
Abstract
Background:
Knee osteoarthritis is a musculoskeletal condition which is most prevalent in the medial compartment. This injury causes considerable pain, disability, and negative changes in kinetic and kinematic parameters. The efficiency of unloader valgus brace as a conservative treatment for medial knee osteoarthritis is not well documented.
Objectives:
The aim of this study was to review the previous research regarding the biomechanical effects of knee valgus braces on walking in medial compartment knee osteoarthritis patients.
Study design:
Literature review
Methods:
According to the population intervention comparison outcome measure methods and based on selected keywords, 12 studies were chosen according to (met) the inclusion criteria.
Results:
The results indicated that treatment with knee braces was effective in decreasing pain, improving function, ameliorating improvement in range of motion, and increasing speed of walking and step length in conjunction with a reduction in the adduction moment applied to the knee.
Conclusion:
Osteoarthritis knee braces may be considered for improvement of walking and treatment of medial compartment knee osteoarthritis.
Clinical relevance
Knee braces are an orthotic intervention that could potentially be significant in assisting in improving the walking parameters and treatment of medial compartment knee osteoarthritis.
Background
Knee osteoarthritis (OA) is one of the most common joint disorders. Epidemiological studies have demonstrated that approximately 6% of the population aged 30 years or older and 12% of the population aged 65 years or older have knee OA. 1 Medial compartment OA is more prevalent than lateral compartment disease due to the mechanism of load distribution in normal walking. It has been estimated that 60%–80% of load is distributed to the medial compartment of the knee joint during normal walking. This is due to the external varus moment (otherwise known as the adductor moment) falling medial to the knee joint. 2 OA of the medial compartment of the knee causes considerable pain, immobility, disability, a reduced quality of life, and negative changes in kinetic and kinematic parameters.1,3
In response to pain, patients adapt their gait and these adaptations may result in further progression of OA. This means that the joint degeneration experienced by people with medial compartment knee OA is also associated with alteration to normal gait patterns and the existence of compensating motions in the lower back and lower extremity joints. 3
Treatments for knee OA are designed to alleviate pain by attempting to correct mechanical malalignment.4,5 Treatment approaches for knee OA may be divided into operative and non-operative methods. Operative treatment includes arthroscopy, joint replacement, and osteotomies. Non-operative methods are often prescribed (indicated) in mild to moderate stages or when surgery is not feasible and consist of drug therapy, physiotherapy, and orthopedic devices (assistive devices, walking aids, foot orthoses, and knee braces). 6
According to the categorization of American Academy of Orthopedic surgeons, knee braces are divided into four classifications including prophylactic, functional, rehabilitative, and valgus off-loader knee braces. The valgus off-loader knee braces are common nonsurgical strategy for treatment of people with medial knee OA. 7 It has been reported that the use of valgus brace involves a combination of several mechanisms. 1 Theoretically, valgus unloader braces provide pain relief by reducing the load on the medial compartment through the application of an opposing external valgus moment about the knee that partially compensates for the external varus moment. 7 This is achieved by applying an external corrective force to the knee through the adjustable straps or condylar pads while opposing counter-forces arising from the upper and lower brace supports act proximal and distal to the knee joint. This is called a three-point pressure mechanism of valgus unloading by the brace. The resulting improvement in knee alignment can cause reduction in the moment arm of the knee adduction moment (KAM) and the value of the KAM itself. At the same time, compressive load is shifted away from the medial compartment, thereby improving the distribution of compressive load over the joint surfaces. This mechanism also leads to a reduction in the need for the muscles and ligaments to be activated to counteract the pathological forces. Unloader braces have also been shown to delay the requirement for knee surgery.1,6,7
Several studies investigated the efficacy of different types of knee braces on gait parameter in medial knee OA. Gaasbeek et al. 8 addressed walking parameters (e.g. step length, rang of motion, walking speed, and adduction moment) and reported that utilizing the knee braces results in reduction in the range of motion (ROM) in the arthritic limb and because of that the step length and stride length decrease on the arthritic limb. However, Arazpour et al. 9 in their evaluation concluded that the ROM and step length increased with the knee braced. In addition, there are two reviews that assessed the effectiveness of knee braces for medial knee OA. Ramsey et al. and Feehan et al. performed reviews about the efficacy of off-loader knee braces on the reduction of pain in medial compartment knee OA. They concluded that reduction of pain by wearing off-loading knee brace was instantaneous, and that these braces are cost-effective devices for treatment of patient with knee OA. Both studies only evaluated the changes in pain severity.7,10 According to these controversies and since there is no previous literature published that has evaluated the effectiveness of knee braces on gait parameters in patient with medial knee OA, a literature review was conducted which targeted the efficacy of the knee orthosis on the gait parameter in medial knee OA.
Methods
Search strategy
Using the population intervention comparison outcome (PICO) method (Table 1), and based on selected keywords (OA, medial knee OA, knee joint arthritis, valgus knee brace, knee unloader orthosis, knee sleeve, adduction moment, pain, speed of walking, cadence, step length, kinematics, kinetics) and their composition, a search was performed in PubMed, Science Direct, and ISI Web of Knowledge databases. By using “OR,” “AND,” and “NOT” words as Boolean operators between the selected keywords, relevant articles published in this field were identified. Identified articles were published in English language between 1960 up to and including the year 2013 and met the inclusion criteria. The inclusion and exclusion criteria are shown in Table 2. Finally, 12 articles were selected for final evaluation. The procedure was followed using the preferred reporting items for systematic reviews and meta-analyses (PRISMA) method (Figure 1).
Selected keywords using the PICO method.
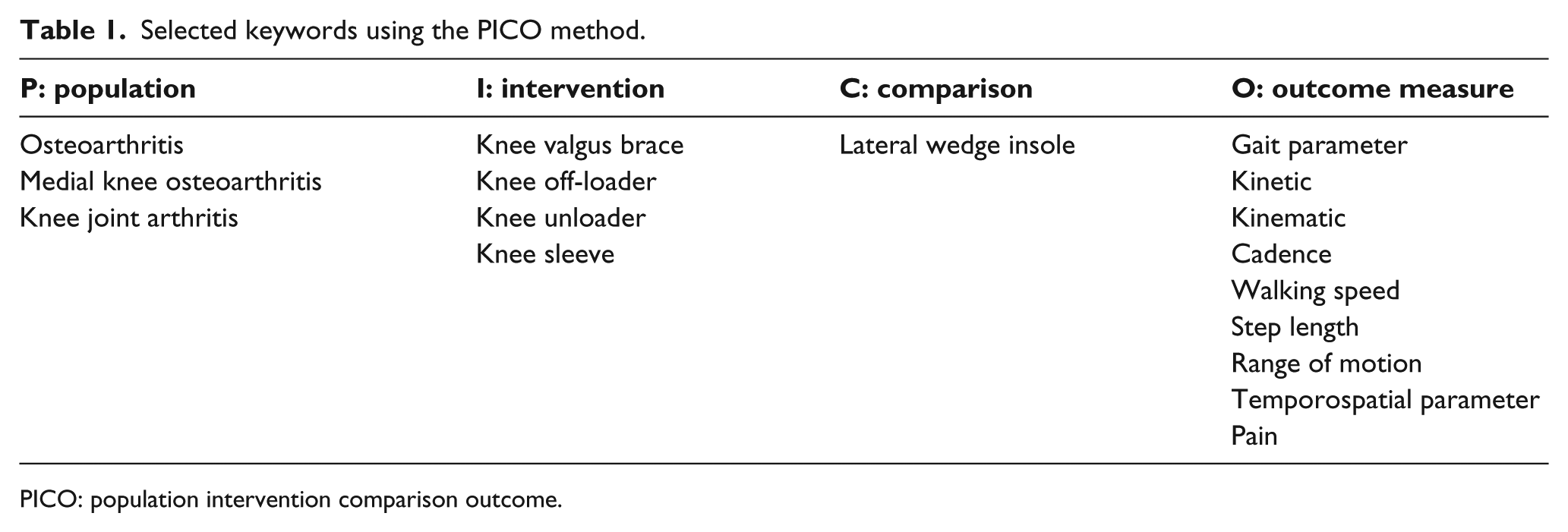
PICO: population intervention comparison outcome.
Inclusion and exclusion criteria utilized to select articles.
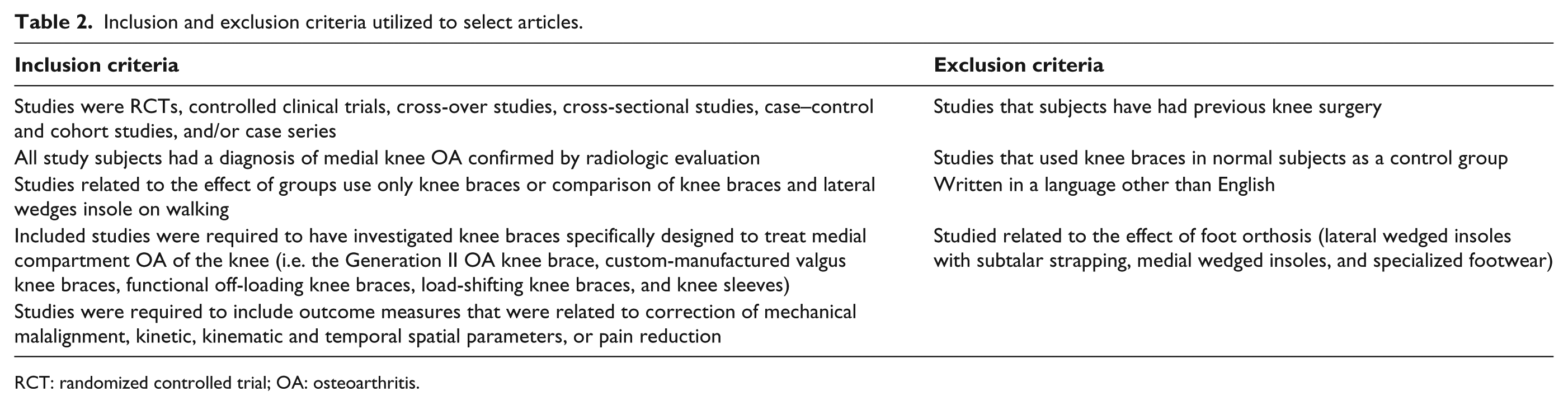
RCT: randomized controlled trial; OA: osteoarthritis.
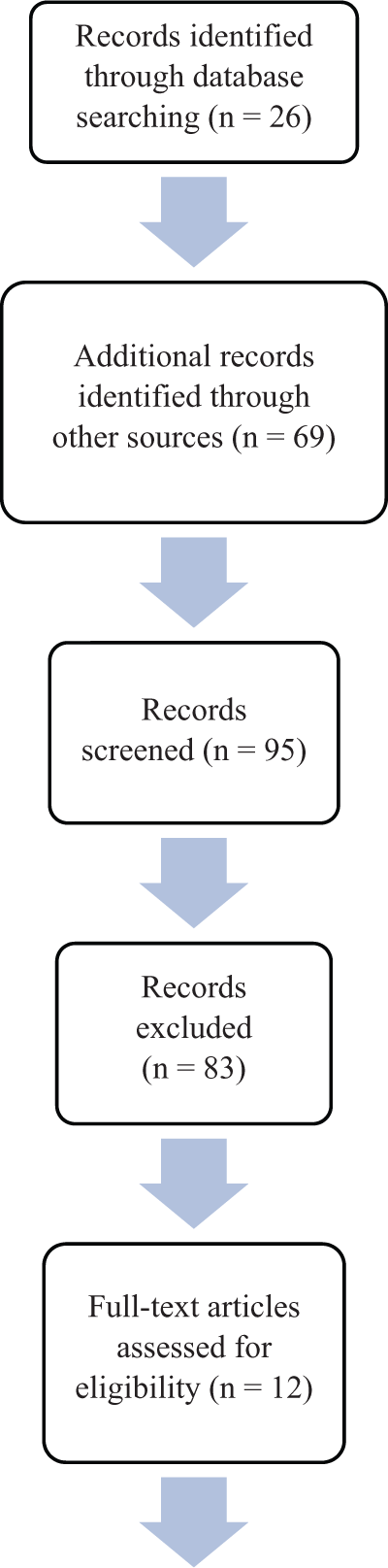
Procedure was followed using the PRISMA method.
Results
Following the selection procedure, 12 studies that evaluated the effect of knee valgus orthoses on walking in medial compartment knee OA were deemed to be suitable for inclusion in this review. Schmalz et al. 6 demonstrated that through wearing knee valgus braces after 4 weeks by 16 patients with medial compartment knee OA, the mean walking speed significantly increased from 1.27 m/s without brace (WOB) to 1.36 m/s with brace (WB). In addition, cadence with the brace increased significantly compared to WOB, from 107 to110 steps/min. The step length for the arthritic limb increased from 0.71 m in the WOB test condition to 0.73 m in WB, while step length of the contralateral limb reduced from 0.75 to 0.73 m. In addition, the results from this study showed that the valgus knee brace could compensate for approximately 10% of the external genu varus moment. 6
In a study following 6 weeks with use of a valgus brace by 15 patients with medial compartment knee OA, Gaasbeek et al. found that the brace had a tendency of lowering the peak varus moment about the knee. Statistically, the peak varus moment was significantly higher in the affected leg than in the unaffected leg without the brace worn (p = 0.021). Furthermore, by wearing the brace, their results showed that the patients walked faster on the second testing day and there was no significant difference between conditions WOB and WB (p = 0.063). Also with the brace, the steps were shorter than without the brace (p = 0.017 and p < 0.001). The ROM was significantly reduced in the braced condition compared to the non-braced condition (p = 0.02). Finally, significant improvements were found for the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) without the brace (50.1 ± 17.6) and with the brace (63.0 ± 18.4). Also, using a Visual Analog Scale (VAS), the knee pain scores were reduced (without brace −6.8 ± 2.5 and with brace −4.7 ± 3). 8
A study by Pollo et al. examined the varus moment caused by a knee brace in 11 patients. They reported that pain and activity levels were improved in all subjects with valgus bracing. During gait, valgus bracing reduced the varus moment about the knee by an average of 13% (7.1 N/m) and the medial compartment load at the knee by an average of 11% (114 N) with the brace in 4° of valgus adjustment. 11
Self et al. used the Monarch (valgus) brace in five patients and found that the valgus brace reduced the varus moment significantly during 20% and 25% of stance phase of gait. The valgus force remained fairly constant throughout the first 80% of the stance phase. 12
Fantini Pagani et al. compared two knee braces with the valgus re-alignment adjusted in two different positions (neutral and 4° valgus) in 11 patients with medial knee OA. They demonstrated that both orthoses induced pain relief and improvement in function compared with the condition without the orthosis. KAMs were significantly decreased with both adjustments, whereas the decrease observed with the 4° valgus adjustment was significantly greater than the flexible adjustment (25% vs 12.5%). Compared with the condition without an orthosis, changes in knee adduction angular impulse of 29% and 15% were found with 4° valgus and the neutral flexible orthosis, respectively. Average walking speed in conditions without an orthosis, 4° valgus, and neutral flexible were 1.45 ± 0.15, 1.47 ± .12, and 1.45 ± 0.14 m/s, respectively. 13
In a cross-over study, Richards et al. evaluated two types of knee brace by 12 patients with OA of the medial compartment. Treatment with a simple hinged brace was compared with a valgus corrective brace. Outcome measurements in this study were knee kinematics, ground reaction forces, pain, and function during walking. Statistically significant improvements in pain, function, and loading and propulsive forces were seen with the valgus brace. 14
Lindenfeld et al. examined valgus braces by 11 patients. When wearing a brace, pain decreased by 48% and function increased by 79%. The mean adduction moment without the brace was 4.0 ± 8% and with brace was 3.6 ± 0.8% (a 10% decrease). 15
In a cross-over randomized design, Jones et al. compared valgus knee braces and lateral wedge insoles on their biomechanical effects in 28 patients for 2 weeks. Their results demonstrated that walking velocity was significantly increased by wearing the valgus knee brace (1.17 (0.12) m/s) and the lateral wedged insole (1.18 (0.11) m/s) significantly increased walking speed, but no significant differences were reported between them in walking speed. Also, the knee valgus brace and a lateral wedge insole alleviated the early stance external knee adduction moment (EKAM) by 7% and 12%, respectively. That means that the lateral wedged insole reduced the early EKAM more effectively compared to the valgus knee brace (p = 0.001). 16
Fantini Pagani et al. evaluated the effect of a valgus knee brace and a lateral wedged insole on knee and ankle kinematics and kinetics, in 10 patients with medial knee OA. The knee orthosis was tested in two valgus adjustments (4° and 8°), and the laterally wedged insole was fabricated with an inclination of 4°. They found that with regard to the second peak KAM, decreases of 18%, 21%, and 7% were observed between baseline and test conditions for the orthosis in 4° of valgus, in 8° of valgus, and the insole, respectively. Knee adduction angular impulse decreased 14%, 18%, and 7% from baseline to conditions for the orthosis in 4° valgus, in 8° valgus, and insole, respectively. Knee angle in the frontal plane reached a more valgus position during gait using the valgus knee brace. The valgus moment applied by the orthosis with 8° valgus adjustment was 30% higher than with 4° valgus adjustment. 17
In a prospective open-label (completely unblinded) parallel randomized controlled trial (RCT) study, Van Raaij et al. compared the effect of a 10-mm laterally wedged insole (index group, n = 45) and a valgus brace (control group, n = 46) on their improved pain, function, and correct varus malalignment. After 6 months, they observed no differences between both groups for VAS pain scores (mean 0.06; 95% confidence interval (CI): 1.05, 0.93; effect size 0.03) and WOMAC function scores (mean 0.15; 95% CI: 7.95, 7.65; effect size 0.008). Compared with baseline, the pain severity and WOMAC function scores improved in both groups. Also, varus alignment correction when wearing the insole or brace was similar in the two groups (0.22; 95% CI: 0.68, 0.25; effect size 0.22). The mean varus alignment (Hip Knee Ankle angle) for the insole group (6.9; standard deviation (SD): 3.6) was similar (p = 0.8) at baseline compared with when wearing the wedge (6.9; SD: 4.1). 18
Girija et al. in a randomized study (n = 28) compared the efficacy of a lateral wedged insole and valgus knee brace. The patients wore their respective orthosis 8 h per day for 4 weeks. The outcomes were isokinetic concentric peak torque of quadriceps and hamstrings, pain, and functional status (WOMAC), pre- and post-intervention. There was a statistically significant reduction in VAS during rest and activity after the intervention difference in both the groups. There was highly significant difference in improvement of the WOMAC scores in both the groups. Both interventions improved the isokinetic concentric peak torque of the quadriceps, hamstrings muscles, functional status, and in producing reduced pain. 19
Arazpour et al. compared the effect of an unloader knee orthosis and insoles on kinetics and kinematic in 24 patients with medial compartment knee OA. They found that after 6 weeks, both orthoses improved all parameters compared to the baseline condition (p < 0.001). However, no significant differences in pain (p = 0.649), adduction moment (p = 0.205), speed of walking (p = 0. 056), or step length (p = 0.687) were demonstrated between them. Also, the knee ROM (p < 0.001) was significantly different between the two interventions. The increase in knee ROM for the lateral wedge condition (46.98 ±1.88)°, was significantly less (p = 0.205), than that noted for the unloaded knee brace group; (53.6 ±3.00). 9
Kinetic and kinematic parameters
Knee ROM
Two studies were found which evaluated the influence of a knee valgus brace on knee ROM (Table 3). Gaasbeek et al. reported that a valgus knee brace significantly reduced the ROM compared to the non-braced condition. Their results showed that the brace prevented full extension at the end of swing phase. 8 On the other hand, Arazpour et al. 9 found mean increases in the knee ROM with braces (46.9°) compared to baseline conditions (42.21°).
Studies that evaluated the efficacy of knee orthoses on kinetic and kinematic parameters in medial compartment knee osteoarthritis.
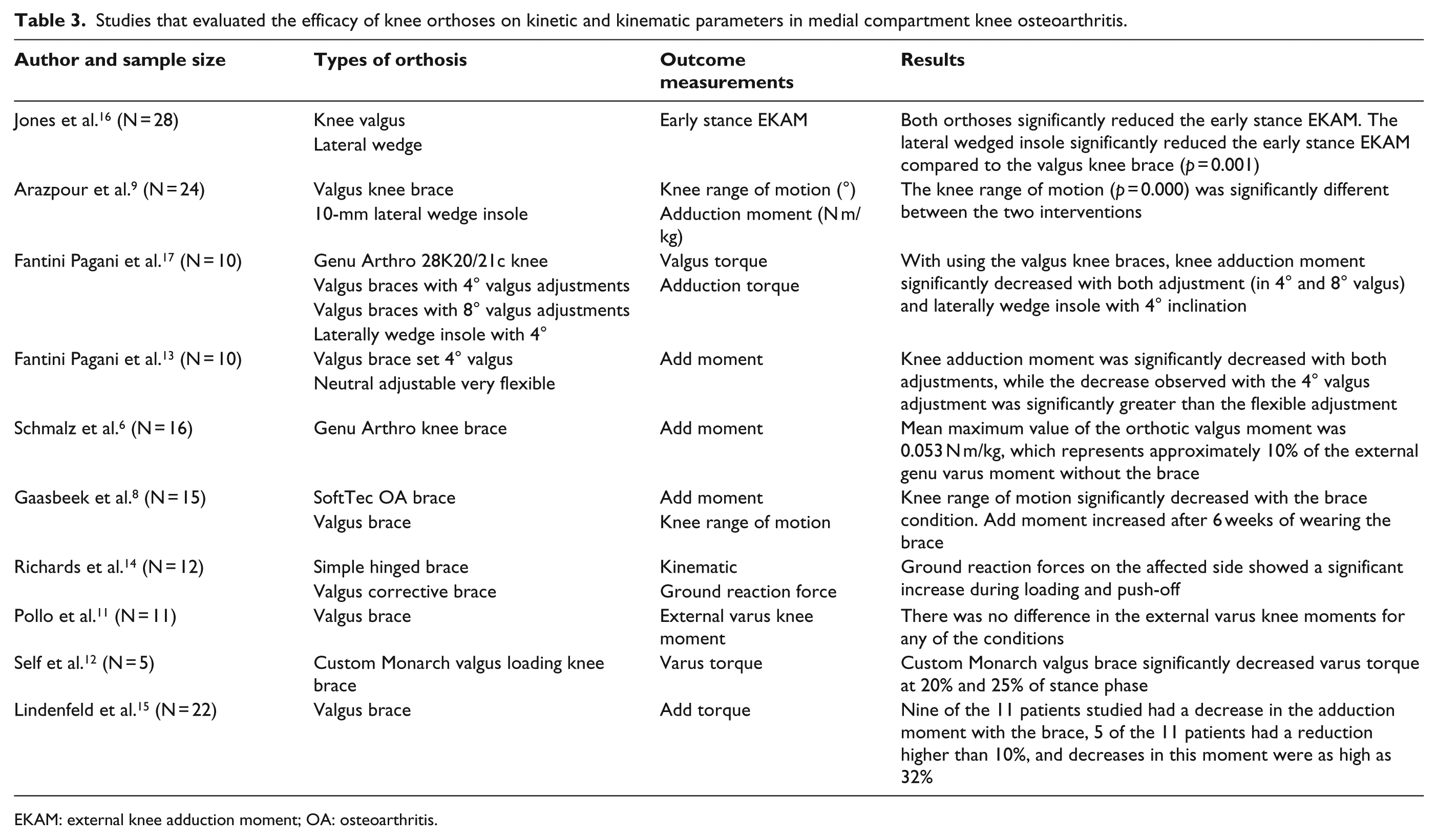
EKAM: external knee adduction moment; OA: osteoarthritis.
Adduction moment
Most of the evidence in the literature demonstrates that knee braces result in a reduction in the adduction moment about the knee. Fantini Pagani et al. 17 demonstrated that the KAM was significantly decreased with both adjustments (4° and 8° valgus), but the decrease observed with the 4° valgus adjustment was greater than the flexible adjustment (25% vs 12.5%). In another study by Fantini Pagani et al., 13 they showed that compared to the baseline condition, setting the knee braces in 4° valgus and in 8° valgus results in decreases of 18% and 21% in second peak KAM, respectively. Also, Lindenfeld et al. 15 reported 10% decease in the mean adduction moment compared to without-brace condition.
Temporospatial parameters
Speed of walking
Four studies reported the positive effects of knee valgus braces on the speed of walking (Table 4). Schmalz et al. found that the mean walking speed significantly increased from 1.27 m/s WOB to 1.36 m/s WB. Gaasbeek et al. 8 demonstrated that patients with a valgus unloader brace walked faster. Also, Arazpour et al. 9 found that speed of walking in baseline was 0.90 (0.028) and after 6 weeks of brace used this increased to 1.08 (0.034). Fantini Pagani et al. 13 showed that average walking speed in test conditions without an orthosis, with 4°of valgus angulation, and a neutral flexible test condition were 1.45 ± .15, 1.47 ± .12, and 1.45 ± .14 m/s, respectively, and no significant differences were reported for gait velocity among these conditions.
Studies that evaluated the efficacy of knee orthoses on temporospatial parameters in medial compartment knee osteoarthritis.
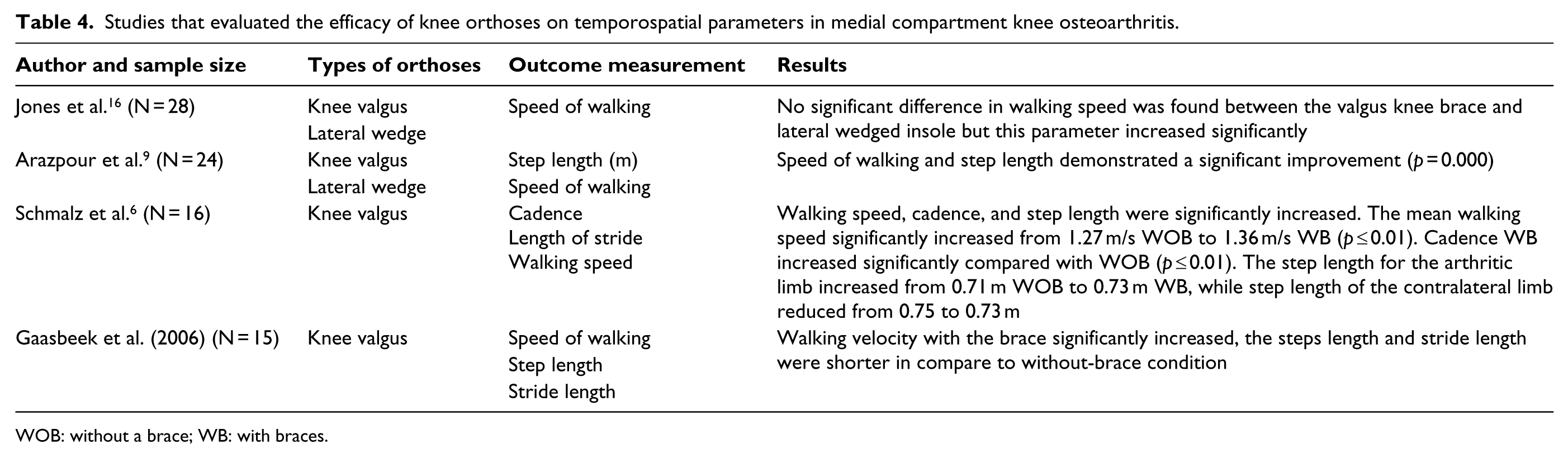
WOB: without a brace; WB: with braces.
Cadence
Only one study has reported about changes in cadence. In 2010, Schmalz et al. 6 showed that this parameter was increased significantly when walking with a brace compared to WOB, from 107 to 110°steps/min.
Step length
The review of the literature indicates that knee braces are efficient in improving step length in the arthritic limb. This has been shown to increase from 0.71 m (WOB) to 0.73 m (WB), while step length of the contralateral limb reduced from 0.75 to 0.73 m. 6 However, Gaasbeek et al. showed the opposite effects of knee braces on step length and stride length. They reported that the duration of swing phase was decreased, which would explain the decreased step and stride length during walking with brace. 8
Pain
Numerous analyses have demonstrated that pain can be significantly reduced through using a knee valgus unloader brace.11,14,18,19 Lindenfeld et al. 15 found that by wearing a brace, pain was reduced by 48% and also overall function may be increased by 79%. Also, Gaasbeek et al. 8 reported that the WOMAC score may be altered from 50.1 ± 17.6 without wearing a brace to 63.0 ± 18.4 with a brace in situ (Table 5).
Studies that evaluated the efficacy of knee orthoses on pain in medial compartment knee osteoarthritis.
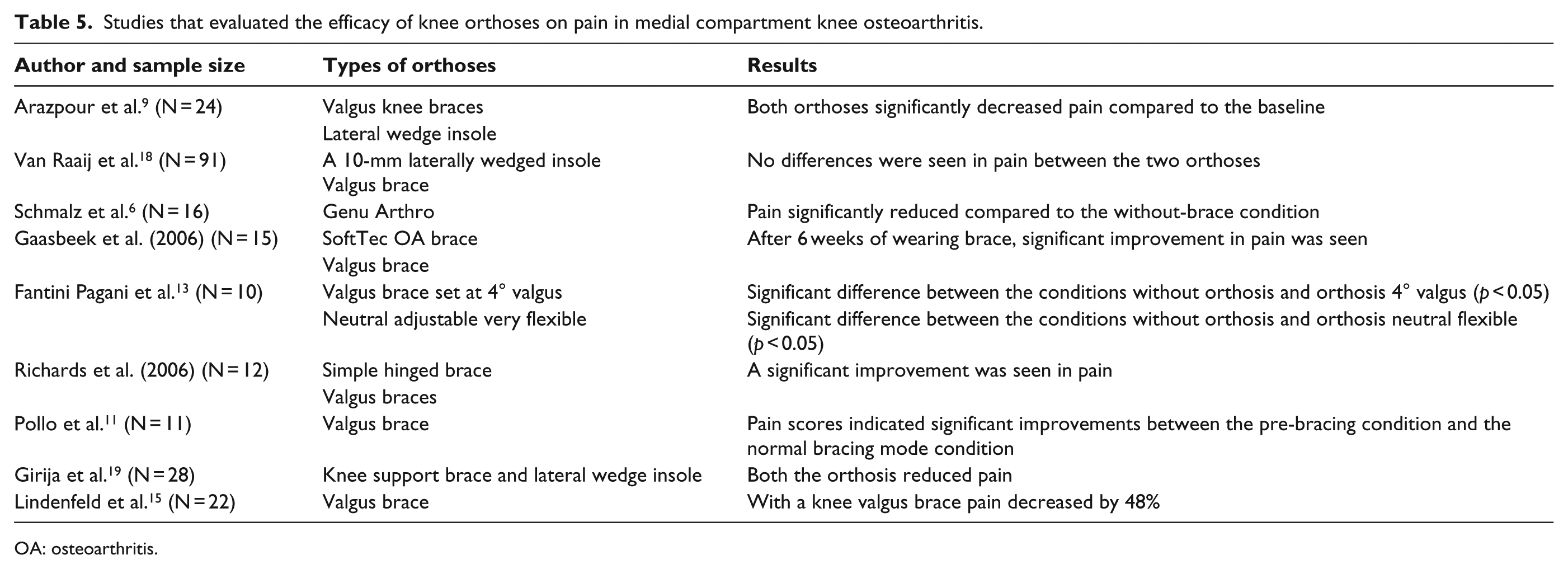
OA: osteoarthritis.
Discussion
This literature review was developed to evaluate the effect of valgus knee unloader braces on gait in medial compartment knee OA patients. Knee braces with corrective valgus adjustments have been commonly prescribed for persons with medial compartment knee OA in recent years.
It has been reported that valgus bracing is used to correct and protect against externally applied adduction moments around the knee. The functional mechanism of valgus bracing is to facilitate a reduction in loads acting on the painful medial compartment by the application of an external valgus moment through three- or four-point force systems acting around the knee joint. Therefore, this externally applied valgus moment reduces the adduction moment responsible for excessive medial compartment loading seen in tibiofemoral OA. This results in an increase in the medial joint space and causes relief of signs and symptoms associated with knee OA.1,6,7
Pain affects the kinetics and kinematics of gait in the subjects with medial knee OA. 20 The results from gait studies have indicated that patients with medial compartment knee OA show lower walking velocity, reduced knee ROM, decreased cadence, reduction in step length and stride length, and increased peak varus moments about the knee during the stance phase of walking in the affected leg. 8 Also, an asymmetry in gait patterns has been observed. 6 Evidence suggests that wearing a valgus unloaded brace results in modification of compressive force in the medial knee compartment, reducing the KAM and alleviating symptomatic pain. Following this mechanism, improved gait symmetry and increased activity of patients who have medial OA of the knee have been demonstrated, 13 but because of the small sample sizes of some studies, conclusive evidence of these positive effects of knee braces on gait parameter has not yet been proven, and this suggests that future studies should evaluate valgus unloaded brace efficacy using larger sample sizes.
The evidence also suggests that the gait characteristics demonstrated by medial knee OA subjects are improved when walking with unloaded valgus braces. Knee brace wear results in pain relief and improvement in function by increasing the medial joint space and decreasing joint contact pressure.6,13,20 It has been demonstrated that medial knee OA patients walk at slower velocities to reduce loading in the medial compartment of the knee, and this may be increased by wearing a valgus unloader knee brace which provides an improvement of function and reduction of pain after brace treatment.6,8 However, knee ROM in the sagittal plane has been shown to be significantly reduced in braced conditions. 8
In response to the pain experienced by this patient group, adaptive mechanisms such as shortening stride or step length are commonly seen in order to lower the adduction moment during gait. During walking with knee braces, patients have been shown to demonstrate a significant increase in stride length when compared to an un-braced test condition.1,8 This has been attributed to the reduction in pain by use of a knee valgus brace. Although Fantini Pagani et al. 17 adjusted the knee brace in only 4° and 8° of valgus setting, they found that the more the valgus adjustment, the more the decrease in adduction moment could be demonstrated. Future study designs should therefore compare the various valgus adjustments along with an instrumented orthosis for measuring the valgus force that may be produced by an unloader knee brace.
Despite the positive effects of valgus unloader brace use, brace wear has some functional drawbacks. They can cause a significant reduction in knee flexion during swing phase. This restriction can result in reduced foot clearance 14 and a shorter stride.8,14 Simple hinged braces do not produce such a restriction. The main causes of restriction are that the valgus brace is significantly larger and, with only a single hinge, is prone to torsional misalignment.1,14 Therefore, future studies should evaluate and design the valgus unloader brace that is light and is manufactured from high-quality material which can resolve these issues through imaginative new designs.
Future studies should therefore include the following:
Comparison of the various valgus adjustments available along with instrumented orthosis design for measuring the valgus force that is produced with knee unloader braces.
Investigations should employ high methodological quality, particularly in randomization and blinding techniques.
Investigation of the energy consumption in patients with medial knee OA.
Evaluation of valgus unloader brace efficacy in improving specific outcome measures in medium- to long-term longitudinal studies in patients with medial compartment knee OA.
Evaluation of valgus unloader braces using larger sample sizes than previously.
Conclusion
In summary, this study suggests that valgus unloader braces can re-distribute loads in the degenerative compartment of knees and can subsequently reduce the adduction moment acting on the knee. Finally, treatment with knee braces is effective in decreasing pain and increasing speed of walking and step length in conjunction with a reduction in the adduction moment applied to the medial compartment of knee joint.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.