
Abstract
Background
The effectiveness of arthroscopic treatment for knee osteoarthritis (OA) has been controversial. This study compares the clinical outcomes of the arthroscopic cartilage regeneration facilitating procedure (ACRFP) and conservative treatment.
Methods
During the year of 2016, 524 patients (882 knees) who were older than 40 years of age and diagnosed with different stages of knee OA were scheduled for ACRFP under the protocol of knee health promotion option (KHPO) for knee OA. Of those, 259 patients (413 knees) eventually received ACRFP (the ACRFP group), and 265 patients (469 knees) didn’t receive ACRFP but received conservative treatment (the non-ACRFP group). A telephone questionnaire was used to evaluate the subjective satisfaction and the incidence of receiving arthroplasty for these patients.
Results
After the mean follow-up period of 61.6 months (SD 4.5), there were 220 patients (374 knees, 90.6%) in the ACRFP group and 246 patients (431 knees, 90.0%) in the non-ACRFP group completed the outcome study. The satisfactory rate was statistically higher for the ACRFP group (90.64%) than for the non-ACRFP group (70.3%) and the difference in subjective satisfaction was more obvious in patients with more advanced knee OA. As for the incidence of patients having subsequently received arthroplasty, it was higher (13.46%) in the non-ACRFP group than in the ACRFP group (4.28%).
Conclusion
Compared with conservative treatment, ACRFP could satisfy more patients with knee OA and modify their natural course by decreasing the incidence of subsequent arthroplasty.
Introduction
Knee osteoarthritis (OA) remains a tremendous public health concern, both in terms of health-related quality of life and financial burden of the disease. Conservative therapies, such as nonpharmacological interventions, systemic drug treatment and intra-articular therapies ranging from corticosteroids to hyaluronans to more recently platelet-rich plasma and even stem cells have been used for symptom relief before resorting to surgery, but conservative therapies have often provided inadequate disease control. There was no evidence to verify their effectiveness in reversing the natural course of knee OA till now. Arthroscopic intervention has been commonly used for many years to treat knee OA and to address degenerative articular cartilage and menisci,1–3 however, several studies have verified that it is not an effective treatment for the majority of cases and should generally not be considered when managing knee OA.4–8
Based on a series of studies highlighting medial abrasion phenomenon (MAP) as a cause of knee OA,9–14 an integrated protocol for the treatment of knee OA called “knee health promotion option (KHPO)” was established. 15 A concept of arthroscopic cartilage regeneration facilitating procedure (ACRFP) under the protocol of KHPO was also developed and reported in 2012 which pointed out that stress and inflammatory responses are the key events that lead to the onset and progression of knee OA caused by MAP and that the ACRFP procedure, by eliminating stress and inflammatory responses as well as comprehensively improving the environment of the knee joint for cartilaginous regeneration, will bring forth long-term favorable effects. 16 Not only for medial compartmental OA, the effectiveness of ACRFP has also been validated for lateral compartmental OA, according to a recent study. 17 Although the clinical effectiveness of this concept has been reconfirmed by other series,18,19 the evidence has not been strong enough to support the popularity of the ACRFP due to a lack of control group in those studies. We therefore conducted a modified randomized controlled study to verify the clinical effectiveness of ACRFP in comparison with conservative treatment.
Material and methods
The protocol of KHPO for knee OA
The first step of KHPO for the treatment of OA knee is thorough evaluation of the patient’s knee condition and establishing the clinical staging for each weight bearing compartment of the knee by both physical and roentgenographic examinations (Figure 1 and Table 1).
15
The staging of OA of the knee is given as the most advanced stage of the two weight bearing compartments. Once the clinical staging has been made, the decision of treatment option for individual patient was made according to our guideline of treatment (Table 2).
15
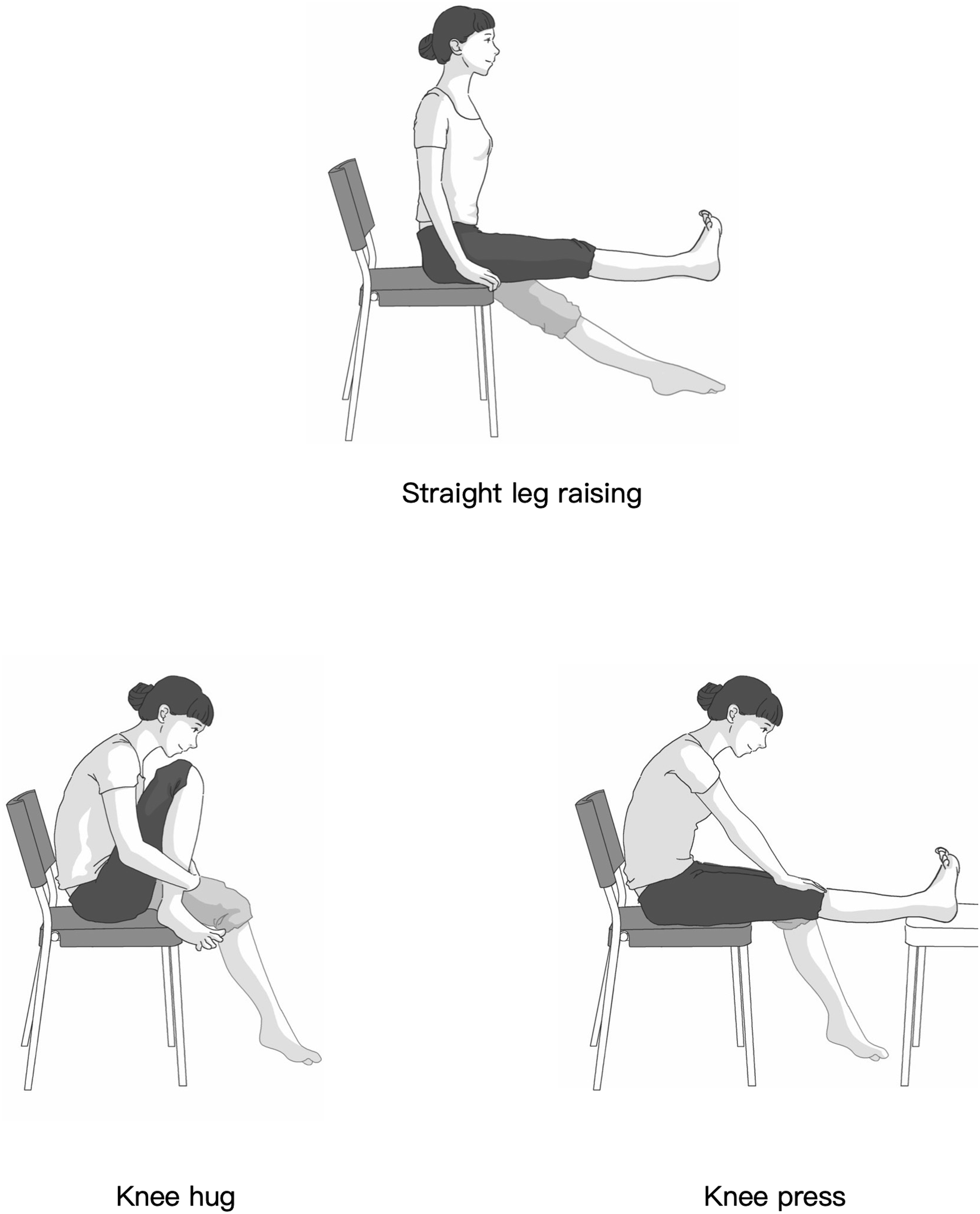
For stage I or II patients, all patients were recommended to encounter into the supervised conservative treatment which we call smart knee care for at least 3 months before the decision of receiving ACRFP was made. The sine qua non for a successful smart knee care is to make patients and the family completely understand our concept that the MAP is an important etiologic factor for knee OA. Daily activities, job and sport modification were tailored for individual patient focusing on the avoidance of the MAP. In general, activities and sports need repeated or quickly knee bending are regarded as harmful. Moreover, home exercises including muscle strengthening by straight-leg-raising and stretching exercises to increase the flexibility by knee hug and knee press were emphasized (Figure 2). For stage III and IV patients, ACRFP is the best choice compared to osteotomy and arthroplasty if the deformity is less severe. However, if the deformity exceeds 7°, arthroplasty including high tibial osteotomy, unicompartmental arthroplasty or total knee arthroplasty with elimination of the MAP which we call precision arthroplasty would be recommended considering patients’ preference and biopsychosocial condition. Protocol of knee health promotion option for knee OA. Clinical staging for OA of individual compartment based on roentgenographic and clinical findings. Surgical treatment guideline for knee OA. ACRFP: arthroscopic cartilage regeneration facilitating procedure; UKA: unicompartmental knee arthroplasty; TKA: total knee arthroplasty. Three home exercises for muscle strengthening and increasing flexibility of the knee.


The arthroscopic cartilage regeneration facilitating procedure
Either spinal or general anesthesia was used for this procedure. Throughout the procedure, patients were put in a supine position and bloodless surgical field was obtained by pneumatic tourniquet. The arthroscopic examination was performed through the inferolateral portal. The presence of medial plica related MAP and its sequelae 9 was first investigated and confirmed. Medial release was then performed step by step as described in previous publication. 16 The inflammatory tissue occupying the space over the inferomedial region of the patella including ligamentum mucosum, fibrotic or inflamed synovium, capsule and distal part of the medial plica was first eradicated. Then, the tight and obliterated medial facet of patellofemoral joint was released by resection of the fibrotic synovium, capsule, and the proximal part of the medial plica. Sometimes, medial retinaculum including fibrotic fascia of pes anserinus and even medial patellofemoral ligament was released as needed. After the medial release, the patella would always deviate laterally. Lateral release was performed by inserting a No. 11 scalpel into the inferolateral portal and cutting the lateral retinaculum percutaneously. Finally, any focal synovitis or loose chondral flaps on the cartilaginous surface was removed as conventional arthroscopic debridement for knee OA. No bony procedure such as drilling or microfracture was performed. From the day of surgery, full range of motion, full weight bearing, and free ambulation were allowed as tolerated. A suction drain was used for 24–48 h. The patient was discharged 2 days after the operation. Home exercise programs, including quadriceps strengthening and passive range of motion, were emphasized. The compliance of patients regarding the home exercise program was strictly monitored by case managers. No supplementary treatment including oral glucosamine sulfate, steroid injections, or intraarticular injection of HA or PRP was given throughout the post-operative follow-up period
The patients
Comparison of demographic data between ACRFP and non-ACRFP groups.
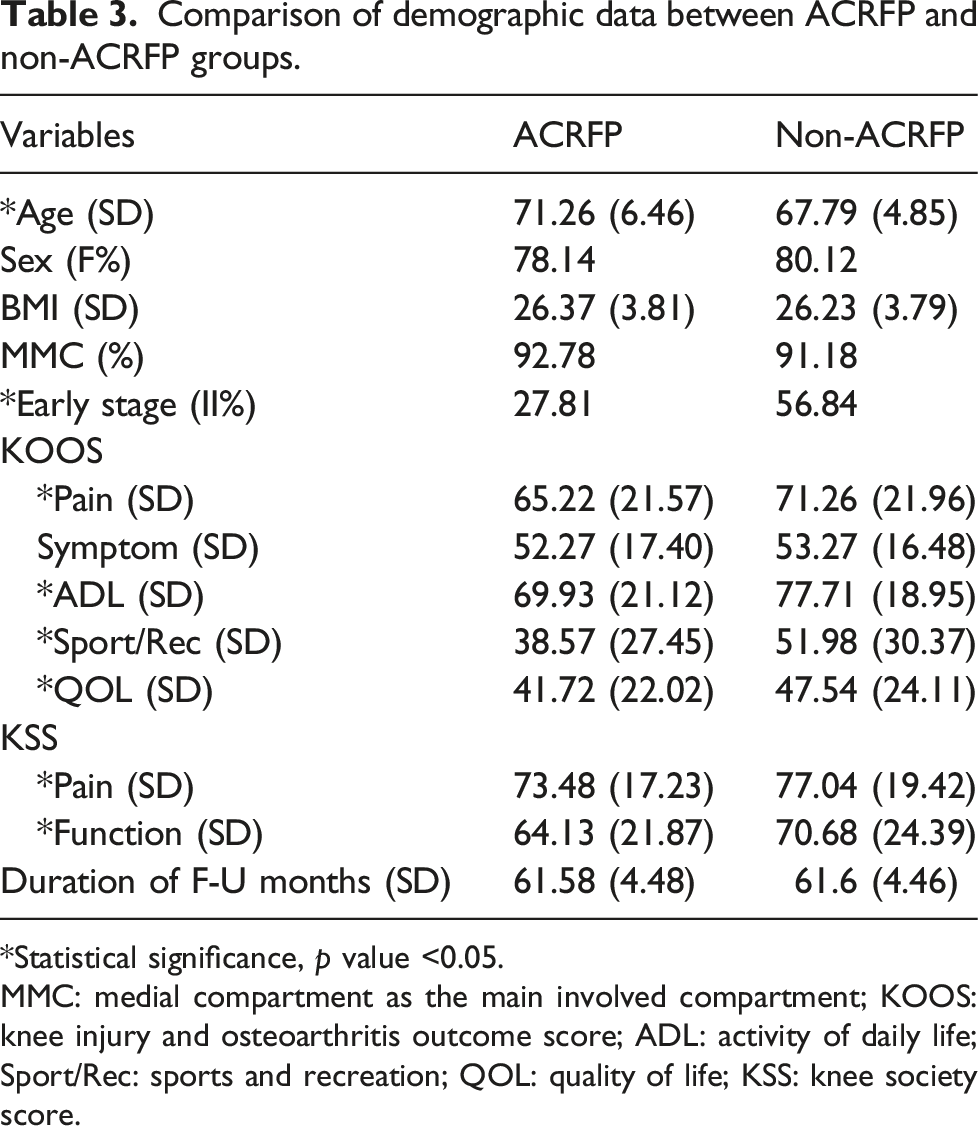
*Statistical significance, p value <0.05.
MMC: medial compartment as the main involved compartment; KOOS: knee injury and osteoarthritis outcome score; ADL: activity of daily life; Sport/Rec: sports and recreation; QOL: quality of life; KSS: knee society score.
Outcome study
A telephone questionnaire was used to evaluate the subjective satisfaction of these patients after a minimum of 5 years. Subjective satisfaction was derived from subjects’ answers to direct questions using a categorical scale prepared for this study: (1) excellent, free of symptoms, no limitation in activities; (2) good, greatly improved, occasional pain, normal activities; (3) fair, same as the condition of the first evaluation, no improvements; and (4) poor, has received arthroplasty. The outcome was regarded as satisfactory if subjective satisfaction was rated as “excellent” or “good”. The inquiries into subjective satisfaction were conducted by our nursing specialists. All investigations focused on individual knees in bilateral cases.
Statistical analysis
Statistical analysis was carried out using JMP, the Statistical Discovery Software (Version 5.0.1.2, SAS Institute Inc., Cary, NC, USA). All values were presented with means and standard deviations. Analyses for comparing demographic data, satisfactory rate, and incidence of patients received arthroplasty between the ACRFP and non-ACRFP groups were performed using Pearson’s Chi-square test. A p-value <0.05 was considered statistically significant.
Results
Satisfactory rate of different stage of OA for ACRFP and non-ACRFP groups stratified by main involved compartment.

Satisfactory rate presented as % (N).
*Statistically significant by comparisons for each pair using paired t test (p < 0.05).
Incidence of arthroplasty for ACRFP and non-ACRFP groups stratified by main involved compartment.

Incidence of arthroplasty presented as % (N).
*Statistically significant by comparisons for each pair using paired t test (p < 0.05).
Discussion
In this report we present and compare the satisfactory rate and incidence of arthroplasty between knee OA patients who have received ACRFP and those who haven’t received this procedure. Although the ACRFP group was older in age, in more advanced stage of knee OA, and clinically more severe according to the parameters of KOOS and KSS, after at least 5 years of follow-up, the satisfactory rate was significantly higher in the ACRFP group (90.64%) than in the non-ACRFP group (70.30%). The incidence of patients receiving arthroplasty was remarkably lower in the ACRFP group (4.28%) than in the non-ACRFP group (13.46%).
The satisfactory rate in our ACRFP group is not only higher than that in the non-ACRFP group, but it is also significantly higher than what was shown in a previous study which reported that the medium-term outcome (mean follow-up: 49.2 months) was poor in about 71.7% of patients with isolated Kellgren-Lawrence grade 2 (definite osteophytes and possible narrowing of joint space) 20 medial-compartment knee OA who subsequently underwent arthroscopy. 21 A meta-analysis of 30 papers for the effects of arthroscopic debridement in knee OA showed satisfactory outcomes in around 60% of all patients. The required conversion rate to arthroplasty increased as the follow-up interval increased: 1 year–6.1%, 2 years–16.8%, 3 years–21.7% and 4 years–34.1%. 1 In comparison, our data disclosed that ACRFP could modify the natural course of knee OA. The incidence of patients receiving arthroplasty in our ACRFP group was 4.28% after 5 years follow-up. According to a report investigating the likelihood of TKA following arthroscopic surgery for knee OA, 22 the annual incidence of TKA was 2.62% after arthroscopic surgery for OA and is compatible with our 5 years incidence of 13.46% in the non-ACRFP group. This conversion incidence in our non-ACRFP group is compatible with some studies regarding conventional arthroscopic management or conservative treatment. A study found that compared with conservative treatment, arthroscopy did not decrease or delay TKA in a 5-years retrospective study of 382 patients with knee OA. Of the 214 patients treated with arthroscopy, 32 (15%) eventually underwent TKA, compared with 30 of the 168 patients (17.9%) treated conservatively. 23 Another study found the incidence of TKA after corticosteroid and/or HA injections for 5 years was 13.9%. 24 A study conducted in patients who participated in a single 8-weeks multimodal knee OA treatment program consisted of five intra-articular knee injections of sodium hyaluronate, structured physical therapy, knee bracing, and patient education disclosed that TKA was performed in 22.8% of knees during mean follow-up of 3.7 years. 25
Since there is no consensus in the pathogenesis of knee OA, the efficacy of arthroscopic debridement or lavage for knee OA was disputed after publication of several randomized controlled trials and meta-analysis.4,6,7,26 The effect of these negative studies have led a trend to decrease the utilization of this procedure in patients with knee OA. 8 Besides a non-coverage Medicare determination was made in United States in 2014, 27 some national or professional society guidelines were implemented for the same purpose in other country.28–32
Our report might shed some light on the confusing and negative impression about arthroscopic treatment for knee OA. Unlike the uncertain beneficial mechanism and the diverse outcomes of common arthroscopic techniques including lavage, debridement, abrasion arthroplasty, microfracture, and autologous chondrocyte implantation (ACI) for knee OA, the concept of ACRFP has precise rationale of treatment and more beneficial, reproducible outcomes. It was developed and conceptualized according to a series of studies regarding MAP as a cause of knee OA. The outcomes of previous studies affirm that, besides eradicating the MAP, the key to a successful ACRFP is to adequately decompress the tight patellofemoral joint and maintain this appropriate tension around the patella with skillful supervised post-operative home-rehabilitation. The immediate effect of ACRFP was obtained by releasing the tension around patella caused by chronically inflamed soft tissue and by eradication of the hypertrophied and inflamed synovium that may have caused pain in these osteoarthritic knees over the medial compartment and the patellofemoral joint. Furthermore, by eliminating these stress/inflammatory responses that are the key events on the onset and progression of OA, this procedure also brings forth to long-term favorable effects as a consequence of the global improvement of the environment of the knee joint for cartilaginous regeneration. Just like the release-handcuffs effect for the repeated injured skin on the wrist, by a purposeful and timely eradication of all prejudicial factors in the degenerative knee, the jeopardized cartilage could have a chance to regenerate by its innate healing response.
There are limitations in this study. First, this is not a standard randomized controlled study. The long waiting list phenomenon might produce some bias considering the different intention-to-treat effect between groups. The ACRFP group might have higher motivation to preserve their knees according to their understanding of MAP as a cause of knee OA. Second, the compliance of doing home exercise according to our KHPO protocol by the patients in the ACRFP group was monitored by case managers. On the other hand, the patients in the non-ACRFP group were in a status of loss-of-follow-up. This difference in the intensity of medical care might have affected their outcomes. Third, the decision making of performing arthroplasty by different surgeons might have produced biases for the incidence of arthroplasty in the non-ACRFP group. Fourth, by using telephone questionnaires as the investigation method, we could not perform clinical and radiological evaluation. However, the simple and clear questionnaire designed for this study might still obtain informative outcome data. Fifth, although we have cited some publications about conventional arthroscopic surgery for knee OA for comparison, a study using conventional arthroscopic procedure as the control group would have been more convincing. All these limitations warrant more precisely designed investigations.
In conclusion, compared with conservative treatment, ACRFP could satisfy more patients with knee OA and modify their natural course by decreasing their incidence of receiving arthroplasty.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.