
Abstract
This report presents objective motion analysis measurements of 14 stance control orthoses (SCO) users during a prospective open-enrollment 6-month clinical field trial. Participants were fitted with a Dynamic Knee Brace System (DKBS) which is a novel electromechanical SCO developed by the authors. Seven of the 14 subjects that had been prescribed but did not use a KAFO at the time of enrollment were defined as novice users. Those subjects who at the time of enrollment were using a locked KAFO for ambulation were defined as experienced users. Results showed that all subjects significantly increased peak knee flexion from 49.0 ± 15.5° to 55.9 ± 11.4° between the initial and six month tests (p = 0.02). They also tended to increase peak hip flexion from 39.6 ± 13.4° to 46.0 ± 14.5° between the 3 month and 6 month tests (p = 0.09). Novice users significantly increased velocity from 74.7 ± 19.4 cm/s to 81.2 ± 19.0 cm/sec between the initial and 3-month tests (p = 0.005). These same users increased stride length from 109 ± 15.3 cm to 112 ± 16.6 cm over the same time period (p = 0.008). Experienced KAFO users, however, tended to increase velocity from 68.8 ± 20.5 cm/s to 83.2 ± 16.8 cm/s at 3 months (p = 0.06). This was combined with a significant increase in cadence from 76.2 ± 14.1 steps/min to 83.9 ± 8.3 steps/min between the initial and 3 month tests (p = 0.05). Joint kinetics showed no changes for users over the duration of the testing period. These results indicate that KAFO users make significant gains in temporodistance measures, while changes in joint kinematics take longer to develop.
Introduction
Knee-ankle-foot orthoses (KAFOs) are prescribed for those individuals that have significant weakness of the knee extensor musculature. The diagnoses of people requiring KAFOs includes but is not limited to polio, neurovascular pathology and trauma, and neurological and developmental defects such as spina bifida. In the United States approximately 989,000 people wear KAFOs (Russell et al. 1997). These orthoses are typically fabricated with hinge joint mechanisms that lock the knee in full extension thus providing unyielding knee stability to the patient. Oxygen cost of walking is increased however, with the knee immobilized by as much as 23 – 33% (Waters et al. 1982; Mattsson and Brostrom 1990; Kaufman et al. 1996a). A stance control orthosis (SCO) is designed to allow swing phase freedom for the knee joint to minimize the impact on oxygen consumption while automatically providing stance phase stability. The desirability of the SCO concept has been appreciated by orthosis designers since the first half of the last century (Spahn 1913; Taylor 1941). Over 20 patents have been issued in the US and internationally for SCO devices.
Test reports from several experimental SCO systems have been published since 1978 demonstrating a range of potential benefits (Lehmann and Stonebridge 1978; Malcolm et al. 1980; Kaufman et al. 1996b; Suga et al. 1998; van Leerdam and Kunst 1999; McMillan et al. 2004; Rietman et al. 2004; Irby et al. 2005). All reports include changes in kinematic and temporodistance measures when comparing locked knee and SCO gait patterns. However, these reports have all studied subjects shortly after receiving their SCO. With one exception (van Leerdam 1993), there are no reports in the literature that document the gait changes over time. Therefore the objective of this report is to document the results of a prospective 6-month open label clinical field trial of a novel SCO. The authors hypothesized that there would be improvements in gait over time.
Methods
The Dynamic Knee Brace System (DKBS) used in this study is a novel stance control orthosis. It is comprised of a custom designed wrap spring clutch (Irby and Kaufman 2002), an electromechanical release, and sensors at the knee and footplate, all fit to a conventional KAFO (Figure 1) (Irby 1994; Irby et al. 1999a, 1999b). The wrap spring clutch is designed to provide 113 Nm of braking capability about the joint axis while withstanding 100 Nm of varus/valgus loading and/or 7 Nm of transverse (i.e., axial) moments. The clutch along with the electromechanical release mechanism measures 22×10×5 cm. The control circuitry is housed in a case measuring 11×8×2 cm and is typically mounted on the lateral border of the thigh shell of the KAFO. A typical DKBS KAFO weighs approximately 3.1 kg, with about one-third of the weight attributed to the clutch, electromechanical release, and electronics circuitry. The remainder of the weight is due to that of a typical KAFO with thermoplastic thigh and shank sections, stainless steel uprights, and medial-side stainless steel hinge. The lateral hinge is replaced by the wrap spring clutch assembly. A rechargeable battery pack providing approximately two full days of use measures 13×7×2 cm, weighs 0.37 kg, and is carried by the user in a waist pack. Two sensors provide input to the control circuit. One at the knee joint provides knee angle information. The second at the foot provides foot-floor contact information.
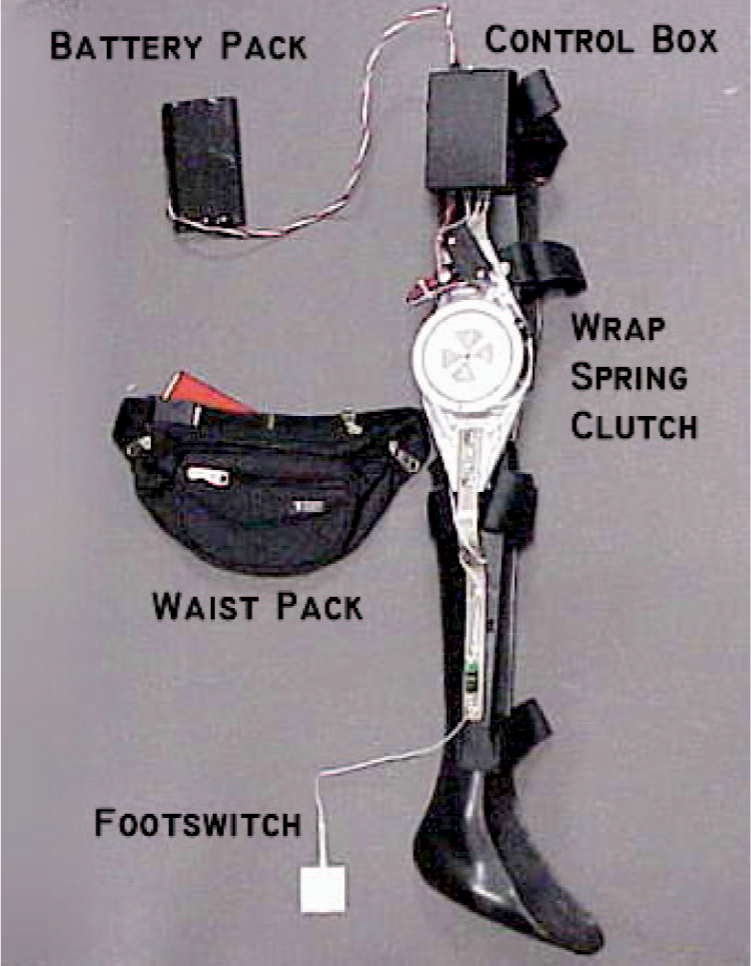
The Dynamic Knee Brace System (DKBS) is a stance control orthosis (SCO) and consists of a standard knee-ankle-foot-orthosis with the lateral hinge replaced with a novel wrap spring clutch designed for this application. The electromechanical release system includes a rechargeable battery pack, control electronics and a footswitch. The battery is carried by the user in a waist pack.
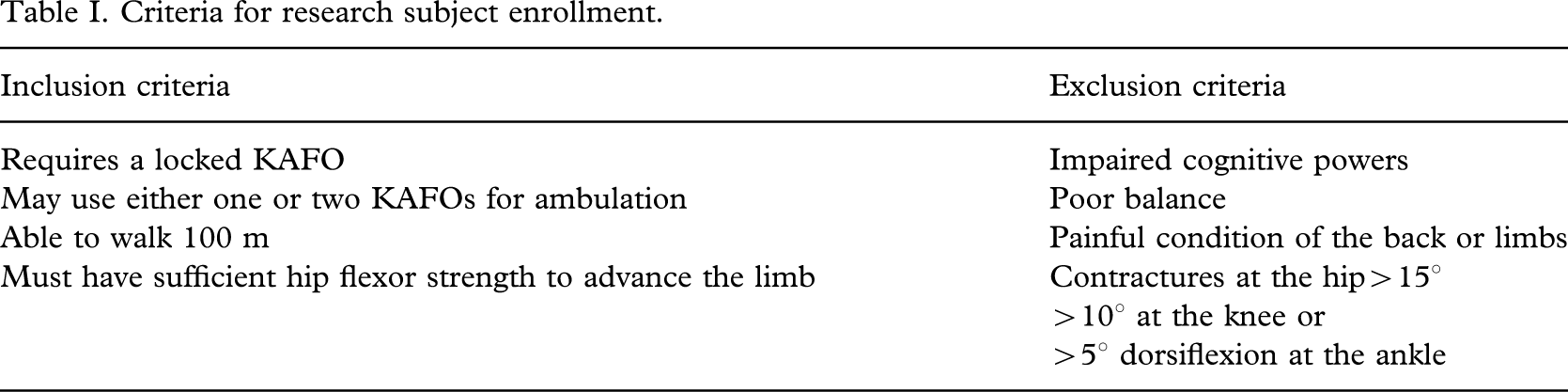
Research participants were recruited based upon the inclusion and exclusion criteria shown in Table I. The testing protocol and consent forms were approved by the local institutional review board prior to subject enrollment. Written consent was obtained from each participant prior to initiation of the laboratory testing. KAFOs were fabricated by certified professional orthotists. Proper fit was carefully evaluated and modifications made as needed to eliminate problems with orthosis alignment and fit. Testing was conducted using a single DKBS even though in some cases patients had bilateral involvement. In those cases the weaker limb was fitted with the DKBS.
Criteria for research subject enrollment.
Objective gait measurements were acquired with a computerized video motion analysis system utilizing ten infrared cameras (EvaRT 4.0, Motion Analysis Corporation, Santa Rosa, CA). Motion measurement markers were placed at bony prominences for establishing anatomic coordinate systems for the pelvis, thigh, shank, and foot (Kadaba et al. 1989). Where orthosis componentry interfered with placement of markers directly on the skin, offsets were recorded and joint centre locations were corrected in subsequent post-processing. One set of data corresponding to the standing position (static data) were recorded in order to calculate the location of the joint centres. After a brief orientation session, the subject was instructed to walk on the laboratory walkway. Participants were allowed to choose walking aids befitting their ambulatory status and confidence. Floor reaction forces were recorded using two AMTI force plates (Advanced Mechanical Technology, Inc., Watertown, MA; model BP2416) and two Kistler force plates (Kistler Instrument Corp., Amherst, NY; model 9281B) embedded in the floor in the centre of the calibration volume. The 3D marker coordinates and force plate data were used as input to a commercial software program, OrthoTrak 5.0 (Motion Analysis Corp., Santa Rosa, CA), to calculate the joint kinematics and kinetics. Joint moments reported are internal moments normalized by body mass (kg). Temporal-distance factors such as stride, cadence, and velocity were calculated from the kinematic data. Gait cycle periods were selected by heel-strike to heel-strike events. All gait events were expressed as a percentage of the gait cycle, irrespective of the actual time for a stride, to yield a normalized gait cycle. Testing was conducted in a permanent motion analysis laboratory environment with a level vinyl tiled floor. Data were collected with the DKBS activated, providing automated stance phase control. Gait data were collected at 0, 3, and 6 months.
Gait data for the hip, knee, and ankle were analyzed for differences between users' experience level and across time in the field. Peak values for pelvic obliquity, hip flexion, hip extension, and hip abduction were evaluated. These parameters were selected because they would reflect compensatory effects for a stiff-knee gait. Kinetic data analysis included peak contralateral hip abduction in swing and ipsilateral extension moments during stance, average knee extensor moments during stance, knee moment at foot-off, and peak contralateral ankle plantarflexion moment during stance. Statistical analyses were performed using a commercial analysis package (JMP 6.0 and SAS 8.2, SAS Institute Inc., Cary NC). Data were lumped together as well as stratified according to the subjects' current KAFO status. The ‘experienced’ group routinely used a locked KAFO for ambulation. The ‘novice’ group had been prescribed but did not regularly use a locked KAFO for ambulation. A two-way Analysis of Variance with repeated measures was used to compare between experienced, novice, and aggregate groups at time points of 0, 3, and 6 months. Statistical significance was set at p = 0.05.
Results
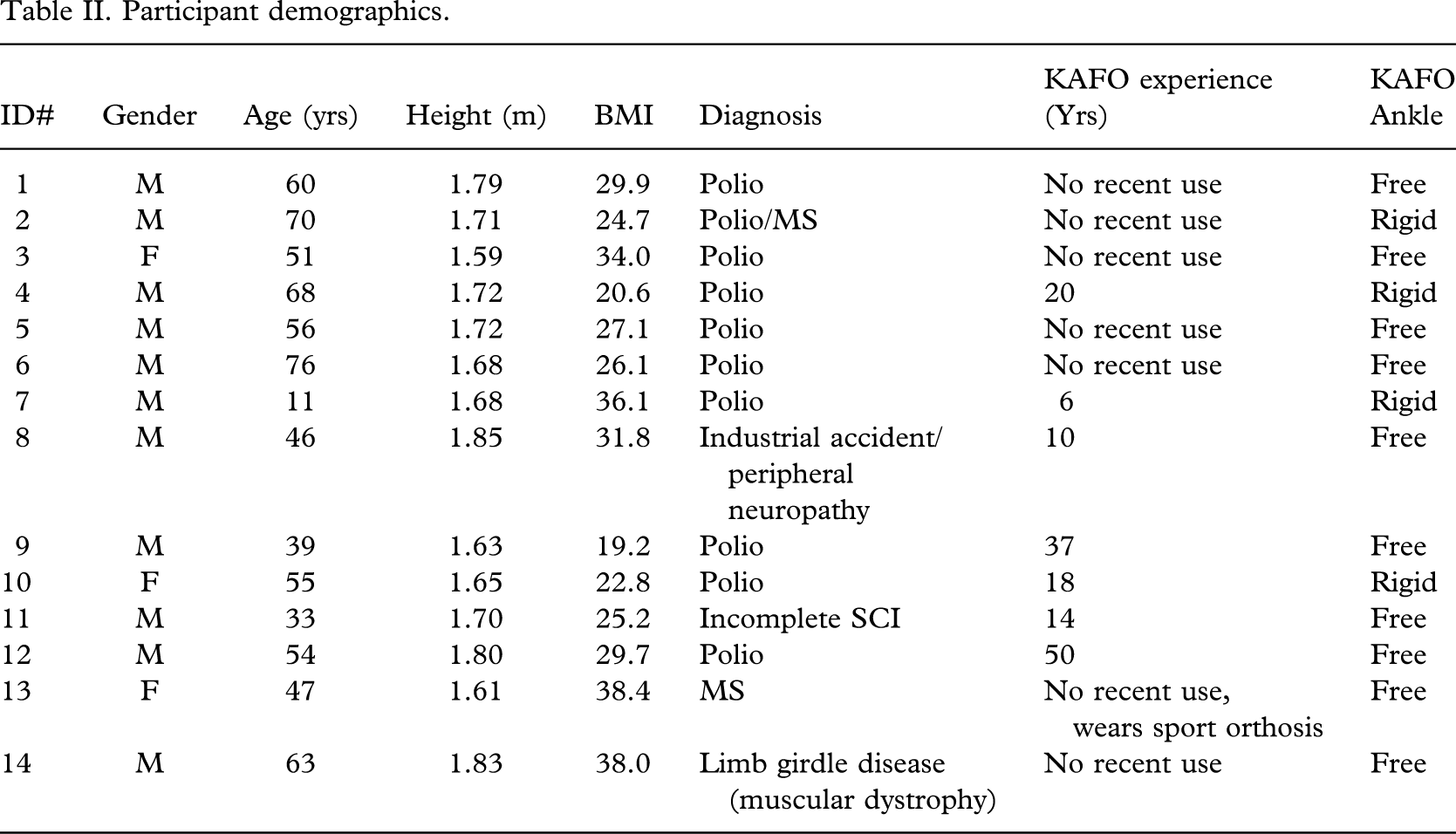
Fourteen research participants (11 males: 3 females) were enrolled (Table II). Of these, 11 returned at 3 months and all 14 returned for the 6-month testing. Average age was 51 ± 17 years ranging from 11 – 76 years. Body weight was 84 ± 22 kg ranging from 51 – 127 kg. Body Mass Index (BMI) for this group was 28.6 ± 6.4 ranging from 19.2 – 38.4. Nine research participants had polio while the balance of the patients had other pathologies or trauma including neuropathies, incomplete spinal cord injuries, spina bifida, multiple sclerosis, and muscular dystrophy. Seven subjects currently used a locked KAFO and were designated ‘experienced’ users. Of these, 3 had rigid and 4 had articulated or ‘free’ orthotic ankle joints. The remaining 7 ‘novice’ users in this study had chosen to manage their ambulatory needs up to this point without the aid of a KAFO. Six of the seven novice participants used articulated or ‘free’ ankle joints while the 7th decided upon a rigid ankle for their orthosis.
Participant demographics.
Temporodistance measures of velocity, cadence, stride length, and percent single limb stance were evaluated over time for all participants. Self-selected walking velocity increased from 72 ± 19 cm/sec at the initial test to 82 ± 16 cm/sec at 6 months (p = 0.005). Cadence increased from 78 ± 13 steps/min at the initial test to 83 ± 8 steps/min) at 6 months (p = 0.009). Stride length increased from 107 ± 18 cm at the initial test to 117 ± 15 cm at six months (p = 0.03). Single limb support time remained unchanged throughout this field trial, measuring 31 ± 5% across all data sets. Dividing the data by KAFO experience provided further insight. Between the initial and three month tests, novice users showed significant changes in velocity and stride length (Figure 2).
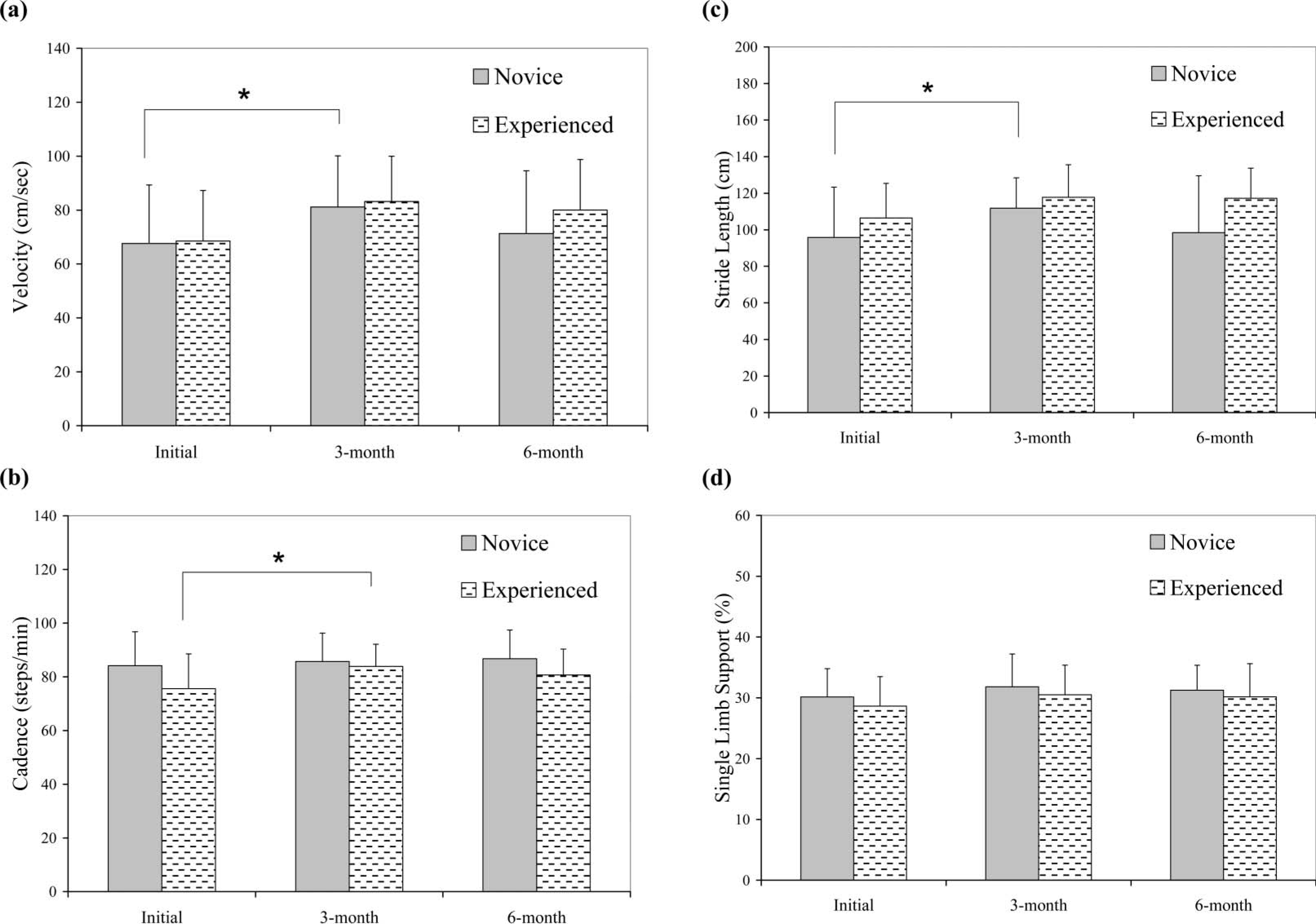
(a – d) Changes in temporodistance parameters of velocity, cadence, stride length, and % single limb stance (braced limb) over the six-month trial. Parameters indicated by an asterisk were significantly different. ∗p ≤ 0.05.
Velocity increased from 75 ± 19 cm/sec to 81 ± 19 cm/sec at 3 months (p = 0.005). Stride length increased from 109 ± 15 cm to 112 ± 17 cm (p = 0.008) at 3 months. Experienced users showed significant increases in cadence from 76 ± 14 steps/min initially to 84 ± 8 steps/min at three months (p = 0.009). They increased walking velocity from 69 ± 21 cm/s to 83 ± 17 cm/s at 3 months, but this change was not statistically significant (p = 0.06). No significant changes were observed in the 3 – 6 month period for either the novice or experienced groups. Percent single-limb stance demonstrated no changes across experience group or test session.
Peak hip flexion tended to increase between the 3 month and 6 month tests (40 ± 13° to 46 ± 15° respectively, p = 0.09). No significant changes over time were observed for pelvic obliquity, hip abduction or hip extension. Peak knee flexion increased for all users between the initial and six month tests (49 ± 16° and 56 ± 11° respectively, p = 0.03) (Figure 3). Experienced KAFO users showed a significant increase in knee flexion between the initial and six month tests (44 ± 12° and 54 ± 12° respectively, p = 0.03). Novice users showed no significant change between the three time points but had greater peak knee flexion during swing. Average values over the three laboratory sessions were 58 ± 14° for novice users and 48 ± 12° for experienced users (p = 0.002). Ankle motion plantar flexion and dorsiflexion maxima did not differ between experience groups or over time. No significant changes were found in the kinetic data across the 6-month field trial period. Knee extensor moments during stance averaged 0.14 ± 0.11 Nm/kg. Knee extensor moments at foot-off averaged 0.051 ± 0.029 Nm/kg across all test periods.
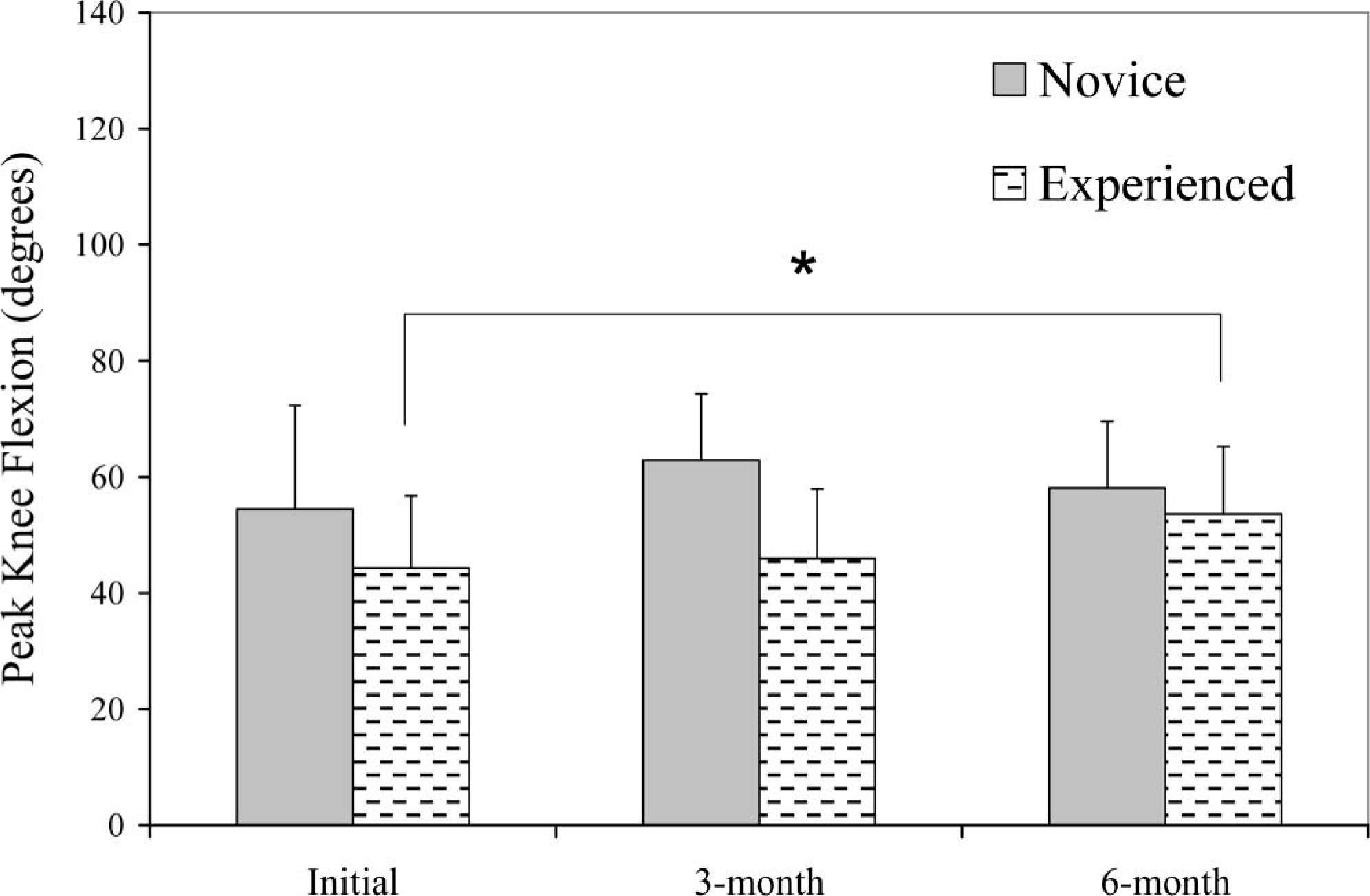
Peak SCO knee flexion versus time in the field. Statistically significant increases in peak knee flexion were observed between the initial and 6-month tests. ∗p ≤ 0.05; ∗∗p ≤ 0.00.
Discussion
Objective laboratory data collected at the initial three- and six-month milestones provide means to evaluate the functional benefits provided by the SCO. Significant changes were observed in walking velocity, cadence, stride length, and knee flexion. In general users tended to increase walking velocity between the initial and three month test point. Previous KAFO experience had an impact on outcome. Novice KAFO users increased velocity and stride length over the first 3 months. Experienced KAFO users increased cadence over the same period with a trend of increased velocity. The flexed knee effectively shortens the swing limb thereby reducing the natural period of oscillations. Thus a minimum of three months of time may be required to realize objective kinematic benefits of SCO technology.
Compensations for pathologic stiff knee gait are circumduction, and contralateral ankle plantar flexion (Sutherland et al. 1990). One may reasonably add increased pelvic obliquity (rotation in the coronal plane) to the list of compensations that KAFO users could employ to manage a locked knee joint. The authors expected a diminution of these compensatory motions as more ‘normal’ gait patterns were developed over time. No statistically significant changes were observed however. This outcome may be due to the spectrum of compensations adopted by individuals. Regardless of the original walking style for these subjects, each individual adopts a unique combination of compensations at the hip, knee, and ankle. As a result one would expect that the adoption of new compensations for the SCO would vary from one person to the next without statistically significant changes found in the aggregated data.
In a similar vein, percent single-limb stance was included in this review as an indicator of change in right-left symmetry. Again, no significant changes were observed either between experience groups or across laboratory sessions.
The body-mass indices (BMI) of participants in this study ranged from 19 – 40. According to the CDC, the group consisted of 4 ‘normal’, 6 ‘overweight’, and 4 ‘obese’ participants (CDC 2004). Nonetheless, no mechanical failures of the DKBS occurred during the accumulated 7 years of field use.
As of this writing there are five commercial SCOs in the marketplace. Only two offer different sizes, both based upon body weight. However, half of the subjects in this trial would not have qualified for any of the commercial SCOs because they exceeded body weight restrictions. Knee moment data collected in this project will be useful in the design of future SCO systems by providing a realistic upper bound on the forces across the orthotic knee joint. Furthermore, this study documents the knee joint moment at the instant of foot-off; knee extensor moments at foot-off averaged 0.051 ± 0.029 Nm/kg equalling 4.3 ± 2.4 Nm in absolute terms. This net moment would tend to collapse the knee and cause binding of most locking mechanisms. This highlights an important benefit of the DKBS system and its use of a wrap spring clutch. During gait the position of the limb just before foot-off (pre-swing) creates an extrinsic knee flexion moment as confirmed by this laboratory data. The wrap spring clutch is able to disengage under this load allowing a normal knee flexion pattern. Other self-engaging mechanisms cannot provide this functionality.
Comments from the research subjects after field trial experience included ‘hard to find clothes to wear’, ‘fanny pack is too bulky’, ‘walking is easier, but the weight tires me out’, and ‘I like the function, it's just too bulky’. Spontaneous comments during initial gait training included ‘walking is easier’, ‘feels lighter when it is turned on’ and ‘I don't have to think about my knee or ankle, I can just pick my foot up and go’. These comments highlighted areas for future DKBS development. The size and weight of all components should be reduced to ease clothing selection and presumably walking energetics. However, the size and weight concerns have been shown to be secondary to operation and stability of the DKBS stance control orthosis (Bernhardt et al. 2006). User comments such as ‘I don't have to think about my knee or ankle’ encourages the authors to continue DKBS development and SCO testing.
Limitations of this study were lack of documentation of the actual use in the field and limited number of subjects enrolled. This study design did not include objective measures of DKBS use in the field. From interview data we know that use during the six-month field trial varied markedly from ‘only on Sundays’ to every day, all day (Bernhardt et al. 2006). The time course of accommodation would logically be linked to actual use in the field. As part of the remuneration, the custom-made KAFO shell was made available to each subject at the end of their participation. Overall however, remuneration was low and did not equal the costs of time away from work, travel, or room and board. For future studies automatic electronic surveillance of use in the field will be built into the electronics control package. In this way unbiased data will be available to help correlate changes in kinematics and kinetics with actual time in the SCO. Additional incentives to encourage completion of future research protocols need to be considered. These may include increased remuneration to compensate for absence from work as well as for travel and lodging expenses.
Conclusion
This report is the culmination of a six-month open enrollment field trial of a stance control orthosis (SCO). The Dynamic Knee Brace System, a wrap spring clutch based SCO was used exclusively in this project. Fourteen individuals requiring a KAFO were enrolled and fitted with the DKBS. Testing under laboratory conditions was conducted at 0, 3, and 6 months of SCO use. All users benefited from SCO use, demonstrating significant improvements in temporodistance factors at 3 months. Gait changes, however, depended upon previous KAFO use. Experienced users demonstrated a significant increase in peak knee flexion but they did not “catch up” to the novice users during this six-month trial. Novice users showed increased velocity and stride length while cadence changed for the experienced users. Kinematic variables, however, reached significant change levels only at the six-month mark. Therefore, three months represents the minimum time required for the SCO technology.
Footnotes
Acknowledgements
This project was supported by the National Institutes of Child Health and Human Development, Grant HD30150, and the Mayo Foundation. The authors wish to thank Robert Lotz CPO of Prosthetic Orthotic Center, and Richard Miller CO of Prosthetic Laboratories of Rochester, for their support in KAFO fabrication and patient recruitment. We also wish to acknowledge the staff of the Motion Analysis Laboratory, and in particular Diana Hansen, for motion data collection and reduction. David H. Sutherland, MD, is recognized for his conviction, energy, and generosity that made this project possible. Kaufman and Irby are the inventors technology used in this research, the technology has been licensed, and they have received royalties on it.