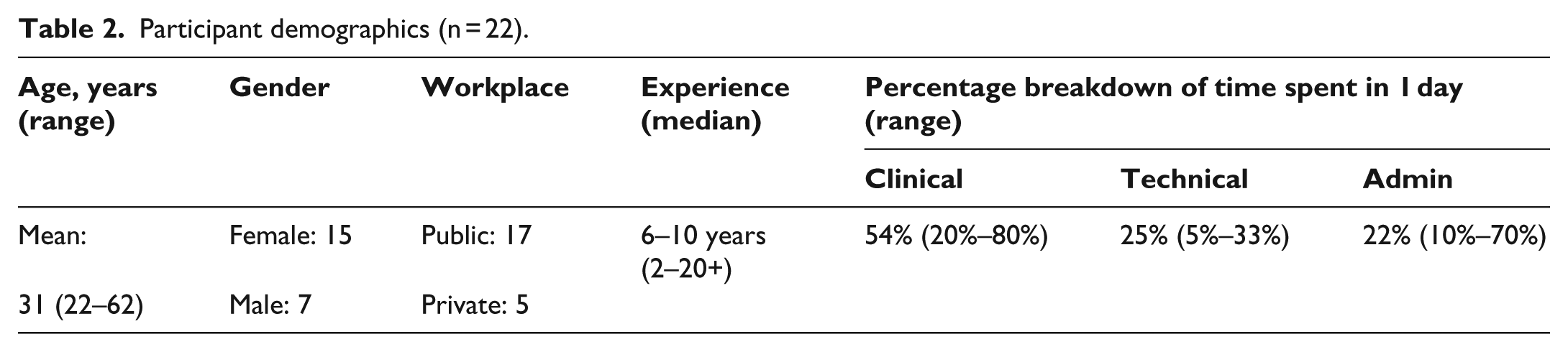
Participants were recruited for focus groups through email newsletters circulated by the Australian Prosthetic and Orthotic Association (AOPA), to all members residing in Victoria and South Australia. (See Table 1: Inclusion and Exclusion criteria.) A total of 22 (15% of the relevant membership base) people agreed to participate and provided informed consent. Membership of AOPA is as a condition of employment in most clinical environments, and as such, the recruitment strategy reached most practising P&Os. Summary participant demographics are shown in Table 2.
Participant’s inclusion and exclusion criteria.
P&O: Prosthetist and Orthotist.
Participant demographics (n = 22).
Research design
A qualitative cross-sectional research design was selected to explore P&Os’ experiences of work in the workplace and across a variety of occupational settings.
Focus groups were used to facilitate an improved understanding of the specific P&O field and increase the relevance of research.21,22 Thematic analysis of focus group data was used to build concepts and categorise the resulting themes.
Data collection
Four focus group sessions were conducted with a total of 22 participants (15 females, 7 males), three sessions in Victoria and one session in South Australia to identify potential state-based differences in work environments to that of Victoria. The P&O workforce is spread across Australia, with the largest proportion of P&Os located in Victoria, 45% of the total 276 AOPA members. South Australia has 20 (7%) of AOPA members and was selected to identify any differences between Victoria and states with lower representation of P&Os.
Focus group questions (supplementary material Appendix 1) were developed based on Macdonald’s (2003) conceptual framework and relevant literature. Questions related to the following areas were included:
Job demands (quantity, intensity, timeframes, physical and mental requirements);
Coping resources (support, feedback, enjoyment);
Other psychosocial characteristics (autonomy, support, job security).
The focus of the questions was not individual experiences of work-related injury or ill health as the aim of the group forum was to identify a comprehensive range of work and workplace demands.
All focus groups were facilitated by the researcher and moderated by an experienced independent observer to ensure consistency and clarity. A research log was kept by the primary researcher to assist reflexivity. As this researcher was a P&O, it was particularly important to recognise and address the potential for bias resulting from their background, perceptions and experiences. In addition to this strategy, the moderator and two members of the research team were from outside the P&O field, thereby ensuring that the experiences and expectations of one P&O researcher were counter balanced and the data analysis and results were truly reflective of the described experiences.23,24 The use of guided questions within the interviews and an independent moderator also assisted in reducing bias and subjectivity data collection. 24
Ethics approval for this research was obtained from La Trobe University Human Ethics Committee. Approval was obtained from the Australian Orthotic and Prosthetic Association for invitations to be circulated among P&O clinicians in Victoria and South Australia.
Analysis
Sessions were recorded, transcribed verbatim, and de-identified prior to analysis. Qualitative thematic transcript analysis was conducted, and NVivo 10 software was used (QSR International Pty. Ltd) to assist with data management. Line by line thematic analysis was undertaken to identify concepts. Using a process adapted from Liamputtong, 25 concepts were coded within NVivo in a node structure and then themes and subthemes were derived. Following the analysis of three focus groups, no new themes were identified and data saturation was reached; thus, an ideal sample size had been obtained. 26 All data were analysed twice by the researcher and reviewed by the moderator to maximise coding accuracy. Consensus was reached through multiple inductive processes applied to the data analysis, including repeated thematic analysis of the data by the researchers and the independent moderator, and repeated coding and recoding, all contributing to the development of concepts and theories from the data. 27 The resultant themes identified the major concepts expressed within the interviews.
Results
Three major themes were identified: Demands of Work Practice, Individual Impacts and Job Design, with a latent theme, Perceptions of P&O, underpinning elements within all major themes (see Figure 2). Perceptions of P&O highlighted particular challenges reported by participants in relation to others’ understanding of their role, and how this impacted a range of other identified experiences.
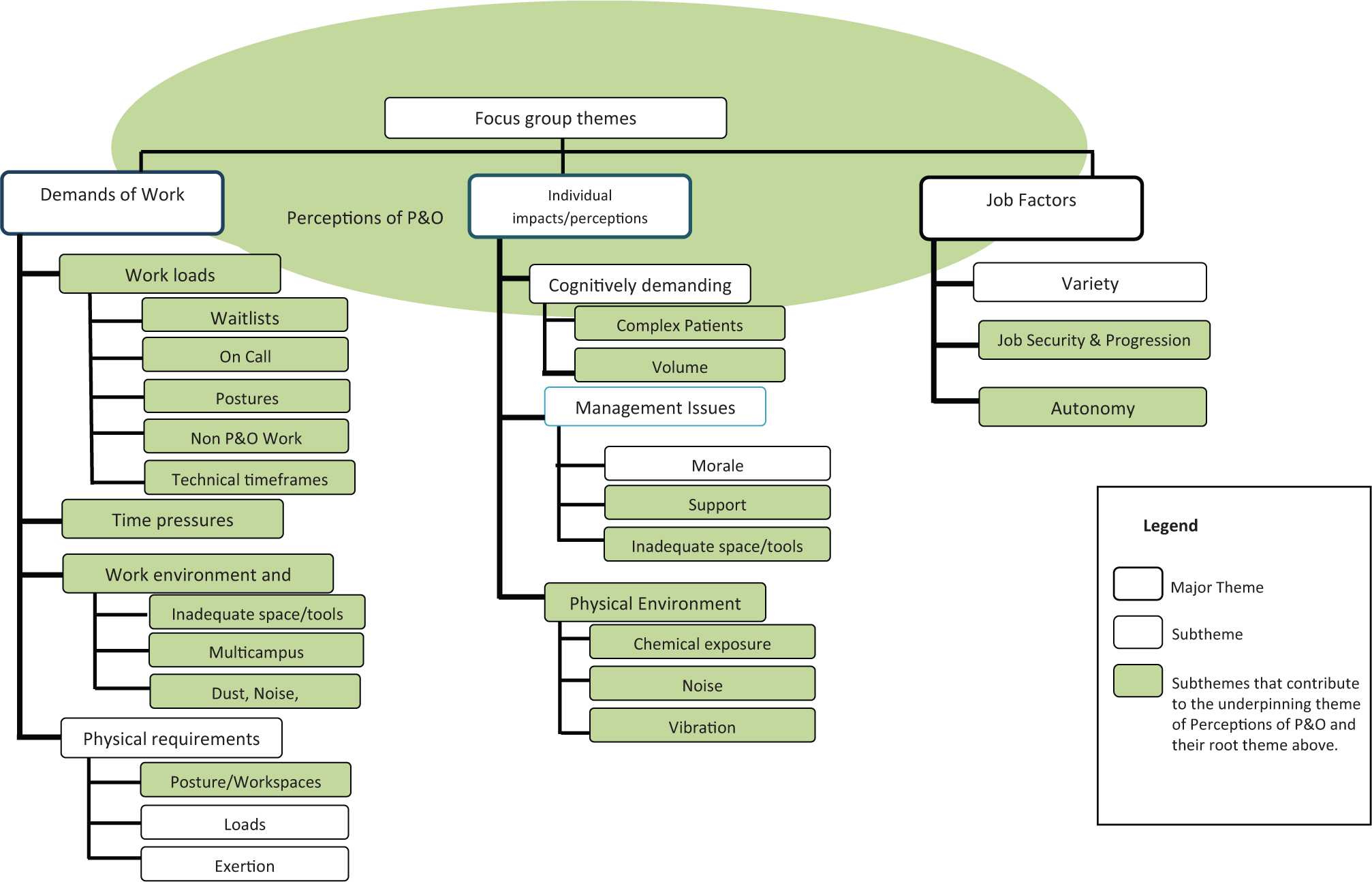
Focus group thematic diagram.
The Demands of Work Practice theme incorporated elements classified as a hazardous job or task demands, with subthemes of workloads, time pressures, work environment/location and the physical requirements of the P&O job. The theme Impact on Individuals included three subthemes: cognitively demanding aspects of the P&O job role, management issues impacting the individual and physical environment impacts. The final theme, Job Design, incorporated the subthemes variety of work, job security and autonomy.
Perceptions of P&O
The poor understanding of the nature of the work undertaken by a P&O emerged as an important, latent and underpinning theme. Other health professionals were unclear about the dual practice role combining a client focus and a manufacturing role: ‘At the beginning we all said we loved the joint technical/clinical aspect of it, but try blending the technical and clinical in a hospital setting where they’re just set up for clinical’ (Mark).
Participants indicated that this role misconception resulted in other health professionals setting unrealistic service deadlines, or providing misinformation to patients on timing related to the delivery of devices, thus placing unreasonable demands on practitioners in terms of pacing of work: ‘There is just no appreciation of … the back work that goes into what we actually give people and how long this takes. We can’t whip it up in half an hour yet that’s the impression they [Doctors] give’ (Carol).
Participants reported that management also had a poor understanding of P&O, and in particular, the manufacturing component of the role. This limited understanding resulted in practical problems that included allocation of inappropriate manufacturing work environments: There is just a lack of awareness about what we actually do that produces these situations where someone designs a department and says yep, you’ve got four meters of corridor to do your gait assessment in, but you actually need forty metres … (John)
These misconceptions appear to be specific to perceptions of the P&O professional group and arise because of their complex roles as practitioners/clinicians and manufacturers working alongside more traditional clinicians.
Demands of Work Practice
Unlike other allied health professionals, the role of a P&O involves activities within a workshop environment, including exposure to hazardous materials, machinery, extraction units, high temperature ovens and poorly designed workspaces that are too small with insufficient airflow (Figure 3): ‘Our environment … is way, way too small for the amount of people and the type of work that we’re trying to do … (results in) not being able to get access to the space and the tools’ (Helen).
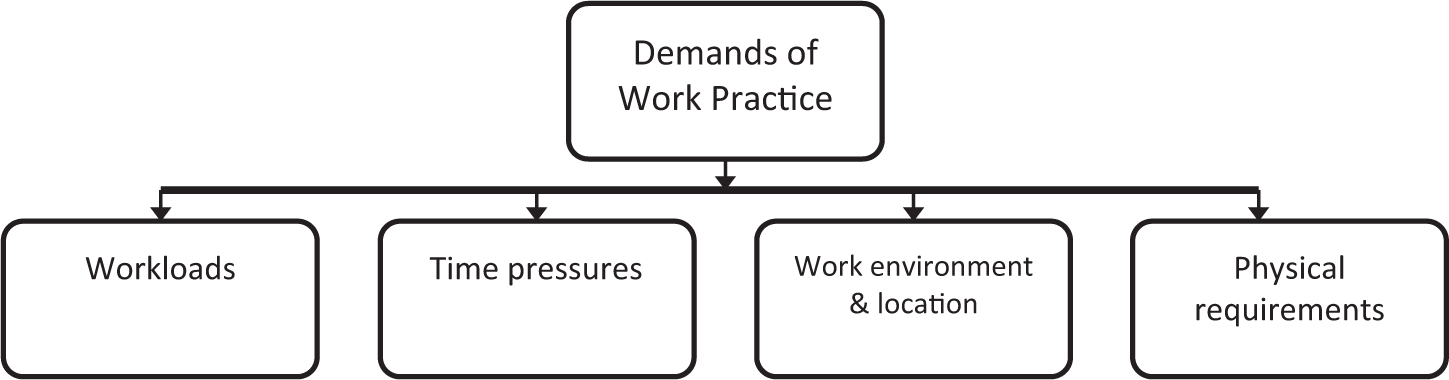
Major subthemes of Demands of Work Practice theme.
Limited space was consistently reported in all focus groups, with subsequent issues accessing tools and machinery.
Work environment and location
A range of characteristics in the physical environment was identified as barriers to productivity including the location of departments and access to windows for natural light, ventilation and airflow: ‘One of the worst things is our environment, actually, where the office is. We did have a nice view onto our park, then they blocked off our windows because we’re a bit of a messy department, in their opinion …’ (Julie).
The workshop environment includes exposure to background noise from extraction fans and more acute sounds from compressed air and pneumatic drills: When there are less people in the department the noisy machines are just not on as much … we get to the end of the day and we all talk about it [the noise] … I go home feeling more relaxed on days when everything [noisy machinery] hasn’t been on as much. (Julie)
Concerns around high levels of dust and poor air quality were identified: I just get sick of dust that’s everywhere, and you’ve got to always blow stuff down. I know there’s no solution to it, but it is a frustration of mine, tedious and you wonder what it’s doing to your health, long-term … (Cooper)
Dust was identified as both an individual exposure issue and a concern regarding Management’s OHS responsibilities for hazard controls. Concerns regarding the impact of exposure to dust and other airborne particles on individual’s short- and long-term health were frequently discussed: ‘The thing that I worry about most is the atmospheric OH&S risk that we suffer from. So, be that constant noise or fumes or dust or whatever, the things that are in our department that we don’t necessarily see’ (John).
Physical requirements
The poorly designed physical environment resulted in excessive and unreasonable postural demands: You still find yourself sitting on the floor and putting yourself in strange positions to adjust things. We do occasionally get extremely large people that go beyond the capabilities of our department. We need slings and things like that to lift those [people]. (Helen)
While participants understood what they were doing was not ideal for their health, other imperatives such as time requirements and wanting to ‘get the best cast’ were identified as reasons for putting themselves in these often risky situations.
Workloads and time pressures
Most participants identified concerns related to workload and short deadlines. Related experiences included unpredictable peaks and troughs in their workload demands and other time pressures outside their control: ‘I often think that if I could just fit an extra day between Tuesday and Wednesday, and with all other staff away, I might be able to get to it but it never happens’ (Kim). A sense of being overwhelmed was another common report: ‘You’re just never going to get through it (the work), and you’re sick of it. You want to go home’ (Cooper).
Some participants outlined their strategies to manage what they felt were often-overwhelming workloads: I … favour the patient treatment side of things and postpone all the administrative tasks, which there are a lot of. So I guess, administrative tasks, quality projects and research all get put on the backburner a lot of the time. … which again increases my overall inefficiencies and feeling that I can’t actually get it all done. (Louise)
Working on-call and outside regular hours were identified as negatively impacting participants’ home life and mental health. Participants reported a feeling of not being able to ‘switch off’ or constantly working which contributed to the perception that workload was out of their control.
Broader systemic characteristics negatively impacted time demands including matters related to payment systems and other demands beyond an individual P&O’s control: We’re across wards, we’re across disciplines, we’re across all the units and then you think you’re under control and then three things come out of left field and then you’re just. … – the inability to plan kills me, every day. (John)
Mismatches between work demands and resources particularly in the areas of scheduling, staffing and time management were identified as being of particular concern: I think it’s more mentally exhausting than physically exhausting. In my workplace there are days when you do a big session of tech work and you will be physically tired. Or days when you are seeing 12 patients on the ward then it’s easy it does take a toll but it’s more mental exhaustion than physical I would say. (Andrew)
Staffing resources (quantity and consistency) were identified as impacting on both quality of service provision and work satisfaction: Staffing levels become frustrating because not only are you overworked but you also know that the department can’t meet the needs of all our clients, because they’re on a waiting list for months and months they have to lie flat on their back in bed for an extra 48 hours or whatever it might be. (Nicolas)
Impact on Individuals
Management issues
Participants identified a number of issues relating to both their personal and work management, including poor morale and inadequate support and resources (Figure 4). Discussions related to funding for devices and other services with clients were identified as uncomfortable for P&Os, especially when this impacted the quality of service delivery: With some of the systems you’ve got to wait so long for funding to be approved. That can be frustrating when people need things quickly and also the time that they’ve got to wait between your first assessment and their actual supply, things can change quite a lot and what you’ve applied for funding for might not be appropriate any more. (Debra)
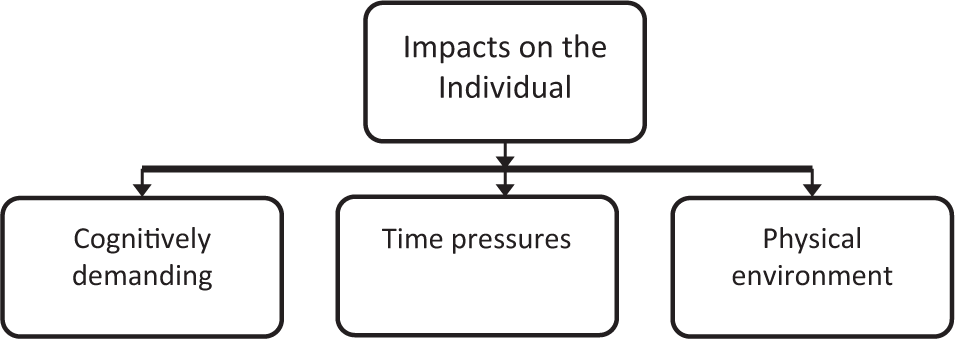
Major subthemes of Impacts on the Individual theme.
A range of administrative issues were raised which included managing buildings requiring modifications and the ‘red tape’ associated with purchasing even very basic equipment such as a dustpan and broom. These resulted in participants feeling their work was undermined by ‘higher up management issues’ (Nicole).
A common thread emerged in relation to a lack of management support and the lack of constructive feedback: You hear about when you do the negative performance or that brace that wasn’t quite a good fit. Then you get pulled into the manager’s office and [told] why is this wrong, what can you do better, how about we correct … it’s never said the other way, or not often enough. (Prue)
Cognitive demands
Addressing challenging and complex patient problems was identified by participants as an extremely satisfying part of the role. However, this could also be a negative factor: ‘Frustration when you just can’t get something right and you’re banging your head against the wall. It’s that issue where you look at the problem so long you can’t see the problem for what it is anymore’ (Emma).
Inadequate time to deal with complex patients was an issue: … when you’ve got quite a complex patient, and you’re having to find solution after solution after solution, just to make an alignment work, and then something happens and then something else happens and then there’s a fit issue because it’s changed. (Kim)
Job Design
Autonomy
Autonomy was frequently discussed in relation to workload and time pressures (Figure 5). An autonomous work environment was viewed as both a positive and negative factor. P&Os with higher levels of autonomy in their work, including what they did and how this was scheduled, felt more in control of their workplace situation and reported reduced time pressures. However, they also reported they often saw extra patients and extended their workday to meet deadlines: I’m booked out for three weeks, that’s fine. By the way, you need to go to this meeting about stats at 12 o’clock on Wednesday, and on Friday, you’ve got this on. … so I now have to squeeze that in, and I’ve told this patient, and Mum’s taken the day off work to bring them in, so I’ll squeeze them in around that. I’ll do that, and that’s okay. They’re all squeezed over lunchtime. So, that’s a real time pressure for me, the constant very short notice. (Matilda)
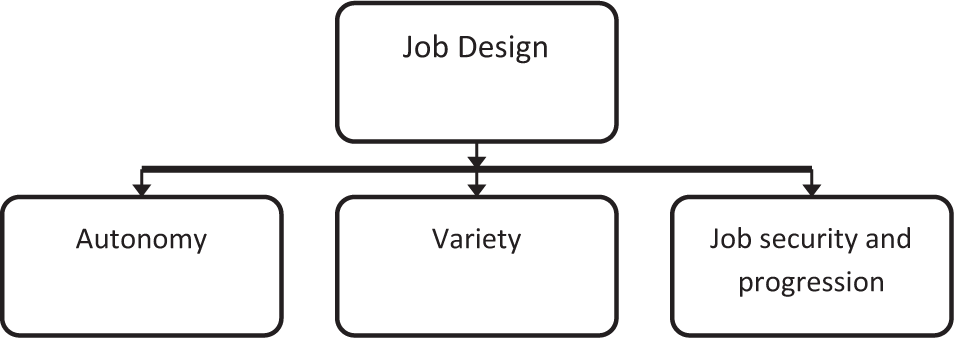
Major subthemes of the Job Design theme.
Variety
Focus group participants reported both positive and negative responses to high levels of job variety. One participant indicated that variety was instrumental to retaining interest in the job: ‘Fitting off the shelf CAM walkers can become boring and lack variety … I really do enjoy the problem solving side of the job’ (Nicole).
However, dealing with a range of conditions was cognitively challenging due to complex decision demands: ‘… It’s just a lot of mental problem solving and often those are the times when you forget to have morning tea, or you get a ten minute lunch …’ (Kim).
Participants identified a combination of low autonomy and low variety as an issue. Being able to alternate mundane tasks and more enjoyable tasks was seen as a coping strategy: ‘You’ve got x amount of workload to do so you’ve got to get that all the way done, so you can’t do … another part your interested in …’ (Harry).
Career advancement
Respondents reported good opportunities for career advancement in P&O for approximately 5 years during which a lack of experienced staff and recruitment challenges enabled relatively easy movement up through clinical grades: ‘At the moment I think there’s a very low ceiling so you can reach the top very quickly. I feel there are lots of inexperienced people in higher level positions currently’ (Louise).
However, these opportunities then quickly diminished: ‘I am 30 years old and I am maxed out at Grade 3, I have no job progression from here if I want to stay here working clinically’ (Harry).
This was identified as a significant skill retention risk for both individuals and the broader profession: There’s not those opportunities that you get in many of the other professions. But you can always do another degree and move into management in many areas, or use your expertise along with another degree and move sideways somewhere else. (John)
Most participants indicated an intention to leave the P&O profession within the next 15 years, to seek more challenging work: … I feel as though I’ll continue to work ‘til maybe 35 and then get sick of it. I can’t go in any other direction, so I’ll do something else. Just when I think about my future and what I’ll be doing in 15 years, I imagine that I just haven’t got anywhere to go to keep me interested and challenged. (Cooper)
Job security
Lack of access to reliable and ongoing government funding was identified as a stressor, with funding restrictions undermining job security and the ability to provide timely and quality service. Significant investment in training and retraining staff as a result of this short-term funding was a source of frustration for clinicians and a cyclical problem at department level. When funding was available, clinicians were able to work in environments with sufficient staff, reduce waitlists, and have reasonable workloads across the department: X was just offered one year because of funding issues. It was very stressful for him because at the end of that one-year he was instructed to just keep turning up to work. He kept turning up and we kept paying him to turn up even though he didn’t have a contract, he was out of the contract. He got another 12 months out of that. (Nicolas)
Discussion
Workplace characteristics reported by participants suggest that within the P&Os’ work and work environment there are physical and psychosocial hazards and risks that have been previously linked to the development of injuries including WMSDs in other allied health workers. Oakman et al. 1 describe WMSDs’ risk factors that include inadequate job design and physical and psychosocial demands impacting an individual’s ability to both undertake their job role and maintain their physical and psychosocial health.
Demands of Work Practice
Within the P&O context, the Demands of Work Practice theme and subthemes reflected risk factors described in Macdonald’s 6 model of hazardous Job and Task demands. Excessive workload combined with time pressures for completion, or work with a high physical load and insufficient rest, results in high levels of fatigue and stress creating biological responses increasing the risk of injury including WMSD. 9 P&Os identified that the pressures placed on them by other health staff and patients not only increased their workloads, it also resulted in unrealistic time pressures to complete tasks. One strategy to address this issue is to educate others on the role of a P&O and the requirements to complete tasks to ensure that expectations are more realistic.
Individual impacts
Macdonald’s 6 model describes the risks related to an imbalance between workplace demands and an individual’s coping resources, imbalances reported as experienced by P&Os. For example, high workloads combined with unreasonable timeframes are likely to lead to a stress response, high fatigue levels and other physiological changes – a ‘hazardous personal state’, and subsequently an increased risk of injury. This supposition is further supported by Karasek’s model of control and demand, in which a job or task that has a high demand and low control can lead to an anxiety or stressed state developing. 28 This may be compounded by factors such as constant noise in the workplace, insufficient management support and not having the right tools or access to the tools required to perform your job to your best ability, all of which can impact the P&Os coping resources and in turn lead to an increased risk of injury development.
Job design
Our results suggest that for P&Os, Job Design is a standalone theme of equal importance to the other main themes, Demands of Work Practice and Individual Impacts. Work design, which includes autonomy, responsibility and variety, has been shown to reduce boredom and is therefore likely to reduce a number of work characteristics that potentially impact the individual and the demands of the work.6,9 For P&Os, two major job design concerns are job advancement and security, and the majority of participants reporting feeling there was little opportunity for professional advancement beyond the age of 30 years or after 9–10 years of work. The most effective way to address these issues is by the use of multifactorial preventive interventions that address physical and psychosocial hazards at multiple points within a person’s career. These should include strategic interventions during training and education, in workplace environments, through organisational systems, and education of other Health Professionals and patients. 1
Limitations
The Victorian location of the majority of the focus groups could suggest a regional bias, a concern that was addressed by conducting one focus group in another jurisdiction. The sample size for these focus groups was considered to be appropriate, as sample sizes for qualitative research are considered to be one that is obtained by interviewing until there is no emergence of new themes, data saturation being reached. 29 The focus groups did not include or exclude people based on their individual injury status, and participants were not asked to comment specifically on any current or past injuries or illness. As such, the findings are not specific to hazards that directly related to the development of work-related injuries or illnesses including WMSD, but rather to issues within the total P&O work and work environment identified by the participants as impacting their general health and well being.
Internationally, models of education and workplace design differ from the Australian experience that may undermine the application of these findings to some other countries. However, most tasks including the clinical and technical ‘dirty work’, undertaken by P&Os in most developed countries have similarities to those of Australian P&Os. Regardless of work location and context, the issues raised by the focus group participants in Australia are likely to resonate with other P&O practitioners.
Conclusion
Three major themes, Demands of Work Practice, Impacts on the individual and Job Design, were identified as problematic within the P&O workplace. A latent theme, Perceptions of Others of P&O, highlighted a lack of understanding of the P&O job role outside the profession. This first study of OHS in the P&O profession identifies a number of important physical and psychosocial issues, including characteristics which have been previously identified as risk factors for WMSDs. Findings from the study indicate that some organisations lack understanding of the P&O job role, which results in inappropriate expectations of P&O professionals. Preventing injuries and retaining experienced P&Os in the workplace is vital for the international profession; therefore, issues raised in this study require further exploration and then development of appropriate management strategies.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Australian Orthotic and Prosthetic Professional Development Grant.