
Abstract
Background and aim:
When a mandibulectomy causes discontinuity, the patient will need a rehabilitative prosthesis to achieve a proper occlusal relationship.
Technique:
This article describes step-by-step guidelines for measuring the patient-specific mandibular guide flange angulation. In the presented technique, the flange angulation is determined by dividing the horizontal overlap of the maxillary posterior teeth plus the maxillary buccal clasp thickness by the vertical distance of the mandibular continuous clasp up to the maxillary buccal clasp.
Discussion:
The mandibular guiding flange prosthesis must achieve an angulation that is appropriate for the particular circumstances of each patient to minimize the complications with mandibular deviation.
Clinical relevance
The introduced method for measuring the patient-specific mandibular guide flange angulation can help prosthodontists to prepare the mandibular guiding flange prosthesis with higher accuracy and predictability.
Keywords
Background and aim
Deviation, rotation, and retrusion of the mandible are debilitating problems for maxillofacial patients with mandibular discontinuity, which cause the residual segment of the mandible to rotate inferiorly upon closure and deviate toward the resected side and be retruded compared to presurgical positions.1–3 Reconstruction of mandibular continuity using a bone graft or metal plates at the time of surgery can resolve most of the patient’s problems.1,2 Left unsolved, however, the deviation will cause loss of occlusion on the nonresected side and an anterior open bite that can affect the patients’ speech, swallowing, control of salivary secretions, and esthetics.1,2,4
Although challenging, prosthetic rehabilitation of such patients to achieve acceptable occlusal function can be obtained by using a palatal- or mandibular-based guidance prosthesis. 2 In a mandibular-based guidance prosthesis, the guide flange is attached to a mandibular removable partial denture (RPD) on the nonresected side. The flange is extended into the maxillary buccal fold, to guide the remaining segment of the mandible superiorly and laterally to the proper jaw relationship. 1 “The flange mechanically maintains the residual mandible in the proper position for the vertical chewing stroke, with little or no lateral movement.”3,5–7 This extension may be processed in acrylic resin, casted with RPD alloy, or a heavy wire loop may be used.6–12
Although acrylic flanges are adjustable in the mouth, they are susceptible to abrasion and lack rigidity, thus requiring additional thickness or metal support. Metal flanges can be thin and rigid, will not assault the cheek space, and will not distort or abrade. However, metal is not modifiable in the patient’s mouth; therefore, the angle and length should be predicted before casting. It has been proposed that the flange “extend 7 to 10 mm superiorly and diagonally from the mandibular RPD, shorter than the maxillary vestibular depth.”3,4,8 However, individual differences in the jaw relationship, amount of mandibular deviation, muscular potency, and ability to guide the mandible toward the nonresected side have necessitated more exclusive methods of determining the flange angulation. The aim of this article is to present guidelines for determining the patient-specific inclination for the mandibular guide flange.
Technique
Manipulate the patient’s mandible to the proper relationship with the maxilla. Adjust the occlusion, if indicated.
Make an accurate definitive impression of the maxillary and mandibular jaws. Ask the patient to close his/her mouth toward the nonresected side (or guide the patient’s mandible to proper intercuspation, if required) and record the interocclusal relationship.
Mount definitive casts using the face bow and jaws’ relation records.
Survey the maxillary cast and design the framework. Wax up the RPD against the mandibular cast. Involve most of teeth in the maxillary framework design to provide cross-arch stabilization. Provide buccal clasps for the maxillary premolars and molars on the nondefected side to protect them against abrasion and excessive stress that are caused by contacting the mandibular flange. For accurate measurement of the maxillary buccal clasp thickness, wax up of the maxillary framework should be completed before the mandibular flange wax up. The maxillary RPD framework should preferably be casted before the mandibular frame and flange wax up for appropriate occlusal relationship (Figure 1).
Mount the mandibular refractory cast against the maxillary cast and frame, using the jaw relation record.
Survey the mandibular cast and design the framework. Wax up the mandibular framework. The guiding flange will originate from the buccal continuous clasp on the mandibular premolars and molars on the nondefect side.
The guide flange makes an angle with the mandibular framework (α) that is calculated using the following formula (Figure 2):
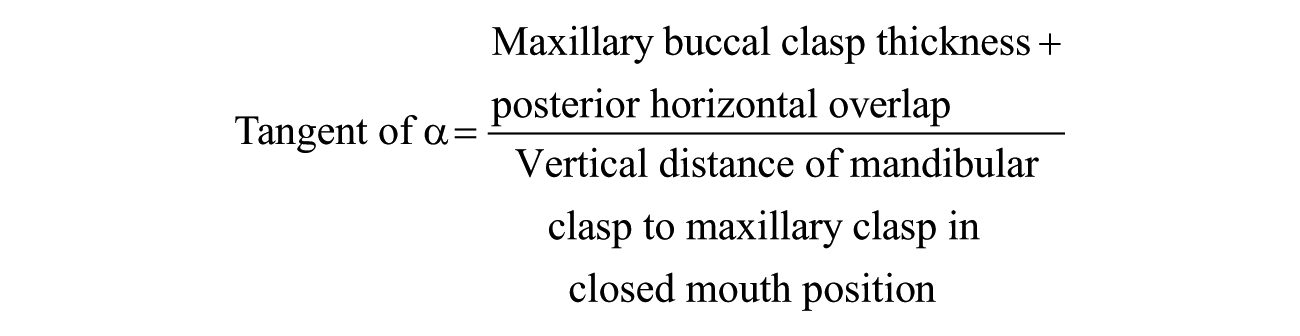
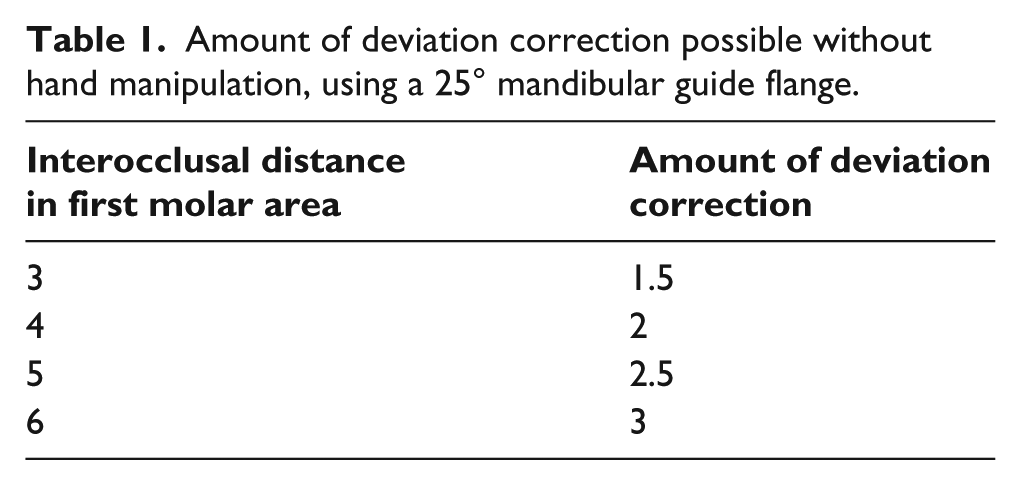
After calculating the angle of the guiding flange, the amount of correction for the horizontal deviation can be calculated according to the amount of the interocclusal distance in the first molar area. For example, if the mean horizontal overlap of the posterior teeth is 2 mm, 13 the maxillary buccal clasp thickness is 2 mm, and the vertical distance between the mandibular clasp and maxillary clasp is 8 mm, then the tangent of α is (2 + 2) ÷ 8 = ½ and α is about 25°. In this angulation, if the mandible is opened 3 mm in the molar area, then 1.5 mm of horizontal deviation correction is possible without manipulation (Table 1).
Wax up the mandibular guide flange using 14-gauge wax (1.63 mm) with the calculated angle, and connect it to the mandibular RPD wax up. Cast the RPD with selected alloy and prepare the framework using routine procedure.
Ask the patient to close her/his mouth toward the intact side while both frames are in the mouth. The guiding flange should be evaluated for smooth guidance of the mandible into appropriate occlusion. Complete the RPD. Add the teeth (if indicated), evaluate, and process.

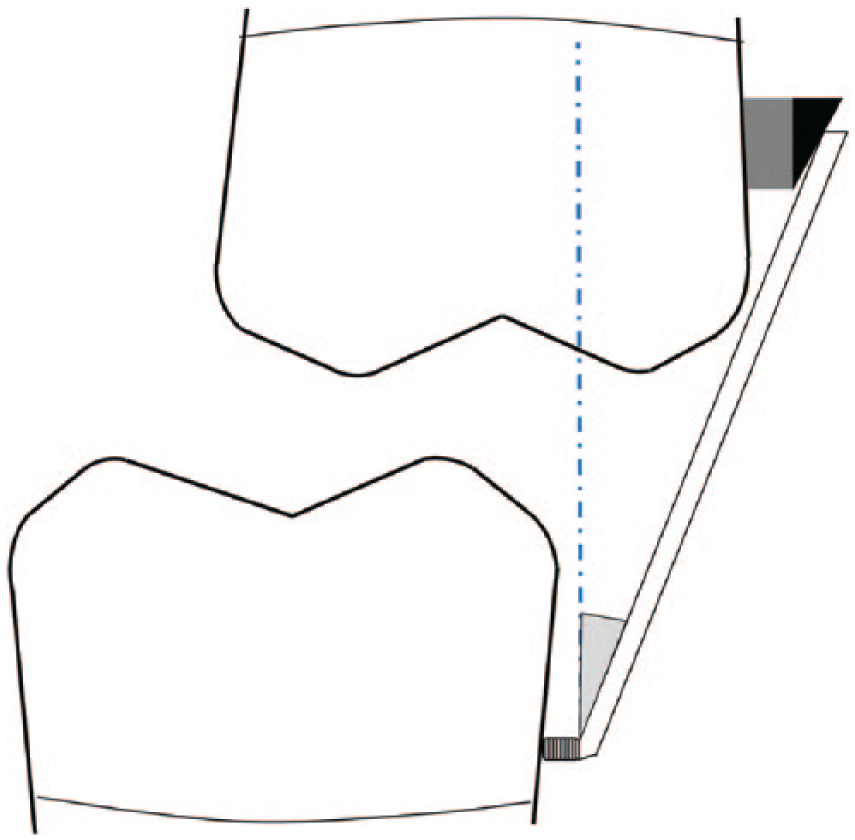
Mandibular prosthesis casted before maxillary framework. After positioning, the horizontal overlap was inadequate.
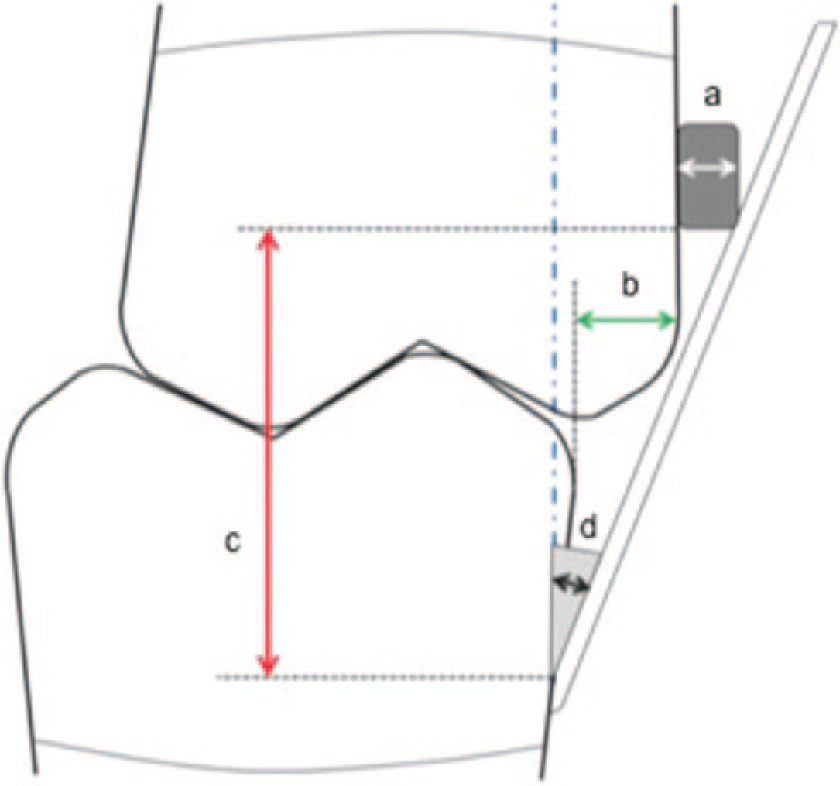
Overall schematic illustration of mandibular guiding flange. The details are demonstrated with arrows. (a) Maxillary buccal clasp thickness, (b) posterior horizontal overlap, (c) vertical distance of the mandibular clasp to the maxillary clasp, and (d) angle of connection.
Amount of deviation correction possible without hand manipulation, using a 25° mandibular guide flange.
Suggest physiotherapy to the patient, to assist in improving the symmetrical arc of closure and finding the centric occlusion position without manual manipulation of the mandible. 6
Discussion
Guide flange prostheses are used in patients with mandibular discontinuity to correct the resulting deviation of the mandible and achieve acceptable occlusal function. In this article, flange angulation is determined by dividing the horizontal overlap of the maxillary posterior teeth plus the maxillary buccal clasp thickness by the vertical distance of the mandibular continuous clasp up to the maxillary buccal clasp.
The presented process could be compared with the Beumer method. Specifically, Beumer et al. 4 proposed to take an interocclusal wax record in 3 mm of the posterior opening while the mandible is deviated toward the nonresected side and to determine the ramp angulation according to this record. It has also been proposed that the flange “extend 7 to 10 mm superiorly and diagonally from the mandibular RPD, shorter than the maxillary vestibular depth.”3,4,8 However, the presented method of determining the guiding flange angulation can help prosthodontists to prepare the mandibular guiding flange prosthesis with higher accuracy and predictability. As an acrylic resin, flange can be refined in the patient’s mouth and its inclination is correctable; this technique is primarily introduced for metal flanges; however, it can also be applied to acrylic flanges, to reduce flange adjustment in the prosthesis delivery session.
Excessive angulation of the flange could violate the maxillary buccal mucosa and leave an irritating space between the flange and the maxillary alveolar mucosa in the closed mouth position. This angle could be reduced by increasing the mandibular buccal clasp thickness or by patient hand manipulation of the mandible toward the nonresected side.
Flange angulation is limited by the maxillary vestibular depth, pulls from the contraction of scar tissue on the resected side, the arch of closure, and the thickness and strength of the buccal mucosa. If the estimated flange angulation in proper occlusion exceeds the patient’s tolerance, it can be reduced by increasing the horizontal thickness of the mandibular buccal clasp to which the guide flange is attached (Figure 3).
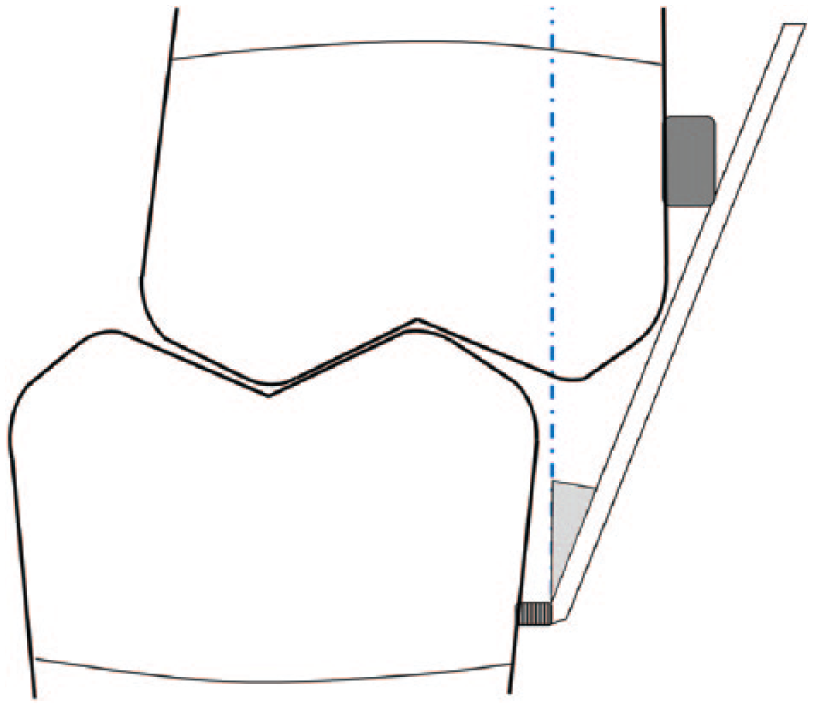
Thickness of the mandibular buccal clasp has been increased to compensate for excessive horizontal overlap of posterior teeth.
On the other hand, if the deviation of the mandible during jaw opening exceeds the amount that can be corrected by the flange at the determined angle (Table 1), and correction of deviation without manual manipulation is desired, then the thickness of the mandibular buccal clasp to which the guide flange is attached should be increased. Additionally, an inclined surface should be formed on the buccal surface of the maxillary posterior teeth, to aid the flange in mandibular guidance and to achieve a proper occlusal relationship. This inclined surface is in the form of a right triangle (Figure 4), with a base length equal to the added horizontal thickness of the mandibular buccal clasp. This design will compensate for the non-correctable deviation of the resected mandible.
In addition to the increased mandibular buccal clasp thickness, an inclined plane has been formed on the buccal surface of the maxillary posterior teeth.
The vestibular depth of the maxillary molar area in the closed mouth position limits the vertical flange length. Excessive length impedes the insertion and removal of the prosthesis. If the mouth opens wider than the measured amount, then manual reengagement of the mandibular guiding flange with the maxillary posterior teeth will be necessary during mouth closure. In this situation, the patient should be instructed to open wide until there is no contact between the maxillary teeth and the flange, manipulate the mandible toward the nonresected side, and then close the mouth. However, restricting mouth opening should be recommended, as this approach will help the patient to return to the proper relationship without excessive effort.
The mandibular guiding flange prosthesis is used from the second week after surgical resection. 4 In subsequent sessions, when the freedom of the mandibular movement has improved, the flange angulation can be reduced by adding acrylic resin to the medial surface of the flange, after creating macromechanical retention in the flange.
Footnotes
Key points
The mandibular guiding flange prosthesis must achieve an angulation that is appropriate for the particular circumstances of each patient. Flange angulation is determined by dividing the horizontal overlap of the maxillary posterior teeth plus the maxillary buccal clasp thickness by the vertical distance of the mandibular continuous clasp up to the maxillary buccal clasp. The guidelines described can be useful to preserve mandibular functions after resection and to minimize the complications with mandibular deviation.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.