
Abstract
Background: Modern prosthetic systems with more degrees of freedom offer the patient clearly improved functions. However, the influence of functional arm prostheses on body posture and gait have never been quantified.
Objectives: The purpose of this investigation was to observe the impact of a functional arm prosthesis on body posture and gait of shoulder disarticulation patients.
Study Design: Experimental, biomechanical.
Methods: Eight patients with unilateral shoulder disarticulation were enrolled. Static posture and gait analyses were conducted with and without using a functional arm prosthesis. Static posture analysis using the L.A.S.A.R. Posture device as well as kinematic and kinetic gait analysis using an optoelectronic camera system combined with force plates were conducted with and without prosthesis in eight unilateral shoulder disarticulation patients.
Results: Static analysis confirmed that an arm prosthesis improves body posture of amputees. Gait analysis revealed that compensatory movements during walking as well as external knee moments on the prosthetic side leg are significantly reduced when using a free swinging shoulder joint.
Conclusions: An arm prosthesis does not only offer functional and cosmetic benefits. The results confirm that unilateral shoulder disarticulation patients benefit from a functional arm prosthesis with a free swinging shoulder joint in terms of optimized posture and gait dynamics.
This study demonstrates that shoulder disarticulation patients benefit from a functional prosthesis with a free swinging shoulder joint. Such prosthesis significantly improves body posture and gait characteristics, reduces compensatory movements and relieves distress to the musculoskeletal system. This should be considered when prescribing a prosthesis for shoulder disarticulation amputees.
Keywords
Background
After upper limb amputation in the shoulder joint or shoulder girdle region patients can be fitted with a prosthesis. There are different options for functional prosthetic fittings.1–4 From the literature, we know prostheses with a shoulder joint that swing freely in the sagittal plane are perceived as very comfortable during walking.2,3,5 It is known that natural shoulder movement influences the gait pattern significantly. 6 In 1939, Elftman stated that the sound arm does not swing like a usual pendulum, but is driven by shoulder muscles. The angular acceleration of the arm corresponds to that of the trunk, but in reverse direction. 7 Also, Jackson confirmed that the reason for arm swing is not definitely identified and controversially discussed even today. 8 Pontzer et al. described that there is an elastic connection between trunk, shoulder and arm. Acting as a damper, the arm reduces trunk and head rotation. 9 A shoulder-amputated patient is not able to support arm swing by muscles with a free-swinging shoulder prosthesis. Therefore the artificial limb behaves like a pendulum. The effect of pendulum movements on the gait pattern of upper limb amputees is not described in detail today. Bierwirth 2 only noticed that the pendulum movements of the prosthetic arm are low. Collins et al. demonstrated this swinging behaviour in a test using a model. 10 Li et al. described that the free vertical moment grows due to missing arm swing. 11 Amputation and prosthetic fitting in the upper limb region lead to specific pathological movement patterns. According to the author’s knowledge, there is very little information on the influence of these upper limb movement patterns on the total load conditions of the locomotor system during walking and standing.
Umberger explained in his study that reduced arm swing leads to a significant increase of the gross and net rate of metabolic energy by 5.0% or 7.7%, respectively. In addition, the knee moment increases if arm swing is reduced in the sagittal plane. 12 Detailed findings in this field may optimize prosthetic fittings and increase the acceptance of prostheses.
In the present study, for the first time upper limb prostheses were studied considering important load parameters relevant to the lower limbs. Based on biomechanical parameters this is a contribution to objectify the effect of different types of prostheses on standing and walking of patients with a unilateral shoulder disarticulation.
Methods
Subjects
The tests of this investigation were conducted in eight subjects with unilateral shoulder disarticulation. Six patients lost their arms due to trauma and the rest of the subjects, due to tumour or sepsis. The mean time since amputation was 14 ± 9 years (4–27 years). Patients had been using their prostheses for 9 ± 9 years (0–27 years) on average. One of the patients was fitted for the first time during this study even though he had been amputated 23 years ago. The mean age of the patients was 44 ± 13 years (29–71 years), the mean height 179 ± 8 cm (169–190 cm) and the weight 97 ± 22 kg (73–142 kg).
The control group consisted of six healthy subjects to obtain the physiological reference values for this study. The mean age was 27 ± 3 years (24–30 years), the mean height 176 ± 4 cm (170–180 cm) and the weight in this group was 79 kg ± 15 kg (62–95 kg).
Prosthetic fitting
To test the components in each patient, an individual test socket was fabricated under identical conditions. The prosthesis was equipped with the shoulder joint MovoShoulder Swing (Otto Bock, D).2,3 This shoulder joint allows free swing in the sagittal plane. Free swing is controlled by means of a friction adjustment screw. In addition, the shoulder joint permits damped swing in the frontal plane. The DynamicArm® (Otto Bock, D) 13 was selected as the elbow joint. This joint is controlled without harnessing making it especially suitable for shoulder amputees. Due to the Automatic Forearm Balance (AFB) unit integrated in this elbow joint, the swing characteristics of the forearm can be individually adjusted and reproduced.14,15 In all prostheses the setting of the AFB unit of the DynamicArm® was reduced under maximum tension by five full turns of the adjustment screw. The slightly increased weight compared to other components provided an improved compensation of the weight of the amputated arm and was another reason to choose this elbow joint. The System Electric Hand (Otto Bock, D) was used as the prosthetic hand.
Instrumentation
For the measurement of static loads the L.A.S.A.R. Posture device (Otto Bock, D) was used. 16 This device allows for visualization of the centre of pressure of the ground reaction force by a laser beam and to define the distances between the line of action of the vertical ground reaction force (load line) and the rotational axes of the joints.
The gait parameters were biomechanically analyzed during level walking using two force plates (Kistler, Winthertur, CH) and six optoelectronic cameras (VICON, Oxford Metrix, UK). Both systems are controlled by a data processor and synchronized via a light barrier signal. The optoelectronic cameras determine the coordinates of reflecting markers with a measuring frequency of 120 Hz. The markers are attached to anatomical landmarkers of the amputee and the prosthesis according to Ludwigs et al. 17 The shoulder girdle rotation was determined as depicted in Figure 1.
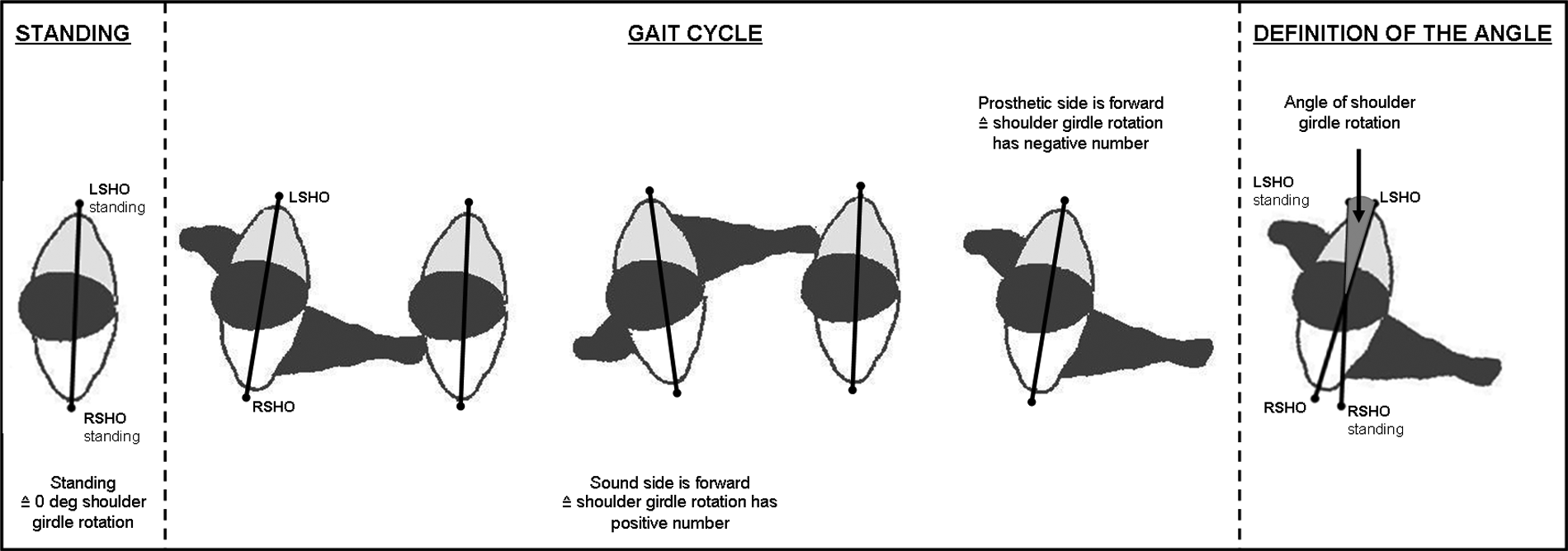
Determination of the shoulder girdle rotation.
The force plates measure the ground reaction forces for both sides of the body during the gait cycle. The external sagittal moments considered in this study were calculated based on the ground reaction forces and the coordinates of the joint axes using the method described in an earlier paper. 18
Measurement procedure
At the beginning of the investigation, the static condition of each subject was analyzed with and without the prosthesis. For this purpose, the distances from the load line to the joint rotational axes of the lower limbs in the sagittal plane and to the ankle and centre of the knee in the frontal plane were measured. In addition, in the dorsal view, the distance between the 7th cervical vertebra (C7) and the load line was determined in the frontal plane (Figure 2).
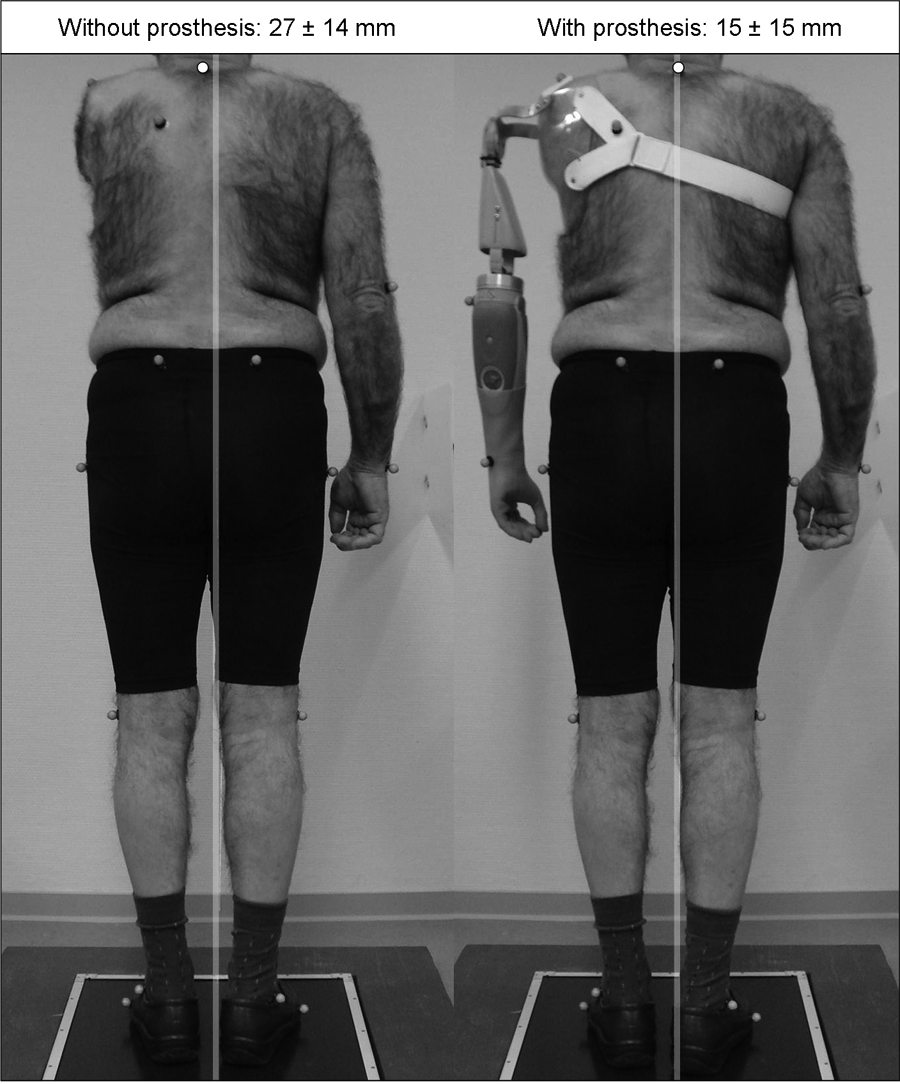
Distance between C7 and load line.
Next, the gait of the subjects was analyzed in the following three situations: without the prosthesis, with the prosthesis with locked shoulder joint – simulating a prosthetic socket without a shoulder joint – as well as with a free-swinging shoulder joint. Measurements were performed in random order. In both cases with a prosthesis, damped swing of the joint in the frontal plane was allowed. To identify the mean value, the patient practices for a distance of approximately 12 m at a self-selected speed, repeating this nine to 12 times.
For each gait parameter, a representative mean value was calculated for each subject based on these nine to 12 single measurements. The results illustrated in the graphs show the mean curve of the mean values of all subjects. The mean values of the biomechanical key parameters were analyzed for significant differences between the test situations using the Wilcoxon test. During the investigation the subjective impressions of the patients were noted.
This study was conducted in agreement with the guidelines of the University of Göttingen Ethics Committee.
Results
Static analysis
On the lower limbs, no relevant differences between the test situations could be identified, neither in the frontal nor in the sagittal plane. The results for the distance between C7 and the load line, however, show highly significant differences in the frontal plane (Figure 2). Without the prosthesis, the body’s centre of gravity is shifted to the non-amputated side. The mean distance between C7 and load line is 27 mm without prosthesis. With a prosthesis the value is significantly reduced to 15 mm (p = 0.01).
Gait analysis – kinematic parameters
The mean self-selected walking speed of the subjects of the control group was 1.44 m/s ± 0.05 m/s. The patient group selected a walking speed of 1.41 m/s ± 0.13 m/s without a prosthesis, 1.42 m/s ± 0.12 m/s with the prosthesis with locked shoulder joint and 1.40 m/s ± 0.11 m/s with a free swinging shoulder joint. Any significant differences between these mean values were not measured.
In the patient group, it is observed in all investigated prosthetic situations, that the non-amputated upper arm segment intensively swings in the sagittal plane (Figure 3). The mean amplitude without a prosthesis is 33.0 degrees. When wearing a prosthesis with a locked shoulder joint, swinging of the non-amputated arm is significantly reduced to 23.4 degrees (p = 0.02). If the prosthesis can freely swing in the shoulder joint, the flexion angle significantly decreases to 25.5 degrees (p = 0.01) compared to the situation without prosthesis. The amputated side with a locked shoulder joint swings 5.5 degrees. If the shoulder joint is set to free swing, the upper arm segment angle is significantly increased to 11.3 degrees (p = 0.01).
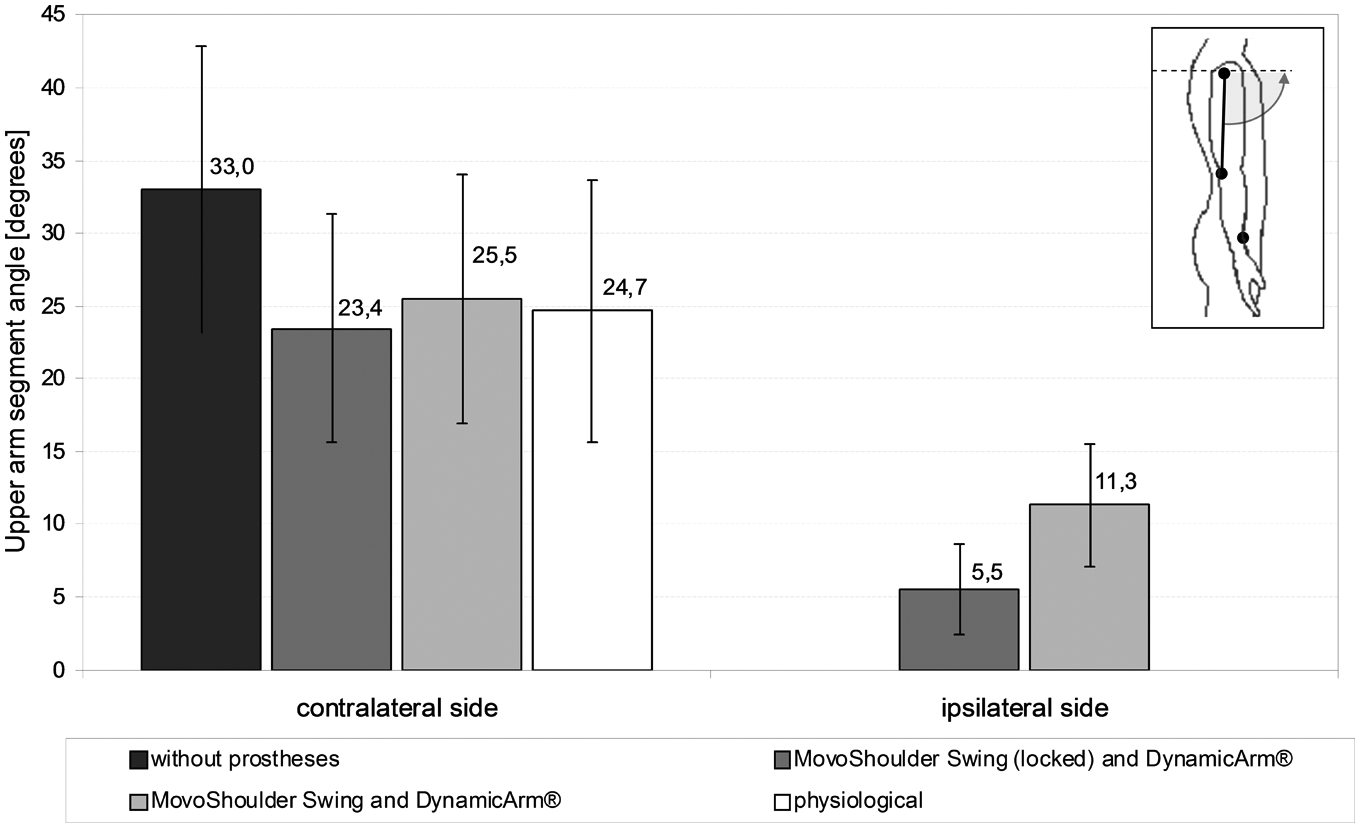
Mean range of shoulder motion during level walking in sagittal plane with standard deviations.
In the elbow joint of the non-amputated arm in the sagittal plane, similar effects can be observed (Figure 4). The amplitude of the forearm segment angle without prostheses is 32.1 degrees. When the prosthesis is used, the forearm segment angle of the contralateral side is significantly reduced. With a locked shoulder joint the maximum angle is 29.1 degrees (p = 0.01). If the shoulder joint is unlocked, the forearm swings 27.8 degrees (p = 0.04) compared to the situation without a prosthesis. With a locked shoulder joint, the forearm of the amputated side swings 12.9 degrees. If the shoulder joint is set to free swing, the forearm segment angle is 12.1 degrees. The difference between both prosthetic situations is not significant.
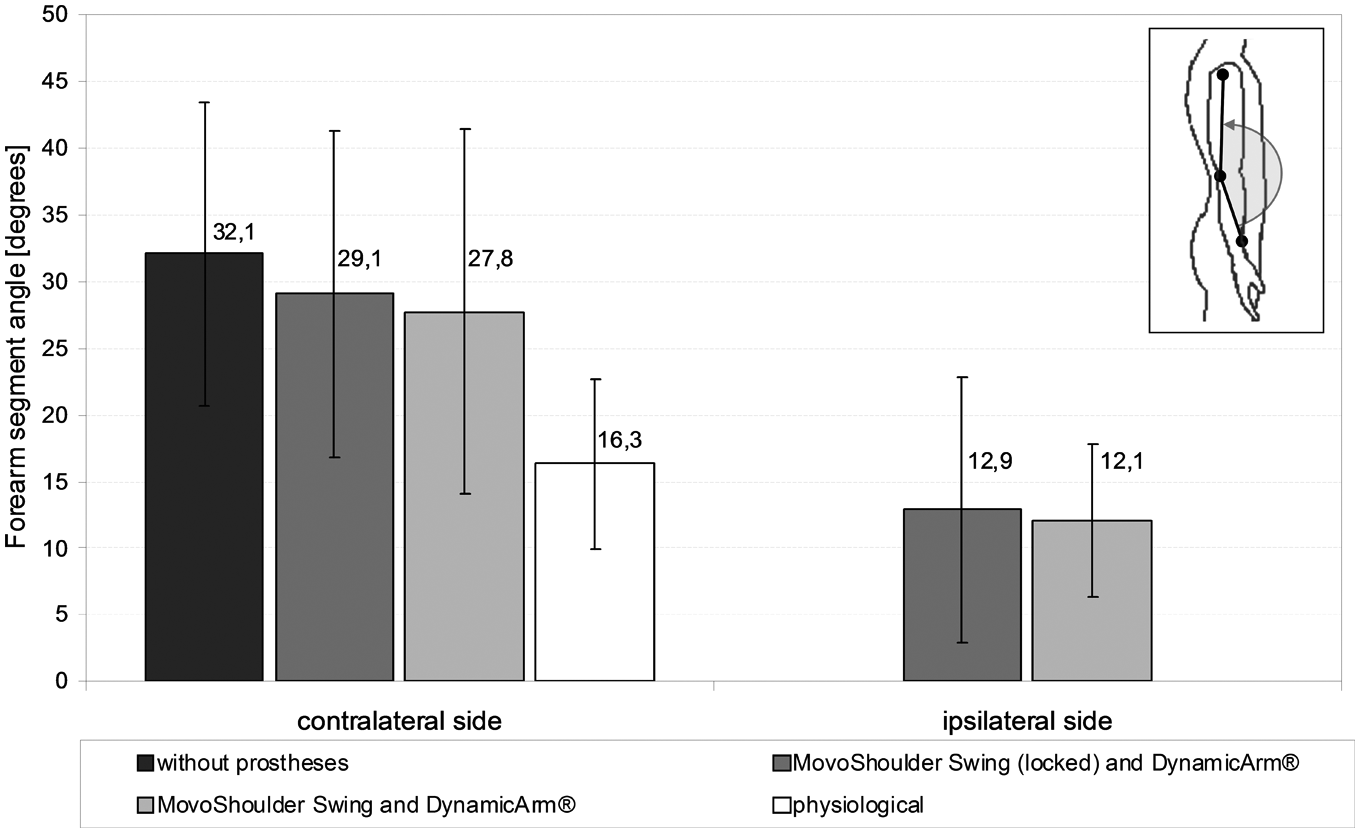
Mean range of forearm motion in sagittal plane with standard deviation.
The values of the contralateral shoulder are used to illustrate the results of shoulder rotation. Thus the position of the measuring point was identical with all subjects. In early stance phase, the non-amputated shoulder shows a mean backward rotation of -6.4 degrees without the prostheses (Figure 5). With the locked shoulder prosthesis, the mean angle reduces to -3.8 degrees compared to the situation without a prosthesis. The reduction is insignificant (p = 0.07), shows, however, a clear tendency. If the shoulder joint can swing freely, backward rotation decreases significantly compared to the mean value without prosthesis to 3.7 degrees (p = 0.04).
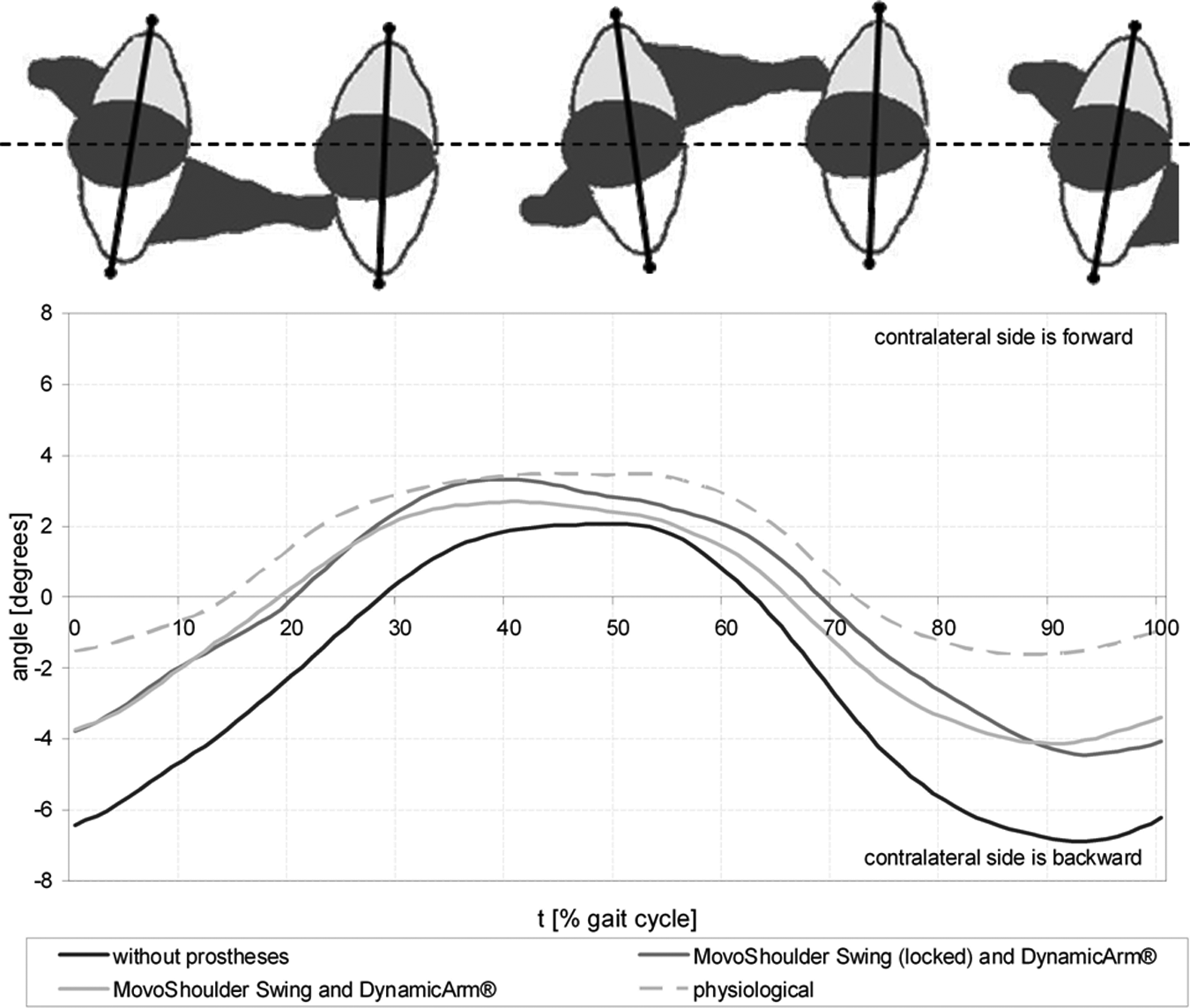
Shoulder rotation of the contralateral side during the gait cycle.
Gait analysis – kinetic parameters
The analysis of joint moments shows prosthesis-dependent effects, primarily with respect to the external moment acting on the knee joint in the frontal plane. Further kinetic results did not reveal any significant differences between the tested prosthesis situations. The result of the varus/valgus moment of the knee is presented in Figure 6. Without a prosthesis, a mean maximum varus frontal moment of 0.66 Nm/kg on the amputated side is found. If the prosthesis with locked shoulder joint is used, the value reduces without significant proof to 0.62 Nm/kg. The freely swinging shoulder joint causes a significant reduction of the mean maximum frontal moment in the amputated knee to 0.58 Nm/kg (p = 0.02). Without a prosthesis, the varus moment of the knee on the non-amputated side is reduced to 0.50 Nm/kg compared to the prosthetic side. When wearing the prosthesis with a locked shoulder joint, a varus moment of 0.53 Nm/kg is measured. With the freely swinging shoulder joint, the moment amounts to 0.54 Nm/kg. Any significant differences between the mean values of the contralateral limb were not identified, however, there seems to be a clear tendency.
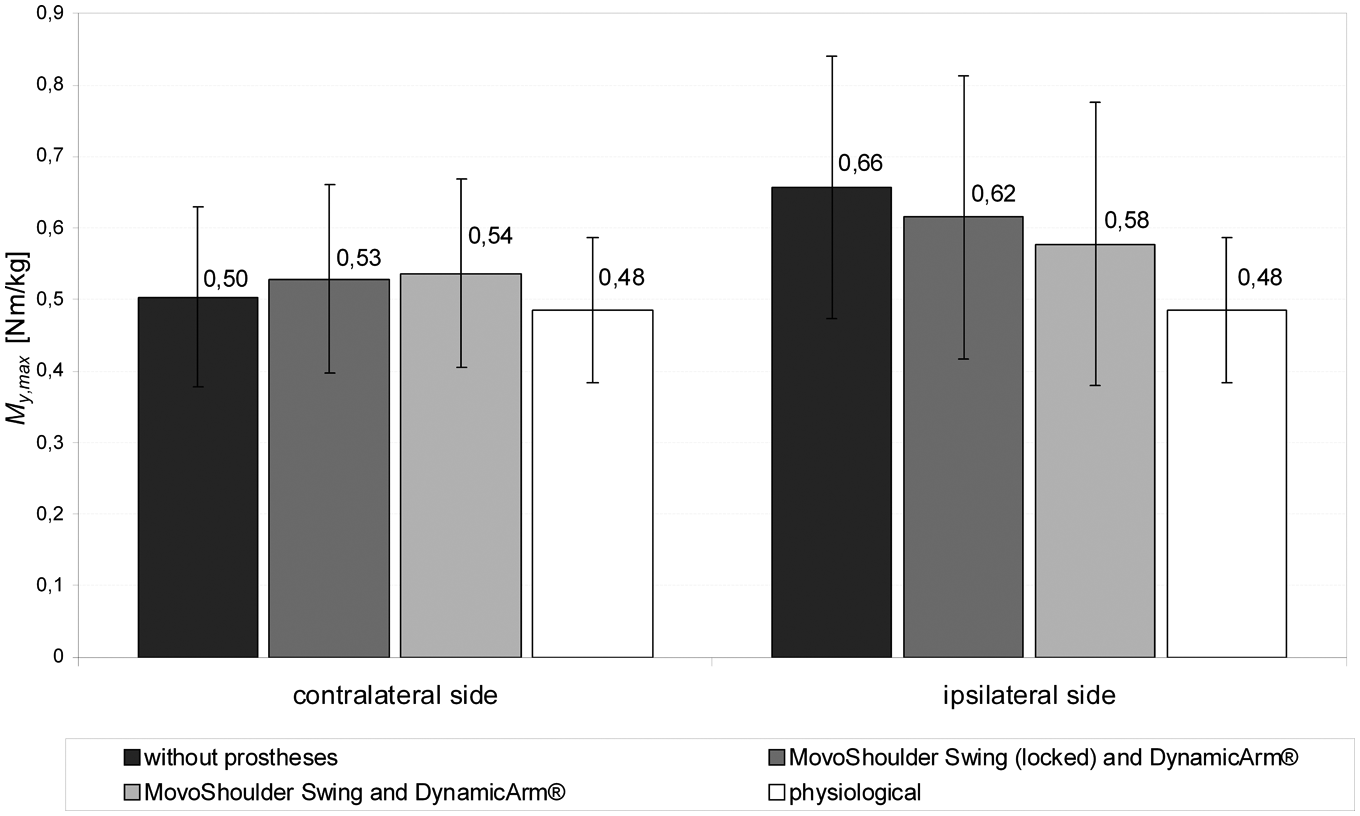
Mean maximum values of the external moment acting on the knee joint in frontal plane.
Subjective evaluation
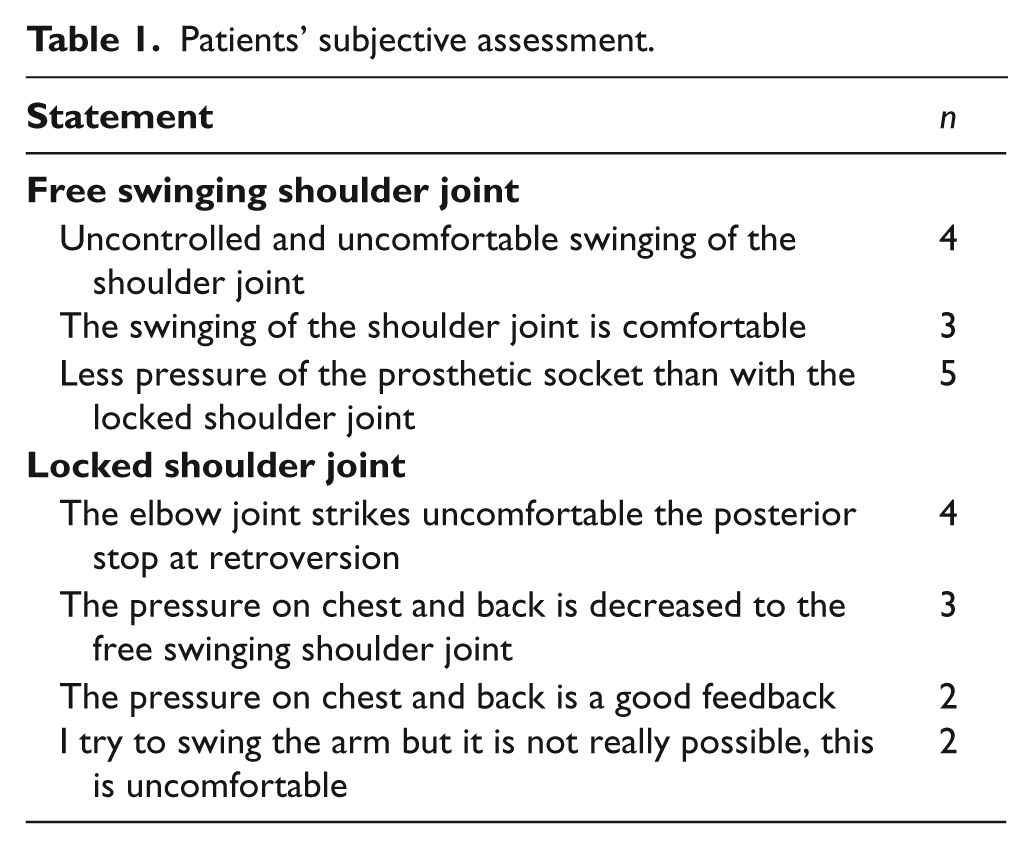
The results of subjective assessments are summarised in Table 1.
Patients’ subjective assessment.
Discussion
Prosthetic fitting of the shoulder region has the objective to restore the natural function as best as possible. The patient is supported in his daily activities. Appearance is another important aspect. When wearing clothes, restoring of a uniform appearance is desired. 19 This study aimed at describing the biomechanical benefits of a shoulder prosthesis.
The weight reduction the patient experiences due to an arm amputation amounts to approximately 4.2 kg. 20 Unilateral arm amputations lead to asymmetric body postures caused by shifting of the position of the centre of mass due to the lost weight of the amputated arm. This effect is known in the literature.20,21 If a prosthesis is used, clinical impairments such as poor posture, back pain and so on, may be reduced. 20
The study revealed that a standard prosthetic system with a weight of approximately 2.4 kg may reduce this asymmetry by 45% on average. The prosthesis clearly supports the patient’s upright posture. This is confirmed by Greitemann. 21 In addition, Greitemann explained that muscular and static asymmetries and poor posture could be reversed by compensation of the weight of the amputated arm under the condition that the treatment had started as soon as possible after amputation. Therefore early prosthetic fitting with adequate physical and occupational therapy is required to minimize long-term effects, such as scoliosis.
The measurements of the study were primarily based on biomechanical parameters of walking that are in principle velocity dependent. However, as in all investigated situations only insignificant speed differences of maximum 0.04 m/s were identified, all measured differences can be discussed regardless of the velocity aspect.31,32
Without a prosthesis, extensive swinging of the patient’s contralateral arm at the shoulder and the elbow level is observed. When the prosthesis is used, swinging of the contralateral arm is reduced approximating the physiological movement pattern. This is independent of whether the prosthetic arm freely swings or the shoulder joint is locked. The compensating weight of the prosthesis is sufficient to cause the contralateral arm to swing more physiologically. It could be assumed that the effects of the body’s obliquity are compensated by extensive swinging of the contralateral arm. In addition, the prosthetic arm is not directly driven by muscles. Therefore, the swing movement of the prosthetic arm has to be imitated by the trunk.
Bierwirth 2 describes the advantages of a freely swinging shoulder joint. The pendulum movements that are transferred during walking to the prosthetic shoulder socket are eliminated. The results of the present study show that the upper arm segment angle on the amputated side is clearly reduced in the sagittal plane as compared to the physiological reference values (Figure 3). Thus Bierwirth’s findings are confirmed. Although the shoulder joint is completely locked, a mean range of motion of 5.5 degrees is measured. This movement results from the residual limb-socket-pseudoarthrosis between socket and trunk. All measurements were performed using a shoulder cap of polyethylene (Figure 2) that does not provide strong adhesion to the skin. Thus slight relative movement between socket and trunk cannot be avoided. The shoulder angle is only determined by means of the markers attached to the prosthesis (Figure 3). Therefore tilting of the socket on the trunk reflects a movement in the shoulder joint leading to the apparent movement in the locked prosthetic shoulder joint.
As described by Greitemann, 21 the missing limb causes general trunk torsion with forward rotation of the shoulder on the prosthetic side. This study shows that torsion of the contralateral side in the early stance phase may be reduced by one third when a prosthesis is used (Figure 5). Again, it does not matter whether the prosthetic arm freely swings or the shoulder joint is locked. Weight compensation, as described by Greitemann, is the distinctive factor for optimized forward rotation of the shoulder.
The analysis of joint loading has clearly confirmed that, without a prosthesis, the external varus moment acting on the knee joint of the ipsilateral side is unphysiologically increased. Numerous studies verify that values of this magnitude are characteristic for patients with varus osteoarthritis. If such values are measured in healthy subjects, the risk of contracting this joint disease in the long term is increased.22-26 This has the following biomechanical background: increased varus moments correlate with increased joint forces in the medial compartment, a fact that has been proven by means of biomechanical models.27,28 Our results document that the external varus moment is significantly reduced when a shoulder disarticulation prosthesis is used, contributing to more natural joint loads. The assumption that the more symmetric mass distribution in the upper body provided by the prosthesis leads to lateral shifting of the ground reaction force acting on the ipsilateral limb during stance phase of the gait cycle may be a first explanatory approach. The effective lever arm of the ground reaction force at the knee joint as well as varus moment and joint force are reduced. In addition the results give reason to conclude that the more natural the prosthetic arm movement, the stronger the beneficial effect. Figure 6 demonstrates that the weight compensation is still insufficient. Only with free swing of the shoulder joint, loads are equally distributed over to both knees. In addition, the prosthetic arm is uncoupled from the trunk. The moment of the swinging arm is no longer transferred to the prosthetic socket and the patient. Furthermore, the maximum of the varus moment in the knee of the amputated side is reduced. The data of the control group originate from an earlier study. The differences in the mean age are not relevant as we know from the literature that only people over 60 show clear age-related changes of the gait pattern. 29
The patients’ subjective impressions are confirmed by Bierwirth, 2 Kloss 3 as well as Wutzler. 5 They described the beneficial relief of the prosthetic socket, if the shoulder freely swings. The locked joint generates increased pressure on the chest and back region. Three subjects perceived this as uncomfortable and one of them felt uncomfortable pressure on the scar tissue. This effect increases if the elbow strikes the posterior stop. The pressure of the prosthetic socket with an unlocked shoulder joint is minimized. Swinging of the prosthetic arm with very little friction was perceived as uncontrolled movement by four patients (Table 1). The shoulder joint used allows for adjustment of the free swing friction. If the friction resistance is increased, a slight pressure on the chest and back is produced during walking. This feedback is sufficient to give the patient a perception of improved control.
Limitations
Only a small percentage of upper limb amputations are shoulder disarticulations. 30 For this reason, a group with only eight subjects could be enrolled for this study. Prior to this study, the patients had only been familiar with their existing prosthetic system. Therefore the period for adaption to the situations to be measured was rather short. The present data do not allow a conclusion, whether the use of a shoulder disarticulation prosthesis also changes the load situation of the spine. In future studies, the gait analysis data could provide the basis for calculating load parameters by means of constructed biomechanical models. This would allow for an even more complex assessment of changes in loads of the locomotor system caused by using such a prosthesis.
Conclusion
From the biomechanical point of view, unilateral shoulder disarticulation patients benefit greatly from modern prosthetic systems as described in this paper. This study shows that the patient’s body posture is significantly improved by using a prosthesis. Compensatory movements, such as abnormal swinging of the contralateral arm, are reduced. In addition, unphysiological loading of the knee joint decreases if the prosthetic shoulder joint freely swings in the sagittal plane.
Footnotes
Acknowledgements
The authors gratefully acknowledge Anett Elsner, Sandra Ramdial and Dr Andreas Kannenberg for their valuable contribution to the preparation of this manuscript.
The authors state no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors