
Abstract
Background:
Knee osteoarthritis is a major contributor to the global burden of disease. There is a need of reducing knee joint load and to improve balance and physical function among knee osteoarthritis patients.
Objectives:
To test the hypothesis that toe-out gait will reduce second peak knee adduction moment further and increase fall risk when combined with knee brace and laterally wedged insole in knee osteoarthritis patients.
Study design:
Single visit study with repeated measures.
Methods:
First and second peak knee adduction moments, fall risk and comfort level. First and second peak knee adduction moments were determined from three-dimensional gait analysis, completed under six randomized conditions: (1) natural, (2) knee brace, (3) knee brace + toe-out gait, (4) laterally wedged insole, (5) laterally wedged insole + toe-out gait, and (6) knee brace + laterally wedged insole + toe-out gait. Fall risk was assessed by Biodex Balance System using three randomized stability settings: (1) static, (2) moderate dynamic setting (FR12), and (3) high dynamic setting (FR8).
Results:
The reduction in first peak knee adduction moment and second peak knee adduction moment was greatest (7.16% and 25.55%, respectively) when toe-out gait combine with knee brace and laterally wedged insole. Significant increase in fall risk was observed with knee brace + laterally wedged insole + toe-out gait (42.85%) at FR12. Similar significant balance reductions were found at FR8 condition for knee brace + toe-out gait (35.71%), laterally wedged insole + toe-out gait (28.57%), and knee brace + laterally wedged insole + toe-out gait (50%) as compared to natural. However, knee brace decreased fall risk at FR12 by 28.57%.
Conclusion:
There is a synergistic effect of toe-out when combined with knee brace and laterally wedged insole concurrently in second peak knee adduction moment reduction but with a greater degree of fall risk. Simultaneous use of conservative treatments also decreases comfort level.
Clinical relevance
Patients with mild and moderate knee osteoarthritis are usually prescribed conservative treatment techniques. This study will provide an insight whether or not a combination of these techniques have a synergistic effect in reducing knee joint load.
Background
Knee osteoarthritis (kOA) is the most commonly occurring type of osteoarthritis in the world, 1 largely because of its wearisome mobility and load-bearing characteristics during gait. It inflicts an irreversible damage to the skeletal structures, including bone, cartilage, and joint capsule. 2 Pain and stiffness observed in this degenerative disease are mainly caused by narrowing of the joint space. 3 A higher share (~70%) of the knee joint load is borne by the medial compartment of the joint; hence, this compartment of an osteoarthritic knee is the most severely affected by the deteriorating effects. 4 A resulting varus alignment of the knee joint is not only a major risk factor in medial compartment kOA progression but also further aggravates the imbalance of load distribution between the medial and lateral compartments of the knee joint. 5 The knee adduction moment (KAM) when calculated through three-dimensional (3D) motion analysis of kOA patients has proven this imbalanced load distribution across the osteoarthritic joint.6,7 Across these analyses, KAM has been accepted as a fairly reliable and accurate surrogate measure of the load exerted on the medial compartment of the knee joint.7–10 It is also reported to be highly related to kOA severity and progression, and as a result, to the knee joint damage.10,11 Due to this reliability, the aim of most of the conservative treatment techniques for kOA is to reduce KAM during gait. Biomechanically, KAM is the frontal plane component of ground reaction vector and is a product of ground reaction force (GRF) and its lever arm.6,12 In order to reduce KAM, one can reduce either GRF or its perpendicular distance to the knee joint center. Since GRF is a reaction force in response to the weight of a person, it cannot be reduced. The only plausible option hence is to reduce the lever arm. The aim, therefore, of conservative treatments for medial kOA is to reduce KAM by reducing its lever arm thus slowing down the progression of kOA. Generally, conservative treatments include the use of knee brace (KB), laterally wedged insole (LWI), and gait retraining methods. The KB is designed to apply 3-point or 4-point pressure system around the knee joint to either push or pull the joint into a lesser-degree varus position during both stance and swing phases of gait. 3 The LWI attempts to reduce KAM by laterally shifting the center of pressure (CoP) at the base of the foot and increasing the subtalar joint valgus moment. This lateral shifting of CoP and the counteractive moment lead to a decrease in GRF lever arm, decreasing KAM.13–15
Currently, it is a matter of interest among healthcare professionals and a subject of many scientific studies that an alteration in gait may result in a reduced joint load and a symptomatic relief among kOA patients.16–19 The gait alterations include medio-lateral trunk sway,20–22 reducing the walking speed19,23 and an alteration in the foot progression angle (FPA).16,24–29
An increase in the FPA, commonly called toe-out gait (TO), is found to be reducing the GRF lever arm by shifting the CoP laterally, just around heal-off. 19 This lateral shifting reduces the lever arm of GRF and reduces the KAM. Validated results from several studies suggest that KB, LWI, and gait retraining methods are effective in KAM reduction individually.19,30–34 As the next step, there is a growing research interest in the synergetic effect of these conservative treatment techniques when they are used in a combination.18,35 One of such studies examined the combined effect of KB and LWI and found better results in reducing KAM with their combined usage. 36 Another study has showed that the combined effects of TO and LWI lead to a better reduction in KAM. 18 However, the combined effect of all three conservative treatment techniques (KB, LWI, and TO) on KAM has not been tested yet.
Another hitherto unexplored effect of conservative treatment techniques is their effect on proprioception of the patients. Since wearing an orthosis or changing the foot’s natural FPA dislocates the body’s CoP, a potentially adverse effect of these techniques may be reducing the already compromised balance of the kOA patients.37,38 This potentially increased fall risk needs to be avoided, especially for the elderly, because of highly reported fall-induced injuries,39–41 hospitalization, 42 and even fatalities. 43 Moreover, the fundamental aim of a conservative treatment technique is to facilitate the performance of the activities of daily living (ADLs). Since maintaining balance and reducing fall risk is a major contributor in performing ADLs, the therapists should make sure that the prescribed conservative techniques are not impairing the proprioception of the patient.
Therefore, our primary objective was to test the immediate effects of the simultaneous use of KB, LWI, and TO on KAM. We hypothesized that TO would reduce the second peak knee adduction moment (sKAM) further when combined with KB and LWI. Furthermore, as we know that the people with kOA also experience a loss of proprioception,44,45 our secondary objective was to test the immediate effects of the simultaneous use of KB, LWI, and TO on fall risk in patients with medial kOA. We hypothesized that TO would increase fall risk significantly when combined with KB and LWI.
Material and methods
Subjects
Twenty participants with bilateral symptomatic medial kOA were recruited from the Department of Sports Medicine, University of Malaya Medical Centre (UMMC). Medial compartment kOA was confirmed through radiographic evidence and was graded according to the Kellgren–Lawrence scoring system. The patients’ diagnosis was confirmed through clinical evidence at the UMMC. The experiment was conducted at the Body Performance and Motion Analysis Laboratory, University of Malaya.
Inclusion and exclusion criteria
Participants aged between 50 and 70 years, and having a body mass index (BMI) of less than 30 kg/m2 (non-obese), 46 were included in the study. The bilateral kOA participants were of Kellgren–Lawrence grades II and III. The participants were required to ascend and descend a 10-step flight of stairs and jog 5 m safely. The participants were excluded on the basis of any neurological or musculoskeletal disorder, cardiovascular or respiratory disease, lower limb fracture/ surgery in the past 12 months, or inability to adapt TO pattern.
Sample size
The sample power calculations were based on KAM variables from previous studies18,36 and considered an F-test statistical design for repeated measures (within effects), with a moderate effect size of 0.25, 47 a power of 80%, and an alpha error of 5% suggesting at least 20 participants for this study.
Ethical approval
Ethical approval was obtained from UMMC Medical Research Ethics Committee (MREC) (MECID.NO: 20161-2070). All participants provided written informed consent for the study.
Interventions
KB
The study uses a 4-point leverage-based KB (Donjoy OA Adjuster™ 3, DJO Global, Vista, CA, USA), as depicted in Figure 1(a). We used more symptomatic leg for KB application.
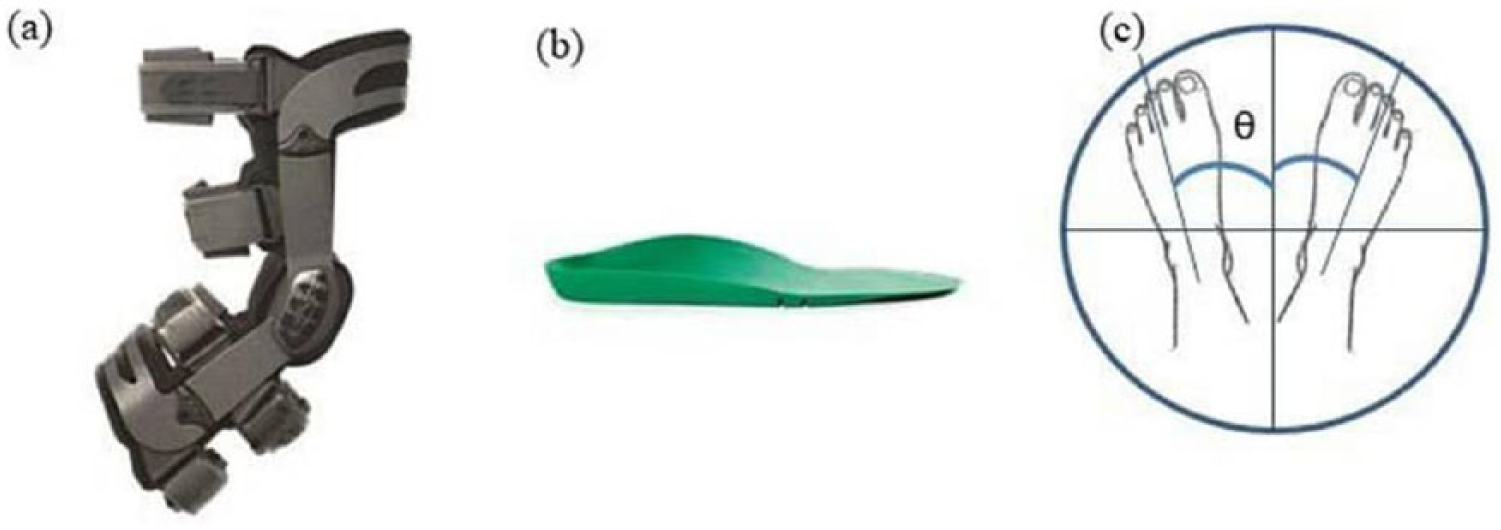
Interventions used as a conservative technique for knee osteoarthritis treatment: (a) knee brace (Donjoy OA Adjuster™ 3, DJO Global, Vista, CA, USA), (b) laterally wedged insole (salfordinsole™, UK), and (c) toe-out foot position, where θ is the foot progression angle, which is greater than 15° normal.
LWI
The LWI (Salford Insole™, Salford, UK) was full-length, with 5° frontal plane inclination, see Figure 1(b).
TO
The participants were introduced to walking with TO (TO: making V-shape with their feet) with the minimum toe-out angle of natural FPA plus 15°, see Figure 1(c). The toe-out angles were calculated by the degrees of which the foot vector (directed from the ankle joint center to the second metatarsal head) deviates from the progression axis of the walkway. 18
Data collection
The study was a single visit study, starting with a briefing about the interventions and the study protocol. Before the start of the experiment, the participants filled out the WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) questionnaire, version VA 3.1. It is a self-reported questionnaire containing three sections, one each for pain, stiffness, and difficulty performing daily activities. Each of the 24 questions is represented by a score of 0–10, with a higher score indicating worse pain, stiffness, or physical function. The participants were then provided with shoes (Supercloud, Adidas, London, UK) in order to minimize the influence of different shoes. Each participant was trained with the interventions especially for TO with adequate practice by the mutual discretion of the participant and the investigator. The data for motion analysis and fall risk assessment were then collected for the following six test conditions in a random order. Randomized orders were obtained through www.randomisation.com:
Natural condition (N);
With knee brace (KB);
With knee brace and toe-out gait combined (KB + TO);
With laterally wedged insole (LWI);
With laterally wedged insole and toe-out gait combined (LWI + TO);
With knee brace, laterally wedged insole, and toe-out gait combined (KB + LWI + TO);
The participants were asked to continue walking with a particular test condition until we obtained five legitimate trials (trials in which one foot is completely placed on one force plate). After each test condition, participants were asked to fill Wong-Baker FACES® Pain rating scale for the measurement of comfort level. The Wong–Baker pain rating scale is a pain scale showing a series of faces ranging from a happy face at 0 “No hurt” to a crying face at 10 “Hurts worst.” The patient must choose the face that best describes how they are feeling.
Procedure for motion analysis
The participants were asked to walk on the 5-m walkway with a constant speed of 1.18 m/s obtained through pilot study. 35 Constant walking speed was maintained for all six conditions by calculating the time taken to cover the distance using s = vt; where s = 5 m, t = time in seconds, and v = 1.18 m/s. An investigator observed the time taken for each walk trial during experimental trials, the ones falling within a standard deviation of <0.05 m/s compared to the target speed that was to be considered for data processing. Data collection was performed via VICON Motion Capture System (100 Hz; VICON, Oxford Metrics, Oxford, UK) consisting of five infrared-sensitive cameras. PlugIn Gait model (Oxford Metrics, Oxford, UK) of the driving software VICON Nexus was used to perform inverse dynamics analyses, obtaining joint moments calculated about an orthogonal axis system located in the distal segment of the joint.
The model attaches infrared markers to the participant’s skin or on the surface of the shoe that was directly above the bony prominence with the help of adhesive double-sided tape. Sixteen bony prominences defined by this model are anterior and posterior superior iliac spines, lateral thigh, lateral femoral epicondyle, lateral shank, calcaneus, lateral malleolus, and second metatarsal head. For the test conditions involving KB, we placed the marker on the surface of the KB directly above the lateral epicondyle of the femur. Two embedded force plates (1000 Hz; Kistler, Kansas City, MO, USA) in the walkway were used for the collection of GRF data. The data were smoothed with a third-order, 6-Hz Butterworth low-pass filter. The Newington–Gage model was used to calculate the hip joint center. 48 The knee and ankle joint centers were defined as the mid-points of the medial and lateral markers placed on the respective joints. The thigh segment was defined by the obtained hip joint center and the medial and lateral femoral epicondyles. The shank was defined by the obtained knee joint center and the medial and lateral malleoli. The foot was defined by the vector directed from the ankle joint center to the fifth metatarsal head. All KAM values were normalized to the percentage of the stance phase. Based on the previously reported two-peak waveform of the KAM, 19 the first peak knee adduction moment (fKAM) was taken as the maximum value during the initial 50% of the stance phase, while the second peak was taken as the maximum value during the latter 50% of the stance phase.
Procedure for fall risk assessment
The Biodex Balance System (BBS; Biodex Medical System Inc., Shirley, NY, USA) assesses a person’s neuromuscular control over balance. In simpler terms, it measures the static standing balance and dynamic standing balance of a person. The machine consists of a circular platform and a display unit, see Figure 2. The subject stands on the circular platform which tilts up to 20° in each direction (360° range of motion). The platform tilts according to the level set through the display unit. There are 12 levels of platform tilt, with level 12 offering the most stable platform (with maximum resistance) and level 1 offering the most unstable platform (with minimum resistance).

Biodex Balance System, Biodex Medical Systems, Inc. (courtesy: operation/ service manual).
For this study, the following set of platform settings was used in random order for all conditions:
FR Static: no platform movement.
FR12: each test trial starts from dynamic level 12 and keeps on decreasing to level 8.
FR8: each test trial starts from dynamic level 8 and keeps on decreasing to level 2.
The platform moves in anterior–posterior (AP) and medial–lateral (ML) axes simultaneously, giving three types of output measures: anterior/posterior stability index, medial/lateral stability index, and Overall Stability Index (OSI). These indices represent the standard deviations indicating the fluctuations around the reference point (a firm, horizontal platform). These indices are calculated by measuring the amount of time for which the platform has been deviated, along with the degree of angulation of this deviation from the reference point:
Medial/Lateral Stability Index (MLSI): represents foot displacements occurring in x-axis (ML axis).
Anterior/Posterior Stability Index (APSI) represents foot displacements occurring in the y-axis (AP axis).
Overall Stability Index (OSI) is a composite of APSI and MLSI and represents body sway in both x and y axes.
This study focused on OSI only because it is reported to be the most reliable parameter for assessing balance. 49 A higher score indicates lesser stability and greater postural variability in balancing the body on the platform. 37 BBS has been proven to have a good inter-tester and intratester reliability.38,50
The participants were asked to stand on the BBS facing the monitor, barefoot with eyes open, and their hands on their hips. Trials were discarded if they supported themselves with handlebars. The distance between the heels was kept constant at 0.16 m in order to avoid the adaptability effects on the stabilizing response due to different heel distances. 51 They were asked to stand straight and sway without changing their foot positions, in order to keep the moving black dot at the center of the crosshair displayed on the monitor. For each platform setting and each condition two trials were obtained, each of 30-s duration and separated by a 10-s rest period. For each participant, 18 data points were obtained (three platform settings × six test conditions).
Variables of interest
The parameters of interest were the fKAM and sKAM, knee adduction angular impulse (KAAI), and fall risk. fKAM and sKAM values were identified as the two peaks in the KAM values (early stance and late stance) obtained from the motion analysis software VICON Polygon™. The cases in which sKAM was not very distinct, it was obtained as the KAM value at the time of second vertical GRF. fKAM, sKAM, and KAAI values were normalized by dividing them by weight times height and taking them as a percentage. 52 KAAI was represented as the area under the KAM curve over stance phase and was obtained by the numerical integration of the curve.
Statistics
The Shapiro–Wilk test was applied to the data to assess normality. Repeated measures analysis of variance (ANOVA) was used to find within-subject effects at α = 5%. The Bonferroni corrections were applied during the post hoc pairwise comparisons to avoid false positives using IBM SPSS (SPSS Inc., Chicago, IL, USA).
Results
Demographics and WOMAC scores
The mean ± SD for age, height, and mass for the given sample were 61.5 ± 8.63 years, 1.63 ± 0.03 m, and 70.45 ± 8.80 kg, respectively. The WOMAC pain (0–50), stiffness (0–20), physical function (0–170), and total scores (0–240) were found to be 13.5 ± 5.65, 7.25 ± 7.16, 61.75 ± 31.45, and 82.5 ± 39.85, respectively.
FPAs
The mean ± SD for FPAs for the six test conditions were observed to be as N: 9.6° ± 3.7°, KB: 8.8° ± 3.5°, LWI: 9.4° ± 3.4°, KB + TO: 22.4° ± 3.1°, LWI + TO: 24.6° ± 3.6°, and KB + LWI + TO: 21.2° ± 4.3°. These FPAs were kept the same for fall risk assessment.
KAM
Figure 3 shows KAM profiles for the test conditions, normalized to 100% of the stance phase. Pairwise comparisons showed significant decrease in the fKAM from N (3.91 N m/%BW*Ht) when walking with LWI (3.66 N m/%BW*Ht, p = 0.03), LWI + TO (3.68 N m/%BW*Ht, p = 0.04), and KB + LWI + TO (3.63 N m/%BW*Ht, p = 0.01), see Figure 4. An insignificant decrease was observed in the fKAM when the participants walked with KB (3.82 N m/%BW*Ht, p = 0.20) and KB + TO (3.85 N m/%BW*Ht, p = 0.11).
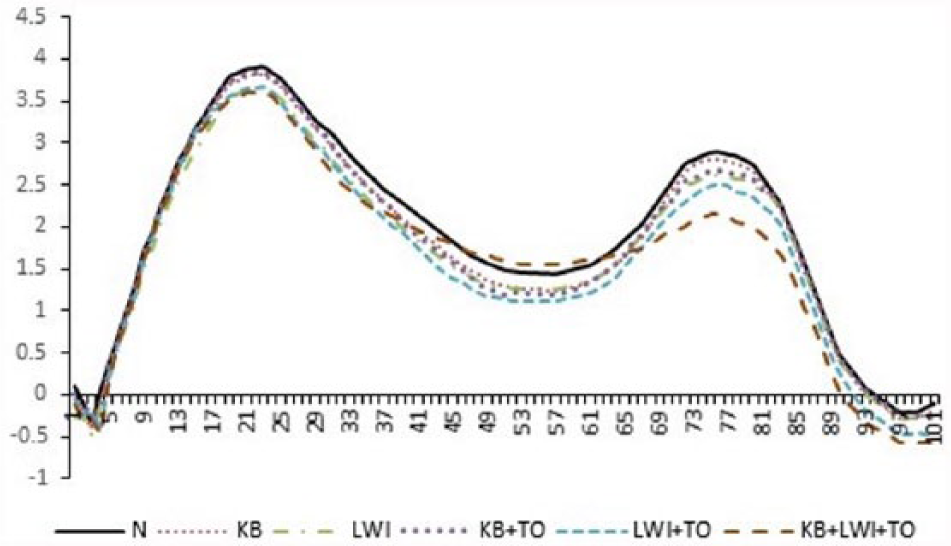
Knee adduction moment profiles of mean values for natural walk and different conservative treatment techniques for knee osteoarthritis normalized to 100% of the stance phase.
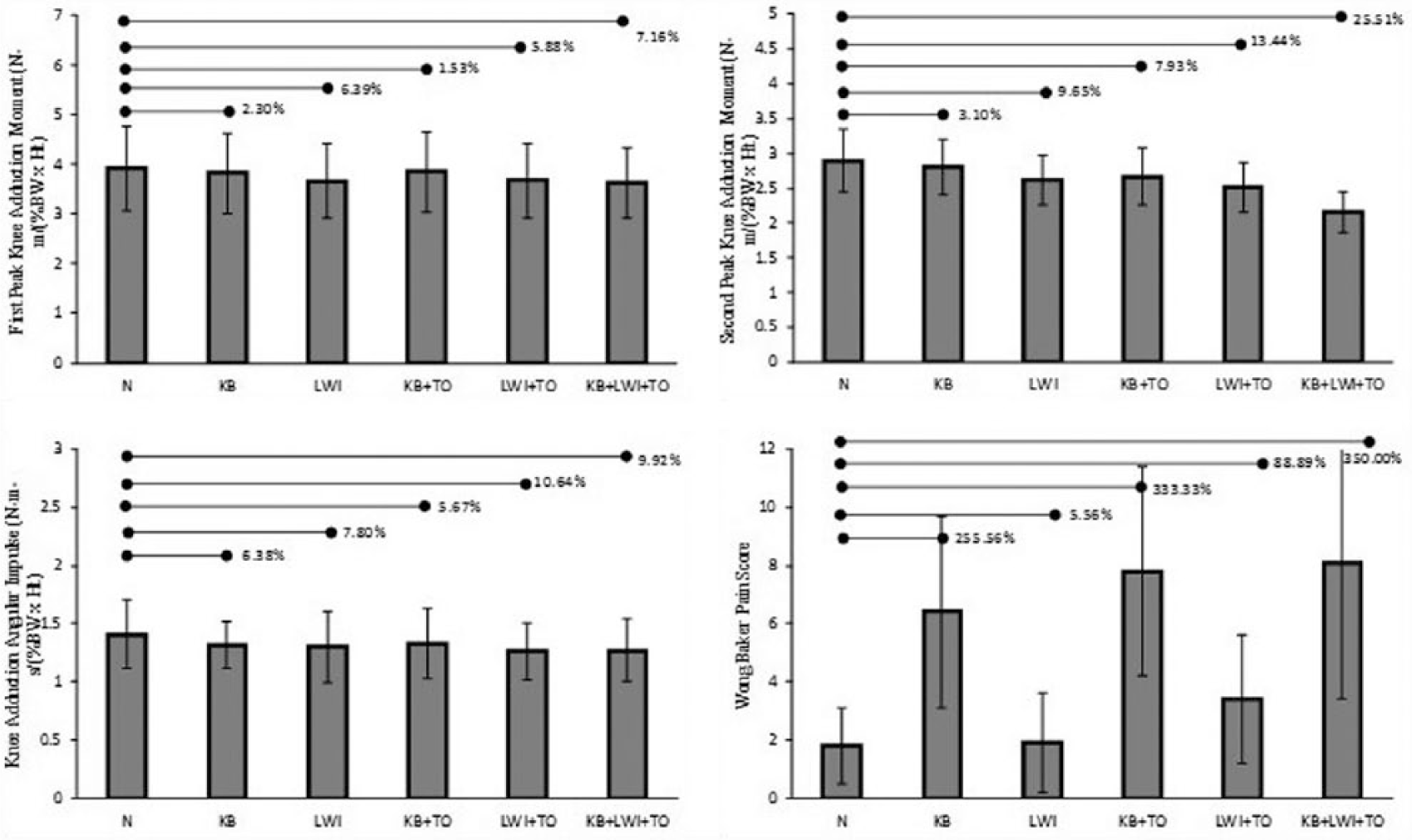
Bar charts representing first peak knee adduction moment, second peak knee adduction moment, knee adduction angular impulse, and Wong–Baker pain scores for N (natural walk), KB (knee brace), LWI (laterally wedged insole), KB + TO (knee brace along with toe-out gait), LWI + TO (laterally wedged insoles along with toe-out gait), and KB + LWI + TO (knee brace along with laterally wedged insole and toe-out gait). The horizontal lines and the accompanying numbers represent percentage difference from N.
For sKAM, pairwise comparisons showed significant main effect among test conditions (p < 0.001) as compared to N (2.90 N m/%BW*Ht). Significant reductions in the sKAM were observed for LWI (2.62 N m/%BW*Ht, p = 0.01), KB + TO (2.67 N m/%BW*Ht, p = 0.02), LWI + TO (2.51 N m/%BW*Ht, p < 0.01), and KB + LWI + TO (2.16 N m/%BW*Ht, p < 0.01), see Figure 3. KB (2.81 N m/%BW*Ht, p = 0.29) remained the only test condition with an insignificant reduction in sKAM.
KAAI
Post hoc analysis of repeated measures ANOVA showed significant differences among all test conditions when compared to N (1.41 N m s/%BW*Ht), see Figure 4. Significant reductions in the sKAM were observed for LWI (1.30 N m s/%BW*Ht, p = 0.01), KB (1.32 N m s/%BW*Ht, p = 0.02), KB + TO (1.33 N m s/%BW*Ht, p = 0.02), LWI + TO (1.26 N m s/%BW*Ht, p < 0.01), and KB + LWI + TO (1.27 N m s/%BW*Ht, p < 0.01)
Fall risk assessment
Table 1 shows the mean values of OSI at different test conditions. Significant reduction in the OSI were observed from N through pairwise comparisons when the participants stood on the BBS with KB + LWI + TO at FR12 platform setting. Similar reduction in the balance parameter was observed for KB + LWI + TO at FR8. The only intervention found to be improving balance was KB at FR12 setting, which decreased the fall risk by 28.6%. No significant differences were observed among the tests condition at static platform setting.
ANOVA results of Overall Stability Index values with natural walk and different conservative treatment techniques for knee osteoarthritis. The bold p-values denote statistical significance.
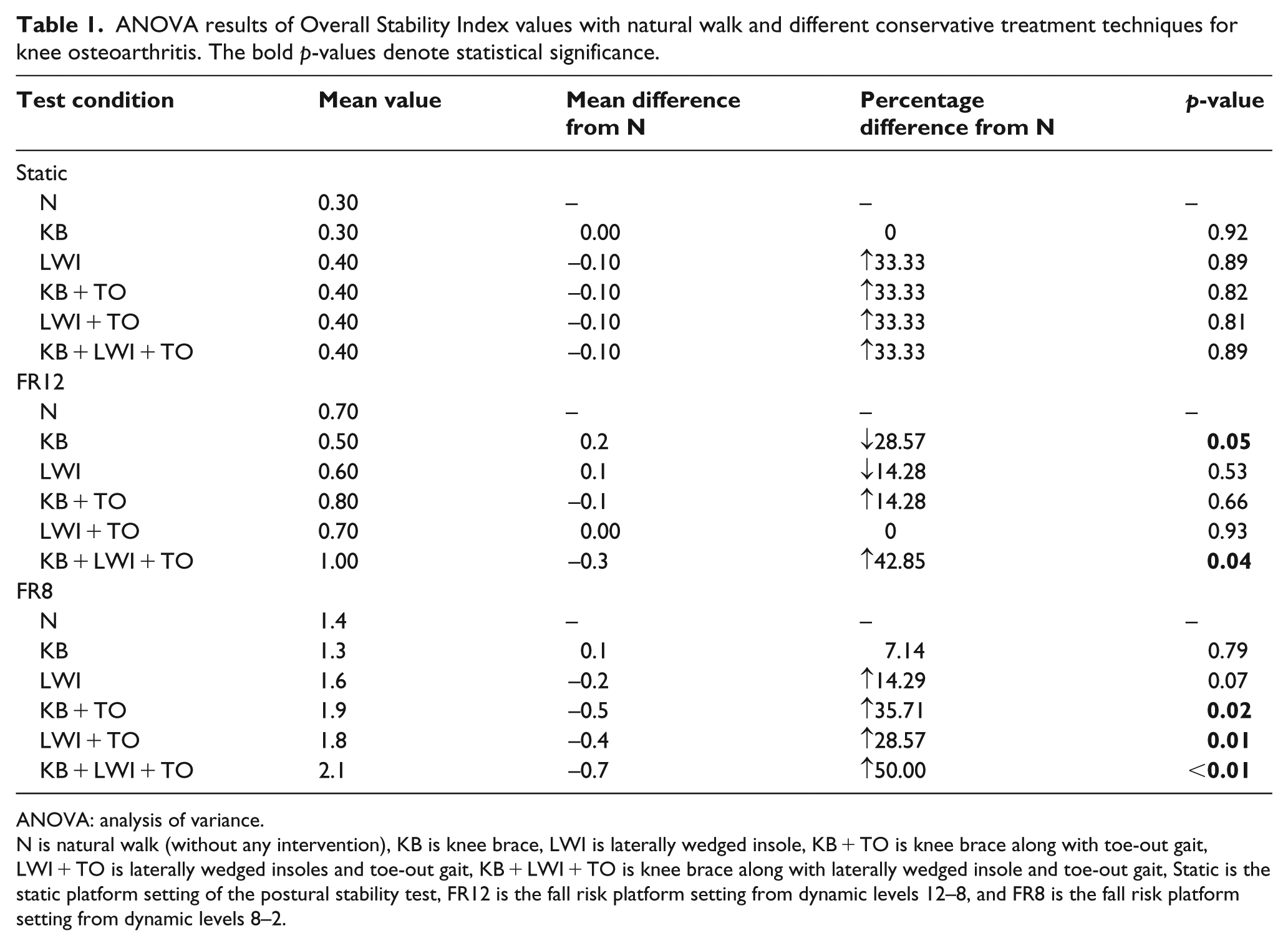
ANOVA: analysis of variance.
N is natural walk (without any intervention), KB is knee brace, LWI is laterally wedged insole, KB + TO is knee brace along with toe-out gait, LWI + TO is laterally wedged insoles and toe-out gait, KB + LWI + TO is knee brace along with laterally wedged insole and toe-out gait, Static is the static platform setting of the postural stability test, FR12 is the fall risk platform setting from dynamic levels 12–8, and FR8 is the fall risk platform setting from dynamic levels 8–2.
Level of comfort
The comfort level of the participants was assessed using Wong–Baker questionnaire, and the results are shown in Figure 4. Significant reductions the in the pain score were observed from N (1.8) for KB (6.4, p < 0.01), KB + TO (7.8, p < 0.01), LWI + TO (3.4, p = 0.01), and KB + LWI + TO (8.1, p < 0.01). LWI showed no effect on the pain score (1.9, p = 0.29).
Discussion
The objective of this study was to test the combined effect of orthoses with TO on KAM and fall risk of medial kOA patients. We also evaluated the participants’ comfort level while using the interventions individually and combined. Walking with the brace alone, resulted in no significant change in peak KAM values. Previous studies have reported significant reductions in both peaks of KAM.33,53 The comparatively smaller and insignificant reductions in peak KAM values by KB might be due to the immediate testing of the intervention, without having any follow-up duration. The insoles, when used individually, reduced the first and the second peaks of KAM by 6.0% and 9.5%, respectively. The reductions, however, are very small as compared to those previously reported,34,54,55 probably because of the effect of different walking speeds. We limited our participants’ gait speed to 1.18 m/s, as per our pilot study, which was lower than the gait speed of previous studies.
The combination of LWI and TO provided similar results as of Tokunaga et al. 18 Toeing out reduced the KAM further during the whole stance phase, when combined with brace and insole simultaneously. The present findings support the concept of combining orthoses with TO specially to reduce sKAM. The study is novel in this nature as it provides insight of the combined effects of three conservative treatments. Previously, KB and LWI have been studied in synchronicity. Schmalz et al. 53 reported changes in KAM during walking with combined use of a wedged insole and rigid foot orthoses in healthy participants. Further extending their work, Hunter et al. 56 tested the combined behavior of valgus brace, customized foot orthoses, and specialized shoes in a randomized cross-over study. They found the combination of these treatment techniques to be further improving knee pain than the control treatment of neutral brace, neutral orthoses, and motion control shoes.
The present results are consistent with the studies which suggest that the combined use of conservative treatments may reduce greater loads than if used individually for medial kOA patients. In our case, TO is very useful in reducing late stance KAM when combined with KB and LWI. Although results are showing a significant reduction in early stance KAM also, which is contradictory to the previous studies showing no change or increase in the fKAM with TO. The reduction in fKAM in this study was due to the use of LWI, not TO. But, it seems important that both KB and LWI limit the movement of CoP by toeing out, which in turn leads to no change in fKAM by TO. The largest change in combining orthoses and TO occurred at sKAM (25.5%), which was 22.4% higher than KB alone and 15.85% higher than LWI alone. This reduction in sKAM might be considered disappointing given that three interventions were combined. Arguably, these smaller changes may have profound effect on disease progression as walking is one of the most frequent ADL.8,57
Toeing out shifts the CoP medially, shifting the line of action medial to the AP axis of the shank. This shifting of the CoP and the line of action produces a torque about the talocrural joint and forces the knee joint center to move laterally. This effect is counteracted by the external rotation of tibia in the transverse plane, which decreases the perpendicular distance of the GRF vector (GRF lever arm) and the knee joint center. The reduced GRF magnitude and the GRF lever arm results in a decrease in early stance KAM. As for the late stance phase, toeing out shifts the CoP externally, resulting a decrease in KAM.24,58,59
Postural stability is not affected by slight perturbations under normal conditions, despite the non-uniform load distribution across the body. 60 This can be changed, however, by several external (injury to the head, vestibular apparatus, and limbs) and internal factors (chronic vertigo, visual impairment, etc.). An alteration in the body posture, intended as a treatment option for any disorder, should be carefully devised such that it does not decrease the postural stability of the patient. Our results showed that the balance of kOA patients can be compromised when two or more than two conservative treatments are combined with TO on unstable platforms. This balance reduction was also reflected in the participants’ comfort level questionnaires where the most uncomfortable situation for them was walking with three interventions simultaneously.
A limitation of the study can be that we provided the brace to the patients for very short period of time and did not have any follow-ups. We did not prioritize a follow-up session, since our objective was not to test the efficiency of KB alone, but to test synergistic effects of immediate application of conservative treatments.
Conclusion
There is a synergistic effect of toe out when combined with KB and LWI concurrently in sKAM reduction, but with greater degree of fall risk. Simultaneous use of conservative treatments also decreases comfort level. However, these results do lend support to future works investigating potential additive effects of combined interventions tailored to ensure patient comfort.
Footnotes
Author contribution
S.J.K., S.S.K., J.U., A.H.M., and N.A.A.O. contributed to study design and manuscript drafting and review; S.J.K. and S.S.K. contributed to conducting the experiment and data processing; S.J.K. and A.H.M. contributed to participant recruitment; and J.U. and N.A.A.O. contributed to resource provision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Postgraduate Research Grant (PPP; grant/award number: PG072-2015B) and University of Malaya Research Grant (UMRG) (grant/award number: RP-020C-13AET).
Informed consent
Informed consent was obtained from all individual participants included in the study.