
Abstract
Background:
For people with lower extremity amputations, the decreased confidence and suboptimal gait associated with dynamic instability can negatively affect mobility and quality of life. Quantifying dynamic instability could enhance clinical decision making related to lower extremity prosthetics and inform future prosthetic research.
Objective:
To quantitatively examine gait adaptations in transfemoral amputees across various walking conditions.
Study design:
Cross-sectional study.
Methods:
Plantar-pressure data were collected from 11 individuals with unilateral transfemoral amputations using an in-shoe plantar-pressure measurement system while navigating rigid and soft ground, ramp, and stair conditions. Six parameters were examined: anterior–posterior and medial–lateral center-of-pressure direction changes, sensor cell loading frequency (cell triggering), maximum lateral force position, double support time, and stride time. Paired t-tests and analyses of variance were used to examine differences between limbs and walking conditions, respectively.
Results:
Values for medial–lateral center-of-pressure direction change, sensor cell loading frequency, and double support time were significantly greater on the intact limb than the prosthetic limb. Significant differences between conditions occurred only for anterior–posterior center-of-pressure direction change and double support time on the prosthetic limb.
Conclusion:
Higher values on the intact limb suggest that it plays a key role in maintaining stability and optimizing body progression during different tasks. Differences between participants, limbs, and walking condition indicate parameter sensitivity to adaptive gait strategies.
Clinical relevance
This plantar-pressure-based approach is a viable option for point-of-care evaluation of locomotor performance, across common various mobility tasks and activities of daily living. The information obtained could be valuable for prosthetic prescription and optimization of prosthetic fit and alignment, potentially improving mobility for prosthetic users with dynamic stability deficits.
Keywords
Background
Safe and confident gait is important for mobility, especially for people with lower extremity amputations. Both safety and confidence are related to dynamic stability. As gait becomes more unstable, confidence may decrease and people with amputations may employ a protective gait pattern, 1 such as slowing down, increasing double support time (DST), widening step width, and activity avoidance. Together, decreased confidence and suboptimal gait can have an adverse effect on mobility and quality of life. Stability is “the property of a body that causes it when disturbed from a condition of equilibrium or steady motion to develop forces or moments that restore the original condition.” 2 Thus, unstable gait is typically characterized by increased variability or fluctuations in gait-related parameters.
During walking, kinematic and kinetic fluctuations can be measured with motion capture systems, inertial sensors, force plates, or plantar-pressure measurement systems. Thus, stability assessment measures can be acquired, such as body center-of-mass (COM) position relative to the center-of-pressure (COP) under the foot,3–7 COM sway angle, medial–lateral and anterior–posterior velocities and accelerations of the COM, 5 and combinations of COM position and velocity.8,9 Unfortunately, these approaches are typically restricted to gait laboratories and do not permit patient point-of-contact assessment, which is of particular importance in a rehabilitation setting where mobility at home and in the community is a key component of quality of life.
Specific to transfemoral (TF) amputees, gait adaptation studies have largely focused on joint kinematics and kinetics,10–12 joint work and power,13,14 and electromyography,15,16 without attention to stabilizing forces applied through the foot. One study focused on standing balance and postural stability as a measure of TF amputee standing postural stability, 17 using an equilibrium score based on COM sway angle. While useful information was obtained about standing internal knee and hip moment adjustment patterns, measures during walking are needed to understand TF amputee strategies for maintaining stable mobility across a range of walking tasks. Lamoth et al. 18 addressed this need with a trunk-mounted accelerometer. TF amputee walking variability and stability were based on walking speed, stride time (ST), and trunk acceleration. Multiple-step stability measurements assessed the consistency of the walking pattern over many gait cycles, predictability or repeatability of the signal, and ability to resist small externally induced perturbations. The study by Lamoth et al. did not address intact and prosthetic limb adaptations during walking.
Plantar-pressure, force, and COP measures have been used to investigate body adjustments that return the body COM to a more stable position.10–20 More recently, the current authors explored portable in-shoe pressure measurement to extract six measures related to dynamic stability, based on plantar COP motion, cell loading frequency, and gait timing.21–23 These measures were useful for assessing dynamic stability for able-bodied individuals and people with transtibial (TT) amputations, using a wearable system that can be applied in most environments. Importantly, the findings of these studies cannot be generalized to the TF population. Further testing is required to determine whether the selected stability measures are appropriate for assessing dynamic stability in TF amputees.
Quantitative analysis of TF amputee gait adaptations, at the point of patient contact or in the community, could enhance clinical decision making related to device prescription and provide useful measures for future prosthetic research. The objectives of this study were to (1) assess the utility of six previously identified plantar-pressure and temporal measures in measuring dynamic stability of TF amputees and (2) gain an improved understanding of gait adaptations employed by TF amputees over various walking conditions (i.e. rigid ground, soft ground, ramp, and stairs).
Methods
Participants
A convenience sample of 11 community ambulators (9 men; 2 women) with unilateral TF amputations (7 trauma, 3 tumor, 1 frostbite) volunteered to participate in the study. Potential subjects were identified from patient files at The Ottawa Hospital Rehabilitation Centre. The project physiatrist reviewed patient files and selected potential participants on a case-by-case basis who were then contacted via mail and invited to participate. The mean age was 57 ± 13 years, mean mass was 75 ± 10 kg, functional levels were K3–K4, and no participants used walking aids. Seven participants used a microprocessor-controlled knee unit (C-Leg; Otto Bock, Duderstadt, Germany) and four used a hydraulic knee unit. All participants were screened by a physiatrist and prosthetist to ensure safe participation and provided informed written consent. This study was approved by the Ottawa Health Science Network Research Ethics Board.
Data collection
Plantar-pressure data were acquired to derive directional (medial–lateral, anterior–posterior) and temporal measures from COP motion, pressure-sensor cell loading, and gait timing.21–23 The wearable F-Scan Mobile system (Tekscan, Inc., Boston, MA, USA) was used to collect all data. F-Scan plantar-pressure-sensing insoles had 900 sensor cells in 60 rows and 21 columns. Each insole was trimmed and fit into the person’s own shoes, to ensure safe and natural gait. Plantar-pressure data were collected at 120 Hz for each of the following conditions:
Rigid ground. Participants walked along a level hallway (5 trials).
Soft ground. Participants walked over an 8 m × 1 m row of foam mats (5 trials).
Ramp. Participants walked on a ramp with a 7° incline (10 trials: 5 ascending and 5 descending).
Stairs. Participants walked up and down a 12-step stairwell (4 trials: 2 ascending and 2 descending). The stair rise was 19.1 cm and run was 27.3 cm.
The walking condition testing order was randomized for each participant. A project assistant walked beside each person during all trials to ensure safe navigation. Participants walked at their self-selected speed.
Data processing
F-Scan plantar-pressure data were processed using custom software to extract the following six plantar-pressure and temporal measures 22 , for each stride and for each foot:
Anterior–posterior COP direction change (AP). The number of times that the first derivative of the anterior–posterior COP curve crosses a dual threshold of ± 0.5 mm/frame. This measure indicates changes in the anterior–posterior direction of the COP.
Medial–lateral COP direction change (ML). The number of times that the first derivative of medial–lateral COP curve crosses a dual threshold of ± 0.5 mm/frame. This measure indicates changes in the medial–lateral direction of the COP.
Cell triggering (CellTrig). The maximum number of times, across all insole cells, that a sensor cell is turned on (triggered) during stance, divided by the number of frames in the stride. When the foot transitions smoothly during gait, each sensor on the insole should be activated only once.
Maximum lateral force placement (MaxLat). The most lateral F-Scan sensor column activated, expressed as a percentage of the total number of columns. A higher value indicates increased lateral excursion of the COP trajectory. Lateral excursion of the COP trajectory has been associated with greater instability. 24
ST. The time from foot strike to the next foot strike on the same foot.
DST. The time that both feet are in contact with the ground during a single stance phase. Intact limb DST is from foot strike on the prosthetic side to foot off on the intact side. Prosthetic limb DST is from foot strike on the intact side to foot off on the prosthetic side.
For each trial and limb, intact and prosthetic, output for several consecutive middle strides was extracted (three for upramp and downramp; five for all other conditions). For each person, mean and standard deviation values were calculated for each measure, limb, and condition.
Data analysis
SPSS statistical software (version 15.0 for Windows) was used to perform paired t-tests to compare measures between the intact and prosthetic limbs for each condition (p < 0.05). The Benjamini and Hochberg 25 method was used to correct for multiple t-tests. A one-way analysis of variance (ANOVA) with post hoc Bonferroni was used to determine whether measures differed between conditions.
Results
For plantar-pressure analysis, higher AP and ML values indicate irregular COP progression in the anterior–posterior or medial–lateral direction. Higher CellTrig values indicate repeated loading of a local foot region, which would occur with irregular foot loading progression. A higher MaxLat indicates greater COP lateral excursion, previously associated with increased instability. 24 ST and DST are common measures and are related to compensatory mechanisms in prosthetics, with greater ST and DST occurring when compensating for mobility issues. All participants used a “step-by-step with handrails” strategy for stair navigation.
Differences between limbs
Figure 1 and Table 1 present means and standard deviations for plantar-pressure and temporal measures, computed for each limb and condition. For 26 out of 36 cases (6 measures × 6 conditions), intact limb outcomes were greater than the prosthetic limb. Of these 26 cases, 12 were significantly different. Table 2 shows significant differences between limbs for ML, CellTrig, and DST. ML was significantly different between limbs for soft ground, upramp, and downramp. CellTrig was significantly different between limbs for all conditions. DST was significantly different between limbs for downramp, upstairs, and downstairs. There were no significant differences between limbs for AP, MaxLat, and ST. When applying a statistical correction for multiple tests (Benjamini and Hochberg 25 ), the difference between limbs for upstairs DST was no longer significant.
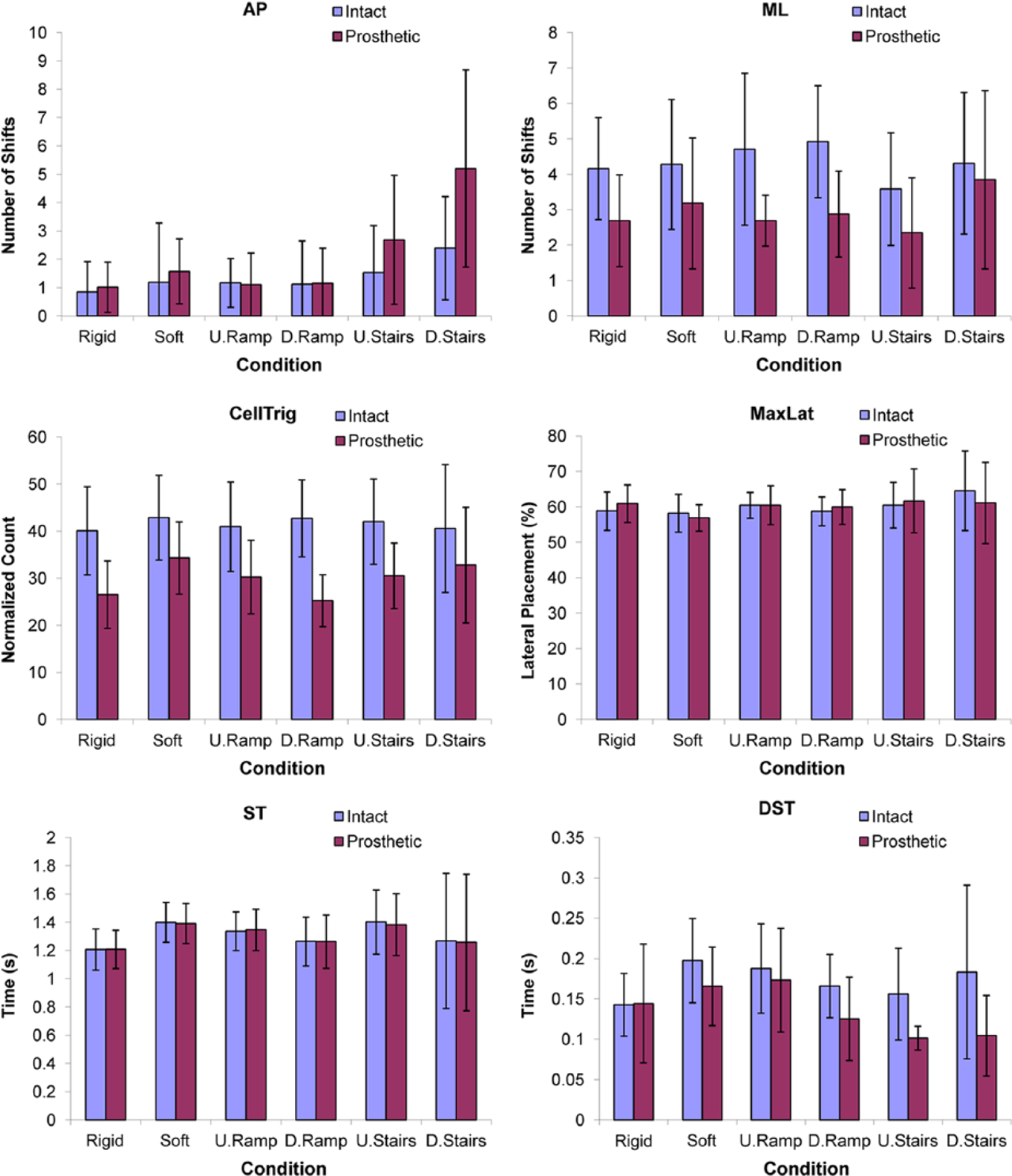
Mean values and standard deviations (error bars) for all plantar-pressure and temporal measures for each foot and each condition.
Mean values and standard deviations (SDs) for all plantar-pressure and temporal measures for each foot and each condition.
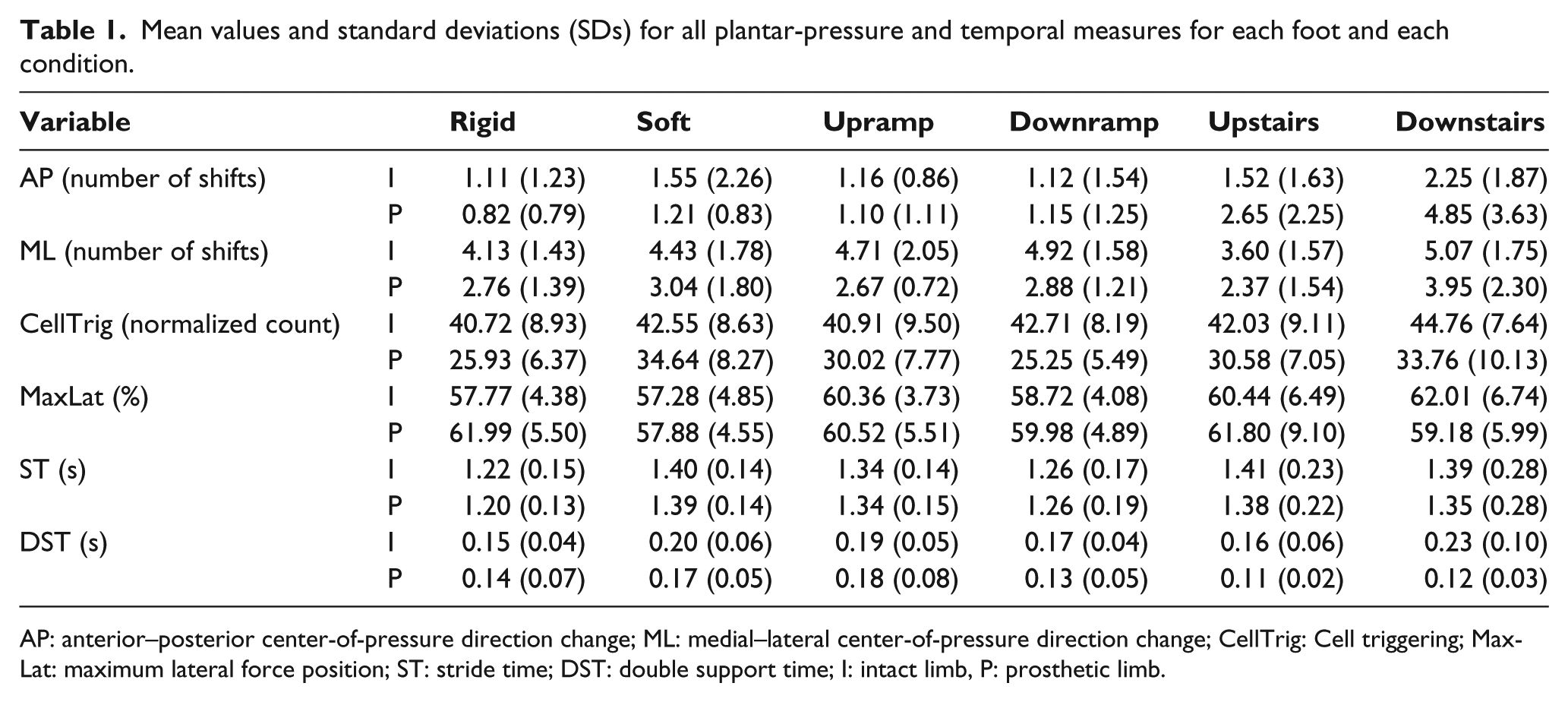
AP: anterior–posterior center-of-pressure direction change; ML: medial–lateral center-of-pressure direction change; CellTrig: Cell triggering; MaxLat: maximum lateral force position; ST: stride time; DST: double support time; I: intact limb, P: prosthetic limb.
Mean value differences and standard deviations (SDs) between intact and prosthetic limbs (intact minus prosthetic) for all plantar-pressure and temporal measures and each condition.
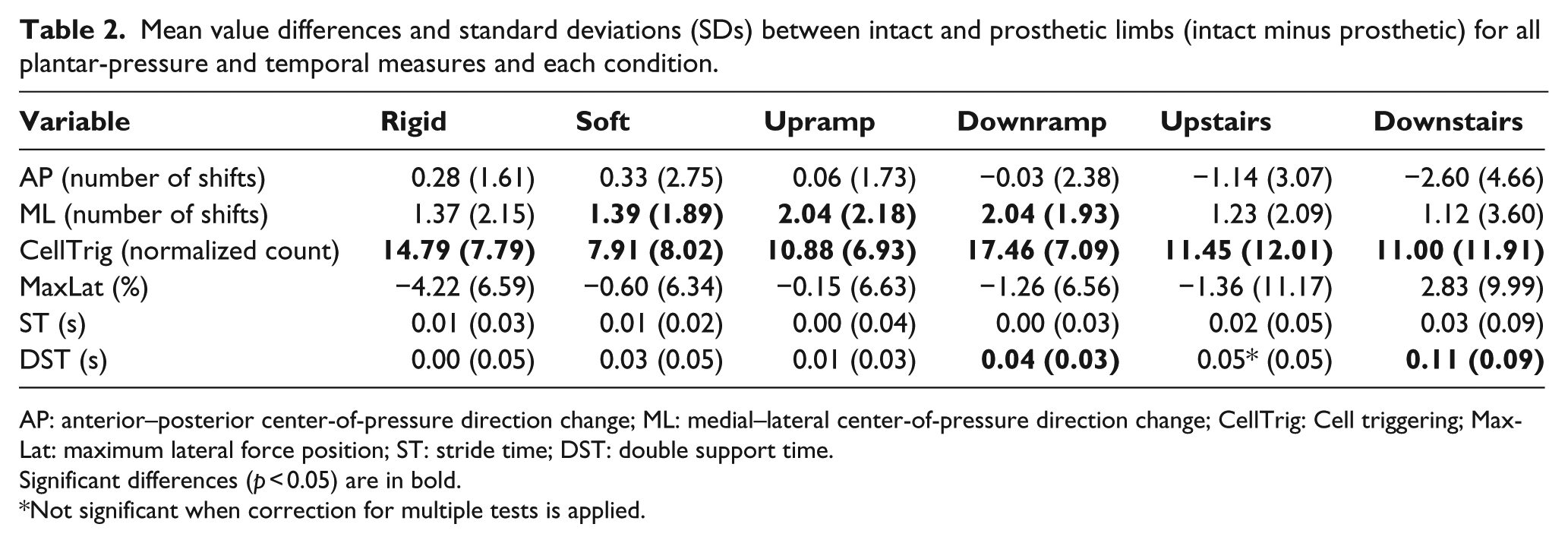
AP: anterior–posterior center-of-pressure direction change; ML: medial–lateral center-of-pressure direction change; CellTrig: Cell triggering; MaxLat: maximum lateral force position; ST: stride time; DST: double support time.
Significant differences (p < 0.05) are in bold.
Not significant when correction for multiple tests is applied.
Differences between walking conditions
Condition had a significant effect on several measures. On the intact limb, ANOVA for condition only showed a significant effect for DST (Table 3). However, post hoc analysis did not find specific significant differences between DST conditions. On the prosthetic limb, condition significantly affected AP, CellTrig, and DST, while significant differences between conditions occurred for AP and DST. AP values were significantly greater for downstairs walking than all conditions except upstairs. Condition had a significant effect on CellTrig; however, there were no significant differences between conditions. DST was significantly greater for upramp than upstairs.
Summary of plantar-pressure and temporal measure ANOVA results and differences between conditions.
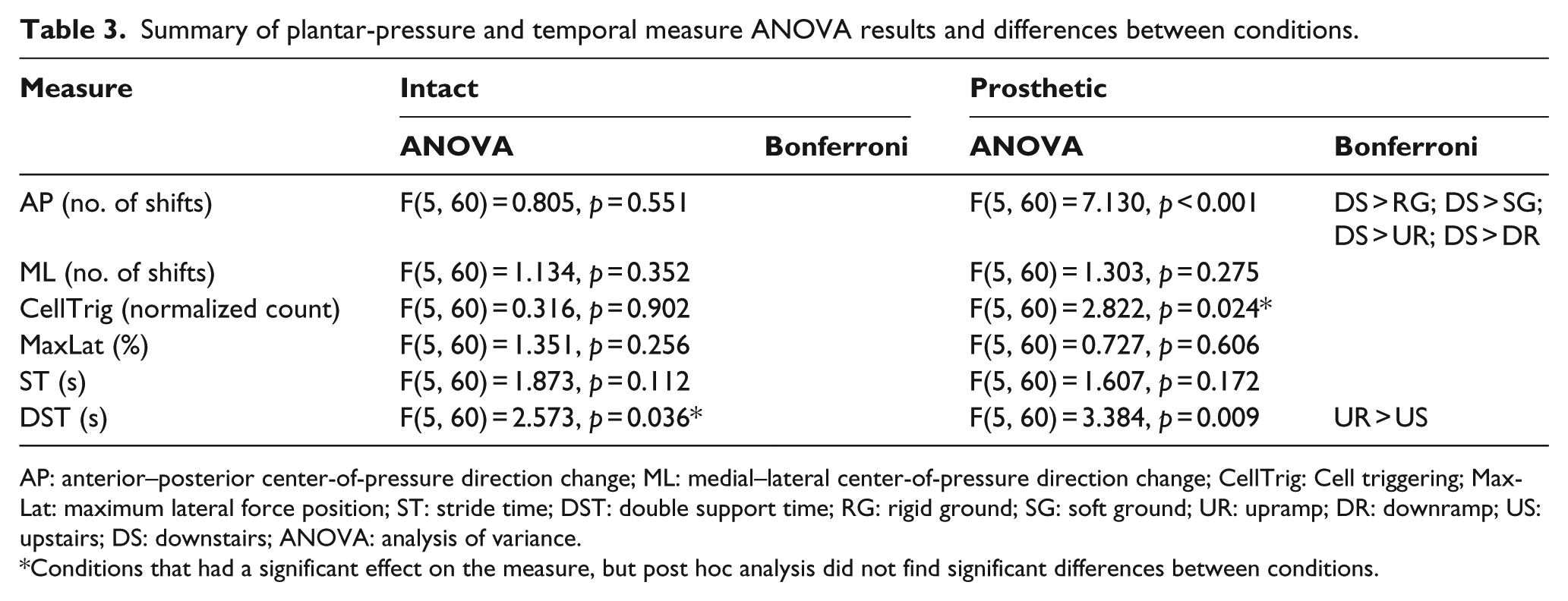
AP: anterior–posterior center-of-pressure direction change; ML: medial–lateral center-of-pressure direction change; CellTrig: Cell triggering; MaxLat: maximum lateral force position; ST: stride time; DST: double support time; RG: rigid ground; SG: soft ground; UR: upramp; DR: downramp; US: upstairs; DS: downstairs; ANOVA: analysis of variance.
Conditions that had a significant effect on the measure, but post hoc analysis did not find significant differences between conditions.
Discussion
Difference between limbs
In most cases, the intact limb had higher values than the prosthetic limb for plantar-pressure and temporal measures; however, significant differences were only found for ML, CellTrig, and DST. Cases without significant differences may be due, in part, to the high standard deviations. Importantly, high standard deviations suggest that the plantar-pressure-based measures were sensitive to differences between participants and were reflective of the walking ability of study participants (i.e. ranged from moderate to excellent) as well as individual’s adaptive gait strategies.
Higher parameter values on the intact side are reasonable, given that the intact limb has the sensorimotor function and musculature to compensate for body instability. The prostheses in this study were passive devices that had a lower capacity for controlling motion at the ankle and knee than an intact leg. For a stable mobility strategy, prosthetic users may optimize for a smooth transition over the prosthetic limb, with little anterior–posterior adjustment, and then compensate during stance on the intact limb, mainly mediolaterally. This smooth AP progression may have enhanced the person’s ability to maintain the prosthetic knee in a safe position during weight-bearing.
The significantly higher CellTrig values on the intact limb compared to the prosthetic limb for all walking conditions demonstrated frequent limb-loading fluctuations in local regions of the intact foot (i.e. pressure-sensor cells being loaded and unloaded more than once). This suggests that frequent adjustments were needed on the intact side to achieve optimal body progression, for all test activities.Significantly higher CellTrig for the intact limb during upstairs and downstairs walking may be associated with the greater hip adduction and abduction and more muscle activity in the person’s sound leg when attempting to correctly position the prosthetic limb. 15
The longer intact limb DST is consistent with clinical knowledge, where the TF amputee spends more time on the limb that generates compensatory and propulsive forces. In contrast, Jaegers et al. 16 reported increased time from “heel strike of the intact foot to toe off of the prosthetic foot” in TF unilateral prosthesis users. Further research is needed to verify between limb DST differences for TF prosthesis users.
Variations in prosthetic technology and device design may have contributed to high inter-subject variability. For example, people with a microprocessor-controlled knee unit can take advantage of automatic adjustments to knee flexion–extension damping during gait, thereby compensating for different tasks and terrain. Hydraulic knee units cannot dynamically adjust and therefore may be less optimal across multiple tasks. A larger sample of micro-processor and regular hydraulic knee users would be required to verify this hypothesis. Other prosthetic factors, such as type of foot and prosthetic fit, can also affect the computed plantar-pressure-based measures. Due to the small sample size, the effects of specific types or combinations of prosthetic components were not analyzed.
In comparison with TT prosthesis users, 22 AP measures for the TF prosthetic limb were generally higher than the TT prosthetic limb for all conditions except upstairs. On the intact limb, TT prosthesis users had greater AP values for all conditions and lower ML values for all conditions except upstairs, compared to TF prosthesis users. Greater AP values on the TF prosthetic limb could be due to the demands of maintaining the prosthetic knee in extension during stance. Lower ML values, on the TT intact limb, may indicate less active compensation than TF amputees. Downstairs walking produced the largest differences between TF and TT groups, with more than triple the AP values and a 50% greater ML value for the TF prosthetic limb. These more frequent changes in TF prosthetic foot loading patterns for the anterior–posterior direction could be related to the lack of a natural knee joint and the loss of proprioception and motor control normally used to maintain dynamic stability. TF prosthetic limb ML values were lower than TT prosthetic limb values for rigid ground, upramp, downramp, and upstairs conditions. The use of a mechanical knee joint instead of an anatomical knee joint may have been a contributing factor, with the TF prosthetic limb less able to make medial–lateral adjustments compared to the TT limb. The lower ML values for TF prosthesis users may reflect that the necessary mediolateral adjustments were instead being made by their intact limb. This is supported by the findings of high hip abduction, hip adduction, and hamstring muscle activity in the sound leg of TF amputees by Bae et al. 15
Difference between activity conditions
During downstairs walking, where AP values were significantly greater than all conditions except upstairs, participants typically placed the middle of their prosthetic foot over the edge of the step to assist in knee flexion and roll-over. Efforts to position the foot over the step edge and safely ride the knee joint until the successive contralateral foot strike may have increased AP values in downstairs walking.
No significant differences were found between conditions for MaxLat. Prosthesis users could have developed a gait pattern in which they avoided extreme lateral deviations to maintain balance. For some participants and activities, longer ST when using their prosthesis may be due to the additional time required to engage and disengage the knee joint.
Intact limb DST was highest for downstairs walking. Longer DST on the intact limb in downstairs walking may be required to help control descent. These results and explanation are partly supported by the longer DST on the intact limb of TF amputees, 10 high hip adduction and abduction, and high muscle activity in the sound leg of TF amputees in attempt to correctly position the prosthetic limb. 15
Quantitative measures of fluctuations in foot load-ing and COP motion, as provided by the four plantar-pressure-based measures together with the two temporal measures, provided insight into the compensation strategies of TF prosthesis users in a variety of mobility tasks. Through further study, this information could be valuable for prosthetic prescription and optimization of prosthetic fit and alignment. These clinical improvements could result in improved mobility confidence, lower activity avoidance, and reduction in the prevalence of falls for prosthetic users with dynamic stability deficits.
Conclusion
Plantar-pressure and temporal measures were appropriate for examining gait accommodations in TF amputees to maintain dynamic stability and provided insight into gait strategies used by TF amputees over different walking conditions. As with TT amputees, 22 the generally higher values for plantar-pressure and temporal measures on the intact limb suggested that TF prosthesis users rely on their intact limb to make adjustments for stability and optimal body progression during different mobility tasks, in addition to relying on the intact limb as a propulsion engine. TF prosthesis user mobility patterns were characterized by frequent limb-loading fluctuations in local regions of the intact foot (i.e. indicated by CellTrig) with predominate medial–lateral adjustments during intact foot loading.
While standard deviation may tend to be larger with smaller sample sizes, the large standard deviations found in this study may also be indicative of measures that are sensitive to inter-subject differences, particularly for AP and ML (COP shifts in direction). For future research, separate analysis of groups with either predominate AP or ML deviations would be advisable.
The use of the plantar-pressure measures together with temporal measures allowed for a multi-factorial analysis of TF amputee gait and furthered understanding of movement adaptations and walking strategies at the foot level across typical mobility tasks. All plantar-pressure and temporal measurements were made using a wearable insole sensor that enables patient assessment at the point of care and in most environments. The separate anterior–posterior and medial–lateral directional information for COP motion and temporal measures permits assessment of gait adaptations based on prosthesis design, fit, alignment, mobility task, and environment.
Since these measurements were performed using portable wearable instrumentation, this plantar-pressure–based approach is a viable option for assessing locomotor performance at the point of care, across common mobility tasks and activities of daily living, and at the most appropriate location, including staircases and outdoors. The analysis method, based on COP signal variations and cell activation, avoided potential errors that could occur from using absolute force measurement from in-shoe pressure-based systems. Future studies while performing activities of daily living would be beneficial since qualitative feedback from many people with disabilities report more falls or stumbles while performing these tasks than straight walking.
Footnotes
Acknowledgements
The researchers would like to thank Jocelyn Fawcett, Julie Kim, Patrick Lebel, David Nielen, and Sylvie Maurice-Langis, for providing clinical expertise and Stephen Baskey, Marc Veilleux, and Shawn Millar for their assistance in the data collection process.
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was supported by The Ottawa Hospital, Center for Patient Safety, Implementation Projects Grants Program.