
Abstract
Background:
Increased impact loading is implicated in knee osteoarthritis development and progression.
Objectives:
This study examined the impact ground reaction force (GRF) peak, its loading rate, its relative timing to stance phase timing, and walking speed during unilateral and bilateral use of laterally wedged insoles with arch supports.
Study design:
Within-subject design.
Methods:
Thirty-three female patients with medial knee osteoarthritis were examined with (unilateral 6° and 11°, and bilateral 0°, 6°, and 11°) and without insole use.
Results:
Repeated measures MANOVA revealed that the impact force increased significantly in bilateral 11° versus unilateral 6° and without-insole conditions. The loading rate decreased significantly in unilateral 11° versus bilateral 6° insoles. The relative timing increased significantly in each of bilateral 6°, bilateral 11°, and unilateral 11° versus bilateral 0° insoles and in each of bilateral 11° and unilateral 11° versus without-insole condition. There were significant positive correlations between the walking speed and each of the force and loading rate. The Chi-square test revealed insignificant association between the insole condition and the presence of impact forces.
Conclusion:
Unilateral 11° insoles are capable of reducing impact loading possibly through increasing foot pronation. Walking slowly is another possible strategy to reduce loading.
Clinical relevance
Unilaterally applied 11° laterally wedged insoles are capable of reducing and delaying the initial impact ground reaction forces and reducing their loading rates during walking in patients with medial knee osteoarthritis, thus reducing osteoarthritis progression. Walking slowly could also be used as a strategy to reduce impact loading.
Background
Knee osteoarthritis (KOA) is a prevalent joint disease that contributes significantly to functional disability. According to the World Health Organization, it is the fourth most important cause of disability in women and the eighth in men. 1 It is a multi-factorial disease with excessive joint loading being one of the main risk factors. 2 Thus, KOA is suggested to be mechanically driven. 3
During normal walking and within the first 50 ms of initial contact, impact ground reaction forces (iGRFs) are created at the foot–floor interface due to energy and momentum exchange. 4 These are sudden vertical forces that result from collision between the heel and ground. 5 Typically, iGRFs have magnitudes of 1.5 times body weight at slow velocities (2 m/s) and 3 times at fast velocities (7 m/s).6–9 These forces are transmitted up the skeleton as shock waves 10 that damage soft tissues, causing leg and back pain, 11 degenerative arthritis, prosthetic joint loosening, and stress fractures. 12 Based on animal studies, iGRFs cause OA through micro-damage in the subchondral bone which causes deep layer cartilage calcification and cartilage narrowing. 13 Fortunately, the locomotor system attenuates these harmful forces through the passive and active systems. 14 The passive system involves noncontractile structures such as the heel fat pads, joint cartilages, and intervertebral discs, while the active system involves the neuromuscular control strategies and lower extremity kinematics. 15 When there is affection of these systems as in KOA, 16 the shock-absorbing capacity of iGRFs is reduced 17 and excessive impact loading occurs during walking. 18
Understanding factors that affect the magnitude of iGRFs represents an important key for managing KOA. 19 These factors include the type of footwear, 20 walking speed, ground surface, 15 velocity and angle with which the foot meets the ground, 21 and foot pronation.22,23
The viscoelastic material used in footwear construction or placed within shoes as insoles appears to provide the greatest protection from these damaging forces. 15 Viscoelastic insoles redistribute pressure beneath the foot, 24 attenuate iGRFs, 25 and provide symptomatic relief in patients with degenerative arthritis. 26 Pressure relief depends on material elasticity,15,24 whereas iGRF attenuation depends on material viscosity.15,25
Similarly, foot pronation/eversion helps in iGRF attenuation.23,27 With increased pronation range of motion or duration, iGRFs are attenuated over an extended time. 28 A longer time requires reduced magnitude of average forces which allows for gradual attenuation of momentum 22 (Faverage = change in momentum/change in time). 29
Combining the beneficial effects of viscoelastic insoles and foot pronation in reducing iGRFs suggested examining the effect of laterally wedged insoles (LWIs) on impact loading in patients with medial KOA. The effect of LWIs on external knee adduction moment (KAM) was extensively studied. This is a compartment-specific measure of knee joint loading with peak values occurring at approximately 30% and 70% of stance phase. 30 KAM has received much interest in OA literature due to its association with clinical outcomes such as disease severity 31 and progression. 2 Despite this great interest, a big controversy still exists toward the effect of LWIs in reducing KAM.32–38 Yet, no studies were conducted on the effect of LWIs in reducing impact loading in this patient population. Impact loading refers to the load imposed on the human body as a result of collision between the body and ground. It is another measure of joint loading that is not compartment specific, occurring immediately after initial contact. 39 Thus, studying the effect of LWIs on this measure may provide additional information and help with reducing joint loading irrespective of the ability of LWIs to reduce KAM.
Our interest involved comparing the effects of unilateral versus bilateral use of LWIs on impact loading. Unilateral use may result in postural asymmetry with one foot being more pronated than the other. 40 Accordingly, the consequent musculoskeletal disorders as scoliosis,41,42 sacroiliac dysfunction, sciatica, and chondromalacia 40 could be avoided.
Finally, we were interested in examining LWIs that have medial arch supports. Such insoles reduce excessive foot pronation (expected to occur with LWIs of high inclinations) while still preserving the ability of reducing KAM similar to LWIs that do not have supports. 43 Excessive foot pronation causes improper stress distribution along the lower extremities long bones through increasing tension on the medial aspect of the subtalar joint, compression on the lateral aspect, and torsion of the tibia, 22 in addition to increasing local peak pressures on the sole of the foot while walking. 44
So, the primary purpose of this study was to compare the effects of unilateral and bilateral LWIs with arch supports on impact loading measures (iGRF magnitude and loading rate (LR)) together with the walking speed that is known to affect GRF measures. 19 We hypothesized that LWIs would contribute to reducing impact loading. The secondary purposes were to examine the association between the walking speed and iGRF loading measures and the association between insole condition and presence of iGRFs. Although it is well known that the walking speed affects GRF loading measures,45,46 we were interested in determining the extent and significance of this association and whether modifying the walking speed could be used as a strategy to avoid the hazards of increased impact loading. Furthermore, since about one-third of adults have iGRFs in their GRF profile 46 and impact loading is typically quantified by testing for the presence of iGRF peaks in the GRF profile aside of examining LRs, 19 we were interested in examining if certain insole conditions are associated with iGRFs.
Methods
Subjects
Upon approval of Cairo University’s Supreme Council of Postgraduate Studies and Research, 33 female patients with primary medial KOA participated in the study after giving informed consent. Their mean (standard deviation (SD)) age, weight, and height were 55.03 (7.52) years, 83.61 (8.81) kg, and 1.57 (0.06) m, respectively. They were referred by two physicians who were informed of subject inclusion criteria. The American College of Rheumatology criteria 47 were used for diagnosing medial KOA. Both unilateral and bilateral KOA affection were tested in this study. Patients had radiographic evidence of Kellgren and Lawrence 48 grade II or III medial KOA and lateral femoro-tibial angle of 176°–180° indicating varus alignment.49,50 The varus degree was defined as it affects the impact LRs and the presence of iGRFs. 19 Exclusion criteria involved having any serious inflammatory disease, previous knee joint trauma, surgery, intra-articular corticoid injection within the previous month, significant foot deformity, and concurrent use of any orthotics.
Instrumentation
A six-camera three-dimensional (3D) motion analysis system (120 frames/s; ProReflex; Qualisys Inc, Gothenburg, Sweden) with an AMTI (Advanced Mechanical Technology Inc., Watertown, MA, USA) force plate with a sampling rate of 1200 Hz was used for measuring the concerned variables. The variables were the iGRF peak, iGRF LR, iGRF relative timing to stance phase timing, and walking speed.
Nonwedged and wedged insoles with 0°, 6°, and 11° lateral inclinations and medial arch supports were tested. The 0° insole was tested bilaterally “0° × 0°” and used as control. Each of the 6° and 11° insole was tested once bilaterally “6° × 6° and 11° × 11°” and another unilaterally “6° × 0° and 11° × 0°.” The 6° and 11° LWIs were used on the tested limb, and the 0° insoles were used on the untested limb in unilateral insole testing. The tested limb was the affected one in patients with unilateral affection and the most symptomatic in patients with bilateral affection. Finally, a without-insole condition was tested to examine the effect of using versus not using insoles on the tested variables. All insoles were inserted in unified shoes as iGRFs are affected by heel heights,10,51 thickness, compressibility, and material of construction. 15 Figures 1 to 3 illustrate the construction of LWIs and shoes.
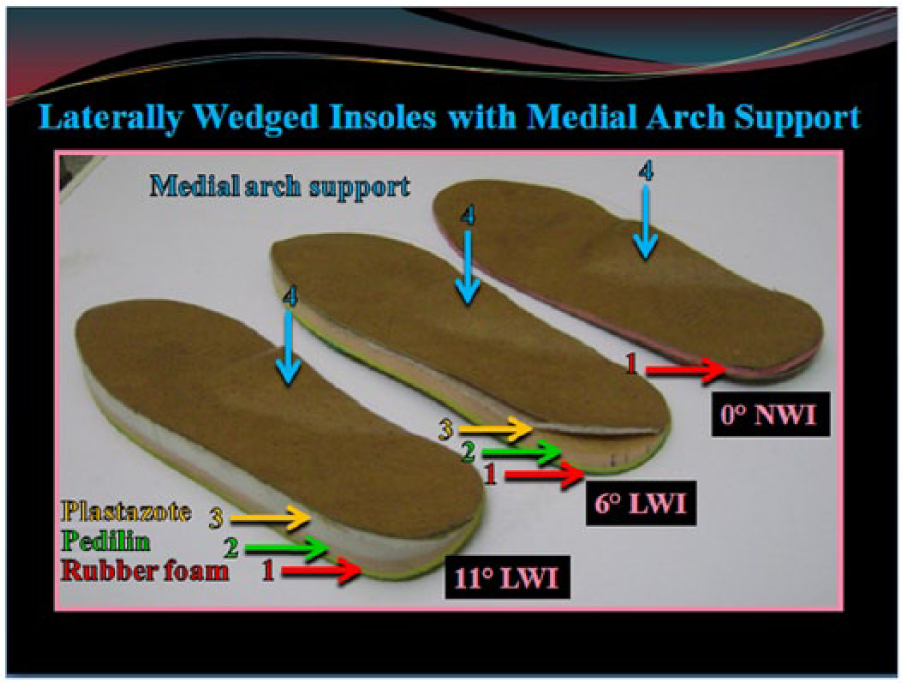
The construction of the tested insoles; a 3-mm even thickness sheet of rubber foam (1), a 5-mm laterally wedged sheet of Pedilin (2), and a 2-mm (in 6° LWI) or 8-mm (in 11° LWI) laterally wedged sheet of Plastazote (3) with a medial arch support (4). Mentioned are the initial heights before considering compression.
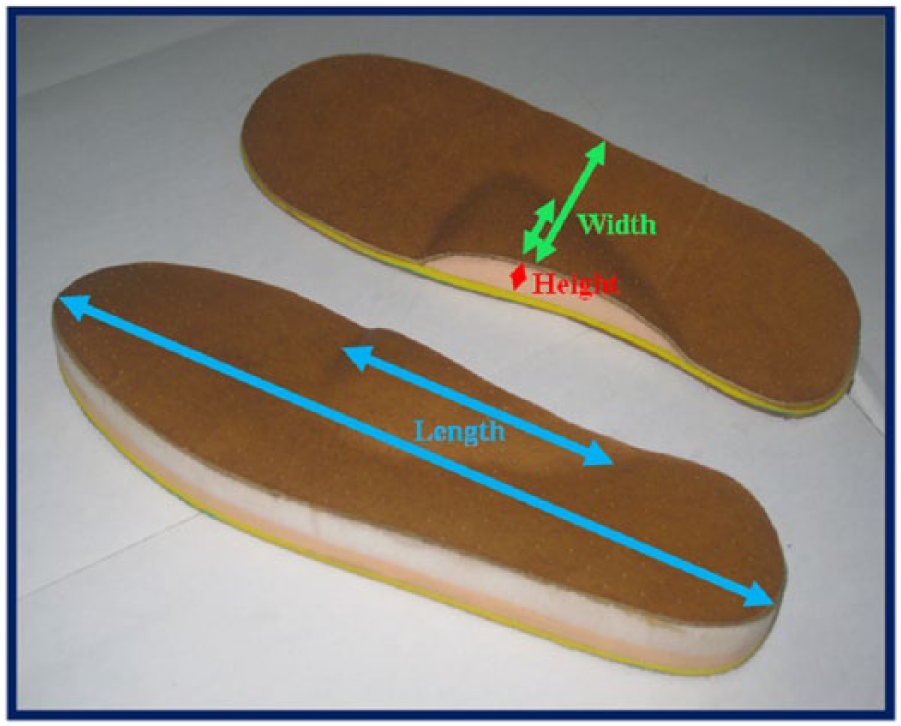
The tested prefabricated medial arch support. Its length is 33% of the insole length and width 45% of the insole width at the level of the peak height of the arch which is 1 cm (excluding the rubber foam height).

A pair of thin flexible-soled shoes with stretchable body to fit adequately to the patients’ feet. Thin flexible-soled shoes were tested so that the loads on the force plate would not be dampened by thick inflexible ones. 52
Procedures
This study involved a within-subject design where one group of patients was tested at all six insole conditions. Patients randomly selected insole testing order by drawing from six folded papers placed in a container. A total of 20 passive reflective markers were placed by the same investigator on their respective landmarks. 53 Patients were accommodated to the testing procedure by walking along a 10-m walkway for few minutes. 52 Four successful trials of foot–force-plate contact were captured while walking at a self-selected speed determined by a 10-m timed walk. 54 Trials were considered successful when the patients contacted the force plate with the involved limbs without adjusting their stride length. Patients took two practice walks with every insole condition to become familiar with its use and ensure that the insoles were properly placed. All investigations followed the ethical and human principles of research.
Data processing
The “Qualisys” system was used for analyzing the kinetic data and assessing the walking speed. The iGRF peak appears as a short spike of force superimposed on the vertical GRF vector just after initial contact 55 (Figure 4). It was normalized to body weight (N/kg). The iGRF LR was calculated as the slope from the point of initial contact to iGRF peak.18,19 This was done by dividing the magnitude of iGRF peak by the time it takes from initial contact to reach this peak (N/kg s). High vertical GRF LRs represent rapid deceleration of the center of mass in the vertical direction 55 reflecting fast rise of the vertical GRF to its peak. 56 The iGRF peak relative timing was calculated by dividing the time it takes to reach the iGRF peak by the whole time of the stance phase (%). Finally, the walking speed was provided directly by the “Qualisys” system.
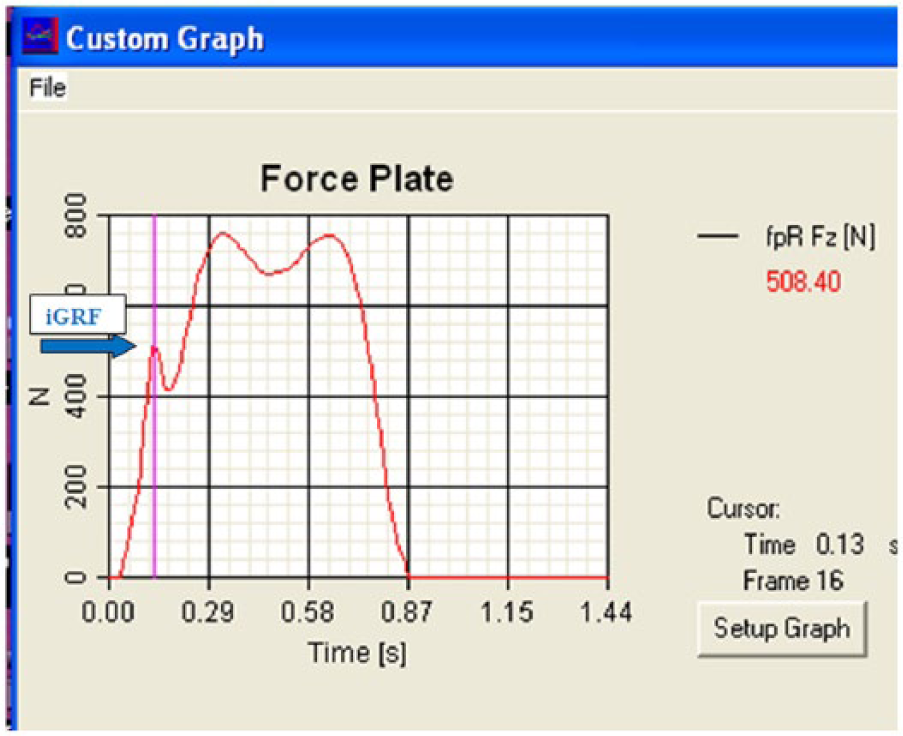
A data output of the vertical ground reaction force vector showing the initial impact ground reaction force (iGRF) peak in patients with medial knee osteoarthritis.
Data analysis
All statistical measures were performed using the Statistical Package for Social Sciences (SPSS) v17. Initially, data were screened for normality assumption through using the Kolmogorov–Smirnov and Shapiro–Wilk’s normality tests and testing for the presence of extreme scores and significant skewness and kurtosis. Once data were found not to violate the normality assumption, parametric analysis was conducted.
Repeated measure multivariate analysis of variance (MANOVA) was used to compare the tested variables among the six insole conditions. Pearson product correlations were used to examine the association between the walking speed and iGRF measures under the different insole inclinations. Correlations were conducted using the data of the five insole conditions only after excluding those of the without insole. Knowing that about one-third of adults have iGRFs in their GRF profile 56 and with the aim of examining the effect of LWIs on iGRFs and the association between the walking speed and iGRF measures, the repeated measure MANOVA and correlation analyses were conducted on 13 (39.39%) patients only. These patients were those who showed consistent presence of iGRFs in their vertical GRF profile. Consistency was determined as having iGRFs in all insole conditions with at least 50% of the trials showing iGRFs at each condition. The four tested variables were not considered in patients who missed iGRFs in any of the insole conditions (20 patients, 60.6%).
Finally, the Chi-square test was used to examine whether certain insole conditions are associated with iGRFs. The Chi-square test was conducted on all 33 patients. The number of patients who had iGRFs in at least 50% of the trials was counted at each condition, and comparison among these numbers was conducted. The level of significance was set at p < 0.05 for all tests.
Results
The repeated measure MANOVA with the subsequent Bonferroni post hoc analysis showed that the magnitude of iGRF decreased significantly (p < 0.05) in 6° × 0° versus 11° × 11° and without-insole versus 11° × 11° conditions. In addition, the iGRF LR decreased significantly in 11° × 0° versus 6° × 6° condition. Finally, the iGRF relative timing increased significantly in 6° × 6° versus 0° × 0°, 11° × 0° versus 0° × 0°, 11° × 11° versus 0° × 0°, 11° × 0° versus without-insole, and 11° × 11° versus without-insole conditions (Tables 1 and 2). However, there was no significant difference for the walking speed.
Descriptive statistics of the initial impact ground reaction force loading measures together with speed of walking in patients with medial knee osteoarthritis during the six tested insole conditions.
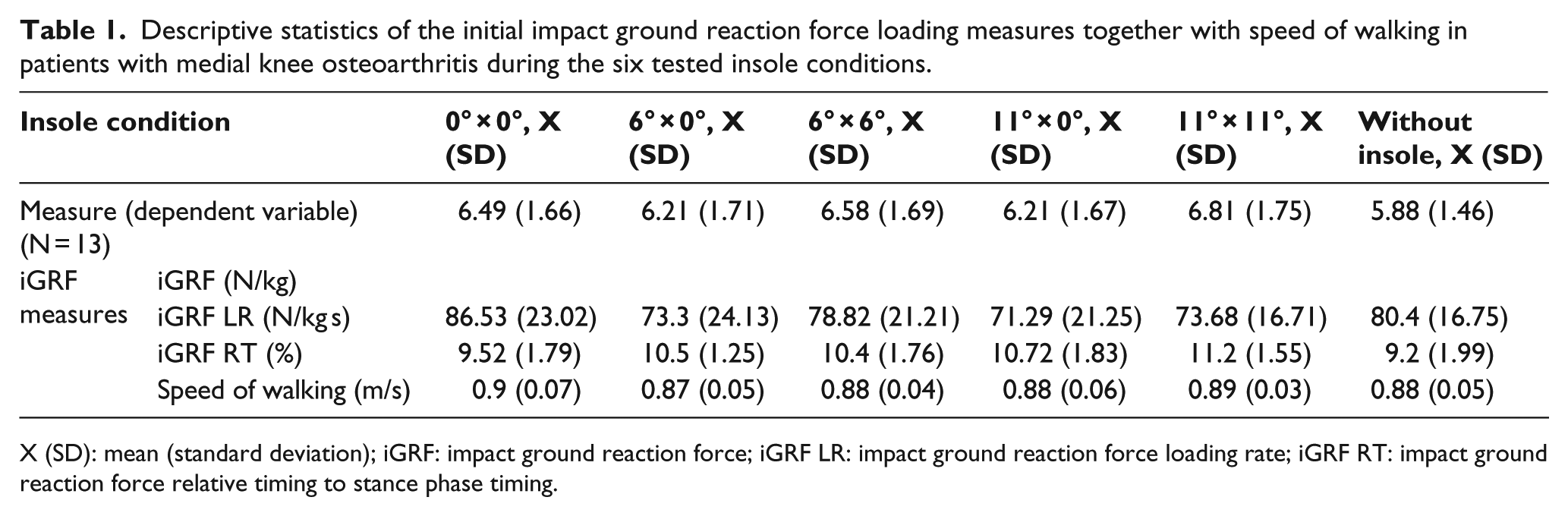
X (SD): mean (standard deviation); iGRF: impact ground reaction force; iGRF LR: impact ground reaction force loading rate; iGRF RT: impact ground reaction force relative timing to stance phase timing.
Multiple pairwise comparison tests among the six tested insole conditions for the initial impact ground reaction force loading measures in patients with medial knee osteoarthritis.
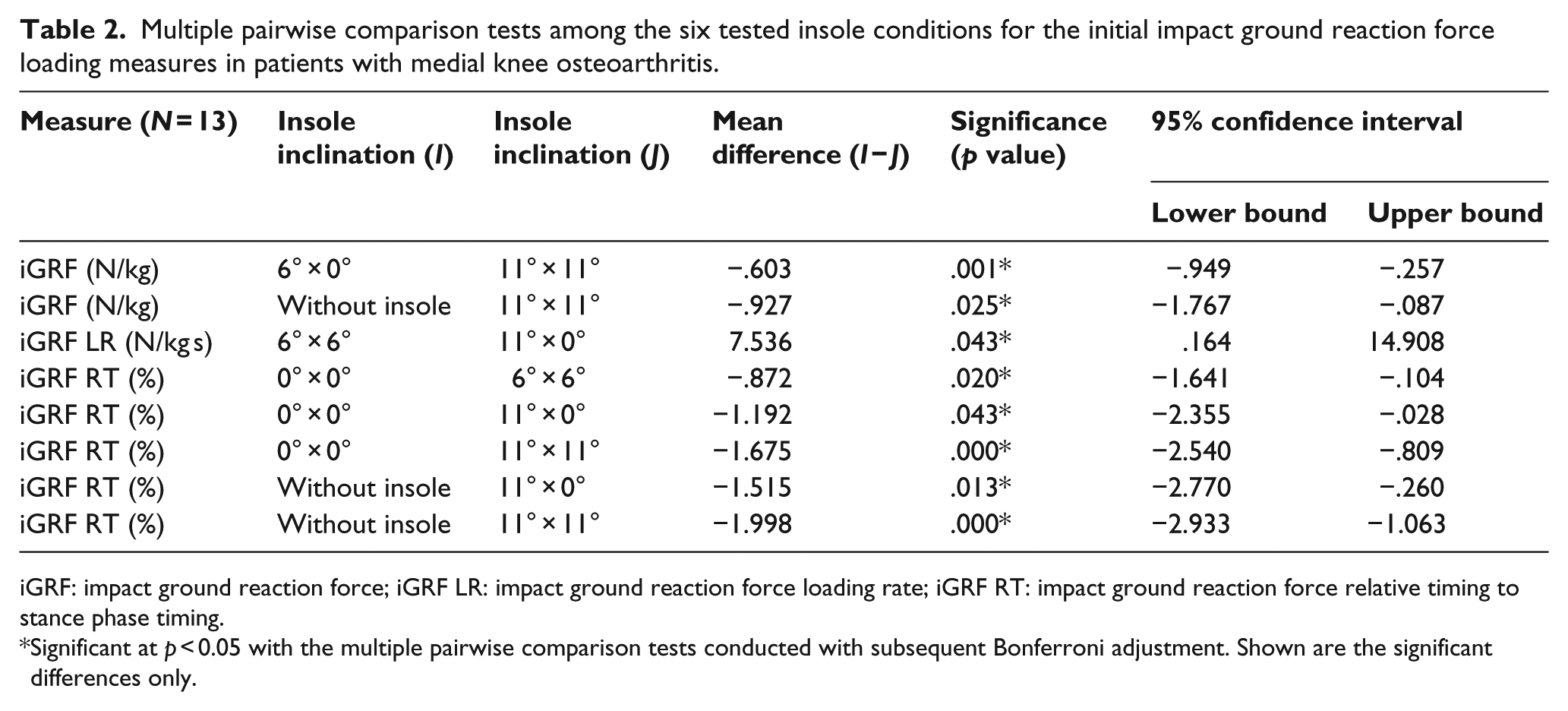
iGRF: impact ground reaction force; iGRF LR: impact ground reaction force loading rate; iGRF RT: impact ground reaction force relative timing to stance phase timing.
Significant at p < 0.05 with the multiple pairwise comparison tests conducted with subsequent Bonferroni adjustment. Shown are the significant differences only.
There were significant strong positive correlations (p = 0.000) between the walking speed and each of the iGRF (r = 0.723) and iGRF LR (r = 0.681). The regression equations were iGRF = −0.82 + 8.216 × walking speed (R2 = 0.523) and iGRF LR = −11.953 + 100.089 × walking speed (R2 = 0.464) (Figure 5).
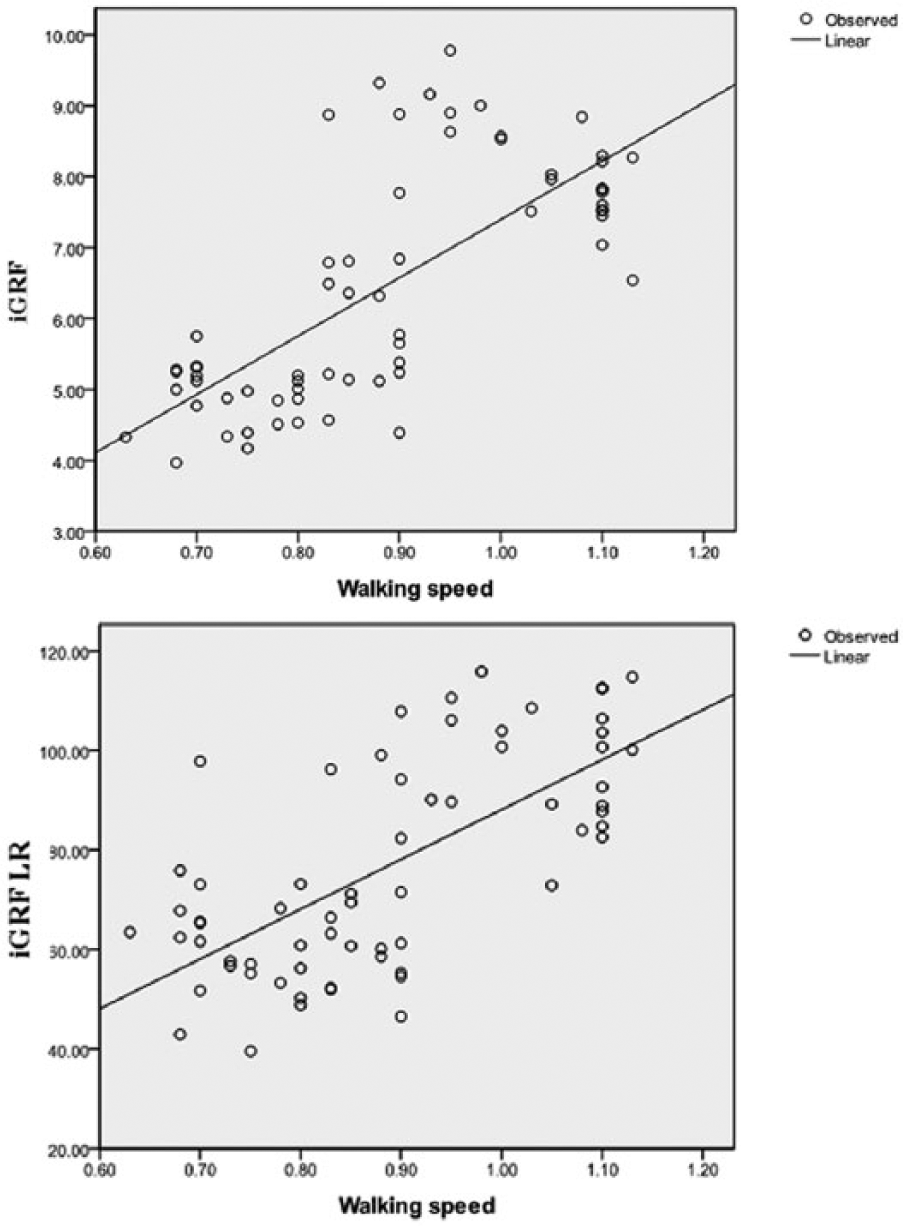
Scatter plot for the bivariate correlations between the speed of walking and each of the initial impact ground reaction force peak and its loading rate with laterally wedged insole use in patients with medial knee osteoarthritis.
Finally, the Chi-square test showed that the number of patients having iGRFs in the 0° × 0°, 6° × 0°, 6° × 6°, 11° × 0°, 11° × 11°, and without-insole conditions was 18, 17, 18, 15, 16, and 17 respectively. There was no significant association between insole condition and the presence of iGRFs (χ2 = 0.829, p = 0.985).
Discussion
Findings revealed that iGRFs decreased significantly in 6° × 0° versus 11° × 11° and without-insole versus 11° × 11° conditions. The poor proprioception 57 in this patient population 16 and unfamiliarity with insole use might have affected the angle and velocity with which the foot contacted the floor. Possible approaches include stopping the foot in air before contact or allowing the ground to stop the foot. 15 When the velocity of the foot is brought rapidly to zero as in such cases, iGRFs are increased due to the increased deceleration. 58 Stopping the foot in air or allowing the ground to stop the foot are anticipated to have occurred with the thicker 11° × 11° LWIs, and accordingly, iGRFs increased in such thick insoles compared with the other two conditions. These swing-to-stance phase gait kinematic adjustments affect the magnitude of iGRFs.15,21,58
As a matter of concern, one may ask why iGRFs increased significantly in 11° × 11° versus 6° × 0° and without-insole conditions with no similar findings being reported for 11° × 0° LWIs despite using the thick 11° LWI on the tested limb. In 11° × 11° LWIs, the 11° LWI was used simultaneously on the untested limb. This means that during the swing phase and just prior to initial contact, the body was supported on the untested limb that became more pronated than its usual. This new pronation posture is believed to have caused postural changes and foot pressure re-distribution on this limb which might have interfered with normal gait mechanics and/or the support sensation perceived by the patient. Accordingly, the patient tried to adjust herself, for instance, through placing the tested limb (swinging limb) on the ground rapidly. The suggested kinematic adjustments and the consequent increased deceleration are believed to be responsible for the increased iGRFs. As opposed to 11° × 11° LWIs, the 0° nonwedged insole was used on the untested limb in 11° × 0° LWIs. Having a 0° inclination, this insole provides a support sensation that is similar to that perceived while being supported on a leveled ground. No postural changes are anticipated to have occurred on the untested limb, and even though if these changes have occurred, their effect was not evident. Yet, our suggestion could be verified in a future study after analyzing and interpreting the kinematic data that were collected during all trails.
Although numerous studies found that knee joint stiffness (extension/flexion position) prior to or at contact affects iGRFs,59–62 other studies suggest it does not.63,64 The former found that the more extended knees result in higher magnitudes of iGRFs. Based on these controversial findings, we do not believe that knee joint position relate to the recorded difference in this study.
With the walking speed being not significantly different among the tested insole conditions and with the tested footwear and ground surface being unified in this study, and the insignificant difference in the external subtalar eversion moment between 11° × 11° and 6° × 0° LWIs reported in our previous study, 53 the examiner does not support these factors to play a role in the detected differences in the iGRFs. However, the variable viscoelastic property of the foot–floor interface may greatly account for these differences especially when comparing 11° × 11° versus without-insole conditions. This affects the transfer of momentum between the foot and ground, hence controlling the magnitude and time course of the generated forces. 15
Considering the iGRF LR, it decreased significantly in 11° × 0° versus 6° × 6° LWIs. Although not statistically significant, the 11° × 0° LWIs were accompanied by lower iGRFs and higher relative timing compared with 6° × 6° LWIs. Accordingly, less LR was found with 11° × 0° LWIs.
Another possible reason for the significant reduction in the LR is the significant increase in the subtalar eversion moment in 11° × 0° versus 6° × 6° LWIs. 53 Our findings are in accordance with those reported by Perry and Lafortune 23 who found that exaggerated pronation reduced the LR although not statistically significant. They related the insignificant difference to the tested insoles that tapered past the posterior one-third of the shoe which might have had minimal effect on the forefoot that contributes to the support function of the foot. It should be noted that they tested recreational runners not patients and the tested sample was small which might have decreased the statistical power.
The proposed effect of pronation on decreasing the LR is further supported by comparing the findings of our previous study 53 with those of the present one. Abdallah and Radwan 53 showed that the subtalar eversion moment increased significantly in 11° × 0° versus 6° × 0° and 11° × 11° versus 6° × 6° LWIs. When comparing the magnitudes of the recorded LRs in this study, it could be noticed that they, although not statistically significant, also decreased in 11° × 0° versus 6° × 0° and 11° × 11° versus 6° × 6° LWIs.
Regarding the iGRF relative timing, it increased significantly in 6° × 6° versus 0° × 0°, 11° × 0° versus 0° × 0°, 11° × 11° versus 0° × 0°, 11° × 0° versus without-insole, and 11° × 11° versus without-insole conditions. The increased relative timing indicates delayed iGRFs. Since reduction in body momentum during stance phase depends on the integration of force and time, a longer time may help with attenuating body momentum through reducing the magnitude of experienced forces. 22 Again, these insole conditions produced significantly higher subtalar eversion moment compared with the 0° × 0° condition. 53
Our findings are supported by that reported by Levinger and Gilleard. 65 They found that their patients had significantly lower and delayed iGRFs compared with the controls. They related this to the rearfoot eversion that was present at the time of iGRFs in these patients compared with inversion in the controls. They declared that these changes were not due to altered walking speed.
Controversially, our findings revealed no significant differences in the walking speed among the six insole conditions. This assures that the obtained significant differences in the iGRF measures were not related to walking speed.
Regarding the correlation analysis, highly significant strong positive correlations between the walking speed and each of the iGRF and iGRF LR were found. Similar findings were reported by several researchers15,19,66 although they did not test wedged insoles. The decreased impact loading with decreased walking speed support the recommendations of walking slowly for this patient population to reduce the stresses imposed on the musculoskeletal system.67–69
Finally, no significant association between insole condition and the presence of iGRFs was found. This implies that the presence of iGRFs is not affected by the degree of insole inclination, application form, or insole use.
Summing it up and after considering the effect of each insole on the tested variables, it was noticed that unilateral 11° LWIs combine the beneficial effects of reducing iGRFs (producing the least magnitude in the insole conditions similar to the unilateral 6° LWIs) and iGRF LR and delaying iGRFs. Thus, it is recommended to use these insoles for reducing impact loading which indicates that our hypothesis was accepted. Moreover, decreasing the walking speed may also help with reducing impact loading.
Last but not the least, it should be noted that 11° LWIs are not associated with great discomfort as expected. Although Toda et al. 70 tested LWIs with subtalar strapping and tested insoles made of urethane, they found that the remission score of the Lequesne index of severity for KOA was greatly improved in 11.2° LWIs than in 8.5° and 16.8° ones. The insoles were worn for 2 weeks with a daily use of 3–6 h and were replaced every week. The adverse effects reported by the participants (most commonly foot sole pain) were not severe enough to stop them from continuing wearing the insoles. The rates of adverse effects were significantly less in each of the 8.5° (10%) and 11.2° (14.3%) groups than in the 16.8° (42.8%) group. The researchers concluded that both the 8.5° and 11.2° LWIs are more comfortable than the 16.8 ones for constant normal use.
The findings of this study are limited by the inability to be generalized to the male population and to all materials used in insole construction. Female patients were tested due to the higher incidence of KOA in females 71 and because impact LRs differ with gender. 55 Construction materials have different material viscoelastic properties and response to repeated compression. 72 This suggests examining different materials with prolonged insole use to see the consistency of findings with repeated compression. Moreover, muscle activity should also be studied prior to applying the findings in clinical settings as additional muscles may be activated in an attempt to control any postural changes caused by new interventions which in turn may affect fatigue, comfort, and work/performance. 73
Conclusion
Patients with medial KOA may benefit from the use of unilateral 11° LWIs. Such insoles can help with reducing iGRF magnitudes and loading rates that are implicated in KOA development and progression.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.