
Abstract
Background:
Although an orthotic device of the lower limb improves the functionality of neurological patients, anecdotally clinical experience suggests that the compliance is rather limited.
Objectives:
The aim was to determine the satisfaction and acceptance of a lower limb orthotic device.
Study design:
A qualitative observational pilot study with a mix-method design.
Methods:
Adult neurological patients who had a prescribed lower limb orthotic device were included. One published and clinically used questionnaire about satisfaction (D-Quest) and one ad hoc constructed questionnaire about acceptance of the orthotic device (MIRAD-ACCORT questionnaire) were used for data collection.
Results:
In total, 33 patients participated (28 ankle–foot orthotic device, 3 knee–ankle–foot orthotic device and 2 other types). In general, they were satisfied about their orthotic device and the services. Less than one-fourth of the patients had some negative comments about the ‘visual aspects’ and the ‘ability to hide’ of their orthotic device. These, however, had a lower priority when compared with functionality, which was reported as a main advantage and is a reason for continuing the use of their orthotic device.
Conclusion:
Patients were satisfied in relation to their lower limb orthotic device. With regard to acceptance, it can be concluded that factors associated with functionality and comfort are more important than the aesthetic and psychological aspects of the orthotic device.
Clinical relevance
Patients were satisfied with their lower limb orthotic device. Some patients had some negative comments about the ‘aesthetics aspects’ and the ‘ability to hide’ their orthotic device. However, improvements in functionality were mostly reported as a main advantage and a reason for continuing the use of their orthotic device.
Background
An orthotic device (OD) is a device that is externally applied to the body to support, align or correct deformities, or to improve the function of a part of the body. 1 Orthotic care includes patient evaluation, fitting and modification of the OD. These devices are used as aid for patients with movement impairments, mostly neurological patients (e.g. multiple sclerosis (MS) patients, spinal cord injury, stroke and cerebral palsy)2,3 but also patients with musculoskeletal disorders (e.g. Duchenne muscular dystrophy, patellofemoral pain syndrome and rheumatoid arthritis)4–6 and orthopaedic injuries (e.g. knee osteoarthritis and anterior cruciate ligament reconstruction).7,8 The use of OD facilitates the continuation of the patients’ participation in their social environment or other activities. 9
Patients with a too complex or non-aesthetic OD often do not use them at home, which is a financial loss to society and a loss of therapy value. 10 Depending on the type of OD, 6%–80% of the patients did not use their prescribed OD for the lower limbs or orthopaedic shoes at all.11–16 This percentage was lower for orthopaedic shoes compared to the other devices. It seems that when patients are able to manage without the OD, they are not using them. 16
User satisfaction is believed to be a predictor of the frequency of wear as well as the long-term use of the OD.17,18 In these studies, user satisfaction was defined not only by the usability of the OD but also by the costs of the devices and support services.17,18 Patient satisfaction is recognized to be important in the management of assistive devices and in the evidence-based health care in general.17,18 Until now, there have been little attempts to develop patient-reported outcome measures concerning OD.17,19
Clinicians, researchers and constructors can improve the OD according to the satisfaction data and the complaints of the users, such as cosmetics, self-image, pain, the fit of the device, poor level of function and interference with activities. 20 Understanding user preferences increases the use and efficacy of the OD and thus creates a greater patient compliance.17,18,21
In this work, we aimed, by using two questionnaires (one published and clinically used questionnaire and one ad hoc constructed questionnaire), to investigate the extent of satisfaction with the OD of the lower limb in neurological patients and to enquire the most important reasons for acceptance of this OD.
The research questions of this study are as follows: (1) how satisfied are neurological patients with their OD of the lower limb? and (2) what are the most important reasons for acceptance of a lower limb OD in neurological patients?
Methods
Participants
Patients were recruited in two rehabilitation centres by medical doctors and physiotherapists.
Adult patients with neurological diseases who had a prescribed OD of the lower limb (a lower limb externally applied device to support, align or correct deformities, or to improve the function) were included in this study. They met the inclusion criteria if they had at least one OD prescribed for the lower limb. The patients had to be cognitively able to understand and answer the questionnaires.
All patients signed an informed consent form prior to the start of the interview. This study was approved by the university ethical committee and the local ethical committees of the rehabilitation centres.
Questionnaires
Two questionnaires, one published and clinically used questionnaire about satisfaction (D-Quest) and one ad hoc constructed questionnaire about acceptance of the OD (MIRAD-ACCORT questionnaire), were used for data collection. The questionnaires were used to organize the semi-structured interview. Two researchers interviewed the patients by reading out the questions. The mean duration of this semi-structured interview was 25 min. In the first part of the questionnaire besides demographical and anthropometric data (e.g. age, height, weight), information about their disease (e.g. type, time after diagnosis) and OD (e.g. type, duration after prescription) were also collected.
D-Quest 2.0
To measure the patients’ satisfaction of their OD, the D-Quest was used.18,22 This questionnaire is a Dutch version of the Quest 2.0.18,23 A description of the questionnaire could be found in the publication of Wessels and De Witte. 22
MIRAD-ACCORT questionnaire
The MIRAD-ACCORT questionnaire is a novel five-part questionnaire constructed to measure the reasons for acceptance of a lower limb OD. This questionnaire was developed within the framework of a project that aims to bring intelligent robotic assistive devices to the user (integrated Methodology to bring Intelligent Robotic Assistive Devices to the user – MIRAD).
In part 1, the question is as follows: ‘With regard to your OD what is your opinion about: “visual aspects,” “used materials,” “ability to hide,” “affordability,” “ease of use,” “comfort,” “firmness and functionality”?’. The answer possibilities were on a 5-point Likert scale: ‘very bad’, ‘bad’, ‘not bad/not good’, ‘good’ and ‘very good’. A sixth answer possibility was ‘not applicable’.
Part 2 focuses on the advantages and disadvantages of the OD. This part consists of two open-ended questions asking what the main advantages and disadvantages of the OD are for the patient.
In part 3, the different aspects used in part 1 were clustered into two groups with the following common properties: (1) aesthetics and financial cost and (2) usability. The first cluster includes ‘visual aspects’, ‘used materials’, ‘ability to hide’ and ‘affordability’; the second cluster includes ‘ease of use’, ‘comfort’, ‘firmness’ and ‘functionality’. Each aspect of Cluster 1 was placed next to each aspect of Cluster 2. For each combination, patients were asked to make their choice between the two aspects or answer that both aspects are of equal importance.
Part 4 is about the reasons not to use the OD anymore. The question is as follows: Are the following aspects a reason for not using the OD anymore: (1) not a nice view of the OD; (2) none or not enough functional improvements; (3) difficult to use; (4) OD leads to pain and discomfort; (5) OD gives you the feeling of being handicapped and (6) OD gives you the feeling that others see you as disabled.
The answer modalities were ‘yes’ or ‘no’.
The last part, part 5, of this questionnaire was an open-ended question: ‘What would you change about the OD if cost and feasibility were not important?’.
Data extraction and analysis
A descriptive analysis of the data was done using Microsoft office 2013: Excel. A combination of non-dichotomous ordinal data from the Likert scales and qualitative data from the open-ended questions was collected as follows.
All nominal and ordinal variables were presented in frequency tables. In reporting the data of the 5-point Likert scales of the D-Quest, response categories ‘very satisfied’ and ‘satisfied’, on one hand, and ‘totally unsatisfied’ and ‘unsatisfied’, on the other hand, were taken together. For the MIRAD-ACCORT questionnaire, this was done for the answer possibilities ‘very bad’ and ‘bad’ and ‘very good’ and ‘good’. Opinion rates for each aspect were noted, and the mean of the percentage for each of the three response categories was calculated.
In parts 2 and 5 of the MIRAD-ACCORT questionnaire, open questions were used and the answers were written down by the examiner. The information received from open questions was processed using a systematic inductive qualitative approach. This approach implies four steps: first, statements were gathered. Second, these statements were clustered into a limited set of keywords. Third, each statement was assigned to one of these keywords. A participant could be assigned only once to a keyword, even if multiple statements could be assigned to the same keyword. Fourth, the number of tally marks under each keyword was transformed into percentages of the total number of participants.
Results
Participants
The patients’ characteristics are reported in Table 1.
Patients’ characteristics.
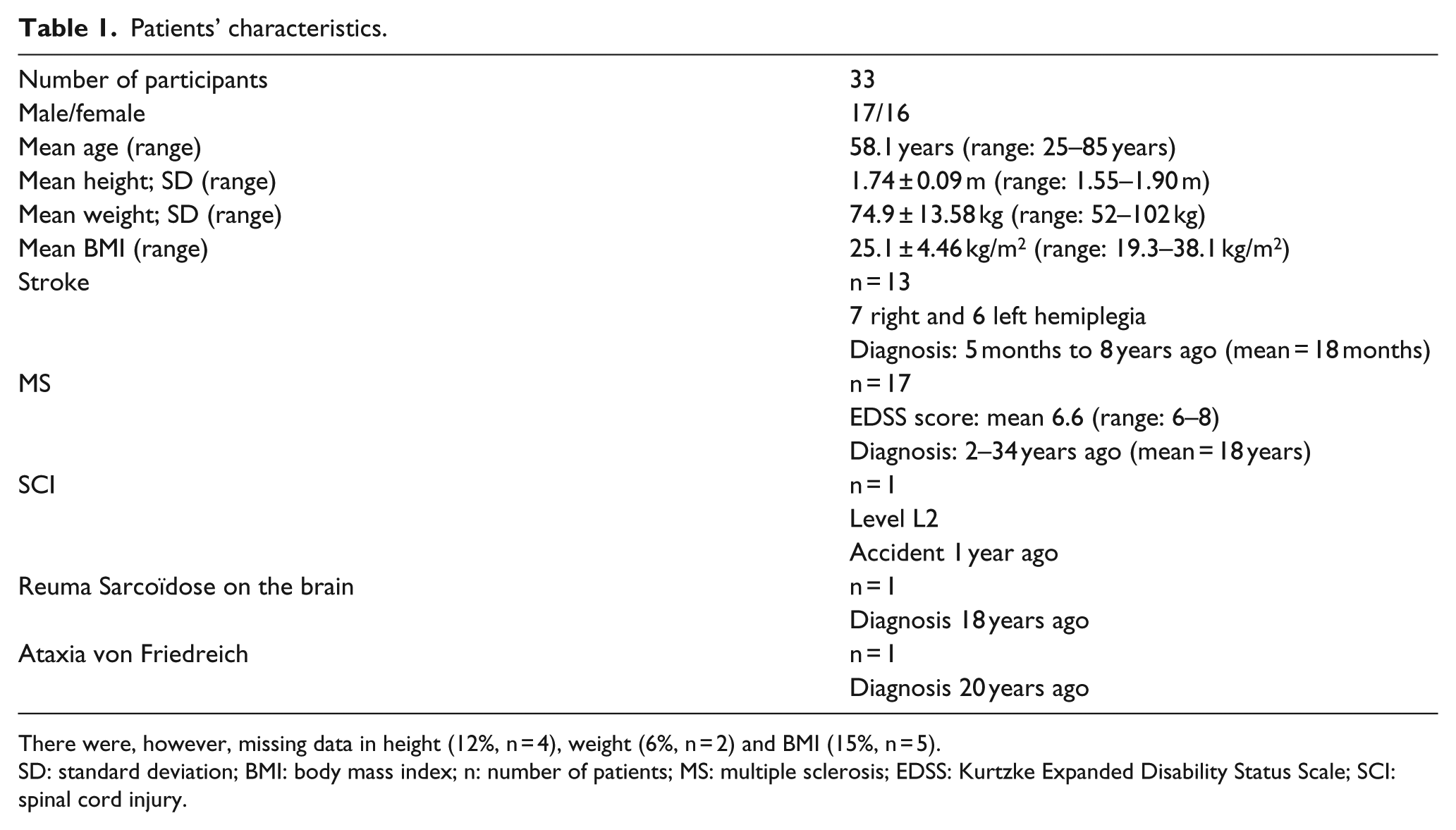
There were, however, missing data in height (12%, n = 4), weight (6%, n = 2) and BMI (15%, n = 5).
SD: standard deviation; BMI: body mass index; n: number of patients; MS: multiple sclerosis; EDSS: Kurtzke Expanded Disability Status Scale; SCI: spinal cord injury.
ODs
A flowchart of the overview of the type, duration of use and complaints of the different ODs is given in Figure 1. The duration of use was defined as the length of time since the patient was prescribed the most recent OD, and the responses to the questionnaires were based on the most recent OD.
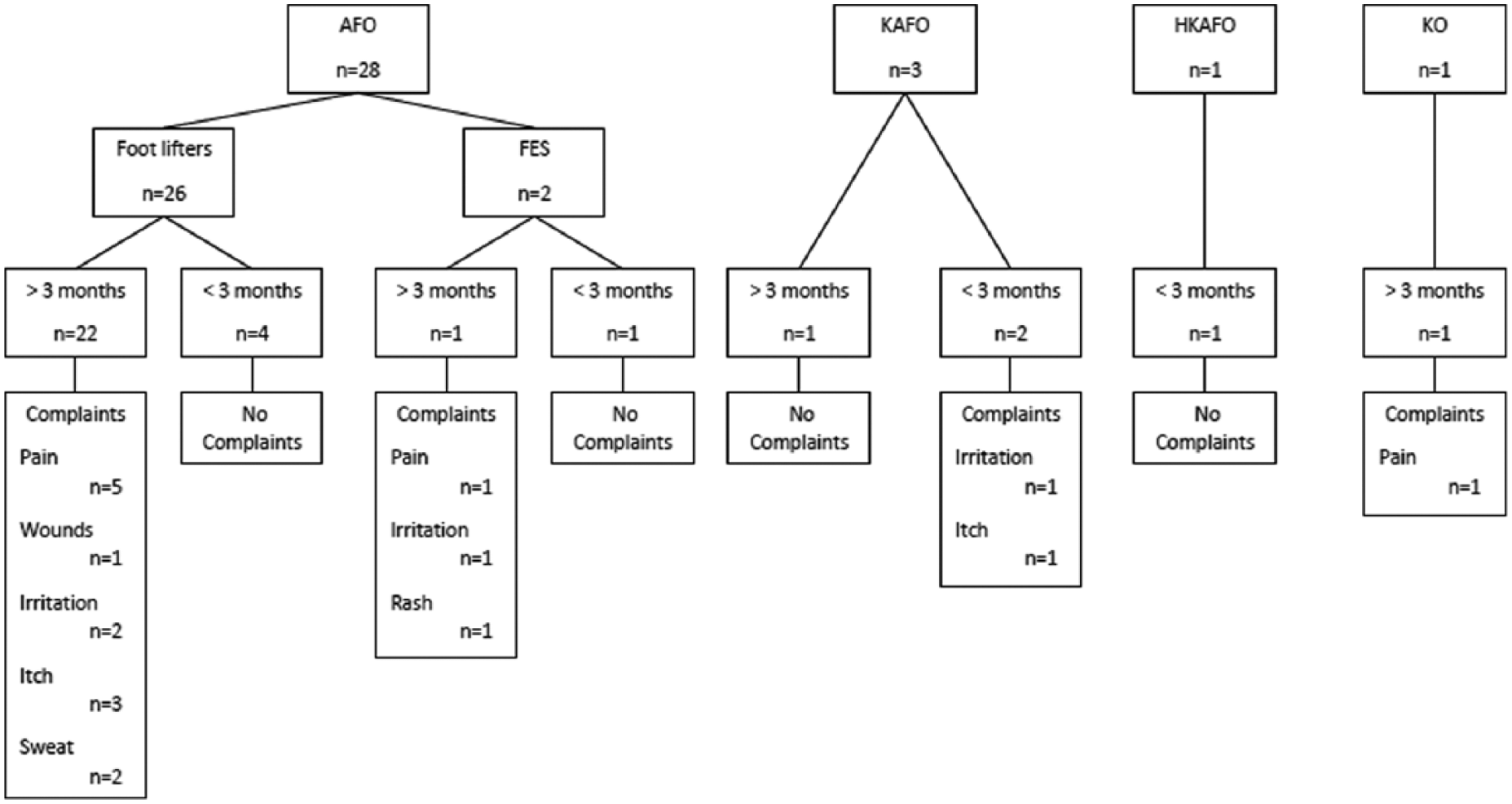
Flowchart of orthotic devices: type, duration of use and complaints.
In total, 21 patients (64%) were wearing their device every day, while the other 12 patients (36%) were wearing it several times a week but not every day. The majority of the participants (n = 23, 70%) wore them the whole day long, four patients (12%) half a day and six patients (18%) 1–2 h a day which corresponded to the treatment session. Of the patients, 18 (55%) were able to put on their device independently. In 11 patients (33%), the nurse or physical therapist put on the device and four patients (12%) were able to apply their OD but needed assistance to do so.
D-Quest questionnaire
The results of the D-Quest questionnaire are reported in Table 2.
D-Quest: satisfaction related to OD and process of providing the OD.
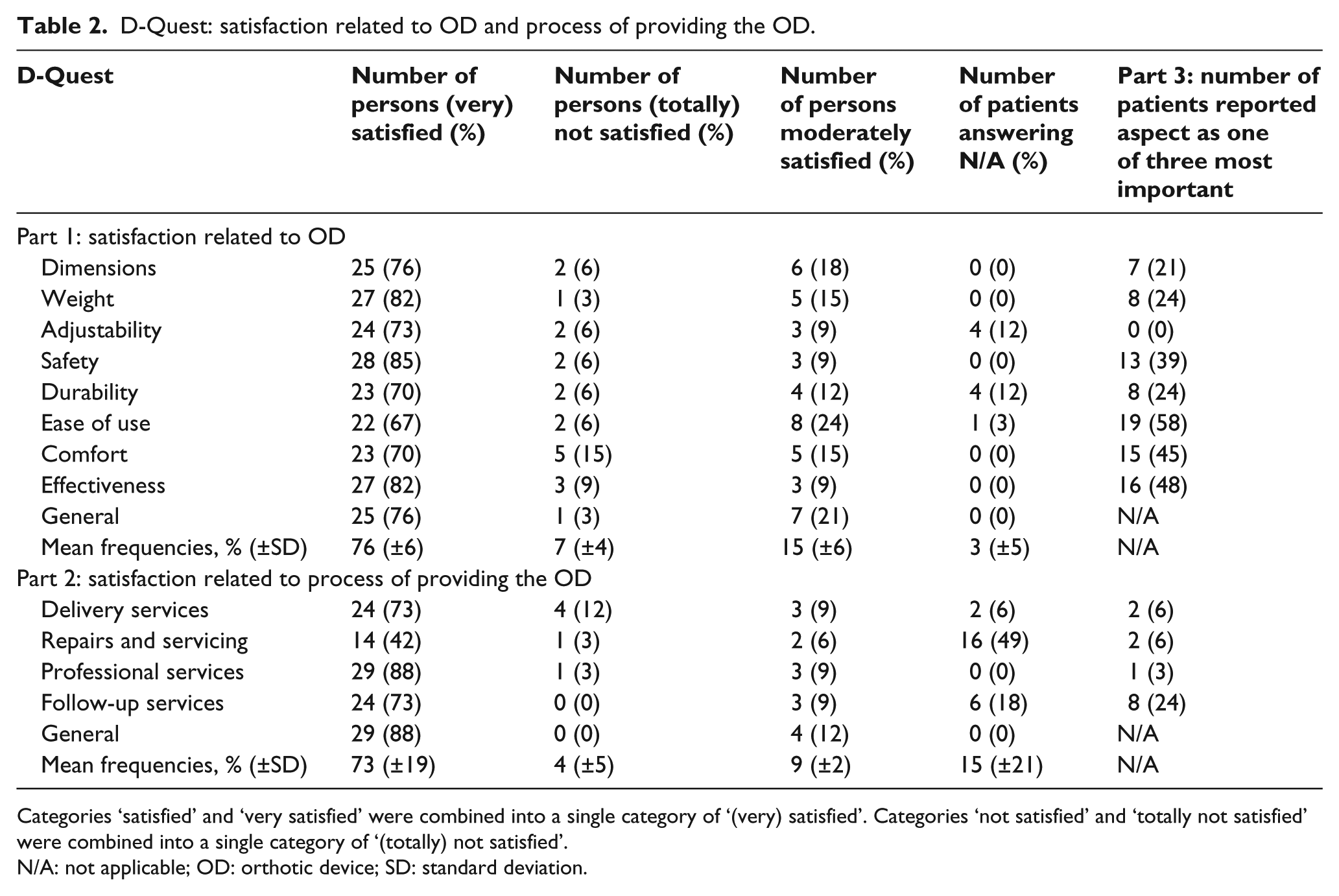
Categories ‘satisfied’ and ‘very satisfied’ were combined into a single category of ‘(very) satisfied’. Categories ‘not satisfied’ and ‘totally not satisfied’ were combined into a single category of ‘(totally) not satisfied’.
N/A: not applicable; OD: orthotic device; SD: standard deviation.
Patients’ satisfaction related to OD
The majority of the participants answered ‘satisfied’ or ‘very satisfied’ when they were asked about their general satisfaction (n = 25, 76%) (Figure 2(a)). The highest satisfaction was found for ‘safety’ (n = 28, 85%), ‘weight’ (n = 27, 82%), ‘effectiveness’ (n = 27, 82%) and ‘dimensions’ (n = 25, 76%). Only a minority of the participants (n = 1–5 for each item) were not satisfied about their OD, with the highest number (n = 5) for comfort.
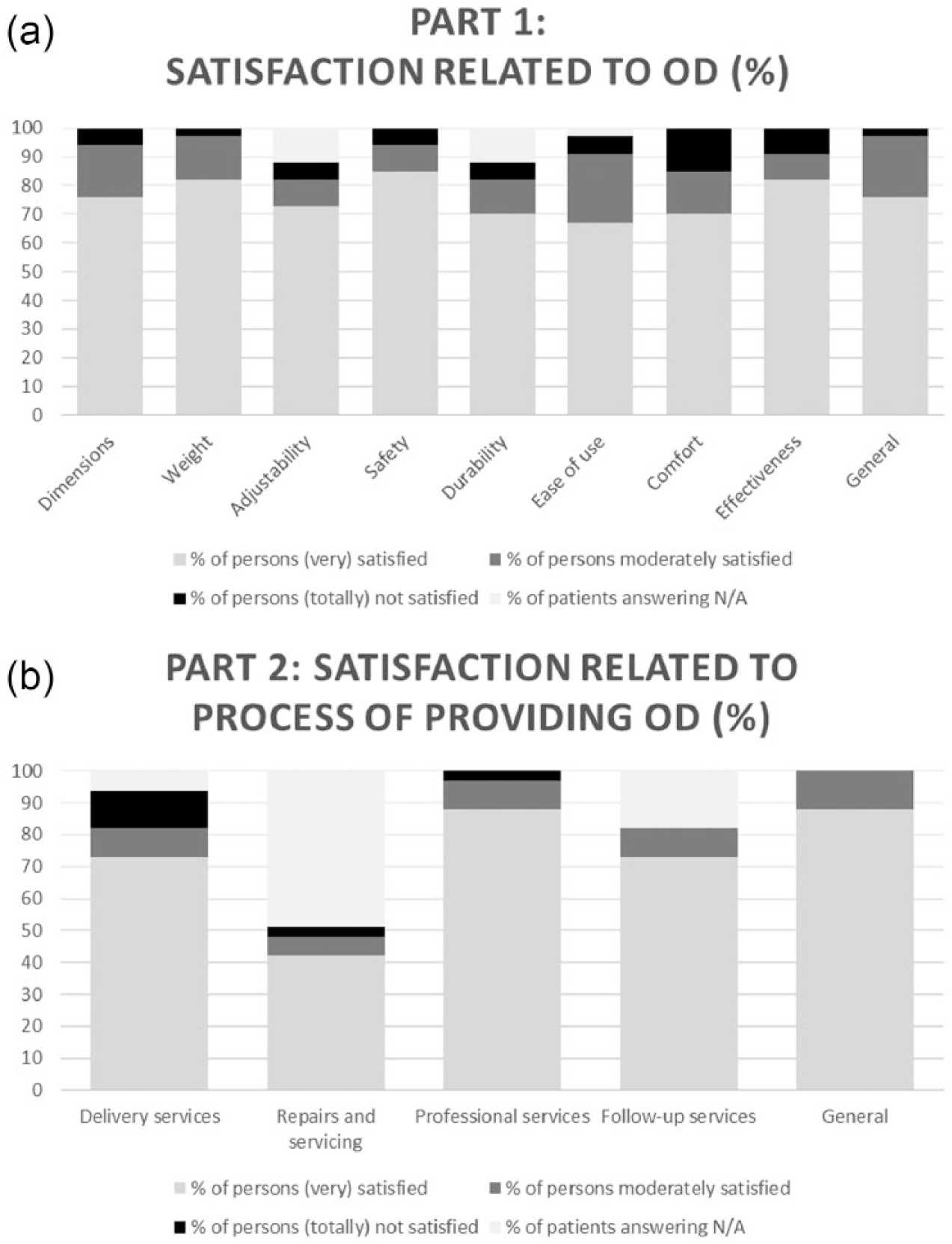
D-Quest: satisfaction related to OD and process of providing the OD: (a) part 1: satisfaction related to OD and (b) part 2: satisfaction related to process of providing the OD.
For ‘professional services’ (n = 29, 88%), ‘service delivery’ (n = 24, 73%) and ‘follow-up services’ (n = 24, 73%), a high number of patients answered being (very) satisfied (Figure 2(b)). ‘Repairs and servicing’ and ‘follow-up services’ were frequently answered as N/A (49% and 18%, respectively), due to the fact that repair and/or other follow-up services were not yet required.
Most important aspects
The three most reported answers on these questions were as follows: ease of use (n = 19, 58%), effectiveness (n = 16, 48%) and comfort (n = 15, 45%).
MIRAD-ACCORT questionnaire
Part 1: patients’ opinion about OD
The results of part 1 of the MIRAD-ACCORT questionnaire are reported in Table 3 and Figure 3.
MIRAD-ACCORT questionnaire part 1, opinion about OD.
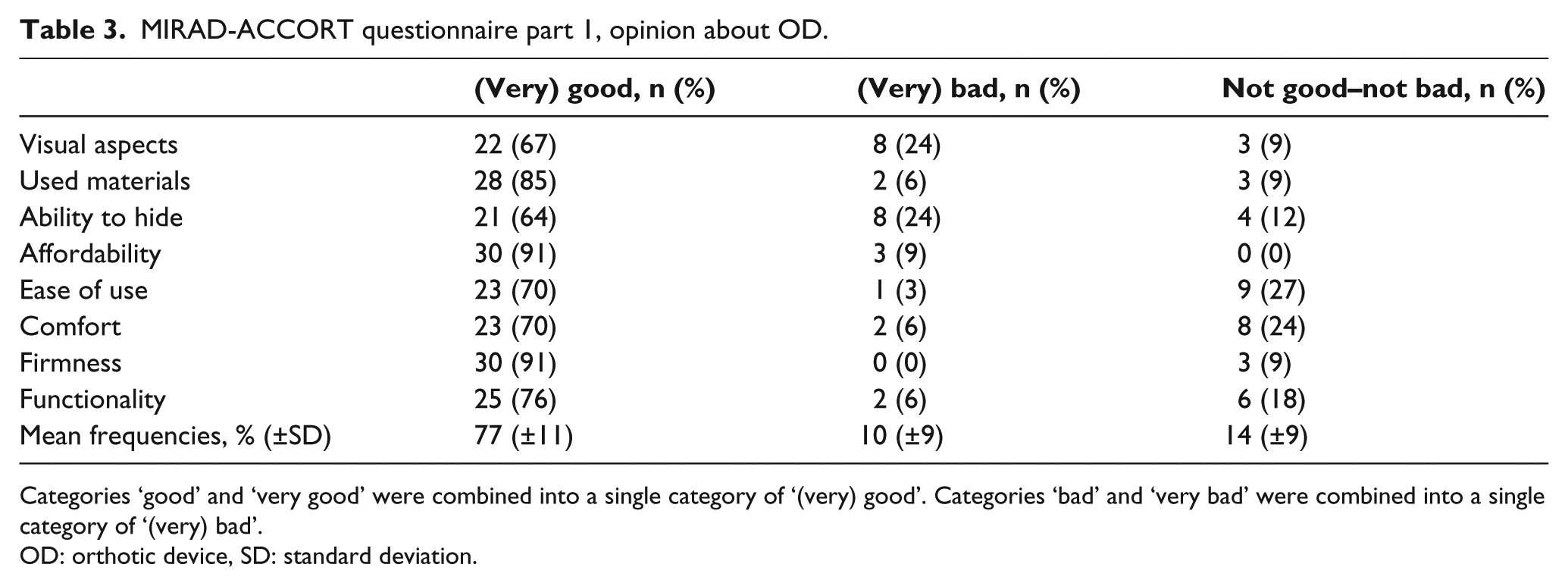
Categories ‘good’ and ‘very good’ were combined into a single category of ‘(very) good’. Categories ‘bad’ and ‘very bad’ were combined into a single category of ‘(very) bad’.
OD: orthotic device, SD: standard deviation.
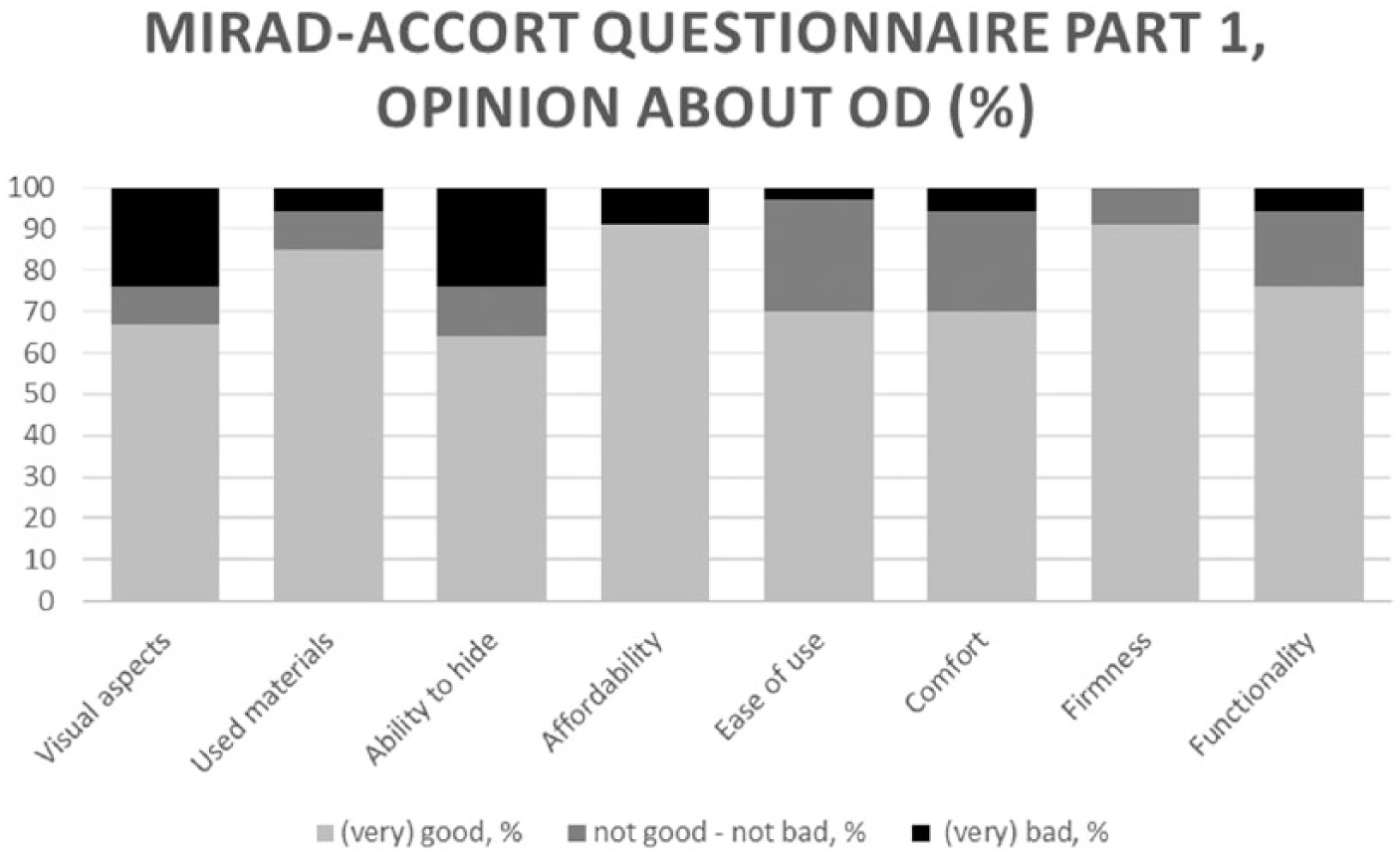
MIRAD-ACCORT questionnaire part 1, opinion about OD.
In total, 30 patients (91%) found the ‘affordability’ and ‘firmness’ of their OD good or very good, followed by 28 patients (85%) who were pleased by the ‘used materials’ in their device. The lowest satisfaction was observed for ‘visual aspects’ and ‘ability to hide’, with 22 (67%) and 21 (64%) patients answered (very) good, respectively. Noticeable is that none of the patients had any complaints about the ‘firmness’ of their device.
Part 2: advantages and disadvantages of OD
In total, 19 patients (58%) mentioned an increase in walking ability and safety. Two patients (6%) could not give any advantage about their OD. The remaining 12 patients (36%) mentioned various advantages such as ‘better positioning’ and ‘provides more support’.
Six patients (18%) found that the main disadvantage of the OD is its ugliness, and three patients (9%) were disgruntled that they could not hide the OD under their clothes. Another three patients (9%) found their OD painful to wear. Seven patients (21%) had no disadvantages to mention about their OD.
Part 3: most important aspects related to OD
The answers of the patients on the various cluster combinations can be found in Table 4.
MIRAD questionnaire part 3, most important aspects related to OD.
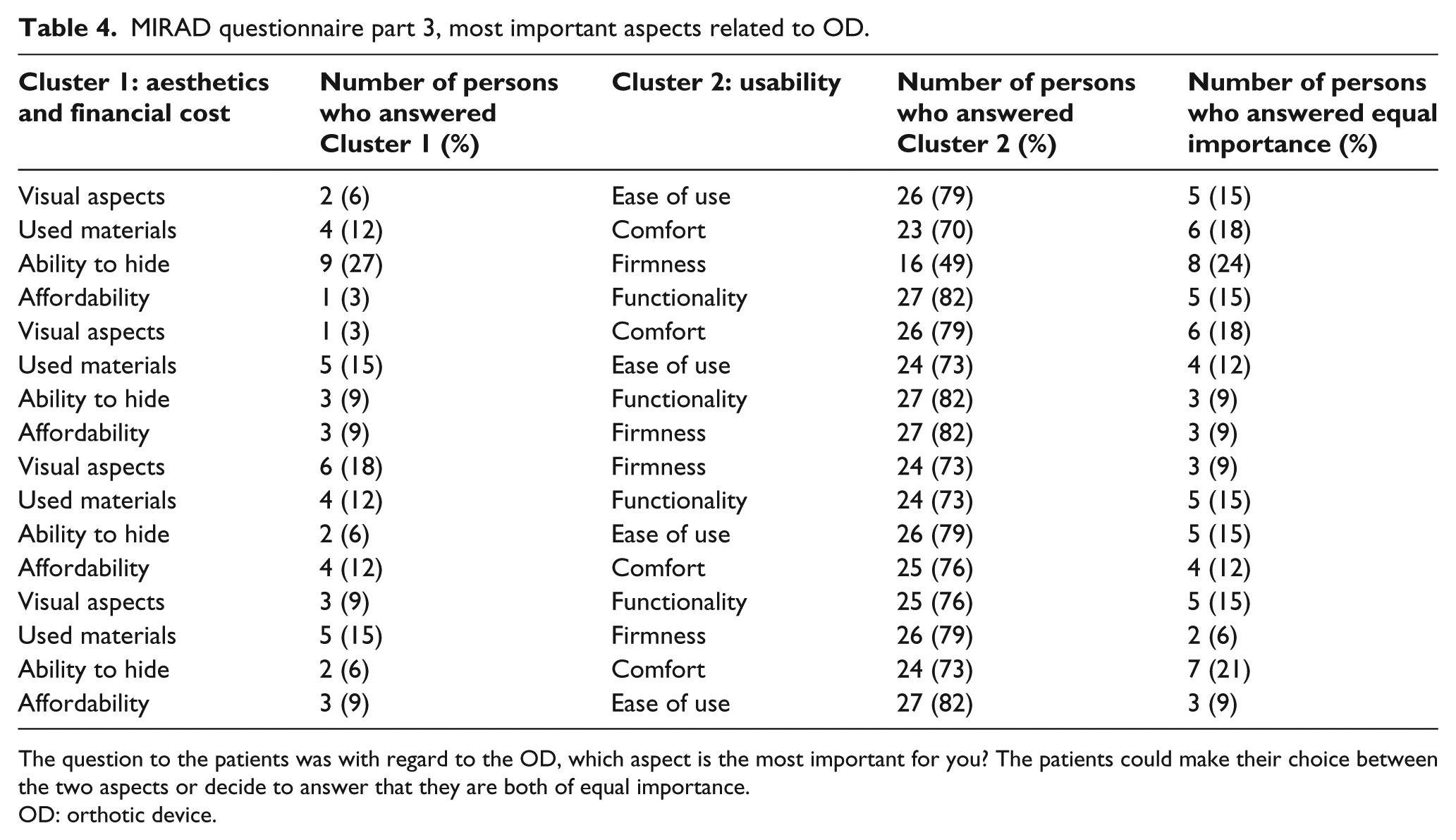
The question to the patients was with regard to the OD, which aspect is the most important for you? The patients could make their choice between the two aspects or decide to answer that they are both of equal importance.
OD: orthotic device.
The general overview of this part of the questionnaire shows that the majority of the patients value the aspects of Cluster 2 (usability) more important than those in Cluster 1 (aesthetics and financial cost). In all the combinations, there were at least 23 patients (70%) who chose for aspects from Cluster 2, with one exception. In the combination ‘ability to hide’ versus ‘firmness’ only 16 patients (49%) chose the latter.
Part 4: reasons not to use the OD anymore
In Table 5, the results of part 4 of the MIRAD-ACCORT questionnaire are reported.
MIRAD questionnaire, reasons for not using the OD anymore.
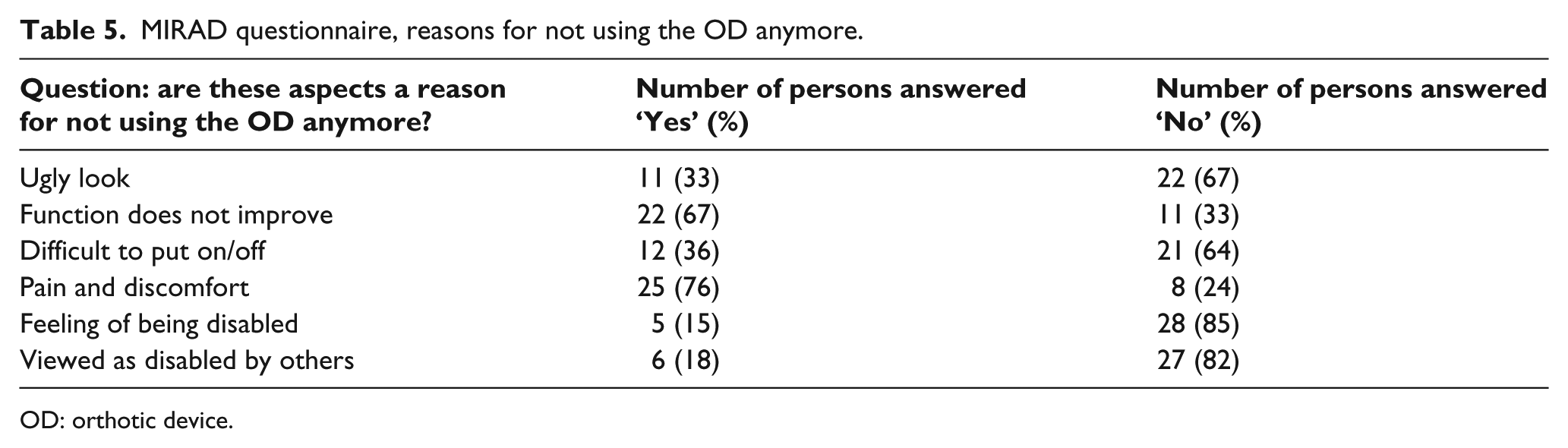
OD: orthotic device.
In total, 25 patients (76%) stated that they would not continue wearing their OD if it was painful or uncomfortable to wear and 22 patients (67%) would consider discontinuing using their device if the functionality would not improve. On the other hand, the majority of the patients would consider continuing using their OD even if the visual aspects were not good (n = 22, 67%), if they felt disabled (n = 28, 85%) or if they had the feeling that others saw them as disabled (n = 27, 82%).
Part 5: what would you change?
Eight patients (24%) would like to change the aesthetic aspects of their OD. The suggestion is to make it smaller or less conspicuous. Also eight patients (24%) would like changes in the used materials. Patients are complaining about the flexibility (e.g. friction) of the materials or the weight. Both MS patients who wear a functional electrical stimulation (FES) want to change the same aspect. They both want it to be easier to place the electrode when they put on their device. Noteworthy is that seven participants (21%) did not want to change their OD at all.
Discussion
The aim of this pilot study was twofold. First, to assess the satisfaction of neurological patients with an OD for the lower limb. Second, to assess the most important reasons for acceptance of an OD. In this study, most patients were satisfied with the OD they currently wear. They were also satisfied with the process of providing the OD. With respect to acceptance, factors associated with functionality and comfort were more important than the aesthetic and psychological aspects of the OD.
Questionnaires
We structured our interview by using two questionnaires. Several surveys are available to measure satisfaction in orthotic users.24,25 However, we chose to use the D-Quest because of its briefness and because it measures specific user-satisfaction, related to assistive devices.
Additionally, we developed a questionnaire, that is, MIRAD-ACCORT, to investigate the factors associated with the acceptance of ODs. The questions were constructed specifically according to the research question of this study. This questionnaire is not yet validated because we aim to modify this version based on the findings of this study. At this time, we want to implement two changes with regard to part 3 of the MIRAD-ACCORT questionnaire. First, the response capabilities of Cluster 1 were always listed first and those of Cluster 2 second. In the new version, a randomization of the order of the different aspects could be implemented. Second, we think that it would be better that, for each combination, the patient could only choose between either of the two aspects, and not be allowed to answer that both are of equal importance. The use of only two answer possibilities would give a more clear impression of the aspect which are priority for the patient. To our knowledge, this is the first study that divides ‘aesthetics and financial cost’ and ‘usability’ related aspects of an OD into two clusters. By letting the patient choose several times between different combinations of items of both clusters, we aim to contribute to a robust decision-making process.
Satisfaction
Patient satisfaction is a complex concept and is influenced by personal and external factors. It consists of the satisfaction with both the assistive devices as and the accompanying services. 17 It also depends on the type of orthotics, the amount of time that the aid is worn and the type of disorder, deformity or injury. In this study, a high number of patients were satisfied with their OD. Previously, different studies were published concerning user satisfaction of assistive devices, not limited to OD of the lower limb, with the use of different methods and questionnaires.15,17,18,24,28–31
In this study, the four aspects of which patients were most satisfied were as follows: ‘professional services’, ‘safety’, ‘effectiveness’ and ‘weight’. Patients were less satisfied with the aspects ‘repairs and servicing’, ‘ease of use’, ‘comfort’ and ‘durability’. Some published studies reported results that are similar to ours.27,32,33 Other studies reported that the highest satisfaction was measured for ‘repairs and servicing’ and ‘durability’ and the lowest for ‘comfort’, ‘dimensions’ and ‘weight’.11,34 These last studies investigate the satisfaction of a wider range of assistive devices. Contrary to this study, they also include, for example, wheelchairs, scooters and aids for daily living.
Acceptance
Factors associated with comfort and functionality were reported as more important than the aesthetic and design aspects of the OD. For example, an ugly design of the OD was not reported as a reason for not wearing the OD. Other studies found the same trend. In a recent study of Bulley et al., 21 the main criticism in the group of MS patients was the appearance of the OD, but the effect and necessity of the aids outweighed this and other downsides. It is shown that the most common reasons for not wearing an OD were ‘function does not improve’ and ‘pain and discomfort’. Earlier studies show comparable results with regard to pain:11,13 pain and discomfort were reported as the main reasons for discontinuing the daily use of an OD. The study of Lobet et al. 24 found a reduction in pain as a main advantage. On the contrary, this study observed that patients indicated that the improvement in walking ability and safety was the main advantage of wearing an OD. This discrepancy may be due to the fact that the research population was different. In this study, neurological patients with a disability in their lower extremities were included, while patients in the study of Lobet et al. 24 experienced haemophilic ankle arthropathy.
‘Cosmetic appearance’,12–16,31,35 ‘weight’,12,13,15,31,35 ‘ease of use’31,35 and ‘functionality’15,31,35 were often analysed in other studies researching ODs. Although other studies assessed the similar aspects as the MIRAD-ACCORT questionnaire, none of them assessed all the aspects of the MIRAD-ACCORT questionnaire simultaneously. ‘Firmness’, ‘affordability’ and ‘used materials’ were aspects assessed in the MIRAD-ACCORT questionnaire that did not occur in other studies. It is noticeable that these aspects have the greatest satisfaction in this study. The definition of ‘functionality’ can vary from study to study. In one study, functionality includes only ‘walking with the device’, 15 while another study includes much more aspects, for example, ‘standing’ and ‘sitting’.31,35 In this study, both definitions were included.
In the study of Van Netten et al., 15 input concerning aesthetic appearance was asked to the patients. They assessed whether patients wanted to make adjustments to their OD, but they did not describe these proposed changes. The MIRAD-ACCORT questionnaire specifically assesses the patient’s perception concerning such specific working points of the OD.
Limitations
The D-Quest has been used in various previous studies18,23,26 and it is a reliable and valid questionnaire to assess the satisfaction of patients using ODs or other assistive devices.18,22,27 As mentioned in section ‘Methods’, to obtain a clearer statement of the patient and because this study focuses on the direction of responses (e.g. a negative, neutral or positive response), all 5-point Likert scales were reduced to a 3-point scale so that answers were more polarized. It has to be mentioned that by doing this, the D-Quest questionnaire needs to be validated again.
In this study, the majority of the patients were post-stroke or persons with MS. They all suffer from gait problems, but the severity of their disease was diverse. Moreover, the evolution of these diseases is patient- and disease dependent, which may influence patient’s ideas about the OD. In this study population, the majority of OD were ankle–foot orthotic device (AFO); although patients with other types of OD were also included. The type of OD could have a large influence on the satisfaction or acceptance. For example, patients with only an AFO (foot-lifter or FES) are better able to hide their device under pants, while patients with a leg OD (knee–ankle–foot orthotic device (KAFO), hip–knee–ankle–foot orthotic device (HKAFO), knee orthotic device (KO)) will wear it over the clothes. Also different opinions are possible dependent on the duration between the first time that they get the OD and the moment of administering the questionnaire. We did not assess these potential associations due to the small sample size. The work by Williams et al. 36 has indicated that women have more complex needs in relation to the appearance of footwear in comparison to men. For women, the loss of femininity imposed by the appearance of the footwear has an impact on many facets of their lives. 36 Women revealed that therapeutic footwear invokes emotions of sadness, shame and anger, resulting in severe restriction of important activities, particularly those involving social participation. 37 No such information was found in the literature on ODs. It would be interesting to measure the satisfaction and acceptation in a much larger group of patients and to cluster the results with regard to, for example, gender, disease, age and duration after diagnosis.
Conclusion
Most patients were satisfied with their OD of the lower limb as well as with the process of providing it. Less than one-fourth of the patients have a bad opinion about the ‘visual aspects’ and the ‘ability to hide’ of their OD. These, however, have a lower priority compared to functionality. An improvement in functionality is mostly reported as a main advantage and is a reason for continuing the use of their OD.
Footnotes
Author contribution
Study concept and design: E.S. and E.K. Acquisition of data: E.S. Analysis and interpretation of data: E.S. and E.K. Drafting of manuscript: E.S. Critical revision of manuscript for important intellectual content: E.K. and D.B. Administrative, technical or material support: S.I., J.V.N. and C.L. Study supervision: E.K.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by SBO IWT (Grant/Award Number: ‘120057’).