
Abstract
Background:
Quality of life is often cited as a key influence in decisions about partial foot and transtibial amputations despite there being no studies comparing quality of life in these groups.
Objectives:
To compare quality of life in people with partial foot amputation or transtibial amputation secondary to peripheral vascular disease and determine factors influencing quality of life in these cohorts.
Study design:
Cross-sectional.
Methods:
Mail-out, mail-back version of the SF-36v2 Health Survey and an adapted version of the demographic section of the Trinity Amputation and Prosthesis Experience Scales–Revised were sent to people recruited through a large metropolitan hospital.
Results:
Both the SF-36v2 mental health component summary and physical component summary scores were comparable in the partial foot amputation (n = 10) and transtibial amputation (n = 23) cohorts. A multivariate linear regression showed that age, time with diabetes and the presence of retinopathy significantly influenced either the SF-36v2 mental health component summary or physical component summary whereas amputation level did not.
Discussion:
Results support existing descriptive data that indicate quality of life is comparable in cohorts with partial foot and transtibial amputation.
Conclusion:
Our results suggest that quality of life need not to be a consideration when deciding between partial foot and transtibial amputation for persons with vascular disease. Surgeons and patients may wish to focus on other considerations, such as the relative risk of ulceration and subsequent amputation, when choosing between partial foot and transtibial amputation.
Clinical relevance
The similarity in quality of life between people with partial foot and transtibial amputation helps inform difficult decisions about amputation surgery by focusing on surgery that will reduce the risk of complications and secondary amputation without fear of compromising quality of life.
Background
The global diabetes epidemic is expected to affect 550 million people by 2030, 1 and the increasing incidence is recognised as a major health care challenge.1,2 Along with increased health care costs, there is significant disability that arises from complications including peripheral vascular disease (PVD) and lower limb amputation. 3
Despite the increasing incidence of diabetes and vascular disease, data from industrialised nations show that the number of transfemoral and transtibial amputations (TTA) has fallen. Meanwhile, the incidence of partial foot amputation (PFA) has increased proportionately.4–6 If current trend continues, the incidence of PFA will triple across the first half of this century. 6
The shift to more distal amputation has been influenced by improvements in diabetic care – better management of diabetes at a community level,7,8 greater access to specialist high-risk foot clinics, 9 as well as advances in revascularisation surgery 10 – that have made PFA an increasingly more feasible option where previously a TTA may have been necessary. There is also a strong preference for PFA given the belief that surgical and functional outcomes are improved compared with TTA.11–13
Recent expert opinion has called into question this preference,14,15 highlighting that 30%–50% of people with a PFA experience complications such as dehiscence, ulceration and wound failure. By comparison, these complications affect just 10%–20% of people with TTA.12,16–18 Subsequent amputation surgery on the same limb is necessary in about one-third of people with PFA, more than double that observed in people with TTA.17,18 Efforts to achieve wound healing in people with PFA often occur over many months and come at a considerable financial and personal cost. 16 By comparison, healing of the TTA residuum tends to be much more predictable and comparatively short. 19
The high rates of complications and secondary amputation affecting people with PFA are of particular concern given that many functional outcomes are similar in people with PFA and TTA. For example, once the metatarsal heads are affected, walking is virtually indistinguishable between people with PFA and TTA.14,20,21 The limited literature describing energy expenditure suggests this outcome is also similar between people with PFA and TTA.14,22,23 The similarities in functional outcomes between PFA and TTA have turned attention to more holistic measures such as quality of life (QoL).14,24
Based on a recent systematic review, 24 just two studies report QoL data for people with PFA or TTA secondary to diabetes and PVD.25,26 Neither of these investigations were designed to compare QoL in people with PFA or TTA and as such, there is only descriptive data available. These data suggest that QoL may be very similar for people with TTA and PFA.
The paucity of research comparing QoL in people with PFA and TTA has allowed poorly evidenced beliefs to perpetuate. For example, QoL is thought to be better in people with PFA because of the ability to ambulate short distances without a prosthesis.11–13 However, physical functioning has been shown to be a poor predictor of QoL, 27 and persons with limb loss report that social support and participation are more important than physical functioning. 28 It may be that the poor wound healing, readmissions to hospital and higher risk of revision surgery associated with PFA have a greater impact on QoL than does the comparative ease of being able to walk to the toilet at night without a prosthesis. 14
There is a compelling need for research that compares QoL in groups with PFA and TTA secondary to vascular disease. Given that there are no experiments that compare QoL in people with PFA and TTA, and only descriptive data available in the literature, there is inadequate evidence to inform decisions about amputation surgery from a QoL perspective. Similarly, there is inadequate data to inform decisions about the sample size requirements for such an experiment, particularly given the need for sophisticated inferential analysis techniques that can control for the confounding influence of demographic and health factors (e.g. age, sex, duration of diabetes, the presence of diabetic complications such as retinopathy, neuropathy and nephropathy as well as time since amputation) that have all been shown to influence QoL.29–34 Results from a pilot study might provide preliminary evidence to assist patients and surgeons to make a more informed decision about the level of amputation from a QoL perspective and guide future research efforts.
The purpose of this pilot study was to compare QoL in people with PFA or TTA secondary to PVD. We hypothesised that QoL would be comparable in people with PFA and TTA. We also sought to understand which demographic or health factors influenced QoL in these cohorts.
Method
Participants
Participants were recruited through the prosthetics and orthotics department of a major metropolitan hospital. We wrote to all patients who met the following inclusion criteria: adults over 18 years of age, amputation due to vascular disease, either a unilateral TTA or PFA, and minimum 6 months post-amputation given that improvements in QoL plateau 6 months following amputation. 35
Apparatus
The apparatus included a revision to the demographic information page from the Trinity Amputation and Prosthesis Experience Scales–Revised (TAPES-R) and the SF-36v2 Health Survey.
The TAPES-R is a survey designed to measure the psychosocial adaptation of lower limb amputees fitted with a prosthesis.36,37 The demographic section records information including age, sex, cause of amputation and time since amputation. We added additional questions to identify the presence of common complications that have been shown to affect QoL such as retinopathy, nephropathy and neuropathy.29–32 To aid comprehension by participants, we used lay terms from diabetes education sources (e.g. describe retinopathy as ‘eye disease’).38,39 With the modifications, this demographic section will be referred to as the TAPES-R-M.
A range of QoL measures have been used in amputee populations, with little agreement as to the most appropriate. 33 Generic measures (e.g. SF-36) have been criticised for not being sensitive to the psychosocial adaptation involved in limb loss.37,40 Amputee-specific measures (e.g. Prosthetic Evaluation Questionnaire) tend to focus on the prosthesis and do not provide a holistic picture of QoL. Given that we know so little about which domains of QoL are affected by PFA and TTA, and that previous work has reported descriptive data in these groups using the SF-36, 25 we chose to contribute to the creation of a pool of data in people with PFA or TTA by using the same outcome measure.
The SF-36 has a low burden to respondents, taking approximately 10 minutes to complete, and has been shown to be a valid and reliable instrument across a range of populations.36,41 Although there have been no validation studies in an amputee population, it has been widely used, suggesting its widespread acceptance as a QoL measure in this population.42–45
Results from the SF-36v2 are reported using a physical component summary (PCS) and a mental health component summary (MCS). The PCS is a summary of the domains of Physical Functioning, Role Physical, Bodily Pain and General Health. The MCS is a summary of the domains of Vitality, Social Functioning, Role Emotional and Mental Health.41,46
The SF-36v2 differs from previous versions of the instrument in that data are transformed to a ‘T-score’ to facilitate comparison between the different subscales and population norms. Given that the population norm for any subscale is always 50, an individual’s score of 45 would be deemed to be ‘below average’.
Procedures
Ethics approval for this study was granted by the Faculty Human Ethics Committee, La Trobe University and Melbourne Health Human Ethics committees.
The survey package was sent to all potential participants, which included a cover letter, participant information sheet, the SF-36v2 and the TAPES-R-M.
Persons, who wished to participate in the study, returned the survey using the reply-paid envelope. Consent was implicit in return of the survey given that no identifying information was contained in the survey. 47
A reminder letter was sent 2 weeks after the initial invitation, as the response rates for postal surveys can be significantly improved with this approach.48,49
Data analysis
Upon receipt of the surveys, the demographic information was entered into a database. Paper copies of the SF-36v2 were checked for missing items and out-of-range values before entering the responses into the QualityMetric Incorporated Health Outcomes Scoring software (QualityMetric Incorporated, Lincoln, RI) for further processing. 46 The use of such software is recommended to minimise errors with data analysis and makes the process of summing raw scores, transforming data to population-based norm (i.e. T-score) and checking data quality more accurate. 46 Following data entry, results were available for the SF-36v2 PCS and MCS.
The reduced data were entered into IBM SPSS Statistics 22 (IBM Corporation, Armonk, NY) for analysis. To compare QoL between the PFA and TTA cohorts, we used a multivariate analysis of covariance (MANCOVA) given the outcome measure consisted of two related dependent variables (i.e. SF-36v2 PCS and MCS) and the need to control for factors known to influence QoL (i.e. age, sex, time with diabetes, time since amputation and the presence of retinopathy, nephropathy, neuropathy and tissue breakdown). The MANCOVA was conducted following the techniques described by Mayers. 50 Accordingly, we tested for violations of the assumptions of correlation, variance–covariance, normality, multicollinearity and homogeneity of the regression slopes. To better understand factors influencing QoL, we used a standard multivariate regression model in accordance with the techniques described by Pallant 51 including assumption testing for multicollinearity, normality, linearity and homoscedasticity. 51
Results
Of the 122 survey packages sent, 47 were returned and a number were excluded because of incomplete demographic information (e.g. level of amputation had not been specified), insufficient data to calculate the SF-36v2 PCS or MCS scores, participants did not meet the inclusion criteria (e.g. bilateral amputation) or data were deemed to be outliers as described in detail as part of the inferential analysis. As such, data for 33 people were analysed including 23 people with TTA and 10 people with PFA (toes: n = 1, forefoot: n = 5 and midfoot: n = 4).
Participants were representative of the population of interest in terms of their age and sex distribution, time since amputation, duration of diabetes and prevalence of diabetic complications (Table 1). While groups were similar in terms of the proportion with nephropathy, the PFA cohort had double the rate of retinopathy, neuropathy and tissue breakdown (Table 1). Also, the length of time living with diabetes was also lower in the PFA cohort (Table 1).
Clinical and demographic characteristics of the partial foot and transtibial samples.
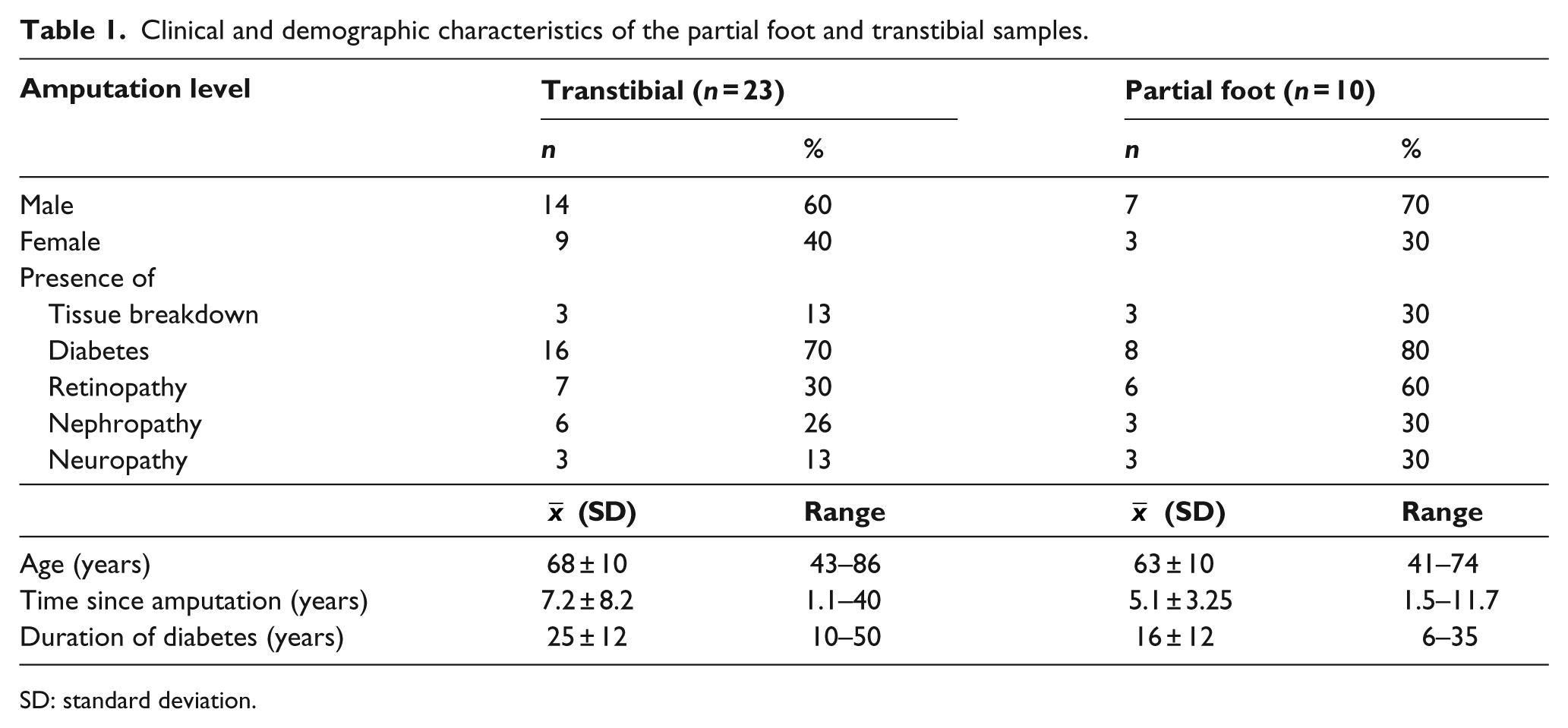
SD: standard deviation.
Comparison of SF-36v2 PCS and MCS between PFA and TTA cohorts was undertaken using a MANCOVA, whereby the influence of covariates – age, sex, time since amputation, duration of diabetes and the presence of diabetic complications including retinopathy, nephropathy, neuropathy and tissue breakdown – was controlled.
Assumption testing showed that the assumption of normality had been violated (Shapiro–Wilk: W = 0.895, df = 35, p = 0.003). Two participants had PCS or MCS scores that were deemed to be outliers based on inspection of the SPSS box and whisker plots. These two cases were therefore excluded from the analysis. With these participants excluded, there was no violation of the assumptions of normality, linearity, multicollinearity, homoscedasticity, correlation between covariates and dependent variables, independence of covariates or homogeneity of the regression slopes.
To understand the influence of the covariates in our comparison of QoL between the PFA and TTA groups, we first ran a multivariate analysis of variance (MANOVA) which showed no significant differences in the SF-36v2 PCS and MCS scores between groups (Wilk’s Lambda: l = 0.964, F(2, 30) = 0.556, p = 0.58, η2 = 0.036). This was confirmed across both dependent variables (PCS (F(1, 31) = 0.077, p = 0.79, η2 = 0.002) and MCS (F(1, 31) = 0.674, p = 0.42, η2 = 0.021)). While the inclusion of covariates reduced the error variance (I = 0.932, F(2, 16) = 0.584, p = 0.57, η2 = 0.68), there was still no statistically significant difference between the groups based on amputation level (PCS (F(1, 17) = 0.184, p = 0.68, η2 = 0.011) and MCS (F(1, 17) = 0.448, p = 0.51, η2 = 0.026)) (Figure 1).
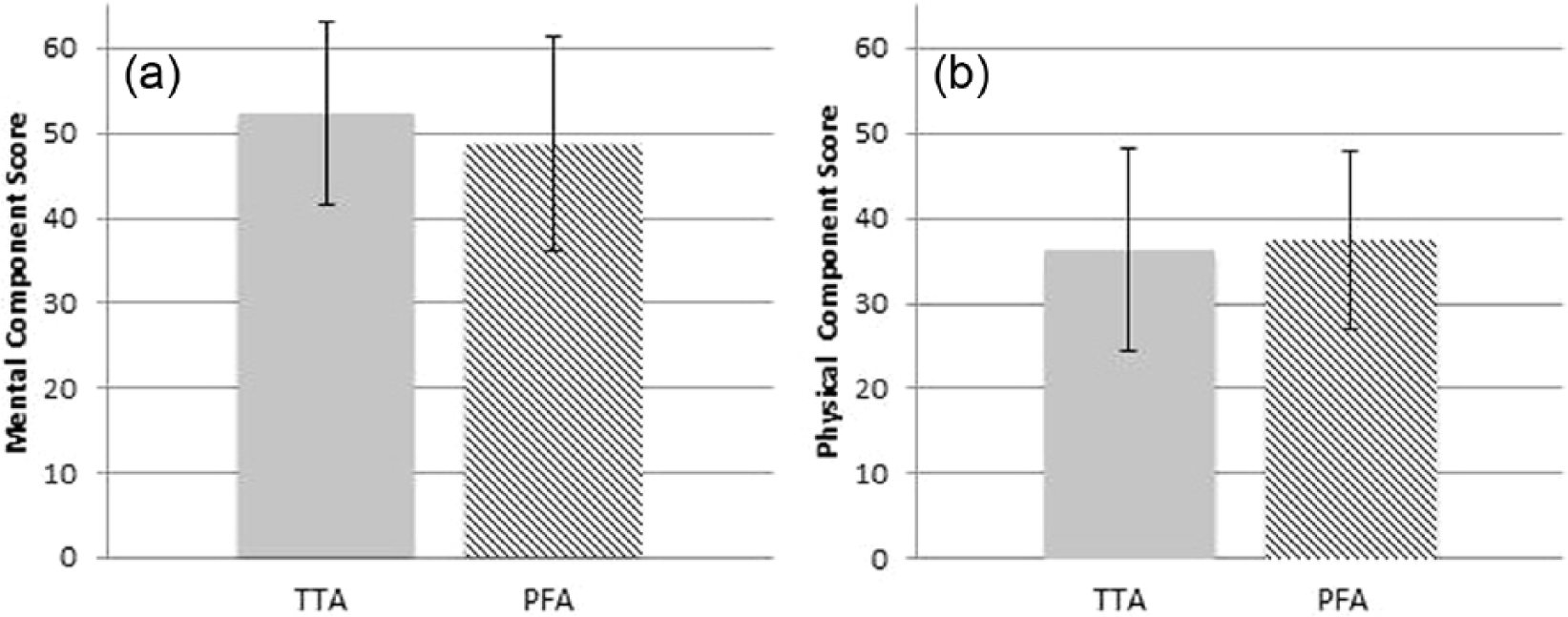
SF-36v2: (a) mental health component score and (b) physical component score for the partial foot amputation (PFA) and transtibial amputation (TTA) groups.
A standard multivariate linear regression was developed to explain which independent variables – age, sex, time with diabetes, time since amputation and the presence of retinopathy, nephropathy, neuropathy and tissue breakdown – explained a significant part of the variance in the SF-36v2 PCS and MCS scores.
Assumption testing for the multivariate linear regression showed no violations to the assumptions of multicollinearity, normality, linearity and homoscedasticity, given that the previously identified outliers were excluded.
PCS score
The regression model explained 47% of the variance in PCS scores (r2 = 0.47), which approached statistical significance (F(9, 23) = 2.229, p = 0.06).
The only independent variables that contributed significantly to the PCS were time with diabetes (β = 0.565, t = 2.874, p = 0.01) and age (β = −0.436, t = −2.149, p = 0.04), explaining 19% and 11% of the variance, respectively. While none of the other variables contributed significantly to change in PCS, retinopathy (β = −0.376, t = −1.818, p = 0.08) and nephropathy (β = −0.399, t = −1.566, p = 0.08) approached significance and each explained a further 8% of the variance. Level of amputation explained less than 1% of the variance in the PCS and was not statistically significant (β = 0.097, t = 0.551, p = 0.59) (Table 2).
Regression coefficients.
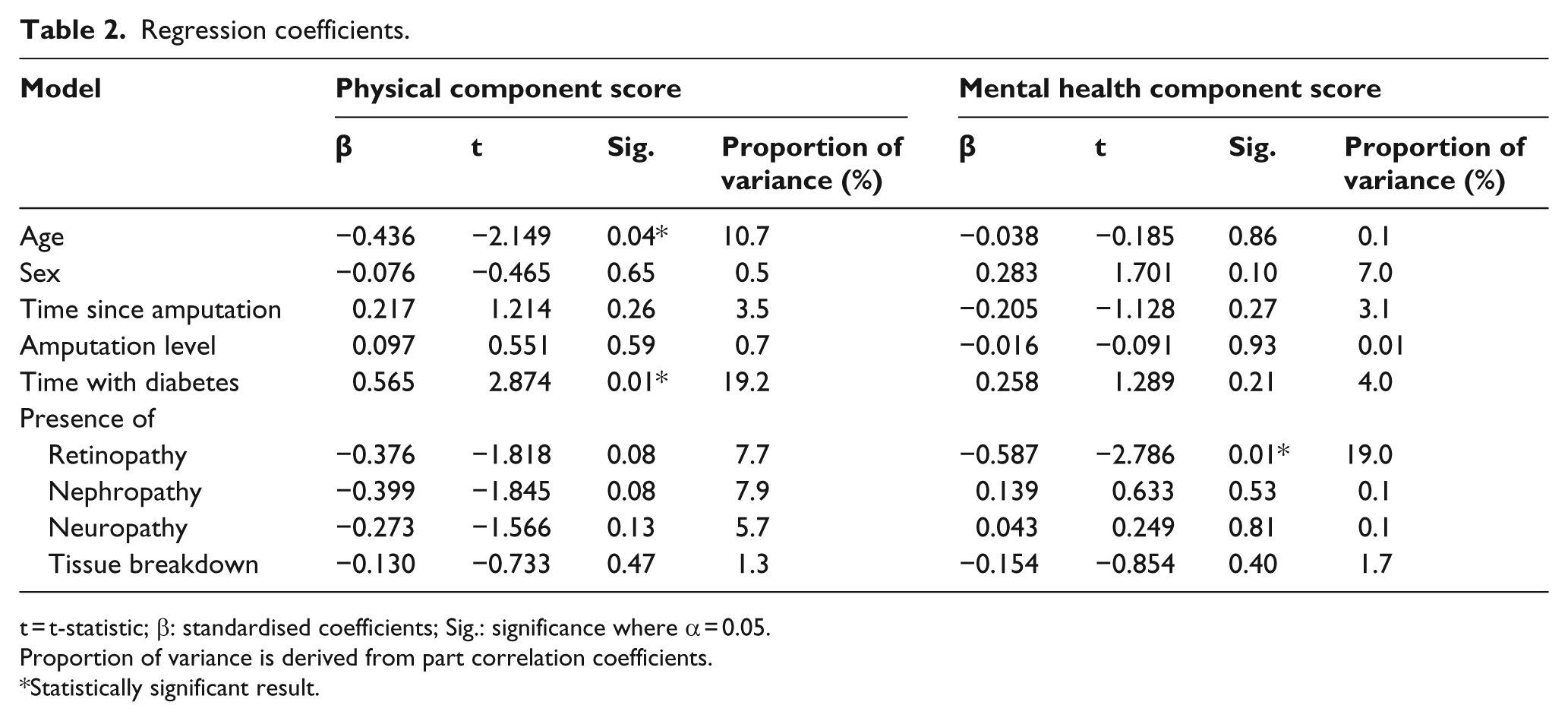
t = t-statistic; β: standardised coefficients; Sig.: significance where α = 0.05.
Proportion of variance is derived from part correlation coefficients.
Statistically significant result.
MCS score
The regression model explained 45% of the variance in MCS scores (r2 = 0.45), which approached statistical significance (F(9, 23) = 2.070, p = 0.08).
Only the presence of retinopathy contributed significantly to the MCS (β = −0.587, t = −2.786, p = 0.01), explaining 19% of the variance. None of the other variables contributed significantly to changes in MCS, including level of amputation (β = −0.016, t = −0.091, p = 0.93), which explained less than 1% of the variance in the MCS (Table 2).
Discussion
In response to our original research question comparing QoL in these two groups, we found no statistically significant differences in either the SF-36v2 PCS or MCS between groups with PFA or TTA.
The level of amputation was not a statistically significant contributor to QoL, explaining just 1% of the variance in the SF-36v2 PCS and MCS. It is noteworthy that the independent variables that influenced QoL in our sample reflect advancing age and systemic diseases (e.g. time with diabetes, retinopathy), factors that are not readily resolved at the point of limb loss.
To the best of our knowledge, this is the first study designed to directly compare QoL in people with PFA and TTA. While previous investigations25,26 were not designed to compare QoL in people with PFA and TTA, the available descriptive data suggest that differences were small and not likely to be clinically meaningful. For example, approximation of the SF-36 MCS and PCS from the eight subscales reported by Boutoille et al. 25 showed similarity with our results. Moreover, the descriptive data reported by Peters et al. 26 also suggest that there was no difference in QoL for persons with PFA or TTA based on the Sickness impact profile (SIP).
Clinical implications
Our preliminary results do not support common beliefs that QoL is better for people with dysvascular PFA compared to those living with TTA.11–13,52 While our findings require corroboration by other investigators, they highlight the need to reconsider the advice given to patients facing difficult decisions about limb loss. Based on our sample, a patients’ age, time living with diabetes and the presence of retinopathy had a significant effect on QoL and should feature in discussions about amputation at the partial foot or transtibial level. We hope this preliminary evidence focuses decisions on factors that influence QoL in these cohorts and not on the perceived differences between amputation at the partial foot or transtibial level. In this way, patients and surgeons might focus their decision-making on other factors such as the disproportionately high risk of comp-lications and revision surgery in PFA compared to TTA.12,13,16–18,53–59
We were surprised that the MCS scores for both the PFA and TTA cohorts were so close to population-based norms, particularly given the effects of chronic disease and complications affecting these groups. 60 Many participants rated their overall health as ‘good’ or ‘very good’ and reported PCS or MCS scores well above the population norm. This suggests that expectations, goals and self-perceived health status may change for some people as their health changes. This phenomenon, known as ‘res-ponse shift’, 61 has been reported in previous studies of QoL in people with amputation.35,62–65 Studies into the process of psychosocial adaptation following amputation have also found that people who strive to attain goals and who have the ability to redefine goals to those achievable with their current health status have higher QoL and better community participation.60,66
While the provision of psychosocial support services following amputation may contribute to improvements in QoL and community participation,60,67 our results suggest that optimal management of diabetes-related complications may also be of benefit.
Limitations and implications for future research
Recruitment for this study was challenging and our experience could help inform future investigations. Identification of large subject samples was difficult given the limitations of hospital records that may not, for example, always stipulate amputation level. We were unable to use data from a number of participants due to incomplete surveys. Large multicentre studies may be required to recruit sufficient participants, and consideration should be given to alternative methods of administering the surveys that make forgetting to complete components difficult. One such option may be to deliver the SF-36v2 in an online format where participation on a global scale is possible, and software could be used to flag incomplete answers before submission.
During the course of our pilot study, we learnt that multivariate linear regression could also be used for the purpose of comparison. In this example, separate regression models would be developed for each of the PFA and TTA groups. The 95% confidence interval of the regression coefficients could then be compared with any overlap indicating that the QoL outcomes were comparable between groups. This certainly extends the typical use of regression for the purpose of prediction or, as was the case in our pilot study, to determine which variables contributed to changes in QoL.
Our pilot work provides some basis for discussing the sample size requirements for future experiments. To inform this discussion, we undertook a sample size calculation for a multivariate linear regression using G*Power 3.1.5 (University of Kiel, Kiel) and data from our pilot study. An a priori sample size was calculated for the transtibial group using a multivariate linear regression: fixed model with R2 deviation from zero. We determined effect size from predictor correlations and halved the alpha level in recognition of there being two dependent variables (i.e. SF-36v2 PCS and MCS). As such, input parameters into the calculation were effect size = 0.48, alpha = 0.025, beta = 0.8 and number of predictors = 8. The required sample of people with TTA would be 46 people. The same sample size calculation would also need to be done to determine the required number of people with PFA; something we were not able to do with any certainty given the smaller number of people with PFA in this pilot study. This sample size estimate should only be considered as indicative. The actual sample required will vary based on the statistical approach chosen, number of independent variables included and the effect size upon which the calculation was based.
Both the amputee cohorts were similar in terms of the distribution by sex, age and number of complications. However, the TTA cohort was larger and had a longer duration of diabetes and time since amputation than the PFA sample. Fortunately, such differences between the cohorts, and their potential to influence QoL, were well controlled for by virtue of the inferential analysis and we would recommend such an approach to other investigators.
We were deliberate in not comparing scores for the SF-36v2 subscales, and some may view this as a limitation. The use of the SF-36v2 PCS and MCS has been developed in order to control ceiling and floor effects seen with reporting of the subscale scores alone. 46 In our investigation, there was no rationale to compare individual subscale scores, as we did not see statistically significant differences between the two amputation levels for the PCS or MCS. 46
It was not our intention to compare groups with different levels of PFA, and some may perceive this as a limitation. Investigators would need to power a study specifically to measure differences in QoL between levels of PFA. Given the many different levels of PFA and our expectation that differences in QoL between groups would be small, such a study would need to recruit a large number of participants. In light of our results, the utility of an investigation comparing QoL in different levels of PFA would need to be carefully considered and justification given for why differences in QoL might exist between levels of PFA.
There may be other variables that are important to include in the regression model. Some authors have noted the influence of depression, anxiety and the presence of phantom or stump pain on QoL,33,34 and future research should consider the appropriateness of these additional independent variables for people with PFA and TTA. This may explain part of the variance not captured in our regression model.
Conclusion
We did not observe significant differences in QoL in groups of people with PFA and TTA from dysvascular causes. In our sample, factors such as age, time living with diabetes and the presence of retinopathy had a significant effect on QoL, whereas amputation level did not. While further research is needed to corroborate these findings, our results suggest that QoL need not be a factor influencing the choice between PFA and TTA. Other factors, such as the high risk of complications and revision surgery, may become more important in decisions about amputation surgery at the PFA and TTA levels, rather than considerations about QoL.
Footnotes
Acknowledgements
The authors wish to thank Associate Professor Brian Hafner for his insightful and valuable comments on the draft version of the manuscript.
Author contribution
Study concept and method design: M. Dillon, M. Quigley, E. Duke. Acquisition of data: M. Quigley, E. Duke. Analysis and interpretation of data: M. Quigley, M. Dillon. Drafting of manuscript: M. Quigley. Critical revision of manuscript for important intellectual content: M. Dillon, E. Duke.
Declaration of conflicting interests
The authors declare no conflict of interest regarding this manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.