
Abstract
Background:
Many stroke and neuromuscular patients with paraplegia or severe hemiparesis cannot control trunk balance.
Objective:
To support the pelvis/hip of paresis patients, a new pelvic/hip support system was developed bearing a convex pressing member placed over the post-trochanteric groove, a cutaneous landmark sited on the lateral portion of the gluteus maximus muscle and indicating the posterior aspect of the greater trochanter.
Study design:
Preliminary study.
Methods:
Stance control differences in two paretic patients (Guillain-Barré syndrome and stroke sequelae) with or without post-trochanteric groove support were examined. The contact pressure on the post-trochanteric groove was examined in eight healthy volunteers using an impact force sensor. The pelvic-lumbar movement was also examined using three-dimensional motion analysis, and the gluteus muscles activity was evaluated using surface electromyography.
Results:
Without post-trochanteric groove support, total three-dimensional displacement of the sacral marker was longer in the paresis patients than in normal controls, while post-trochanteric groove support decreased this distance. Post-trochanteric groove support provided compression pressure on the post-trochanteric groove, and all subjects showed a more upright trunk position, providing more anterior pelvic tilting. Six of eight subjects showed increased lumbar lordosis. Five of eight subjects showed gluteus maximus and/or gluteus medius muscle activation.
Conclusion:
The mechanisms of post-trochanteric groove support were suggested to be spino-pelvic coordination and gluteal muscle activation.
Clinical relevance
The post-trochanteric groove is a cutaneous landmark located behind the pelvis/hip joint. Applying pressure to the post-trochanteric groove from behind pushes the trunk to adopt a more upright position, leading to improved stance control. Underlining mechanisms appear to be spino-pelvic coordination and gluteal muscle activation.
Background
Many stroke and neuromuscular patients with paraplegia or severe hemiparesis cannot control trunk balance; their trunks lean forward, and they cannot achieve single-limb support during stance, leading to difficulty in walking.1–5 Therefore, one of the major goals of rehabilitation is to make the trunk more upright and improve postural balance.1,2
Human beings efficiently maintain an upright bipedal position using three opposing spinal curves (cervical and lumbar lordosis and thoracic kyphosis) that allow efficient absorption of the loads applied to the spinal column and increase the efficiency of the spinal musculature.6–9 The pelvis is an essential structure to join the two lower limbs with the spine. The base for the spine of the pelvis is the sacral plateau. This base is more or less inclined forwards, dictates the position of curvature of the lumbar spine and consequently of the entire vertebral column.6–9 Thus, the pelvis–spine complex plays the pivotal role in maintaining postural balance.
An orthotic approach for pelvic–hip stability has also been studied. Patients with paraplegia or severe hemiparesis showing instability of the pelvis, hip and knee are thought to meet the indications for hip–knee–ankle–foot orthoses, which provide maximal stability and avoid collapse of the weaker hip joint and leg. 10 By relying on the support of the brace, however, the patient lacks knee flexion and pelvic movement, resulting in the adoption of abnormal gait patterns while walking. 10 Some previous approaches using an elastic orthosis for the pelvis/hip (i.e. pelvic belt) or gluteal taping have been reported, making the trunk more upright or the hip joint extended during standing and walking.3,11 However, many paresis patients show that their pelvis/trunk lacks bearing properties,2–5 and their standing posture wobbles back and forth and around. To stabilize their standing posture, their pelvis should be supported from every direction. Previous orthoses could support laterally, but not push on the posterior of the pelvis/hip joint; it is thought that their effect on pelvis/hip joint control might be somewhat limited, especially in the anteroposterior direction.
We hypothesized that, by use of novel hip–pelvic orthoses, which could press against the bulge located behind the pelvis/hip joint and support the pelvis/hip from every direction (especially the anteroposterior direction) directly, stance control would be greatly improved. To test this hypothesis is problematic because the bulge behind the hip joint is covered with thick muscles/subcutaneous tissues and forms a convexity, so that the part of the orthosis exerting pressure could not adapt to the bulge. Therefore, we took note of the post-trochanteric groove (PTG), a cutaneous landmark sited on the lateral portion of the gluteus maximus muscle and indicating the posterior aspect of the greater trochanter (GTr) (Figure 1). The PTG is traditionally known in the field of prosthetics/orthotics, but not in the anatomical, neurological and rehabilitation fields.2,10,12 The PTG region is located diagonally behind the hip joint and has a concave shape, so that an orthotic appliance to press the pelvis/hip posteriorly can fit in the buttock. Thus, we developed a new pelvic/hip support system from the perspective of the PTG. In the present preliminary study, it was confirmed that the PTG support imparted a force that affected trunk control in two paresis patients and eight healthy volunteers. This article shows, for the first time, the importance of the PTG in maximizing effects on stance control through pelvis/hip joint movement.
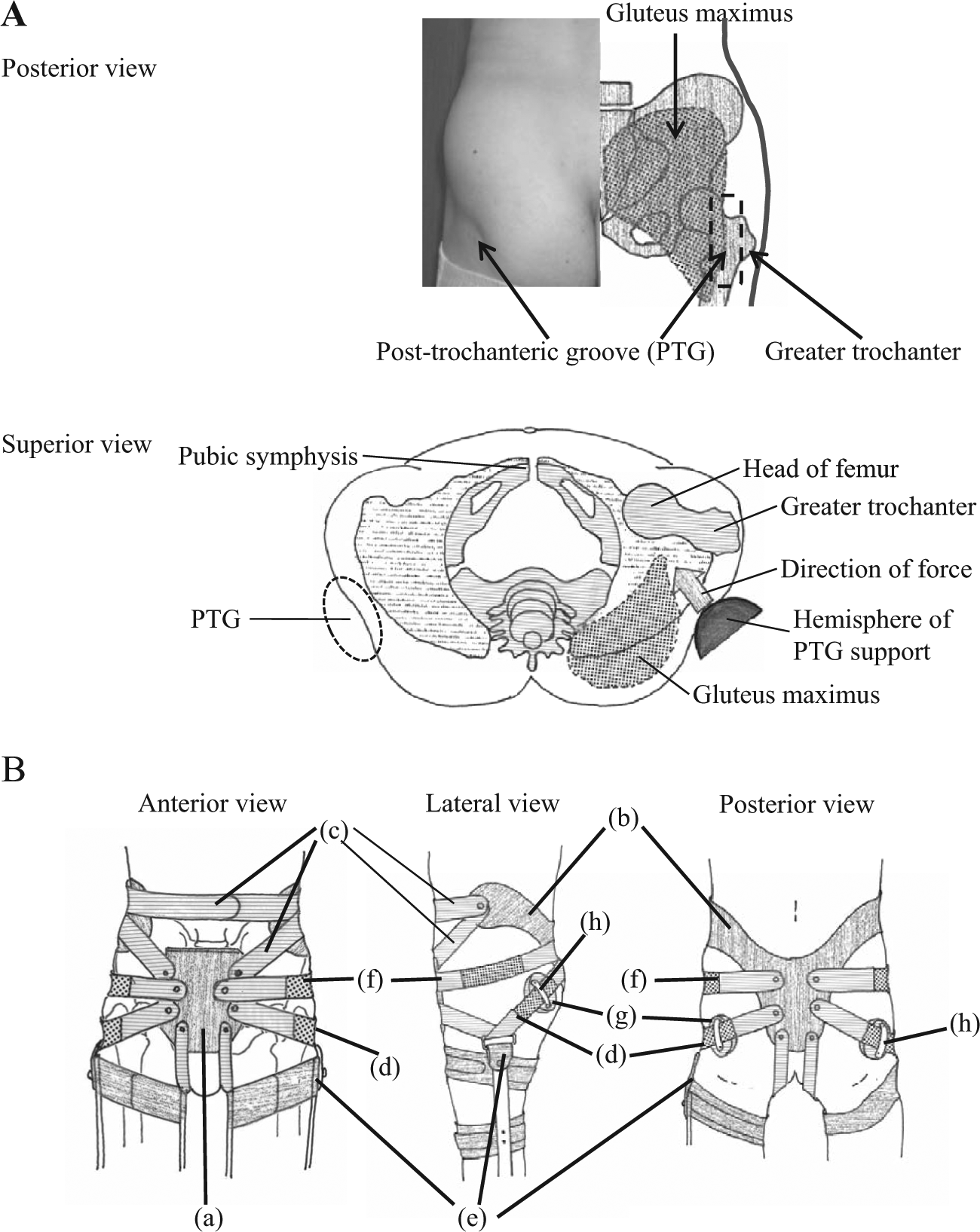
(A) Posterior and superior views of the gluteal area. The PTG is located on the lateral side of the gluteus maximus, posterior to the greater trochanter. The force of the PTG support is expected to be oriented obliquely forward to the hip joint. (B) Anterior, lateral and posterior views of the pelvic corset with PTG support. This system consists of anterior ((a) covering the pubic symphysis) and posterior plastic corset panels ((b) bordering the iliac crest and gluteal fold) that can be adjusted using (c) Velcro belts placed at the side and front. Two latex bands are also attached, providing support to the PTG from behind ((d) PTG support encompassing the hip joint between the iliac pad and PTG, (e) curving up over the upper part of the KAFO or the cuff belt of the upper thigh and (f) then passing up the anterior aspect of the hip joint and over the pubic pad) and (f) laterally). To provide forward-directed forces, we place (g) a hemisphere over the PTG (PTG support). The Velcro belt for PTG support contains a latex band and passes through (h) a belt loop attached to (g) the hemisphere.
Methods
Subjects
Institutional ethics committee approval was obtained for this prospective study. Written informed consent was obtained from all participants (both patients and healthy volunteers) prior to enrolment. A man in his mid-40s with paraplegia (manual muscle testing (MMT): flexion/extension power of bilateral hip muscles, 2; knee, 1; ankle, 0) due to Guillain-Barré syndrome (GBS) and a man in his mid-60s with severe left hemiparesis following stroke (Brunnstrome stage: upper limb/fingers, 1; lower limb, 2) participated in this study. Five men (mean age, 41.6 ± 10.0 years) participated as normal controls for the stance control study.
The subjects of the second study to examine the effect of PTG support on pelvic tilting, trunk-lower limb angle, muscle activity and stance control in the static standing position were eight healthy volunteers (six males, two females; mean age: 28.7 ± 7.2 years, mean height: 170.4 ± 5.6 cm, mean weight: 65.5 ± 9.4 kg).
Pelvic/hip corset with PTG support
In the present study, instrumented stance/gait control analysis was performed with or without backward support for the PTG (Figure 1). A pelvic/hip corset in this study consisted of anterior (covering the pubic symphysis; Figure 1B (a)) and posterior plastic corset panels (bordering the iliac crest and gluteal fold; Figure 1B (b)) that could be adjusted using Velcro belts with (Figure 1B (d)(f)) or without (Figure 1B(c)) latex bands placed at the side and front. To provide forward-directed forces that could control backward motion of the hip joint in the subjects, a pressing member (device) was placed over the PTG (PTG support) (Figure 1B (g)). To apply a force onto the PTG effectively, the pressing member forms a convex prominence. In this study, the configuration of the pressing device of the PTG support had a spherical surface, and its consistency was similar to that of a hard ball so that it would be suitable for taking measurements of contact pressure. The force on the PTG was regulated by changing the shape and consistency of the device. This pressing member over the PTG was attached with a latex band (Figure 1B (d)), which encompassed the hip joint between the iliac pad and PTG, curving up over the upper part of the knee–ankle–foot orthosis (KAFO) or the cuff belt of the upper thigh (Figure 1B (e)), then passing up the anterior aspect of the hip joint and over the pubic pad.
Assessment of standing balance in paresis patients
To characterize balance during quiet standing for the two patients, displacement of a reflective marker attached to the sacrum of each participant was calculated as the range of anteroposterior, mediolateral and three-dimensional (3D) excursions (cm) during five repetitions of a 10-s stance trial using a Frame-DIAS II 3D motion analysis system (DKH, Tokyo, Japan). During analysis, in both patients (both sides for the GBS patient and the affected side for the stroke patient), the KAFO was attached using a spring-assisted extension (SPEX) knee joint (Advanfit, Kumamoto, Japan), which is used for the knee joint to permit knee flexion movement from 0°–60° during standing or walking and can obtain knee stability by the offset joint and constant gentle tension for corrective flexion. The two patients who could not stand independently could achieve the static standing position with minimal assistance from the anterior side.
Assessment of pelvic tilting, trunk-lower limb angle and lumbar lordosis during standing
Each healthy subject stood statically for 30 s with the feet positioned with the mid-heels 15 cm apart, and they were told to look at a fixed point ahead of them. To assess pelvic tilt, lumbar lordosis and trunk-lower limb angle, reflective markers were placed bilaterally on the acromion processes, GTr, anterior superior iliac spine (ASIS), posterior superior iliac spine (PSIS), medial/lateral knee joint space and over the prominences of the spinous processes of Th12, L3 and S1. Analysis was performed using the Frame-DIAS V 3D motion analysis system. Pelvic tilt was examined using the angle formed between the line connecting the ASIS and PSIS and the horizontal as the reference, as in previous reports.13–15
The hip joint centre was calculated using the method of the clinical gait analysis forum of Japan (http://gait-analysis.jp/) modified by Kurabayashi et al. 16 They optimized each parameter of the three methods (the clinical gait analysis forum of Japan, Davis’ method and Vaughan’s method), and they were correlated with each other after estimating errors using data from 43 healthy young adult Japanese males; they concluded that the estimation errors of the revised method of the clinical gait analysis forum of Japan were minimal. 16 The standard point on the skin was placed on the line between GTr and ASIS and 27.2% interpolated from Gtr, and the hip joint was placed on the line connected with bilateral standard points (inserted at 19.7% of the distance between bilateral GTrs).
The trunk-lower limb angle was defined as that formed by the line from the hip joint centre to the acromion and the line from the hip joint centre, and the centre of the knee joint (mid-point between medial and lateral hip joint marker). Lumbar lordosis was defined as the angle that was formed by the line from Th12 to L3 marker and the line from S1 to L3 marker. Each value was calculated using the average of the middle 5 s after the start of static standing. The average of five trials in each trial was used in the following analysis.
Assessment of contact pressure with the PTG support
Contact pressure with the PTG support was assessed during static standing. The contact pressure between the skin of the buttocks and the PTG support was measured using the 65-mm-diameter, disc-shaped, impact force sensor made of a piezoelectric film (polyvinylidene difluoride (PVDF)) covered with an aluminium plate (Keisoku Support Ltd., Higashihiroshima, Japan). The sensor output was detected using Nicolet EDX (CareFusion Co. Ltd., San Diego, CA, USA). A good linear relationship between the impact force sensor output (mV) and load cell output (N) was detected (data not shown). The contact pressure was calculated from the detected output (mV) as follows: contact pressure = 2.5 × sensor output (mV).
Assessment of the surface electromyogram during standing
Surface electromyogram (EMG) recordings were taken from the right side of the subjects for the following muscles: gluteus medius, gluteus maximus and paraspinal muscles at the L1–L2 level of the spine. To record EMG activity, pairs of silver–silver chloride electrodes were placed approximately 3 cm apart along the muscle bellies. The recordings were obtained using a Nicolet EDX, amplified, band-pass filtered (5–10 kHz), sampled at 20 kHz, displayed on a computer screen, and stored for later analysis. The area under the curve (AUC) in the 3- to 8-s time (5 s) window after starting the static standing was analysed, and the ratio (per second) to that of the maximal strength of each muscle was calculated. The average of five trials in each trial was used.
Statistical analysis
The correlations of the values of each trial with and without PTG support were calculated using the Mann–Whitney U test. Values of p < 0.05 were considered significant. All analyses were performed using SPSS version 16.0 software for Windows (SPSS, Chicago, IL, USA).
Results
Stabilizing effects of PTG support on static standing in two patients
Without PTG support, the anteroposterior, mediolateral and 3D distances of sacral marker movement in the two patients (GBS and stroke sequelae) exceeded those in normal controls (Figure 2). However, the distance of sacral marker movement was decreased (but permitted some degree of hip/pelvic movement) in both patients after providing PTG support. Thus, PTG support showed a stabilizing effect on static standing for severe paresis patients.
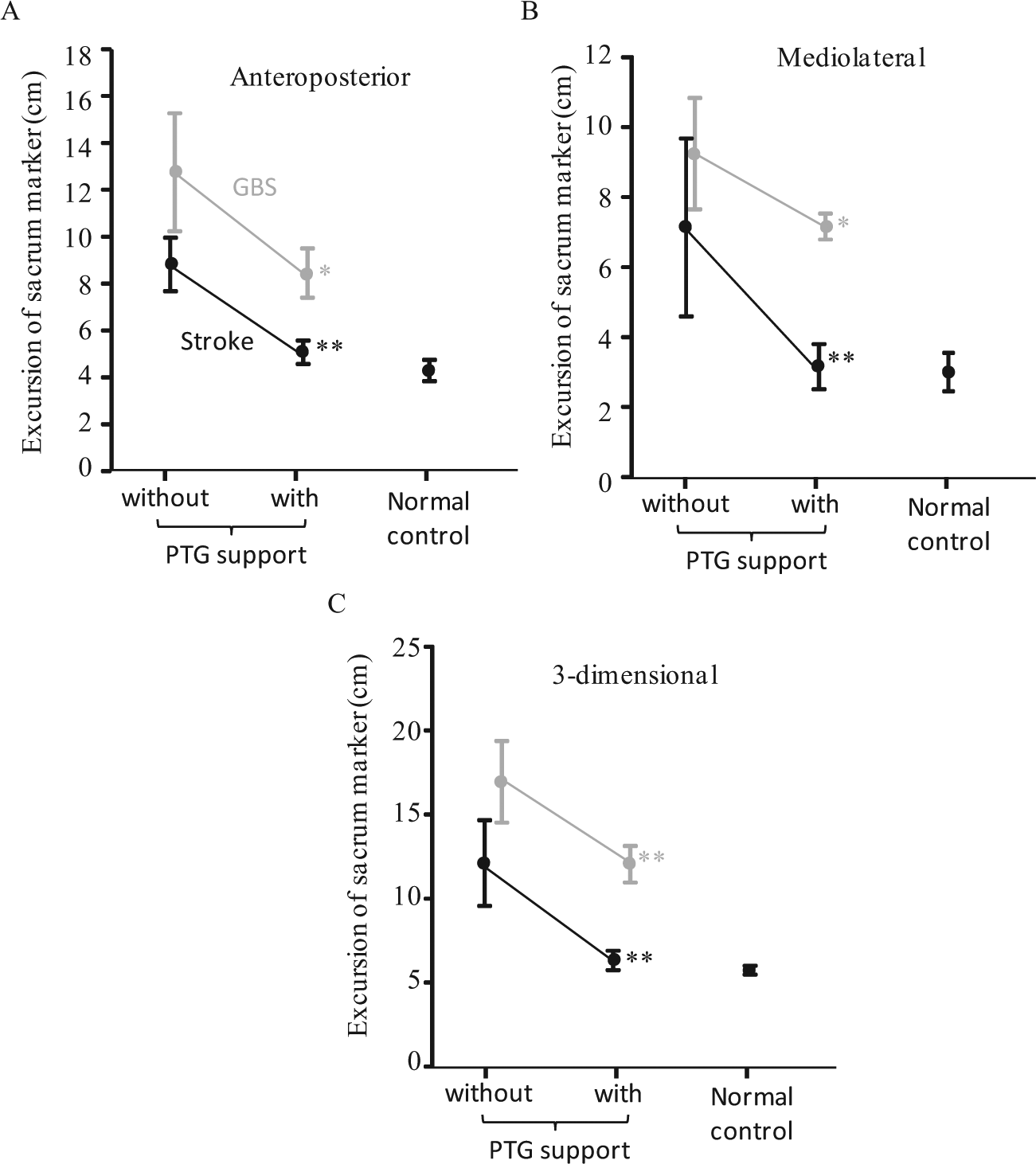
Differences in the (A) anteroposterior, (B) mediolateral and (C) three-dimensional excursions (cm) over 10-s of the sacral marker with/without PTG support were examined using a Frame-DIAS II 3D motion analysis system in two patients with severe paresis who could not sit or stand without assistance. Excursions of normal controls (all men, mean age: 41.6 ± 10.0 years) are shown on the right. The data points are given as means and 95% confidence interval. Differences in the distance of the sacral marker during quiet standing with or without the PTG support were assessed using the Mann–Whitney test. Statistical significance: *p < 0.05, **p < 0.01.
Contact pressure under PTG support in static standing
Contact pressure under the PTG support was 18.2 N ± 5.5 N (8.5 N–25.4 N) on the right side and 18.4 N ± 4.4 N (11.8 N–23.8 N) on the left side. The PTG support band was constricted with the maximum tension without causing pain or discomfort. The dispersion of the data was thought to be related to variability in individual perception.
The effect of PTG support on pelvis tilting, lumbar lordosis and the trunk-lower limb angle during static standing
All eight subjects’ data of the right trunk-lower limb angle, right pelvic tilting angle, and Th12–L3–S1 angle (lumbar angle) are shown in Table 1 and Figure 3. The left trunk-lower limb angle and pelvic tilting angle showed almost the same trend (data not shown). The trunk-lower limb angle and pelvic tilting angle were increased after wearing the PTG support in all eight subjects, indicating the trunk to be straighter and the pelvic tilting to be more anterior. The lumbar angle was decreased (lumbar lordosis increased) in six and increased (lumbar lordosis decreased) in two subjects.
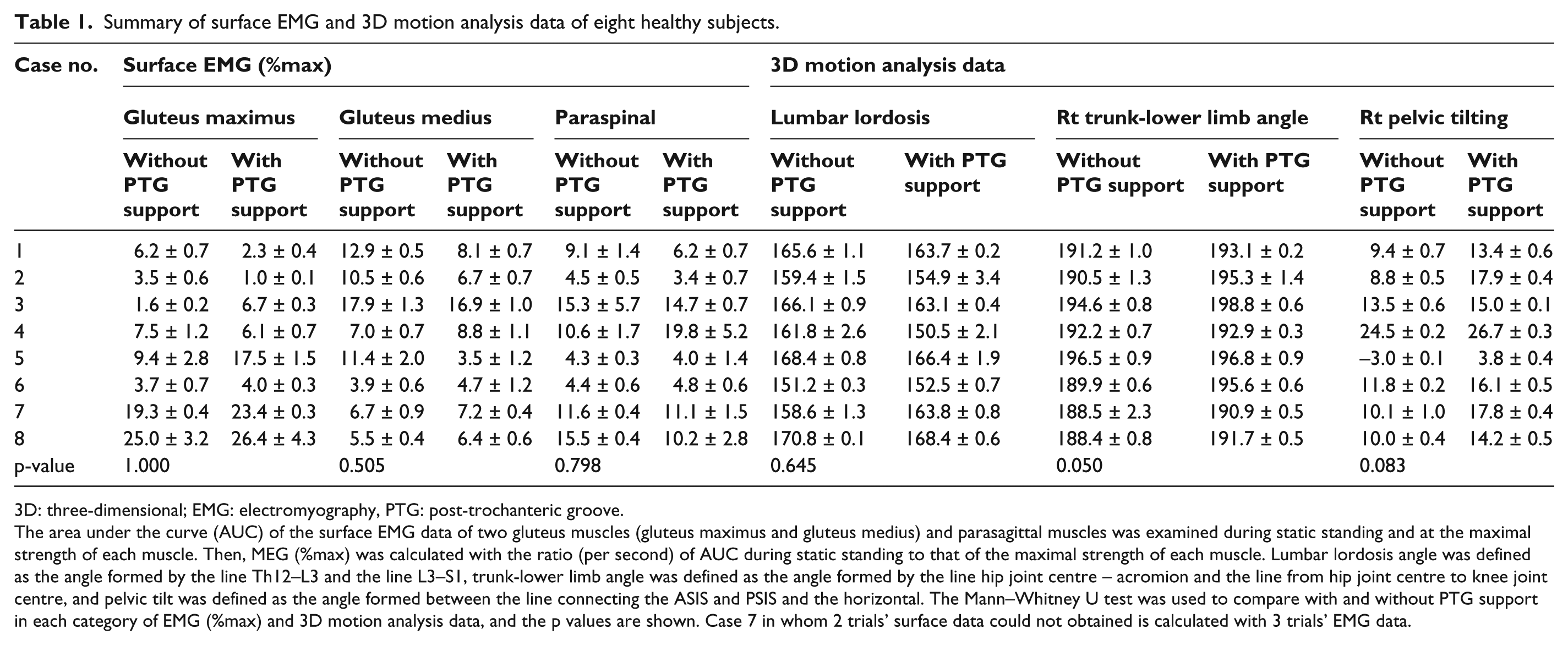
Summary of surface EMG and 3D motion analysis data of eight healthy subjects.
3D: three-dimensional; EMG: electromyography, PTG: post-trochanteric groove.
The area under the curve (AUC) of the surface EMG data of two gluteus muscles (gluteus maximus and gluteus medius) and parasagittal muscles was examined during static standing and at the maximal strength of each muscle. Then, MEG (%max) was calculated with the ratio (per second) of AUC during static standing to that of the maximal strength of each muscle. Lumbar lordosis angle was defined as the angle formed by the line Th12–L3 and the line L3–S1, trunk-lower limb angle was defined as the angle formed by the line hip joint centre – acromion and the line from hip joint centre to knee joint centre, and pelvic tilt was defined as the angle formed between the line connecting the ASIS and PSIS and the horizontal. The Mann–Whitney U test was used to compare with and without PTG support in each category of EMG (%max) and 3D motion analysis data, and the p values are shown. Case 7 in whom 2 trials’ surface data could not obtained is calculated with 3 trials’ EMG data.
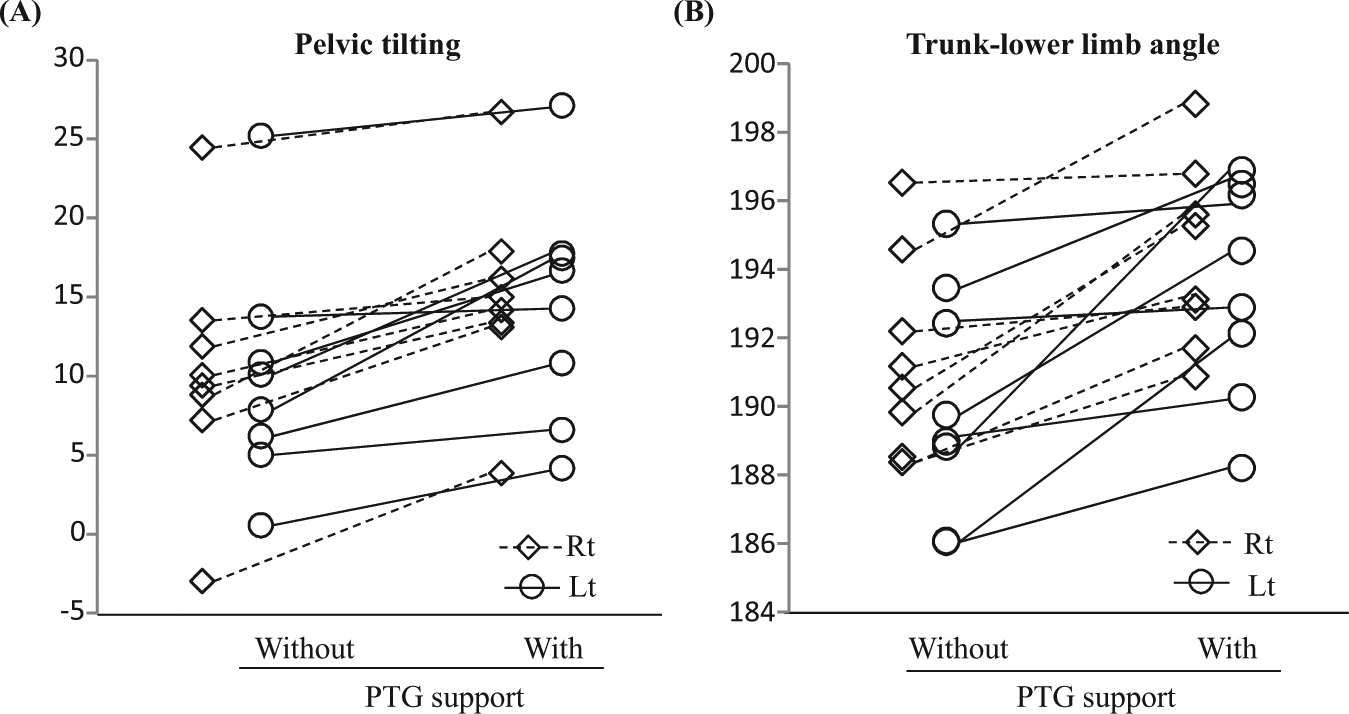
(A) Scatter diagrams show the pelvic tilting angle and (B) trunk-lower limb angle of a normal volunteer with or without PTG support. Circles represent angles on the right side, and diamond shapes represent angles on the left side.
The volunteers were of several body types (body-mass index: mean 22.5 ± 2.4, 19.9–27.4). Several persons were well-muscled (male or female) or had more soft tissue, while the novel device made their pelvis tilt anteriorly and their trunk-lower limb angle extend. Therefore, this novel device could work as well for people with more soft tissue around the PTG area.
The effect of PTG support on muscle activity
The surface EMG data of eight subjects are shown in Table 1. Two cases (cases 1 and 2) showed elevated activity in both gluteus muscles (gluteus maximus and gluteus medius), three cases (cases 3–5) showed elevated activity of one of two gluteus muscles and three cases (cases 6–8) showed no elevated muscle activity after wearing the PTG support. The muscle activity of the paraspinal muscles was decreased in six of eight cases.
Discussion
In the current study, a new pelvic corset bearing the PTG support, which is an object placed over the PTG to compress the pelvis/hip joint from behind, was developed. Two severe paresis patients showed decreased postural sway after wearing the PTG support. In the healthy subjects, PTG support provided compression pressure on the PTG, and all eight subjects showed a more upright trunk position and more anterior pelvic tilting. Six of eight subjects showed increased lumbar lordosis. Thus, the mechanism of PTG support was thought to be related to the pelvis–spine (lumbar) complex.
The spinal reciprocal curves, especially lumbar lordosis, play a role in the maintenance of an efficient upright posture in cooperation with pelvic position, especially pelvic tilting.6–9 Previous reports stated that increased anterior pelvic tilting increased lumbar lordosis in standing subjects. 6 In most pathological settings, that is, ageing or degenerative processes, however, kyphosis is increased and/or the trunk learns forward, and the pelvis compensates with retroversion around the femoral head (hip joint extended), and the lumbar lordosis is decreased.4,8,17 In the end, the pelvic retroversion and hip extension have a limit, and the patients flex the knee to maintain balance, but this postural situation is not efficient.4,8,17 To maintain a well-balanced position, it is important to coordinate pelvic tilting and lumbar lordosis.
The present data suggest that PTG support tilts the pelvis anteriorly and increases lumbar lordosis. Severe paresis patients could not keep their trunk in the right position, with their trunk and pelvis swinging together during standing. When a therapist performs standing exercise for these patients whose trunks are unstable, the therapist tilts many stroke patients’ pelvis anteriorly, but patients tend to lean their trunk forward without extending their trunk (decreasing lumbar lordosis). 2 At that time, PTG support might hold the patients’ pelvis in the right position with their lumbar lordosis increased. Therefore, it is thought that the present data of severe paresis patients showed that PTG support decreased their postural sway during static standing.
On the other hand, in the present surface EMG study, six of eight subjects showed their gluteus maximus muscle, gluteus medius muscle, and/or paraspinal muscles to be activated after wearing PTG support. Therefore, some mechanisms other than the pelvic–spinal system might contribute to the effect of PTG support. Kilbreath et al. 3 reported that gluteal taping on the affected side improved hip extension during the stance phase of walking for persons following stroke. In their study, the stroke patients’ trunk showed a forward lean, but the trunk was more upright after gluteal taping, as in the present study. 3 They hypothesized that the mechanism underlying the gluteal taping is an activation of gluteal muscles under the taping as follows: (1) muscle fibres were stretched, increasing the overlap between the actin and myosin filaments, and activating the muscle directly3,18 and (2) cutaneous stimulation or proprioceptive acuity through the pull of the tape on the skin activates the muscle indirectly.3,19–21 Following their hypothesis, our PTG support presses on the gluteal muscles, and the activities of these gluteal muscles might be elevated directly or indirectly (cutaneous stimulation or proprioceptive acuity).
Several methodological limitations of this study require acknowledgement. This study was preliminary, and the sample size was extremely small; therefore, the results require replication in a larger sample. Next, excessive curvature of lumbar lordosis applies mainly posterior forces on the facet joints, which is an important cause of pain, and probably accelerates arthrosis changes.7,8 In some cases, this posterior force is a main predisposing factor for sliding degenerative spondylolisthesis.7,8 Thus, we should pay attention to the possibility that anterior tilting and lumbar lordosis might be made worse in some cases. Last, the mechanisms underlying the effects of PTG support on the stance control system remain unclear, and further biomechanical research into PTG support systems is needed before practical application on a wider scale.
Conclusion
The present preliminary study showed that PTG support provides compression pressure on the gluteal region (diagonally backward from the hip joint) in the forward direction and makes the trunk more upright. Two mechanisms of PTG support were suggested: (1) pelvic anterior tilt leading to increased lumbar lordosis (spino-pelvic coordination) and (2) elevated gluteal muscle activation directly or indirectly. The PTG has not previously been described in the anatomical, neurological or rehabilitation fields,2,10,12 and this study is the first to focus on the PTG in terms of its beneficial effects for standing.
Footnotes
Acknowledgements
Patents related to the subject of this study are now pending in USA, and issued in Japan and China (WO2009/144877). The authors would like to thank Dr. Sumiko Yamamoto for her helpful comments, and Drs. Shigeto Yamawaki, Hidehisa Yamashita, Kaoru Kurisu, Hitoshi Sato, Seiichiro Hibino, Jyunichi Kanazawa and Masuki Kobayashi for their data analysis and valuable discussions. The authors are also grateful to the staff members of the Department of Rehabilitation at Hibino Hospital and Hiroshima University Hospital, and Ohtsubo Prosthetics & Orthotics MFG for their technical assistance.
Author contribution
Seiji Hama – development of PTG support, data analysis and write this manuscript; Masafumi Otsubo – development of PTG support and preparation of this manuscript; Tsuyoshi Nishiwaki – collaborate of data analysis and preparation of this manuscript; Ayu Miura – collaborated with data analysis; Mie Sanemasu – data collection and analysis; Noboru Shimada – data collection and analysis; Yukio Fujimoto – data collection and analysis of biomechanical findings; Takahiro Suzuki – data collection and analysis; Saori Tao – data collection and analysis; Daisuke Hara – data collection and analysis; Shiori Kawahama – data collection and analysis; Eriko Iino – data collection and analysis; and Daisuke Sato – data collection and analysis.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Tsuchiya Foundation, funding from the Chugoku Industrial Innovation Center and funding from the collaborative project of Hiroshima University with Urabe Co. Ltd. (A1100574) and with Corporation Pearl Star Co. Ltd. (A1000412).