
Abstract
Background:
The devastating earthquake in Sichuan in 2008 has left many adolescent amputees. However, little research has been focused on the adolescent amputees who have high potential to return to premorbid activity level.
Objectives:
To investigate daily step activities and prosthesis-related quality of life of the adolescent transtibial and transfemoral amputees after the earthquake.
Study design:
A prospective and descriptive study.
Methods:
A total of 21 adolescent unilateral amputees (11 transtibial and 10 transfemoral amputees) were recruited. Step Activity Monitors and Prosthesis Evaluation Questionnaire were used to assess patients over a 3-month period.
Results:
The average number of steps per day was 4577 ± 849 and 2551 ± 693 in transtibial and transfemoral amputees, respectively. Transtibial amputees had significantly higher (p < 0.05) levels of step activity than transfemoral amputees in all Step Activity Monitors measures. Prosthetic compliance was good with daily wearing time of above 12 h/day in both groups. Prosthesis Evaluation Questionnaire scores showed no significant difference between two groups.
Conclusions:
The subjective quality of life is similar for adolescent amputees across transtibial and transfemoral amputation levels. Higher levels of step activity of transtibial amputees suggest that they have had lower energy expenditure and more capacity for ambulation.
Clinical relevance
This article involves a unique subset of young amputees who have sustained traumatic amputations following a major natural disaster. It provides a better understanding on the daily activities and quality of life, and could assist in optimizing the prosthetic outcomes of this subset of populations.
Background
The World Health Organization (WHO) defines adolescents as people aged between 10 and 19 years who have specific health and development needs. 1 Many of them are facing challenges, including a lack of access to health information and physical activity. Adolescent lower limb amputees require more attention than the able-bodied group as they have more extensive disability. During the 2008 Sichuan earthquake, many victims were school children in this age group who suffered from lower limb amputations as a result of trauma-related injuries at different levels in order to preserve their lives.
Lower limb amputations impose energy penalties for ambulation, and amputees with higher amputation levels consume more energy. 2 To gain insight into the physical activity and prosthesis-related quality of life of adolescents with lower limb amputations, methods such as questionnaires, interviews, and diaries are used. 3 Studies have also been performed in laboratory settings to measure oxygen consumption, heart rate, walking speed, and gait pattern.4,5 However, research conducted in a laboratory setting is a controlled environment that is not representative of the real-world function and activity of the amputee patients. For adolescents, it is important to have adequate physical activities for long-term health benefits and good quality of life, as the level of childhood physical activity is associated with the general level of physical activity in adulthood. 6 An investigation on adolescent amputees’ daily activities and quality of life could demonstrate the role that step activity plays on prosthesis-related quality of life for groups of transtibial and transfemoral amputation level.
Real-life step activity can be measured by electronic step counters such as Step Activity Monitor (SAM) and ActivePAL physical activity logger.7,8 These devices are small and can be worn on the waist and ankle with Velcro straps. They are designed to measure and store measurements of the intensity, frequency, pattern, and duration of activity. The validity and reliability have been well tested.8,9 Several studies used electronic step counters to monitor the daily activities of lower limb amputees with the mean age of 54–60 years, and found that the average total number of steps were between 2657 and 3218, spending 1.9–4.7 h on low to high activity levels per day.10–13
There was no consensus on the most appropriate measures to assess the prosthesis-related quality of life for the lower limb amputees. Generic instruments like the Short Form-36 (SF-36) and Sickness Impact Profile (SIP) are not specifically designed for amputees and may appear to have some weaknesses. 14 It is suggested to use some amputee-specific measures such as Prosthesis Evaluation Questionnaire (PEQ), Prosthetic Profile of the Amputee and Houghton scale, which have been shown to be valid and reliable tools for this group of patients.15–17 Previous studies found that the mean PEQ score out of 100 of lower limb amputees was between 64.5 and 76.1 with a mean age of 43–66 years,18–21 but there was no significant difference among different amputation levels in PEQ scores in terms of prosthesis-related quality of life. 19 Research has been conducted to address the quality of life of lower limb amputees over time. MacKenzie et al. 22 compared the quality of life of traumatic amputees (18–69 years old) between 2 and 7 years after amputation by using SIP. This was a long-term prospective study and found that the quality of life was becoming poorer over time. However, in another study, Zidarov et al. 23 reported that the quality of life remained stable over a 3-month period by analyzing three outcome measures, including Subjective Quality of Life Profile (SQLP), PEQ, and Amputee Body Image Scale (ABIS).
It is well known that transfemoral amputees (TFAs) consume more energy during walking than transtibial amputees (TTAs);2,4 however, the consequences resulting in daily activity and quality of life have never been tested especially for adolescent amputees. Additionally, the published data on step activity and prosthesis-related quality of life only represent data from older amputee populations. There is a need for more information about the step activity and prosthesis-related quality of life of adolescent TTAs and TFAs. Therefore, the purpose in this study was to investigate in what extent adolescents with a transfemoral amputation resulting from the natural disaster have lower levels of activity than those with a transtibial amputation, and to explore differences in prosthesis-related quality of life by using amputee-specific outcome measures.
Methods
Ethical approval was obtained from the Ethical Committee on Research Involving Human Subjects of the institution. As the main aim of the study was to investigate the prosthetic outcomes of adolescent amputees after the earthquake, the inclusive criteria were as follows:
Amputation secondary to the Sichuan earthquake in 2008;24,25
Lower limb amputees who have K2 activity level or above; 26
Use of prosthesis for at least 6 months;
Age from 10 to 19 years.
All the subjects were recruited in a local rehabilitation center which served the victims of the Sichuan earthquake from March 2011 to December 2012. All of them had gone through the complete multidisciplinary rehabilitation, including orthopedics, nursing, prosthetics, physiotherapy, occupational therapy, social work services, and clinical psychology.
The amputee subjects were divided into two groups based on transfemoral and transtibial amputation levels. All subjects completed the PEQ 15 for the assessment of prosthesis-related quality of life and the SAM 7 was installed to their prostheses. Written informed consent was received from all participants before the study began. For the subjects who were under 16 years old, written consent from their parent or guardian was required to take part in the study (data collection).
Equipment
The SAM 7 (StepWatch; Orthocare Innovations, Seattle, USA) is an electronic step counter that is a performance-based prosthetic outcome assessment instrument. It detects and counts steps for a wide variety of gait styles, ranging from a slow shuffle to a fast run. It can detect the level of physical activities, which can be divided into three groups: low (<15 steps/min), medium (15–40 steps/min), and high (>40 steps/min). Additionally, the SAM records additional measures that describe step activity including time spent in different activity levels per day, peak activity index (average steps/min of the most intensive 30 individual minutes in the day), endurance score (average steps/min of the most intensive continuous 60 min in the day), cardiovascular score (average steps per minute of the most intensive continuous 20 min in the day), peak 5-min burst (average steps per minute of the most intensive continuous 5 min in the day), and peak 1-min burst (peak steps per minute in the day).
The monitor is programmed and downloaded with a standard computer through a docking station that plugs into a USB port. The SAM and docking station communicate through an infrared link that allows the SAM to be completely sealed and impervious to tampering. The SAM was installed onto the prosthesis at the beginning of the research. Subjects were asked to attend a follow-up every month and data were downloaded in every follow-up visit. The investigation came to completion after three follow-up visits.
PEQ 15 is a self-report visual analog scale (VAS)-style questionnaire (100-mm line). It consists of 82 items with nine functional domain scales including (1) ambulation, (2) residual limb health, (3) utility, (4) appearance, (5) sounds, (6) frustration, (7) perceived response, (8) social burden, and (9) well-being. The PEQ also contains items beyond the subscales including satisfaction, pain, transfers, prosthetic care, self-efficacy, and importance.
The PEQ is an amputee-specific outcome measure which has been shown to be valid and reliable tools for this group of patients.15,19 The PEQ is the only amputee-specific outcome measure that has a Chinese version. Therefore, it is the most appropriate and convenient instrument for this study. The questionnaire used in this study was an adaptation that used in the version translated in 2004 for Hong Kong amputees which was tested to be valid and reliable. 18 Simplified Chinese characters were adopted instead of traditional Chinese characters.
In order to reduce the outcome affected by the prosthesis, same prosthetic components and suspension type were used in all subjects. Dynamic response foot (Flex-Foot Assure; Ossur, Iceland) was used in all subjects as it was advised for amputees to achieve a higher activity level. 27 The suspension system used in transtibial subjects was patella tendon bearing socket with supracondylar suspensions. Transfemoral subjects were fit with polycentric knee with hydraulic swing control (Total Knee 2000; Ossur, Iceland). In order to maximize the prosthetic function, the suspension system used in transfemoral subjects was “suction” suspension as to provide a secure external attachment to the residual limb and improve the control of the prosthesis. 28
Procedure
The socket was fit and aligned by a certified prosthetist, without any complaints from the subject and with minimal observatory gait deviations. During the initial fitting of SAM, body height of the participants was measured in order to provide data required for the software to start the SAM. At every 4-week follow-up appointment, the subjects were evaluated by a certified prosthetist to ensure the fit of the socket and assess the condition of the residual limb. The SAM recording was downloaded before being re-installed on the prosthesis, and the PEQ was filled by the subjects at each visit (Figures 1 and 2). The data collection period of each subject lasted for 3 months. At the end of the study, three data points of SAM and PEQ were collected for analysis.

A SAM is installed on the ankle of the prosthetic side of a transtibial subject.

A subject is filling the PEQ.
Data analysis
Statistical analysis was conducted by SPSS 17.0 (IBM Corporation, New York, USA) and the α-level was set at 0.05. Independent t-tests were conducted to compare the mean values of PEQ subscale scores between adolescent TTAs and TFAs. The same test was done to compare the mean values of each SAM parameter between two groups. One-way analysis of variance (ANOVA) for repeated measures was conducted to compare the differences in PEQ subscale scores and parameters measured with SAM across the three follow-up appointments. Data were reported as means ± standard deviations (SDs).
Results
A total of 25 amputee subjects were recruited in the beginning of the study. Four TFA subjects dropped out from the research due to personal reasons. The demographic data of the remaining 21 amputee subjects (11 TTAs and 10 TFAs) are shown in Table 1.
The demographic data according to the amputation level.
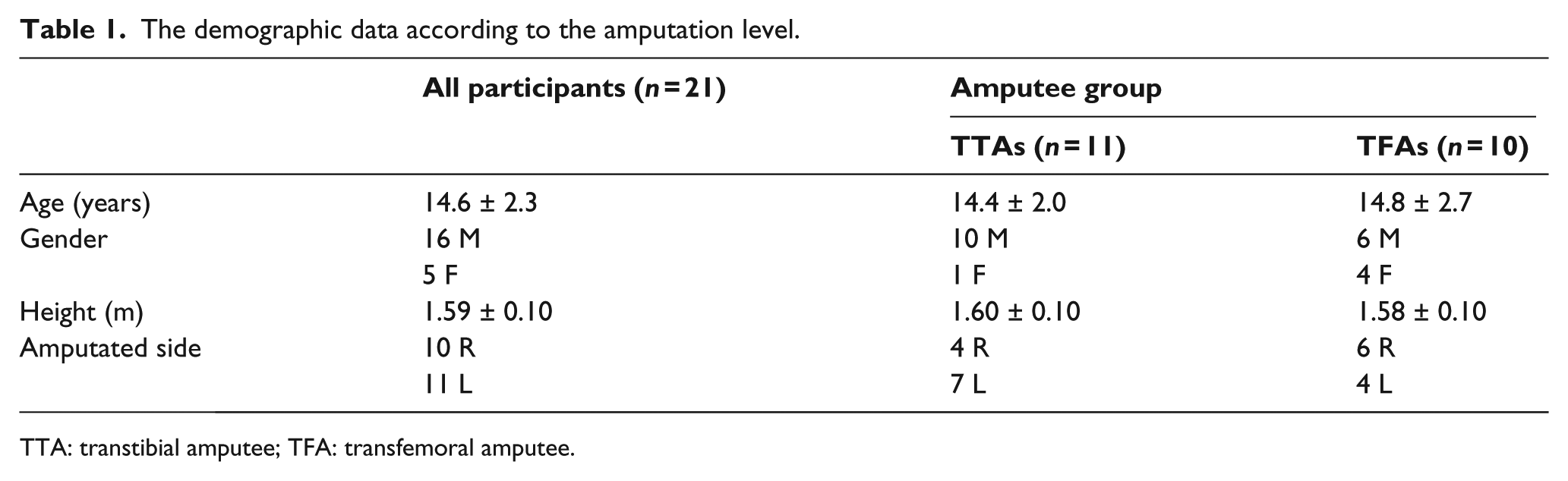
TTA: transtibial amputee; TFA: transfemoral amputee.
Samples of step activity data are illustrated in Figures 3 and 4. Significant differences were found in all SAM parameters between adolescent TTAs and TFAs (p < 0.05). TTAs were more active than TFAs in terms of SAM data including total number of steps, time spent on low (<15 steps/min), medium (15–40 steps/min), and high (>40 steps/min) activity levels, peak activity index (average steps and minute of the most intensive 30 individual minutes in the day), endurance score (average steps per minute of the most intensive continuous 60 min in the day), cardiovascular score (average steps per minute of the most intensive continuous 20 min in the day), peak 5-min burst (average steps per minute of the most intensive continuous 5 min in the day), and peak 1-min burst (peak steps/minute in the day). No significant difference was detected in terms PEQ scores (Table 2). No significant differences were found across the different follow-up appointment time points in either SAM or the PEQ data using the one-way repeated-measures ANOVA.
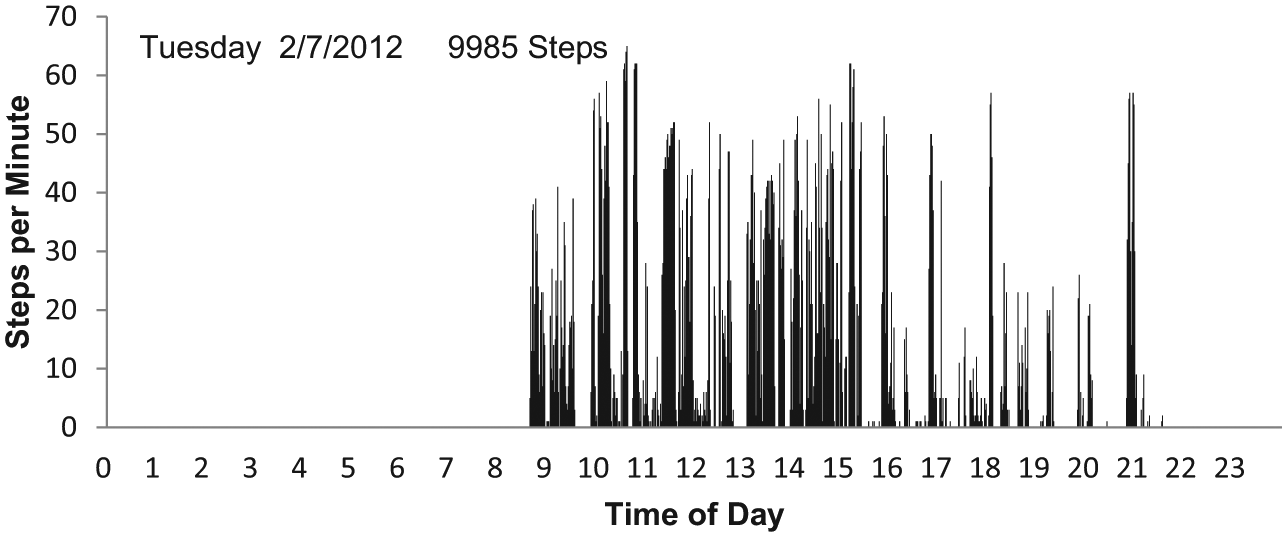
One day of step activity data of a transtibial subject.
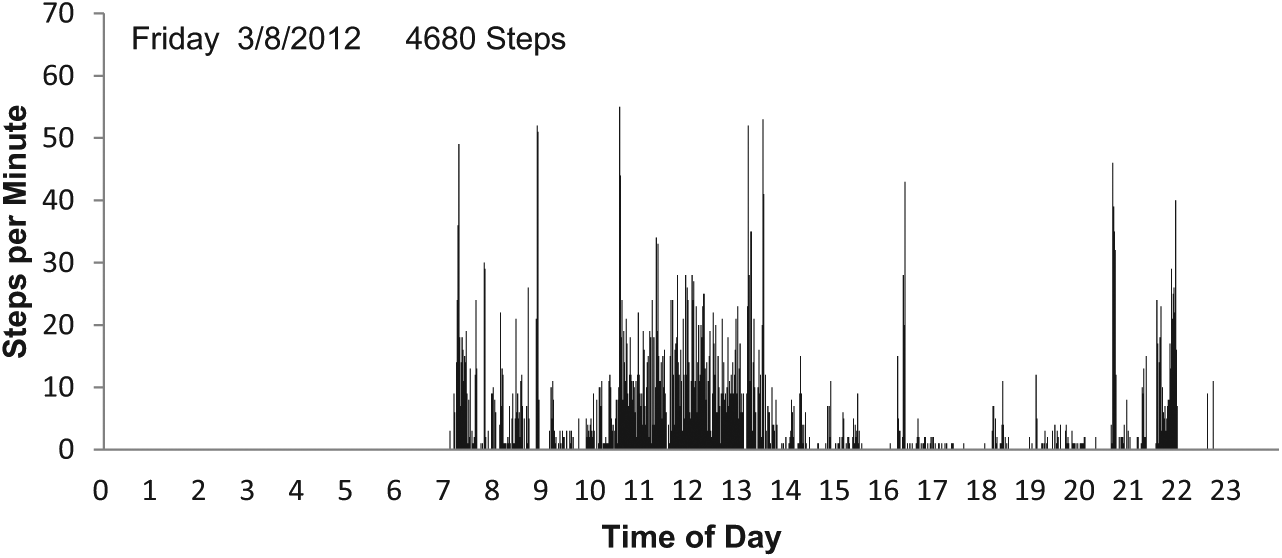
One day of step activity data of a transfemoral subject.
Rehabilitation outcomes between adolescent TTAs and TFAs. Significant difference was found in all SAM parameters but not PEQ scores.
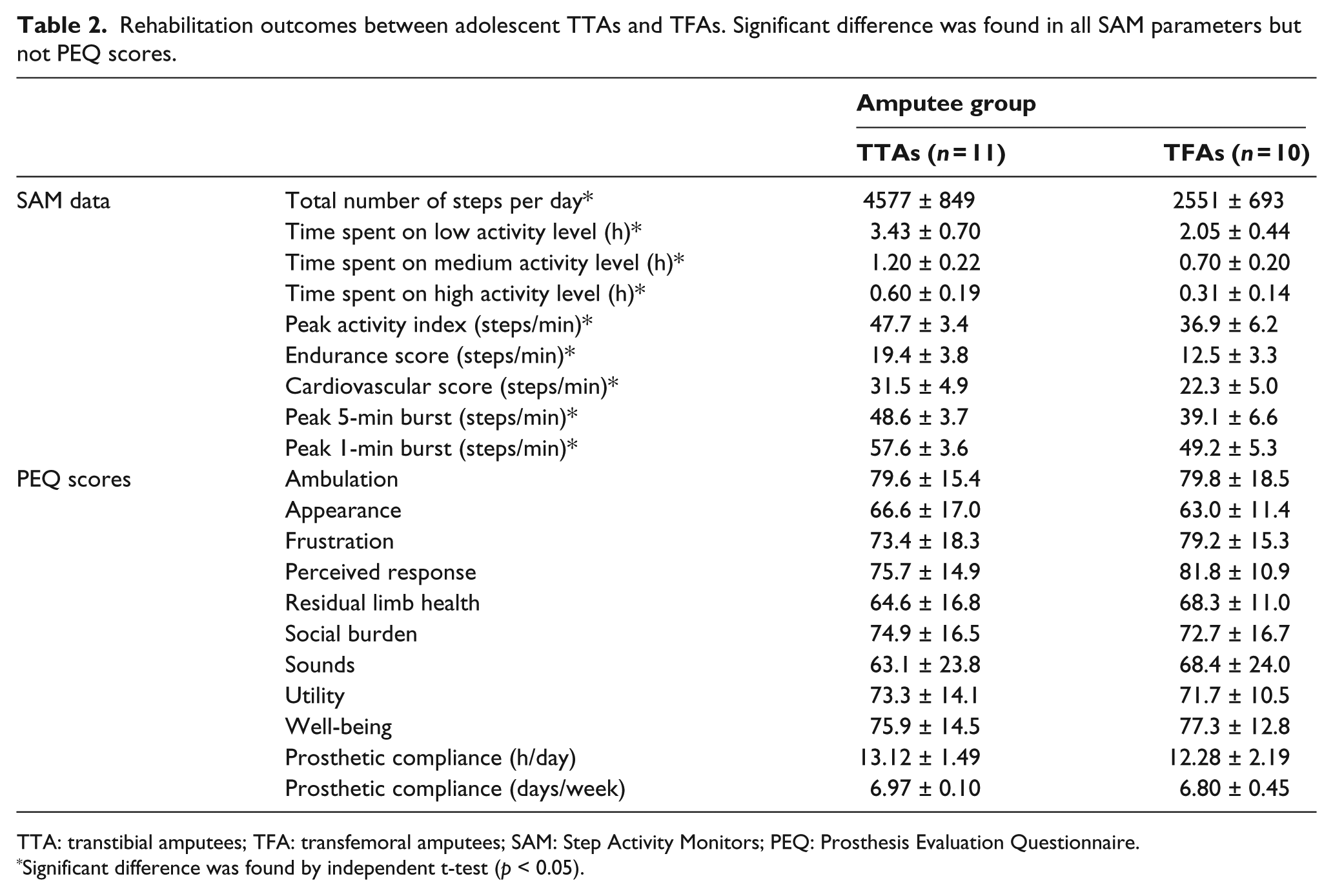
TTA: transtibial amputees; TFA: transfemoral amputees; SAM: Step Activity Monitors; PEQ: Prosthesis Evaluation Questionnaire.
Significant difference was found by independent t-test (p < 0.05).
Discussion
Adolescent TFAs walked significantly less than TTAs, and their daily activities were 56% of TTAs in terms of total steps per day. When compared with able-bodied adolescents from a previous study, the daily activities of adolescent TTAs and TFAs were 90% and 50%, respectively, in terms of total steps per day. 29 TFAs also spent less time on different activity levels than TTAs, indicating they spent more time sitting and standing. The same phenomenon was found in other SAM results, including peak activity index, endurance score, cardiovascular score, peak 5-min burst, and peak 1-min burst. This result agrees with previous studies and supports the hypothesis that adolescents with a transfemoral amputation after the natural disaster are less active than transtibial group. TFAs are shown to consume more energy during walking,2,4 and this study showed that adolescent TFAs are also less active than adolescent TTAs in everyday life.
The average daily step activity of adolescent amputees from this study was 3612 steps with 4.2 h on low to high activity levels, which was relatively high compared to other amputees group from the literature. The step activity found in previous studies in older lower limb amputees with the mean age of 54–60 years was between 2657 and 3218 steps per day, spending 1.9–4.7 h on low to high-activity levels per day.10–13 This confirms that young traumatic amputees have a higher mobility compared to older amputees. Previous studies also verify that a younger amputee walks with a higher self-selected walking speed but lower rate of oxygen consumption than an old amputee due to higher exercise capacity.30,4
The results of this study showed that there was no significant difference in any of the nine domains of PEQ scores between the transtibial and transfemoral subjects. This suggested that both groups have similar prosthesis-related quality of life, in terms of patients’ perspectives, even though this study showed that adolescent TFAs were less active than TTAs. Legro et al. 19 also found no significant difference among different amputation levels in PEQ scores. Previous studies found that the mean PEQ score was between 64.5 and 76.1 with a mean age of 43–66 years.18–21 The mean PEQ score of this study was 72.7, which was within the range of previously reported values of prosthesis-related quality of life from older populations. Although the population in this study was much closer in age (10–19 years old) than the population in the previous study (43–66 years old) and they were much younger and had higher step activity than older populations found in the literature, the comparable PEQ results suggest that the age may not be a dominant factor affecting amputee’s prosthesis-related quality of life.
The result from this study showed no significant difference in both daily activities and prosthesis-related quality of life of the PEQ scores over a 3-month period, which was similar to the research done by Zidarov et al., 23 who reported that amputees’ prosthesis-related quality of life remained stable over a 3-month period by analyzing three outcome measures, including SQLP, PEQ, and ABIS. However, in another study, MacKenzie et al. 22 conducted a long-term prospective study and found that the quality of life of traumatic amputees (18–69 years old) was becoming poorer over time between 2 and 7 years after amputation by using SIP. The diverging results from MacKenzie et al. can be due to the aging effect as it is well known that the physical functioning worsens with age in general. 22 The other possible reason is that the SIP and PEQ measure different constructs, one the impact of sickness on quality of life and the other measuring prosthesis-related quality of life. It could be that SIP decreases over 2 and 7 years for older amputees, while the PEQ remains constant for that same population. A longer testing period would be necessary to see if prosthesis-related quality of life remains constant over longer periods of time.
This study has some potential limitations, of which its relatively small sample size (n = 21) is the first. The subjects were recruited by a convenience sample from a list of existing clients rather than stratifying the recruiting to randomly select a representative proportion of amputation lengths, genders, or ages. Additionally, all subjects recruited in this study are Chinese who live in Sichuan province, and cannot be generalized to the whole Chinese amputee population as people have different living habits in different provinces.
Conclusion
This study describes the step activity and prosthesis-related quality of life of adolescent prosthetic users over 3 months, and the results confirm the hypothesis that adolescents with a transfemoral amputation after the natural disaster are less active than transtibial group. The results indicate that the perceived prosthesis-related quality of life was similar in both groups, and support that adolescent amputees are able to achieve a step activity that is similar to able-bodied populations. This article establishes how active this unique adolescent amputee population is. It also demonstrates that this group has a high demand for prosthetic technology which supports this population to make the increased activity level and prosthesis-related quality of life possible in the future.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.