
Abstract
Study design:
Systematic review.
Background:
Common beliefs about quality of life in people with partial foot and transtibial amputation are often described as passing comments in the literature with seeming little research evidence. A clear understanding of the research evidence is important to inform decisions about amputation level from a quality of life perspective.
Objective:
To systematically gather and appraise research evidence comparing quality of life between persons with partial foot and transtibial amputation.
Methods:
A comprehensive suite of databases (e.g. Cochrane Library, MEDLINE and Web of Science) were searched using terms relating to amputation level and quality of life. Reference lists of articles that met the inclusion criteria were hand searched. Included studies reported quantitative data for persons with partial foot and transtibial amputation secondary to peripheral vascular disease and diabetes. Studies were appraised using the McMaster University Critical Review form.
Results:
There is insufficient evidence comparing quality of life in people with partial foot and transtibial amputation. The available evidence suggests that quality of life may be very similar in people with partial foot and transtibial amputation and the small differences are not likely to be clinically meaningful.
Conclusion:
Without adequate evidence comparing quality of life in people with partial foot and transtibial amputation, it is difficult to inform decisions about amputation level from a quality of life perspective.
Clinical relevance
There is insufficient evidence about differences in QoL between persons with PFA or TTA. Contrary to common belief, the available evidence suggests that QoL may be similar in persons with PFA and TTA. Further research is needed to inform decisions about amputation level from a QoL perspective.
Background
The increasing incidence of diabetes mellitus (DM) has been recognised by leading health authorities as one of the major health challenges of modern times.1–3 Unfortunately, the consequences of diabetes are often unknown to patients until serious complications such as neuropathy, retinopathy, ulceration and amputation significantly impact their quality of life (QoL).4–7
Given that about 85% of lower limb amputations occur secondary to ulceration in people with diabetes who also have neuropathy and peripheral vascular disease (PVD),8–12 it is surprising that the increased incidence of diabetes has not been associated with an increased incidence of lower limb amputation.13–20 Unfortunately many epidemiological studies report only on the incidence of amputation above-the-ankle (i.e. transtibial amputation (TTA) or transfemoral amputation (TFA)) and thereby fail to include persons with partial foot amputation (PFA). Studies with more inclusive criteria highlight that the incidence of PFA has increased exponentially over the last decade and may triple by 2050 if current trends continue.21–24
The increasing incidence of PFA is thought to reflect improvements in revascularisation surgery, earlier assessment at specialist high-risk foot clinics and better management of the early stages of diabetes at a community level.7,25–29
While such improvements in care have made PFA more common, it is unfortunate that at least 25% of people with diabetes will require one further revision surgery on the same limb and 12% will require two or more revision surgeries. 30 This is double the rate observed in people with an initial TTA.30,31
In spite of the low rates of wound healing and frequent re-amputation to a more proximal level, PFA is often preferred to TTA given the purported functional benefits.32–39 For example, it is commonly reported that preserving the ankle joint and residual foot length will contribute to a more normal and less-energy-expensive gait,32,34,37,39–41 despite good evidence that amputation proximal to the metatarsal heads results in a gait pattern almost indistinguishable from that of persons with TTA.38,39,42–56 As the emerging evidence suggests that differences in gait and energy expenditure between PFA and TTA are unlikely, more holistic measures of health such as QoL have become of increasing interest.
QoL measures seek to describe the interaction between the physical, psychological, societal and economic factors relevant to an individual and their health condition.57–63
Given this understanding of QoL, it is important to note that much of the literature about people with PFA and TTA has focused on physical functioning, with little research focused on the many other facets of QoL. This has allowed common beliefs about QoL in people with PFA and TTA to perpetuate through the literature and influence decisions about amputation without adequate research evidence. For example, it is commonly described that being able to walk to the toilet at night without a prosthesis is a significant advantage for people with PFA.32–34 It is disingenuous to suggest that people living with limb loss might place greater value on walking to the toilet at night without a prosthesis, compared to living without pain or recurrent complications and the ability to participate in meaningful social, recreational and vocational pursuit.57,64,65
While there has recently been some commentary suggesting that QoL in persons with PFA and TTA is likely to be very similar,43,66 such editorials provide low-level evidence and carry an inherent potential for bias; particularly without systematic collection and appraisal of the literature.67–69 A systematic search and appraisal of the literature would provide better quality evidence about differences in QoL between persons with PFA and TTA to help inform decisions about amputation level from a QoL perspective.
The purpose of this systematic review was to synthesise literature comparing QoL in people with PFA and TTA secondary to PVD and DM.
Methods
Search strategy
A systematic search of the literature was conducted between 10 and 15 August 2013 by the primary author (M.Q.). The following databases were searched simultaneously as part of the OVID platform: MEDLINE (1946–August 2013), EMBASE (1974–August 2013), PsycINFO (1806–August 2013) and AMED (1985–August 2013). A stand-alone search was also conducted in CINAHL (EBSCO, 1981–August 2013), Cochrane Library (1993–August 2013), Web of Science (ISI, 1955–August 2013), ProQuest Nursing and Allied Health Source (1969–August 2013) and Scopus (Elsevier, 1823–August 2013). Reference lists of articles that met the inclusion criteria were also hand searched.
Search terms related to amputation level included transtibial, partial foot, amputation, Chopart, Lisfranc, tarsometatarsal, midtarsal, below-knee and lower limb amputation, as illustrative examples. Search terms related to QoL included Quality of Life, psychosocial, Health Related Quality of Life as well as common instruments that assess QoL such as Short Form 36 (SF-36), Sickness Impact Profile (SIP), Trinity Amputation and Prosthesis Experience Scales (TAPES), Prosthesis Evaluation Questionnaire (PEQ) and World Health Organization Quality of Life BREF (WHOQOL-BREF). These search terms, as well as their synonyms and acronyms, were used in combination with wildcards and Boolean operators. While there were no constraints on publication date, searches were constrained to the English language. In keeping with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 69 a full description of the search strategy, including a complete list of search terms used, has been included for one database (Figure 1).
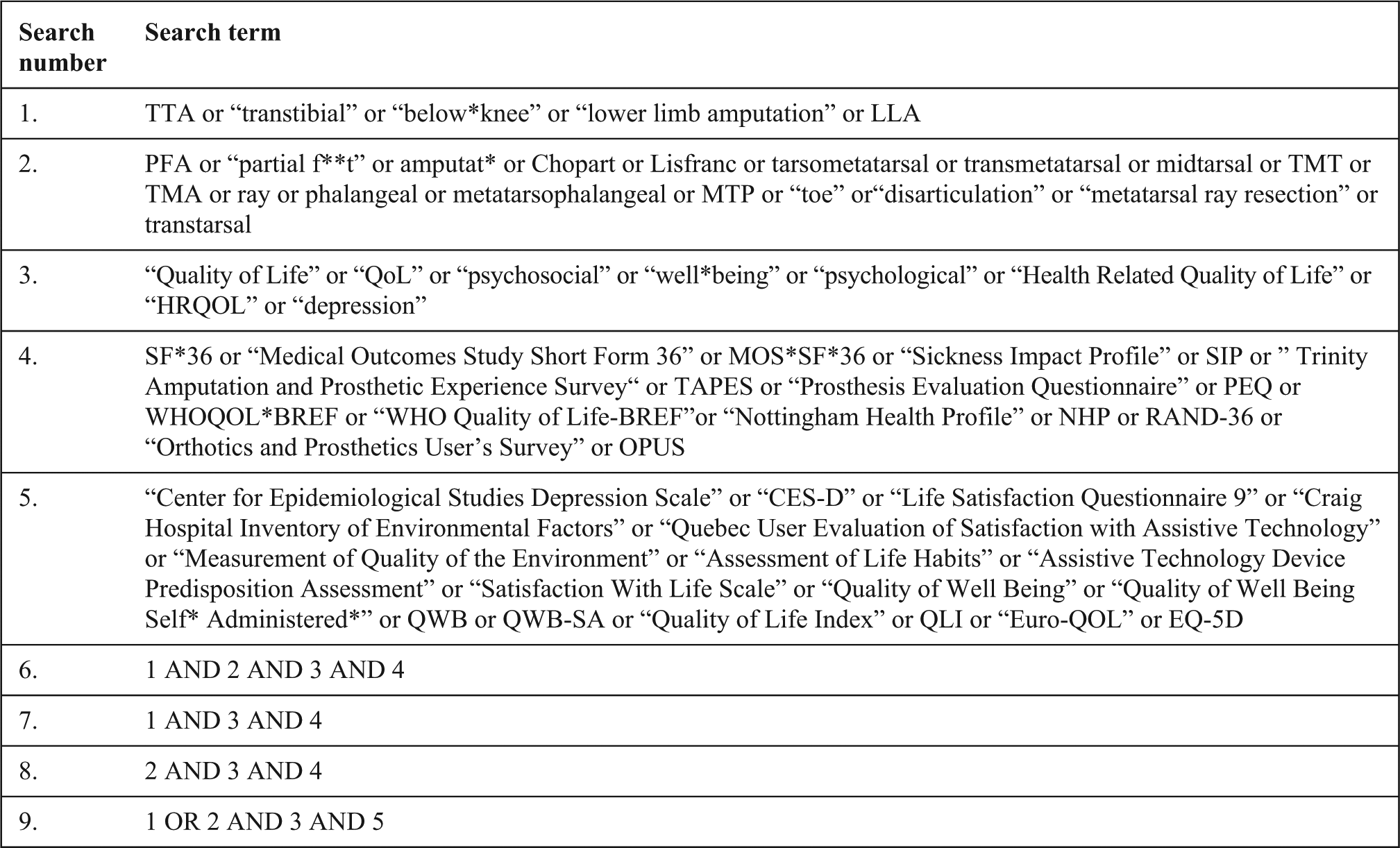
Database search strategy example for CINAHL.
Study selection
Studies were included in this systematic review if QoL data were reported for people with any level of PFA and TTA secondary to diabetes and/or PVD, data could be attributable to a distinct level of amputation and QoL was measured using a quantitative instrument where the psychometric properties had been validated by research. Consistent with the International Standards Organization (ISO) definition of PFA, we did not consider ankle disarticulation as a level of PFA. 70 We did not require that the QoL instrument be validated in an amputee population given that most have been tested in populations with chronic health conditions that similarly impact QoL, such as stroke and diabetes. Opinion pieces were excluded. By virtue of the search strategy, only investigations in English were included.
Eligibility for inclusion was assessed by the primary author (M.Q.), and where necessary, a second opinion was garnered from the second author (M.P.D.). Any disagreement was resolved by discussion until a consensus was reached. As the criteria for inclusion did not require complex judgement, it was deemed unnecessary to routinely involve two authors. 71
Data extraction
A data extraction spreadsheet was developed based on the Cochrane Consumers and Communication Review Group’s data extraction template 72 which allowed demographic (e.g. sex, age, amputation level, cause of amputation), methodological (e.g. study design, outcome measures) and quality appraisal details (e.g. check list items) to be systematically recorded.
The methodological quality was assessed using the McMaster University Critical Review form for quantitative studies. 73 As noted in systematic reviews of critical assessment tools, there are numerous tools to help identify the risk of bias in studies and there is no gold standard.74,75 While we acknowledge that any number of appraisal tools could have been used to help identify the risk of bias in studies, we chose the McMaster Critical Appraisal tool in preference to others given its suitability for the wide variety of study designs common to prosthetics and orthotics literature including experiments and observational studies. 73 It is one of the few schemas with accompanying guidelines that help minimise the likelihood of errors with its use 76 and has been used in systematic reviews in similarly emerging bodies of evidence.77–81 The McMaster schema uses a series of questions to prompt consideration about the internal or external validity of the study (e.g. Question H: were the outcomes measures valid?). This schema does not numerically grade responses, and as such, there was no summary score to characterise the overall methodological quality of the articles.
Similar to the study selection, the quality assessment and data extraction was undertaken by the primary author. When uncertainty arose, the opinion of the second author was sought and consensus was reached through discussion. We did not contact authors to acquire additional information about studies.
Search results
An overview of the selection process has been provided in Figure 2. The search of the databases returned 641 articles. Following the removal of duplicate articles, 334 records were vetted against the inclusion criteria based on title and abstract. A total of 21 articles were considered eligible and the reference lists of articles that met the inclusion criteria were hand searched, yielding an additional 6 articles. Based on full-text review of these 27 articles, 25 articles did not meet with inclusion criteria and were excluded. As such, two articles were included in the systematic review.
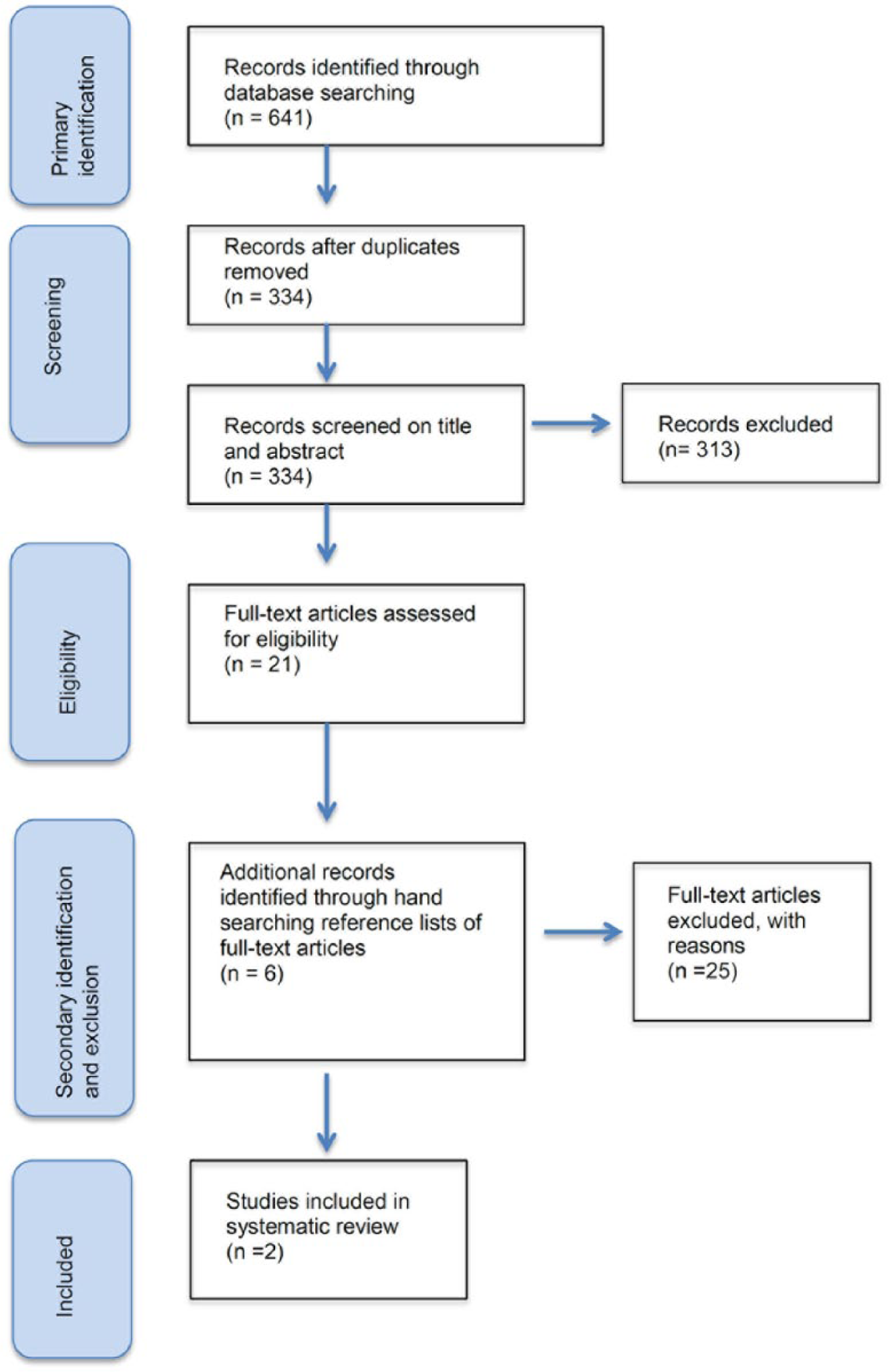
Overview of the selection process.
Study characteristics
Two case-control studies met the inclusion criteria.82,83 Each investigation described a unique population. Data on people with PFA were heterogeneous in terms of amputation level.82,83 For example, persons with toe or transmetatarsal amputation were included in one investigation, 82 while the other included a more representative sample with toe, transmetatarsal, Lisfranc and Chopart levels. 83
Participants were typically representative in terms of age (i.e. mainly older adults aged 40–70 years) and cause of amputation (i.e. amputation due to PVD secondary to diabetes).82,83 One study did not report the sex of participants. 82 The other study had different sex distribution for the case and control groups (i.e. case group was predominantly male and the control group had a fairly even sex distribution). 83
Two different QoL instruments were used in these investigations: the Medical Outcome Study Short Form 36 (MOS SF-36) 82 and the SIP. 83
Neither of the included studies was designed to compare QoL in persons with TTA and PFA (Table 1). By way of example, Boutoille et al. 82 compared QoL in people with foot ulceration (and no amputation) to cohorts with either PFA or TTA. Unfortunately, no comparison of QoL was drawn between the PFA and TTA groups.
Characteristics of included studies.
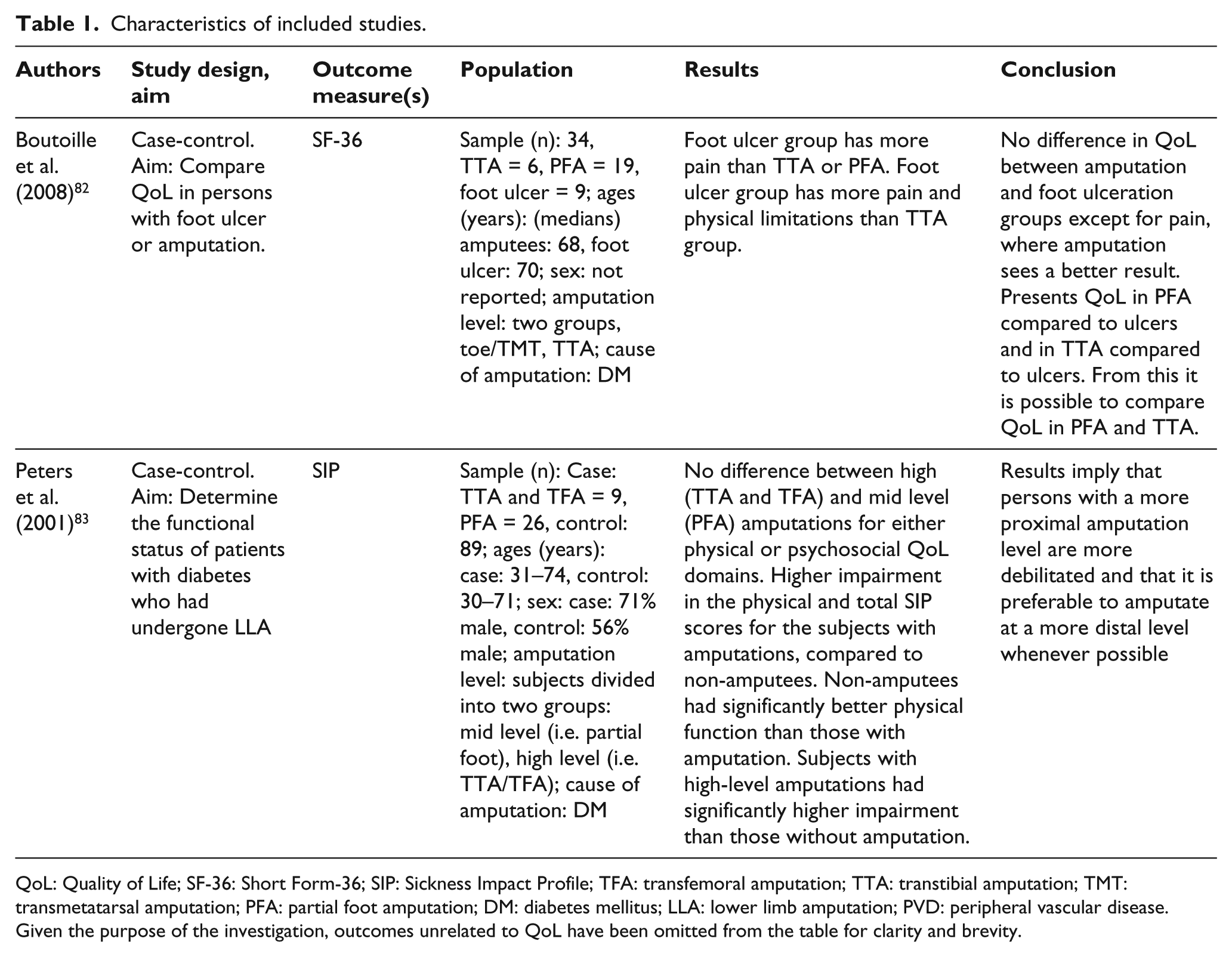
QoL: Quality of Life; SF-36: Short Form-36; SIP: Sickness Impact Profile; TFA: transfemoral amputation; TTA: transtibial amputation; TMT: transmetatarsal amputation; PFA: partial foot amputation; DM: diabetes mellitus; LLA: lower limb amputation; PVD: peripheral vascular disease.
Given the purpose of the investigation, outcomes unrelated to QoL have been omitted from the table for clarity and brevity.
Results
Quality appraisal
Based on the McMaster quality assessment, articles included in this review were generally of poor quality as evidenced by a number of recurrent issues affecting both the external and internal validity. Details of the quality assessment have been presented in Table 2. The most substantive of these issues are discussed in the following sections to illustrate the potential bias.
Results of quality assessment of included articles using McMaster University Critical Review Form – Quantitative Studies.
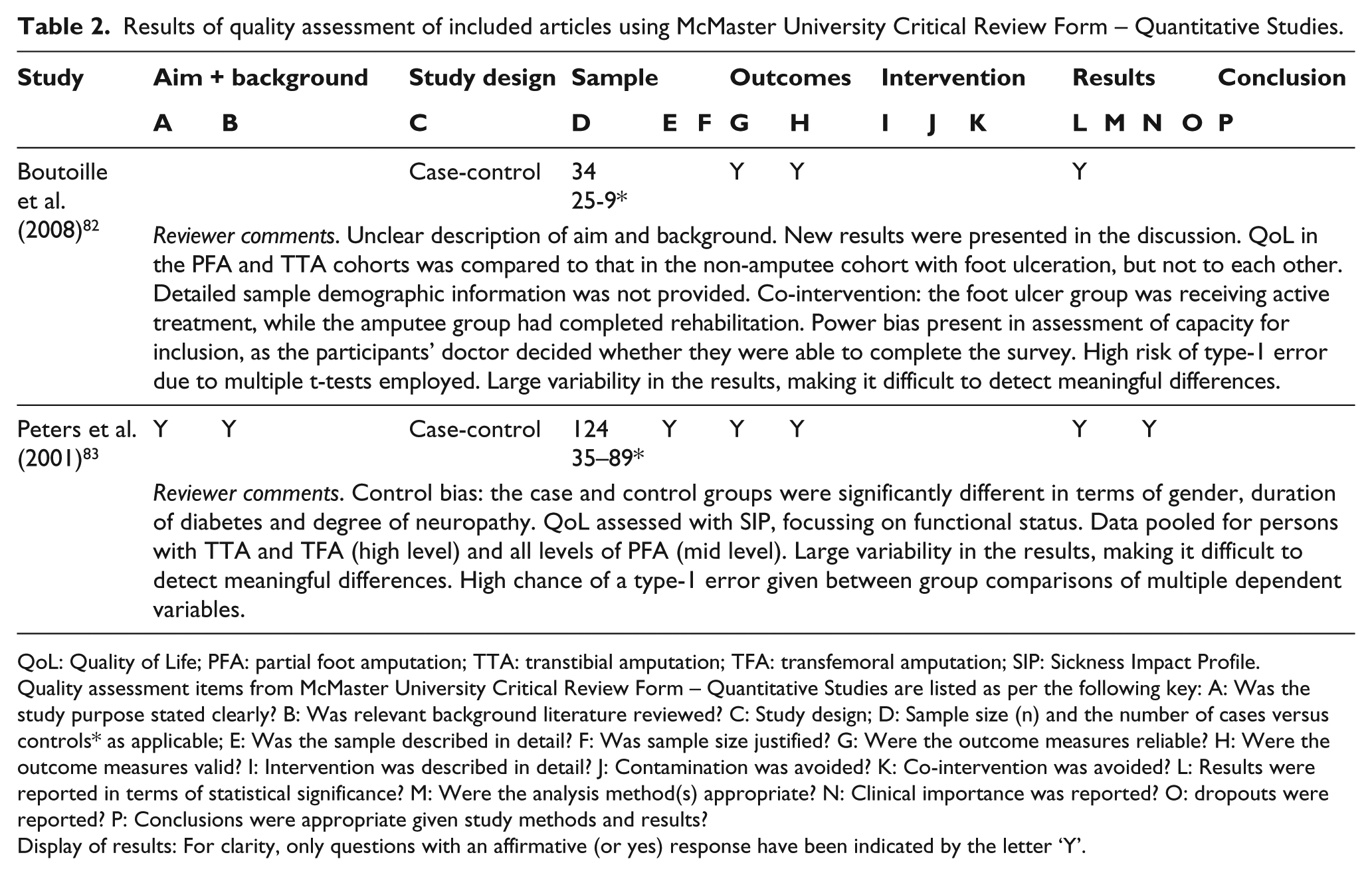
QoL: Quality of Life; PFA: partial foot amputation; TTA: transtibial amputation; TFA: transfemoral amputation; SIP: Sickness Impact Profile.
Quality assessment items from McMaster University Critical Review Form – Quantitative Studies are listed as per the following key: A: Was the study purpose stated clearly? B: Was relevant background literature reviewed? C: Study design; D: Sample size (n) and the number of cases versus controls* as applicable; E: Was the sample described in detail? F: Was sample size justified? G: Were the outcome measures reliable? H: Were the outcome measures valid? I: Intervention was described in detail? J: Contamination was avoided? K: Co-intervention was avoided? L: Results were reported in terms of statistical significance? M: Were the analysis method(s) appropriate? N: Clinical importance was reported? O: dropouts were reported? P: Conclusions were appropriate given study methods and results?
Display of results: For clarity, only questions with an affirmative (or yes) response have been indicated by the letter ‘Y’.
External validity
It was difficult to make an accurate assessment of whether participants in research were characteristic of the broader population of people with PFA or TTA because of insufficient descriptive detail. While both investigations included populations with diabetes and PVD and reported basic information about participants including age and cause of amputation,82,83 one did not report the sex of participants. 82 Both investigations reported the duration of diabetes for participants, but there was little information related to the presence of comorbidities.82,83 The latter is particularly important given that common diabetes comorbidities such as retinopathy, nephropathy and neuropathy have been shown to influence QoL.84–91
Internal validity
Issues affecting the internal validity included inadequate control for co-intervention and likelihood of type-1 error due to multiple pair-wise comparisons.
One of the studies showed issues related to co-intervention, that is, where QoL measures were taken in parallel with active treatment. In this case, QoL measurements were taken while participants were visiting an amputee clinic for wound management. 82
Both studies were at increased risk of finding a false positive (type-1 error), due to the large number of comparisons without adequate controls.82,83 For example, there were a number of multiple comparisons associated with testing each of the eight subscales of the SF-36. 82 Comparison of only the SF-36 summary scores (e.g. the eight subscales of the SF-36 can be summed into a mental health component summary (MCS) or a physical component summary (PSC) score) would help mitigate the risk of reporting significant differences by chance as would the use of more sophisticated statistical techniques such as a multivariate analysis of variance (MANOVA).
Results narrative
In answer to our original research question, there is insufficient evidence to determine whether QoL is different in persons with PFA and TTA because there are just two investigations and these report conflicting results.82,83
The investigation by Peters et al. 83 found no statistically significant difference in SIP scores between people with low-level (PFA) or high-level (TTA/TFA) amputation (Figure 3). By comparison, Boutoille et al. 82 concluded that QoL was better in people with PFA because scores in three subscales of the SF-36 (Physical Functioning, Role Physical and Role Emotional) were higher than in the transtibial group (Figure 4). Only one subscale score (Bodily Pain) was worse in the PFA group compared to the TTA group.
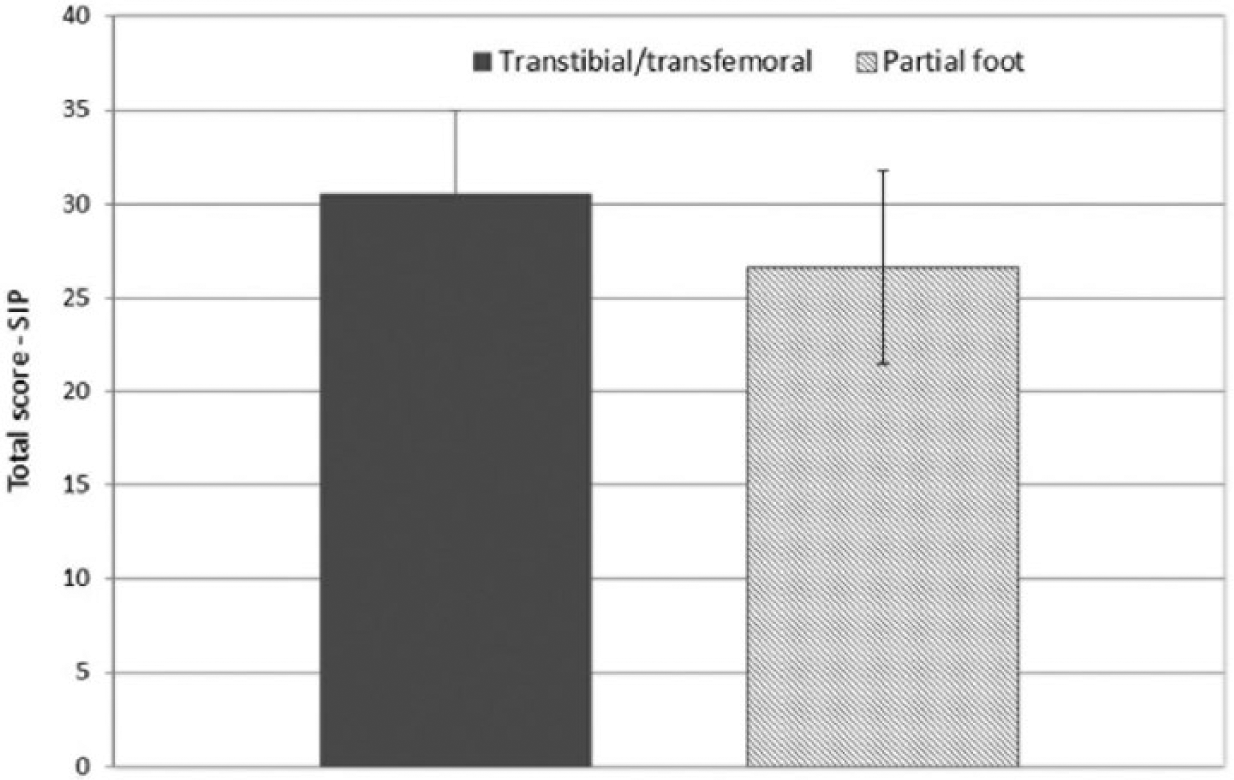
Total SIP scores. Figure created using data from Peters et al. 83 Figure reprinted with permission.
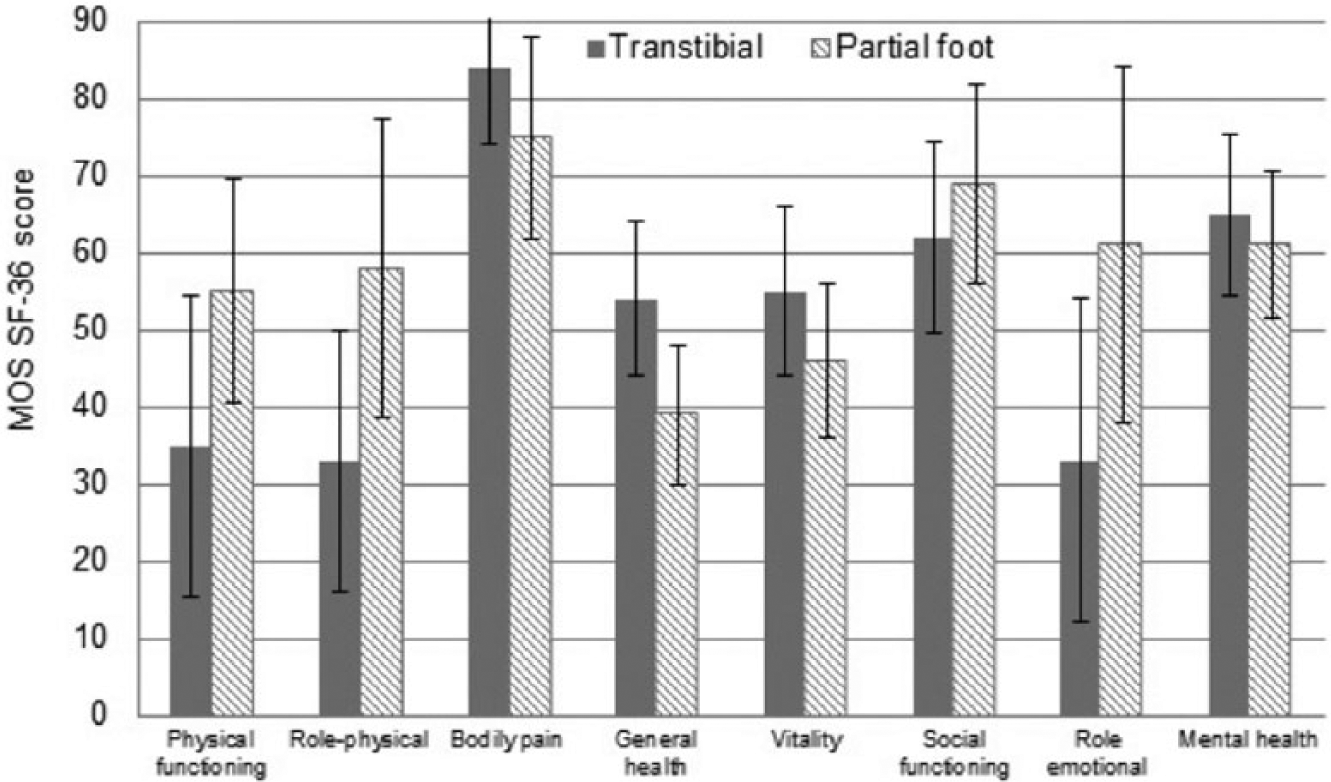
SF-36 subscale scores from Boutoille et al. 82 Figure reprinted with permission.
Unfortunately, the presentation of individual subscale scores 82 makes it difficult to compare overall QoL between people with PFA and TTA. More typically, the individual SF-36 subscales are summarised into two scores: the Physical Component Summary (PCS) and the Mental Component Summary (MCS). Based on data by Barnett et al., 92 we are confident that a reasonable approximation of the SF-36 MCS can be achieved by computing the arithmetic mean of the subscales: Vitality, Social Functioning, Role Emotional and Mental Health. Similarly, the SF-36 PCS can be approximated from the subscale scores of Physical Functioning, Role Physical, Bodily Pain and General Health domains. Presentation of the SF-36 MCS and PCS overcomes the issue of presenting individual subscale data and provides a clearer indication that QoL is very similar in persons with PFA and TTA (Figure 5).
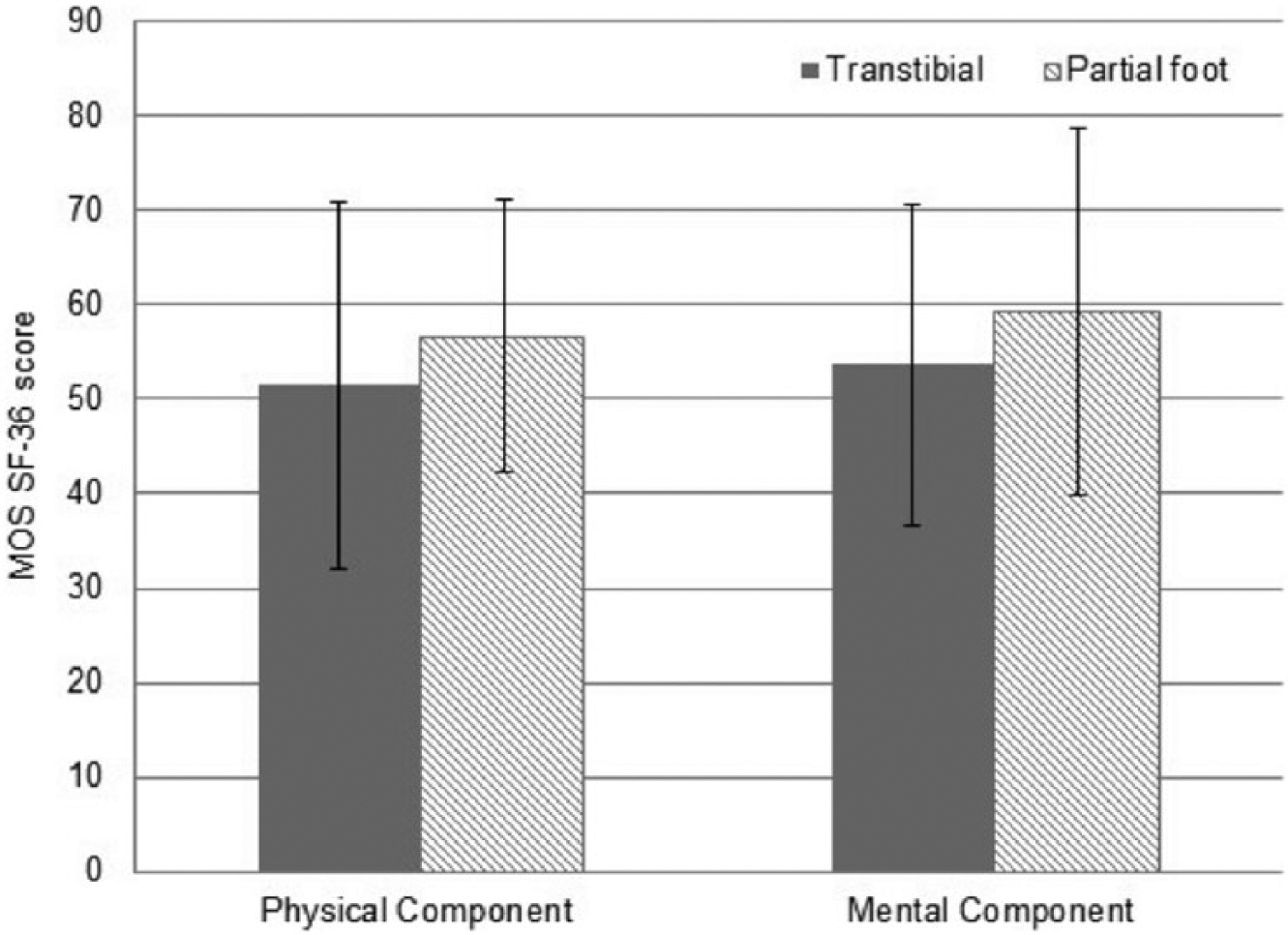
Approximation of SF-36 PCS and MCS from data in Boutoille et al. 82
While at first glance it may appear that QoL is better in persons with PFA (Figure 5), it is important that this interpretation is informed by an understanding of the minimum clinically important difference (MCID). While the MCID has not been specifically established for the SIP or SF-36 in this population, it is commonly reported that a half standard deviation (SD) change in QoL is clinically meaningful in a variety of populations with similar chronic health conditions, such as diabetic retinopathy, rheumatoid arthritis and pulmonary disease.93–98
Given this understanding of the descriptive data, there does not appear to be substantive differences in QoL between persons with PFA and TTA. Unfortunately, neither of these investigations82,83 was designed to compare QoL in groups with PFA or TTA, and the lack of inferential analysis limits the confidence with which we can make this determination.
Methodological considerations
There are a number of method design considerations that help explain the apparent conflict between investigations82,83 and lead to the impression that QoL may be similar in people with PFA and TTA.
Outcome measures describe different aspects of QoL
While the two outcome measures used (i.e. SIP and SF-36) are both recognised tools for measuring QoL, they describe very different aspects of QoL, and this may explain the different results observed.82,83 The SIP is designed to measure changes in behaviour due to illness and the impact on a person’s ability to fulfil activities of daily living.99,100 As such, the SIP could be considered to emphasise functional ability and behaviour limits, rather than reflect more holistic facets of QoL. 101 By contrast, the SF-36 is a more holistic tool that measures a variety of mental and physical components (e.g. behavioural functioning, physical and social functioning, wellbeing and general health) that better reflect the impact of mental health on a person’s QoL, including changes in mood and feelings. 101
Pooling data for different levels of amputation
The pooling of data for different levels of amputation is likely to have impacted the results. Peters et al. 83 pooled data for persons with TFA and TTA which is problematic because the higher mobility afforded by TTA is believed to be reflected in higher QoL.102–104 Similarly, data have been pooled for different levels of PFA,82,83 without first establishing the reasonableness of this approach.
Variability in QoL measures
QoL measures are inherently variable, with SDs equivalent to half 83 or the total mean scores observed. 82 Such large variability makes it difficult to observe relatively small differences in QoL; particularly when common co-variants that impact QoL (e.g. nephropathy and retinopathy) are not controlled for.85–91
Power and MCID
Given the small differences in QoL observed between groups, and the large variability in the data, it is unlikely that investigations reporting data in PFA and TTA cohorts were adequately powered.82,83 Neither of the investigations reported undertaking a power analysis to estimate the required sample size. To better understand the required sample size for this type of study, we undertook a sample size calculation based on the following assumptions: an independent t-test, assuming the MCID was a half SD 96 (5 t-score change in the SF-36), SD in each group was 10 t-score points, alpha = 0.05, beta = 0.8. Based on these assumptions, we determined that the required sample size would be 50 people per group; more than double the number of participants in the PFA cohorts of papers included in this review.82,83
Discussion
We were surprised to find just two papers that report QoL data for people with PFA and TTA, particularly given how commonly beliefs about QoL are described.32–34
There is insufficient evidence to draw conclusions about differences in QoL between persons with a PFA and TTA or to inform difficult decisions about amputation surgery from a QoL perspective.
Although limited, the available evidence suggests that QoL may be very similar in people with PFA and TTA, and the small differences observed would not be considered clinically meaningful. 96
While it is routinely presumed that more distal amputation will improve physical functioning and QoL,102,105,106 it is challenging to recognise that physical incapacity does not necessarily negatively impact QoL.107–110 It may be that QoL is fluid and evolves as a person adjusts to live with his or her health condition.107–110 Health-care providers routinely underestimate the QoL of patients with chronic health conditions compared to the patient’s own, self-evaluated, QoL,111,112 which exemplifies the need for routine measurement of QoL, with a recognised instrument, to gauge the effectiveness of practice. 57
Recommendations for future research
While a number of different QoL measures have been reported in the amputee literature, there is little consensus about which may be the most suitable. Generic QoL measures (e.g. SF-36) have been criticised for not being sensitive to the needs of specific populations.57,113–117 By contrast, prosthesis-related measures (e.g. PEQ) may be able to provide valuable information pertaining to the experience of using a prosthesis, yet are unable to provide information regarding the more holistic measure of living with limb loss beyond the impact of the prosthesis.
Future investigations could add to the body of work by choosing a QoL measure that has been used previously in the population of interest (e.g. SF-36). As the evidence grows with a particular QoL outcome measure, it will become easier to synthesise results across studies and generate recommendations for clinical practice.
The frequent non-reporting of demographic information makes it difficult to assess whether differences in QoL between cohorts are as a result of the amputation level itself or the confounding variables not reported by investigators. 106 Given the number of comorbidities that influence QoL (e.g. presence and duration of diabetes, retinopathy, nephropathy and neuropathy), it is important that researchers control for these. More sophisticated analytical approaches such as multivariate regression techniques could be used to good effect.
Investigators should give careful thought to controlling for the likelihood of type-1 error associated with multiple tests. This may involve using QoL summary scores as the primary outcome (e.g. SF-36 MCS or PCS) and reporting the subscale scores as a secondary outcome. In this way, the number of comparisons is dramatically reduced. Similarly, investigators may adopt more sophisticated analytical approaches, such as multivariate linear regression techniques. With these statistical methods, investigators should be mindful of the need for larger samples depending on the number of independent variables used.118,119
Limitations
There are a number of limitations to this systematic review and the findings should be interpreted in light of these.
We focused on comparing QoL in people with PFA and TTA secondary to PVD and diabetes, and as such, studies involving persons with non-diabetic-related amputation would have been excluded. We deliberately focused on this population given that the overwhelming majority of persons living with PFA and TTA have PVD and diabetes and that disease-specific comorbidities (e.g. retinopathy, neuropathy, depression) are known co-variants influencing QoL, thus making synthesis of data from people without these comorbidities inappropriate.
While we felt it was unnecessary for two investigators to assess eligibility given that the inclusion criteria did not require complex judgement, 71 we recognise and acknowledge the potential shortcoming of this approach.
The body of literature on the topic was limited in terms of the number of investigations and our ability to identify discrete cohorts with PFA and/or TTA. As such, a narrative review seemed the most appropriate means to synthesise literature on the topic. While there is a much larger body of work describing QoL in persons with lower limb amputation, we excluded a large number of studies because we were unable to identify discrete cohorts with either PFA or TTA in keeping with the purpose of the review and our inclusion criteria.
Conclusion
There is insufficient evidence to draw conclusions about differences in QoL between persons with a PFA and TTA or inform difficult decisions about amputation level from a QoL perspective. The limited evidence suggests that QoL may be very similar in persons with PFA and TTA and the small differences between cohorts may not be clinically meaningful.
This has important implications for surgeons and patients facing difficult decisions about amputation surgery. Given that the available evidence is so limited, decisions about amputation level will continue to be informed by experiential and anecdotal evidence until such time as more robust evidence is available. Unfortunately, due to the lack of routine measurement or analysis of QoL in these populations, poorly substantiated views about the correlation between amputation level and QoL have become well accepted. Such views do not take into account the various factors that contribute to the QoL of individuals and leave many unanswered questions regarding the effect of amputation level in the daily lives of those living with limb loss.
Further research should explicitly compare cohorts with PFA and TTA and control for common co-variants known to affect QoL using appropriate analytical approaches. More rigorous research is needed to support observations gleaned from this review; that is, QoL may be very similar in people with PFA and TTA, and that any differences are likely to be small and not clinically meaningful.
Footnotes
Acknowledgements
We thank Fiona Barnett, Dip App Sci (P&O), BP&O, Matthew Major, BSc (Mech Eng), MSc (Mech Eng), PhD, and Phil Stevens, Med, CPO, FAAOP, for their contributions and thoughtful feedback on the draft manuscript.
Author contribution
All authors contributed equally to the preparation of this manuscript.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.