
Abstract
Background:
The functional performance of currently available body-powered prostheses is unknown.
Objective:
The goal of this study was to objectively assess and compare the functional performance of three commonly used body-powered upper limb terminal devices.
Study design:
Experimental trial.
Methods:
A total of 21 able-bodied subjects (n = 21, age = 22 ± 2) tested three different terminal devices: TRS voluntary closing Hook Grip 2S, Otto Bock voluntary opening hand and Hosmer Model 5XA hook, using a prosthesis simulator. All subjects used each terminal device nine times in two functional tests: the Nine-Hole Peg Test and the Box and Blocks Test.
Results:
Significant differences were found between the different terminal devices and their scores on the Nine-Hole Peg Test and the Box and Blocks Test. The Hosmer hook scored best in both tests. The TRS Hook Grip 2S scored second best. The Otto Bock hand showed the lowest scores.
Conclusion:
This study is a first step in the comparison of functional performances of body-powered prostheses. The data can be used as a reference value, to assess the performance of a terminal device or an amputee.
Clinical relevance
The measured scores enable the comparison of the performance of a prosthesis user and his or her terminal device relative to standard scores.
Keywords
Background
The body-powered (BP) prosthesis and the myoelectric (MYO) prosthesis are commonly used devices for paediatric and adult upper limb amputees.1 –3 In a study by Kruger and Fishman, 120 transradial child amputees compared cosmetically identical MYO and BP hands. After wearing each for 3 months, 78% chose the MYO and 22% chose the BP. At 2-year follow-up however, only 44% wore the MYO, 33% used a BP hand or hook, and 23% became non-wearers. Active BP wearers were clearly most pleased with the features of their prostheses. 2 Still rejection rates of upper limb prostheses are high. 4 Various studies focus on the cause of the abandonment and on the use of the prostheses.3,5 –7 There has been little attention, however, on the objective measurement of the performance of the prostheses. A couple of studies measured the mechanical performance of currently available BP voluntary opening (VO) and voluntary closing (VC) hands and hooks.8,9 Quantitative studies measuring functional performance are scarce. Some studies10,11 used the Southampton Hand Assessment Procedure (SHAP) to assess MYO upper limb prostheses.10,11 The SHAP is a clinically validated hand function test, developed to assess the effectiveness of upper limb prostheses. 12 It takes about 30–45 min to complete the test. Some other studies used the Box and Blocks Test (BBT) and the Nine-Hole Peg Test (NHPT) to assess upper limb prostheses.13,14 The BBT and the NHPT were developed to measure manual dexterity. It takes about 1–3 min to complete a BBT or a NHPT. Because these tests take a short time to administer, they can be administered multiple times without imposing a burden on the test subject. Our study assesses the functional performance of three currently available BP hooks and hands, by using the BBT and NHPT. The scores can serve as reference values to assess the functional performance of patients and of new developed terminal devices.
Goal
The goal of this study was to quantitatively measure and compare the functional performance of three commonly used BP upper limb terminal devices.
Methods
Subjects
A total of 10 men and 11 women (sample of convenience), all able-bodied subjects 20–24 years old (mean age ± standard deviation (SD): 22 ± 1), participated. All subjects were right handed and did not have any experience in controlling a prosthesis. Given the limited availability of upper limb amputees, the authors chose to use able-bodied subjects. A study by Schabowsky et al. 14 showed that the learning capabilities of motor tasks by amputees were similar to those of able-bodied subjects. A second advantage of using able-bodied subjects is the level of experience, which is the same for all subjects, whereas generally prosthetic users have different levels of experience in prosthesis control. Ethical approval for this study was obtained from the institutional ethical committee. Before the test started, the test procedure was explained to the subject and informed consent was acquired from the subject.
Materials
Prosthesis simulator
A prosthesis simulator (S in Figure 1) was attached to the left arm of the test subject. It allowed a healthy subject to operate a terminal device (TD). The terminal device was placed at the non-dominant arm (left side) of the subject, as for amputees the side of the amputation usually is, or becomes, the non-dominant side. The terminal device was attached to the simulator, by using the Otto Bock 10V30 Wrist. The terminal device was placed aside of the hand to prevent the length of the arm becoming too long. A figure-of-nine shoulder harness (SH) and a Bowden cable enabled the subject to open or close the terminal device. The SH could be adjusted by Velcro. A triceps pad placed 10 cm above the elbow was used to guide the control cable to the back.
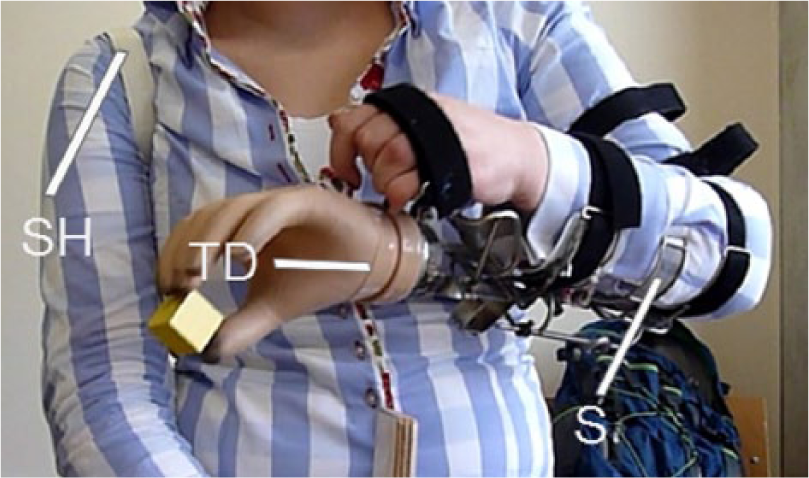
Terminal device (TD) connected to the simulator (S). A Bowden cable connects the shoulder harness (SH) to the terminal device, enabling the subject to control the terminal device.
Terminal devices
The tested terminal devices are shown in Table 1 and Figure 2: Hosmer model 5X hook, TRS VC Hook Grip 2S and Otto Bock VO Hand.15 –17 The devices are commercially available terminal devices. No alterations were made to the devices. The mean pinch force of the Otto Bock hand lies between 9 and 12 N. 8 One elastic band was applied to the Hosmer hook (instead of two or more) to provide the pinch force. One elastic band provides a pinch force of 9 N. Two bands would yield a pinch force of 20 N, which is more than the pinch force of the Otto Bock VO Hand. Therefore, one band was applied. The TRS Grip 2S hook is a VC hook, so the pinch force is delivered by the user instead of by a spring. The chosen terminal devices are commonly used in clinical practice. The Otto Bock VO hand is a commonly used hand and requires the second lowest activation force or cable force compared to other VO hands. 8 Of the VO hooks, the Hosmer model 5XA hook requires the lowest activation force. The TRS Grip hook 2S requires the lowest activation force of the VC devices. 9 VC devices have some benefits over VO devices:18,19 The force to control a VC terminal device is low and the user is able to accurately control the pinch force. VC terminal devices, however, do have some drawbacks: To hold an object, the user has to maintain the tension in the cable, or instead the user has to activate a locking mechanism. Compared to VC devices, VO devices have their own benefits: 18 Once holding an object, no cable force is required because the spring delivers the pinch force. VO terminal devices also have some drawbacks: The maximum pinch force is determined by the closing spring. Opening the terminal devices always requires the maximum activation force, even if the required pinch force is low.
Properties of the tested terminal devices.
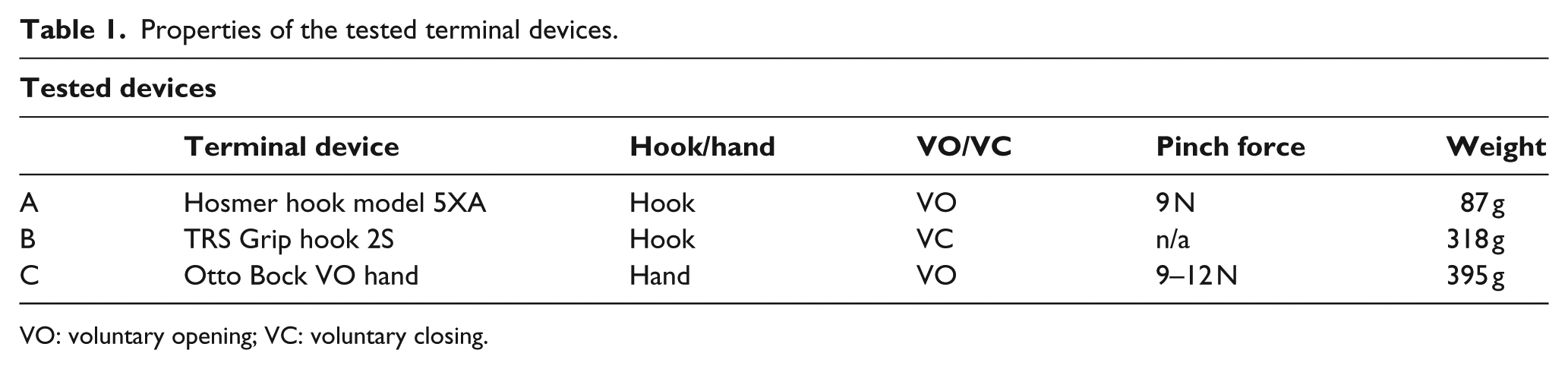
VO: voluntary opening; VC: voluntary closing.

Terminal devices: (a) Hosmer hook (VO), (b) TRS grip hook (VC) and (c) Otto Bock hand (VO).
Measurement tools
The functional performance was tested by using two short tests. The first test was the BBT (shown in Figure 3), a test of manual dexterity for occupational therapists and others to evaluate hand function. 20 The BBT consists of a box with a centre partition. Small wooden blocks were placed in one side of the box. The other side of the partition was empty. The participant was asked to pick up blocks, one at a time, and drop them at the other side of the partition. The participant had to perform the test by using the simulator with the terminal device. After 60 s, the trial was ended. The score of the BBT was represented by the number of blocks transported in 60 s.

Box and Blocks Test.
The second test which the participants had to perform was the NHPT (shown in Figure 4). The NHPT is commonly used by occupational therapists as a quick measurement of finger dexterity. 20 The participant had to pick up the pegs one at a time, using the terminal device only and put the pegs into the holes in any order, until all holes were filled. Subsequently, the participant had to remove the pegs one at a time and return them to the container. The duration of the test was measured and expressed in seconds per peg movement (s/peg.). There are 18 peg movements in total: 9 peg placements and 9 peg removals. The maximum allotted time was 90 s. After 90 s, the test was cut-off, to prevent the subject from getting tired or demotivated. Running the test longer will not provide much useful information. The scores of the cut-off test were also expressed in s/peg, by dividing the 90 s by the number of successful peg displacements. This enables the inclusion of the test results of the unfinished trials. Results of other studies can be expressed in s/peg by dividing the recorded time of a finished trial by 18 peg displacements.

Nine-Hole Peg Test.
Test protocol
All subjects had to control three BP terminal devices with their left arm. They participated at three different days, to investigate the presence of a learning curve. Each day the participant had to use each terminal device to complete three trials of both functional tests (the BBT and the NHPT). So in total, both tests were repeated nine times per terminal device (3 days × 3 trials). All trials were completed within a 3-week period. The sequence in which the devices were tested by a subject during one trial was randomized in order to minimize mutual influences. The sequence was randomized in such a way that each sequence occurred an equal amount of times during the study. This was important because two of the terminal devices were VO and one was VC (TRS Grip 2S). The participant had to get used to a different control mode after changing the terminal device.
Every time a new subject participated, the instructions were explained before the test started. Both tests were completed in a sitting position. All subjects started with the BBT. As the NHPT takes more effort to complete than the BBT, the BBT is expected to have less influence on the NHPT than the other way around. Before starting the BBT, the subjects were given the opportunity to practise for maximal 1 min, adjust their stool height and pronate or supinate their terminal device. All terminal devices could pronate and supinate around their wrist axis. The subjects were given only 1 min to practise to be able to measure the learning curve from the early start. In order to give the subjects an equal start in the BBT, in each new trial the blocks were randomly deposited in the left partition, with six blocks on the top layer. This prevents the first layer of being packed too closely. Before starting with the NHPT, the participant was allowed to practise (1 min. maximum), adjust the stool and adjust the terminal device again. To determine whether there were significant differences between scores of the three terminal devices and between the scores of the nine mutual trials, a repeated measures two-way analysis of variance (ANOVA) was performed. As each terminal device was used in each trial, by each subject, the ANOVA contained two ‘within-subject factors’: the trials and the terminal devices. The ANOVA has been performed twice: once for the NHPT and once for the BBT. To determine whether there were significant differences between the scores of male and female subjects, a t-test was performed. All results were considered to be significantly different when p ≤ 0.05.
Results
BBT
The BBT scores over the nine trials of the 21 subjects are shown in Figure 5(a) to (c). The interquartile range (IQR) values did not decrease during the tests. A significant difference was found between the different terminal devices based on the amount of blocks scored in the BBT (F = 198.640; degree of freedom (df) = 2; p < 0.001). A significant difference was found within the nine mutual trials (F = 104.864; df = 4.288; p < 0.001). The BBT scores increased over time, which means that the subjects got faster in transferring blocks. No significant differences were found between males and females (Otto Bock: p = 0.82, TRS Grip: p = 0.31, Hosmer: p = 0.23).
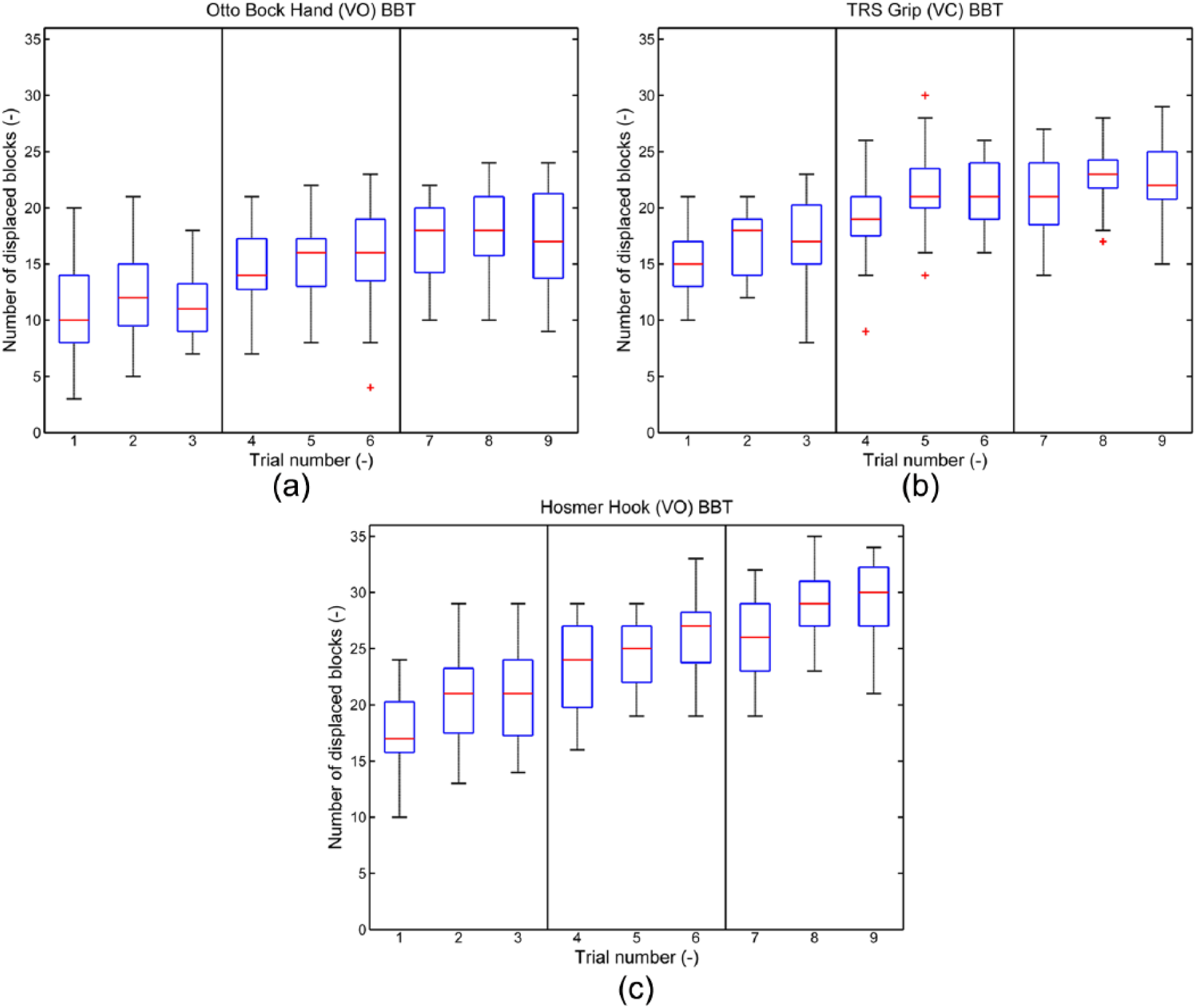
(a) Scores of the Otto Bock Hand during the BBT (n = 21), during nine trials at three different days. (b) Scores of the TRS Grip hook during the BBT (n = 21), during nine trials at three different days. (c) Scores of the Hosmer hook during the BBT (n = 21), during nine trials at three different days.
NHPT
The NHPT scores of the 21 subjects over the nine trials are shown in Figure 6(a) to (c). The scores are expressed in s/peg. The IQR values decreased during the tests. Significant differences were found between the different terminal devices based on the NHPT scores (F = 116.253; df = 1.048; p < 0.001). Figure 6(a) to (c) shows that the scores decreased over time, which means that subjects got faster in transferring pegs in and out the pegboard. The significant difference that was found between the nine trials proves that the scores vary over time (F = 14.308; df = 8; p < 0.001). No significant differences were found in the NHPT between male and female subjects (Otto Bock: p = 0.14, TRS Grip: p = 0.13, Hosmer: p = 0.08).
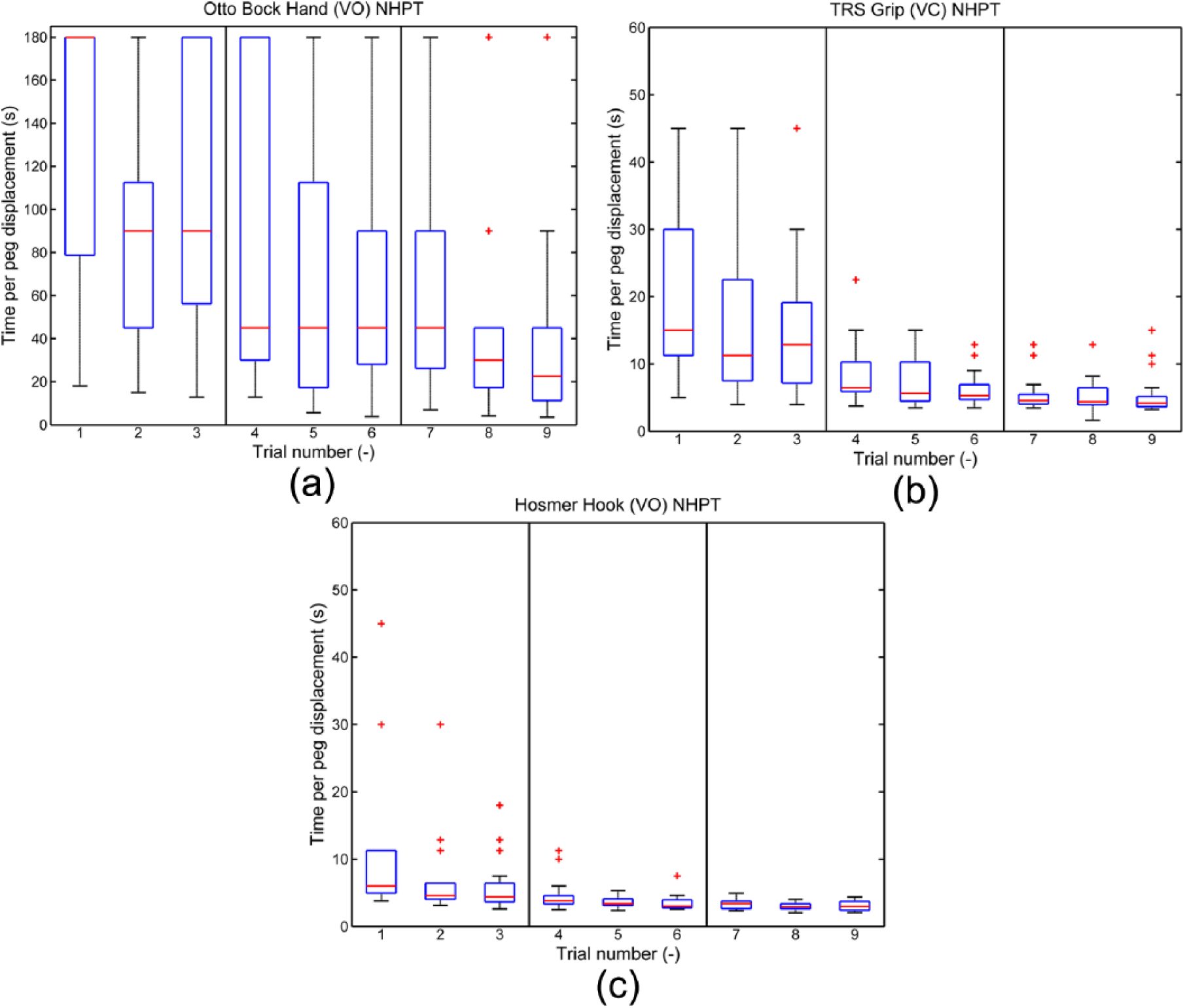
(a) Scores of the Otto Bock hand during the Nine-Hole Peg Test (n = 21), during nine trials at three different days. (The range of the y-axis differs from Figure 6(b) and (c).) (b) Scores of the TRS Grip hook during the Nine-Hole Peg Test (n = 21), during nine trials at three different days. (c) Scores of the Hosmer hook during the Nine-Hole Peg Test (n = 21), during nine trials at three different days.
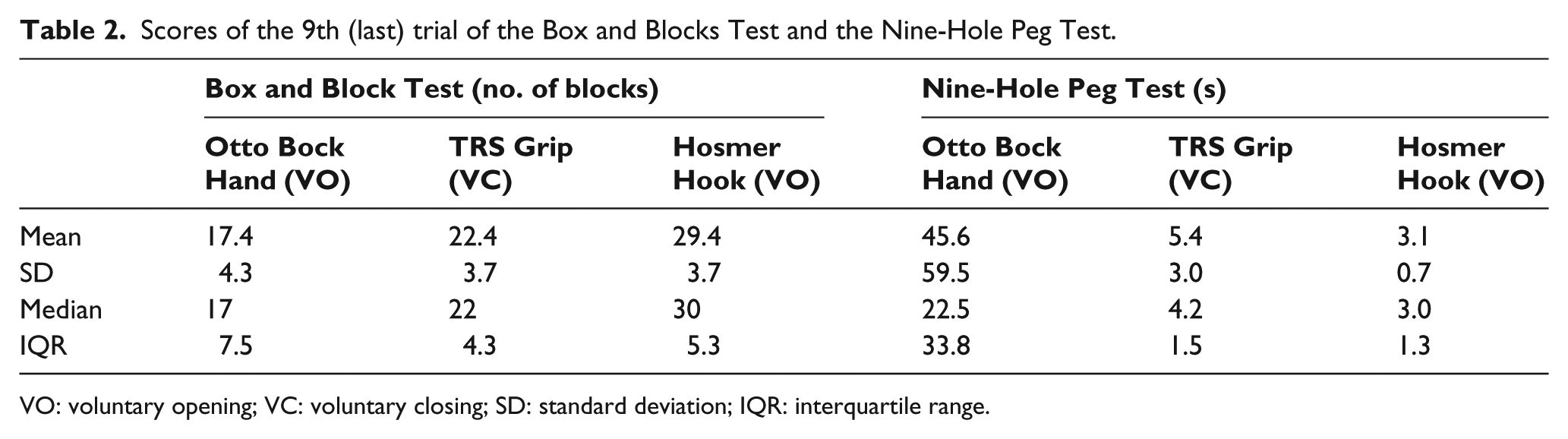
Table 2 shows the scores of the 9th (last) trial of the BBT and the NHPT.
Scores of the 9th (last) trial of the Box and Blocks Test and the Nine-Hole Peg Test.
VO: voluntary opening; VC: voluntary closing; SD: standard deviation; IQR: interquartile range.
Discussion
BBT and NHPT scores
Significant differences were found between the tested terminal devices. The Hosmer hook scored best in both tests, concerning the median and the IQR values of the last trial (BBT: median = 30 blocks, IQR = 5.3; NHPT: median = 3 s/peg, IQR = 1.3). The TRS Grip 2S hook scored the second best on both tests (BBT: median = 22 blocks, IQR = 4.3; NHPT: median = 4.2 s/peg, IQR = 1.5.) The Otto Bock hand showed the lowest scores (BBT: median = 17 blocks, IQR = 7.5; NHPT: median = 22.5 s/peg, IQR = 133.8). These outcomes enable objective comparison between the functional performances of the tested BP terminal devices. When comparing the scores in the BBT with the scores of the NHPT, the Otto Bock hand had a relatively lower score in the NHPT than in the BBT. This is probably related to the more fine motor skills that are required to complete the NHPT. It seems that performing fine motor skills is much more difficult for the Otto Bock hand than gross motor skills. The large IQR for the Otto Bock hand during the NHPT presents the differences in performance between the subjects. Some managed to pick up the pegs and some permanently failed. The shape and material of the fingers combined with the size of the objects might be a factor for this result (block = 25 mm × 25 mm, peg = 9 mm x 32 mm). The decreasing variance in subsequent trials (e.g. OB hand in NHPT) and the improving scores clearly show that the subjects did improve their control skills during the subsequent trials. In the NHPT, the variance decreased and the median scores improved, which means that the scores of the subjects improved and the differences among subjects decreased. In the BBT, the variance did not decrease as the median scores improved. This shows that the difference among different subjects did not decrease, while the group as a whole improved their score. Finally, it is interesting to note that all subjects were able to operate all devices directly after donning, despite the fact that they were inexperienced and were only given basic instructions. This illustrates the straightforward control principle of BP devices.
Comparison to other studies
A small age group (20–24 years) was selected to reduce variances in the tests. A group with a similar age range was also used in the studies of Mathiowetz et al.,20,21 which reported normative scores for healthy people using their sound hand in the BBT and the NHPT. These studies showed for the left hand BBT scores of 84.9 ± 8.2 blocks (males and females together) and NHPT scores of 0.95 ± 0.12 s/peg movement. Both reported scores are three times faster than the fastest prosthetic device in our study, the Hosmer hook. In 2007, Farrell and Weir 13 reported BBT scores for MYO prostheses. After a learning effect over seven trials (n = 20), the ‘fast’ MYO hands showed a score of 28 ± 4 blocks. The scores of these fast MYO hands are comparable with the scores of the Hosmer hook in our study.
Strengths and limitations
There were some factors that could have influenced the scores of the tests. One of the factors was the stool height. Subjects had the chance to adjust their stool height because sitting in a lower position could cause bumping against the table or box, with the lower part of the simulator. Between the days there was minimal one night rest, but the number of nights varied. Also, the moments the subjects were tested each day varied from day to day. These factors could be of influence. By using a simulator, the arm length became longer; however, every participant had to cope with this complication. Amputees using a real prosthesis do not have this problem, as the length of their prosthetic arm is equal to their sound arm. The different shapes of the terminal devices could have had a certain influence on the outcomes, for example, the round fingers of the OB hand make it harder to pick up the small round pegs. Other device properties, like difference in device mass, contact surface or differences in activation force level, might also have influence to the results. This study focused on commercially available terminal devices as a whole, in order to rate their overall functional performance. For prosthetic design purposes, it would however be interesting to vary individual device properties, in order to study their individual influence on the functional performance. Another factor of influence is the learning effect. If one looks at the learning curves in Figures 5 and 6, it can be seen that for some cases, there are still learning effects in trial 9. It would therefore be interesting to see the outcomes in a later stadium, when the curve has flattened and the subjects are totally used to the terminal devices. This might show higher scores for some of the devices.
The goal of this study was to objectively measure and compare the functional performance of three commonly used BP upper limb terminal devices. Based on these outcomes, the Hosmer hook scored best in functional performance. Although the BBT and the NHPT might not be representative for all activities of daily living, the outcomes do present a degree of manual dexterity. The BBT and the NHPT do only measure a limited part of functionality. To evaluate the daily practice of prosthetic users, it might be more useful to choose a functional test which focuses on activities of daily living (e.g. SHAP,10,11 Sollerman and Ejeskär, 22 Jebsen Taylor 23 ).
The measured data can be used as a reference score to compare the functional performance of current and future terminal devices. Such reference scores have not been available so far for BP devices. The measured scores enable the comparison of the performance of a prosthesis user and his terminal device relative to standard scores.
Conclusion
The goal of this study was to objectively measure and compare the functional performance of three commonly used BP upper limb terminal devices. The functional tests showed significant differences between the tested devices. The Hosmer hook scored best in both tests (BBT: median = 30 blocks, IQR = 5.3; NHPT: median = 3 s/peg, IQR = 1.3). The TRS Grip 2S hook scored second best on both tests (BBT: median = 22 blocks, IQR = 4.3; NHPT: median = 4.2 s/peg, IQR = 1.5.) The Otto Bock hand showed the lowest scores (BBT: median = 17 blocks, IQR = 7.5; NHPT: median = 22.5 s/peg, IQR = 133.8). No significant differences were found between male and female subjects. In both the BBT and NHPT, each terminal device showed significant progression in functional performance in a short time (less than 3 h over three different days). This study provides objective quantitative data on the functional performance of commonly used BP terminal devices. The measured scores enable the objective comparison of the functional performance of terminal devices, and of prosthesis users using their terminal device, relative to standard scores.
Footnotes
Acknowledgements
We would like to thank Maurice LeBlanc for proofreading and checking the manuscript for grammatical errors.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.