
Abstract
Background:
Education of Prosthetics and Orthotics is a relatively recent professional program. While there has been some work on various teaching methods and strategies in international medical education, limited publication exists within prosthetics and orthotics.
Objectives:
To identify the teaching and learning methods that are used in Bachelor-level prosthetics and orthotics programs that are given highest priority by expert prosthetics and orthotics instructors from regions enjoying a range of economic development.
Study design:
Mixed method.
Methods:
The study partly documented by this article utilized a mixed method approach (qualitative and quantitative methods) within which each phase provided data for other phases. It began with analysis of prosthetics and orthotics curricula documents, which was followed by a broad survey of instructors in this field and then a modified Delphi process.
Results:
The expert instructors who participated in this study gave high priority to student-centered, small group methods that encourage critical thinking and may lead to lifelong learning. Instructors from more developed nations placed higher priority on student’s independent acquisition of prosthetics and orthotics knowledge, particularly in clinical training.
Conclusions:
Application of student-centered approaches to prosthetics and orthotics programs may be preferred by many experts, but there appeared to be regional differences in the priority given to different teaching methods.
Clinical relevance
The results of this study identify the methods of teaching that are preferred by expert prosthetics and orthotics instructors from a variety of regions. This treatment of current instructional techniques may inform instructor choice of teaching methods that impact the quality of education and improve the professional skills of students.
Keywords
Background
Previous results 1 indicated regional differences in Bachelor’s level professional preparation within a common commitment to objectives-based programming. There was variation in both theoretical and practical teaching methods mentioned in curricula accessible from different university websites, and later expert consultation revealed concern as to whether the approaches now being followed worked against the objectives of the programs. Prosthetics and orthotics require students to develop both technical and practical skills to enable them to fabricate various devices for a variety of clients. Consequently, the mix of teaching methods employed within prosthetics and orthotics education may differ from other forms of health and rehabilitation science education. This article further analyses regional differences in preferred teaching methodology in prosthetics and orthotics and may prove interesting and useful for other allied health programs.
Overall, review of the literature indicates the importance of linking the study of curriculum development to the educational approaches chosen to deliver that curriculum. Biggs 2 considered that effective professional preparation required that presage (combination of previous student knowledge and ability), process (active learning of students), and product (the outcomes of these required activities) should be aligned within teaching and assessment. That is, what students already know should be considered when teacher expectations are being formulated, learning experiences should be designed to encourage student achievement of those expectations, and assessment should evaluate the extent to which such achievement occurs. Contrary to some interpretations of it, this notion of alignment pays significantly more attention to process than it does to product 3 and this signals the importance of instructor choice of teaching strategy in effective curriculum implementation. The priority that other expert instructors place on particular methods may inform such choice.
Education in prosthetics and orthotics calls for a combination of theoretical and practical teaching from medicine and engineering and application in clinical training. 4 However, education in this field is now moving beyond the undergraduate years and this seems an appropriate time to investigate current teaching, learning, and assessment methods. Some such work has already occurred within medicine, nursing, and physiotherapy.5,6 Baozhi and Yuhong, 7 for instance, reported a comparative study of Chinese and American medical schools under the supervision of China Medical Board in New York, which revealed diversity between different categories of courses and divergent teaching and learning styles and varying use of small group discussion, Problem-Based Learning (PBL), and more traditional tutorial teaching. A study 8 seeking to provide a framework as a model for European dental education found similar diversity in courses and methods for teaching them. Interest in teaching and learning methods may increase under the impact of internationalization and some 9 have suggested that combining evidence-based approaches with effective teaching and learning would improve student learning and develop increasing competence.
Many studies have suggested small group learning (and PBL, in particular) as possibly more effective alternatives to traditional lecture/tutorial patterns of instruction 10 that may smooth the way to an evidence-based practice (EBP) approach in clinical education. 11 PBL was first applied to medical education at McMaster University in 1965 and its group research-based approach to student learning seems a natural fit with contemporary attempts to decrease the gap between potentially conservative clinical practice and the increasingly rapid growth of knowledge through EBP. However, adoption of such approaches remains problematic. 5 Loyens et al. 12 explained that the PBL environment increases student collaboration, self-directed learning, and problem-solving skills. They added, however, that there is less evidence to vindicate the impression that PBL improves the factual knowledge of students. Their study also showed no significant difference in motivation between students in PBL and traditional programs. 12 Many authors indicated the success of PBL in clinical settings but noted that it is more problematic for student learning of basic science in medical education. 13 The experience of tutors proved crucial to the success of such PBL groups but, not withstanding such success, there was no significant difference in student science knowledge between PBL and traditional approaches. Such concerns about PBL raise the question of the priority given to it by expert prosthetics and orthotics instructors, among the other teaching methods available to them.
These other teaching methods include more recent approaches to learning, such as e-learning. 14 Institutional use of new technology often involves providing student access to Learning Activity Management Systems (LAMS). LAMS can merely replace distribution of paper documents and reading lists in support of traditional patterns of lecture, tutorial, and workshop or they can provide a framework for learner-centered approaches where teacher, learner, and staff encourage collaboration and communication by means of the new technology. 14
This article is a part of a wider comparative international study of prosthetics and orthotics curricula and educational programs, and reports an investigation of instructor priority given to current teaching and learning methods in prosthetics and orthotics programs at the Bachelor’s level. Which strategies do expert prosthetics and orthotics instructors prefer and how do they manage clinical, practical, and theoretical classes in this field? The answers to such questions are a necessary precondition for the development of suggestions for sustainable improvements.
Methods
The results reported in this investigation come from a wider study that utilized mixed methods across a three-phase design. The study began by collecting international prosthetics and orthotics curricula, analysis of which informed development of a widely distributed Web-based survey in 2007, analysis of which in turn informed a consensus-building Delphi study in 2009.
Phase 1 was a qualitative analysis of curriculum documents. Invitation and consent forms were sent by electronic mail to the head of the prosthetics and orthotics departments in the 26 institutions for which a contact person was identifiable. A total of 10 Bachelor-level prosthetics and orthotics programs from various regions returned their full curriculum documentation or allowed us deeper access to their curricula on university websites. Institutions that responded came from Europe, the Middle East, North America, Oceania, and South Asia. Seven of these respondents offered a 4-year full-time program and the remaining three programs were completed in 3, 3½, and 4½ years.
An initial questionnaire had been developed on the basis of review of the literature, similar previous studies, results of the first curriculum analysis phase, and an existing instrument.5,11,15 The initial questionnaire was modified after a pilot study and then distributed to form the basis of Phase 2 of this investigation. The questionnaire included both 5-point Likert and free response items.
The questionnaire was sent by electronic mail to the 21 institutions that had not explicitly declined to be involved, with the request that it be distributed to instructors in prosthetics and orthotics. A total of 47 surveys were returned by 14 institutions in 10 nations from Oceania, South Asia, the Middle East, Northern Europe, and North America. The nations within these regions differed in terms of economic development. While 14 surveys were returned from developed countries, 33 were returned from developing countries.
The frequency of individual responses was calculated and Chi-square was applied to identify curriculum elements that were common to various institutions (Chi-square > 0.05) and those which were distinctive between them (Chi-square < 0.05). Chi-square was considered to be an appropriate test of the existence of differences worth comment because Likert scales resemble the categorical variables for which the test was designed. 16 Differences between the frequencies which survived this more conservative test yielded group means that could be usefully examined further with parametric measures.
Phase 3 of the study consisted of several Delphi rounds, based initially on the results of the Phase 1 analysis and Phase 2 survey. Participants came from universities that had participated in Phase 2 after being identified in Phase 1 and having their prosthetics and orthotics programs analyzed. The responses to the Phase 2 survey were analyzed to yield the statements comprising the initial Phase 3 instrument, which were arranged into a more contentious set of issues and a further set which appeared to have already achieved a high degree of consensus. Each item was made up of a 6-point Likert item (from 1 = reject to 6 = strongly agree) and space for participants to add explanatory detail. Following precedents from the literature,17,18 this was sent electronically to a panel of 14 experts from 7 institutions from the same regions as the previous phase of the investigation. Baker considers knowledge and experience to constitute expertise, 19 and thus expert was defined as possession of a higher degree or a Bachelor’s qualification in prosthetics and orthotics, followed by at least 5 or 10 years’ teaching experience in this field, respectively. Respondent opinions about the statements making up the initial instrument were fed back to panel members through additions made before the final round. Analysis of patterns of response distinguished between “acceptance,” “agreement,” and “consensus.”
Expert acceptance of any statement on the Delphi instrument is given by the median score for the 6-point Likert item. For instance, a median of 2 would indicate low acceptance, while a median of 6 would represent high acceptance by this group of expert prosthetics and orthotics instructors. However, merely considering any measure of central tendency in isolation could wash out differences between the opinions of these experts. So, Likert responses were paired (1–2, 3–4, 5–6) to allow distinction between “acceptance,” “agreement,” and “consensus” (Table 1).
Levels of acceptance and agreement for each item.
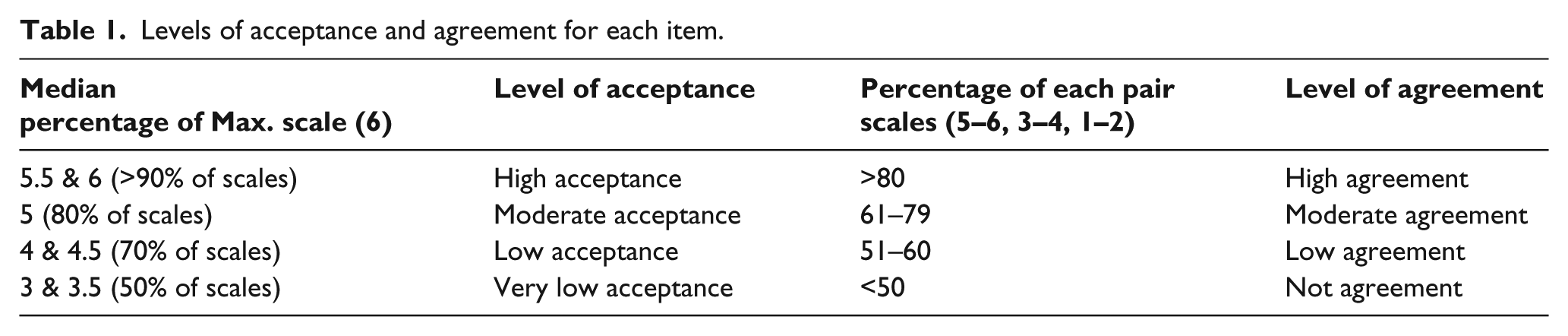
Expert agreement with any statement on the Delphi instrument is given by the percentage of respondents who selected each pair of points on the 6-point Likert scales. This indicates the distribution of responses more finely. For example, an item median of 5 shows high expert acceptance of a statement but lower agreement would be indicated when a substantial percentage of respondents chose one of the lower pairs of Likert points, such as 3–4.
Consensus is the interaction of acceptance and agreement. For example, an item median of 5 was taken to indicate high acceptance of the proposition; 80% respondent choice of the 5–6 pair was taken to indicate high agreement and these two values would interact to indicate high consensus. An item median of 2 with 50% respondent choice of the 3–4 pair would indicate low acceptance and low agreement and also low consensus. In the former case, most of the expert prosthetics and orthotics instructors agreed in accepting the proposition, while in the latter they were less certain about rejecting it.
This article reports analysis of all three phases of the wider study. It discusses the teaching methods revealed by Phase 1, suggested in Phase 2 and preferred by instructors from participating institutions in Phase 3. The Delphi phase allowed expert instructors to explain their own preferences. The results allow instructional patterns in different regions to be distinguished. This study design has echoes of triangulation strategies. Figure 1 indicates how the phases built on each other, the results of each phase providing the basis for the next.
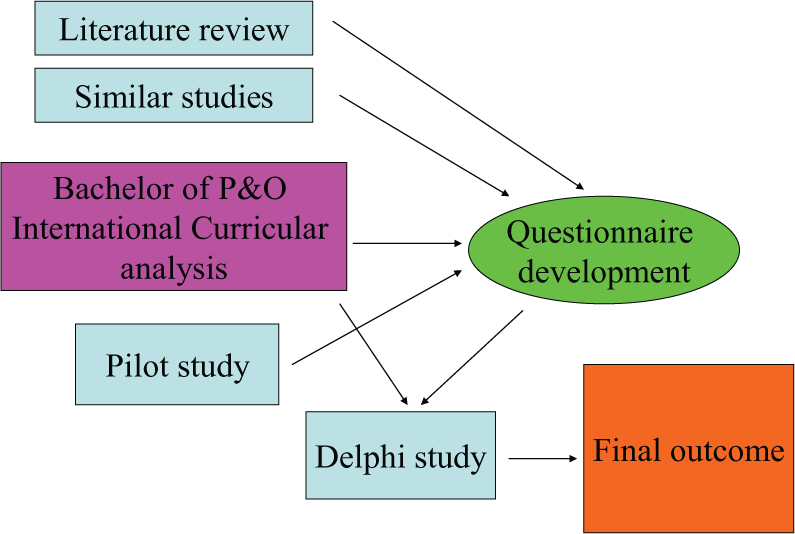
Overall design of study.
Results
Phase 1 of this investigation indicated that theoretical, practical, and clinical teaching contexts are common across prosthetics and orthotics programs, with some variation in the teaching methods used in different contexts.
Lectures remain the most popular method for teaching theoretical material across these programs (6 out of 10, drawn from the Middle East, South Asia, North Europe, and Oceania regions). Responses suggested that student participation in discussion of the subject’s main elements were being motivated by the lecturer. One program from Oceania apparently supported lectures with detailed information on class websites and multidisciplinary group work toward presentations in tutorials. Several programs (4 programs out of the 10, drawn from Northern Europe and North America) indicated that they considered students to be responsible for developing their own knowledge in prosthetics, orthotics, and related sciences. These universities specified student-centered strategies, such as problem solving, to motivate critical thinking, in-depth learning and understanding, and lifelong learning in students. Two programs from North Europe specified PBL, stating that they used it in an attempt to encourage the students to independently acquire the latest knowledge and express their own findings and opinions to other peers through presentation and seminar sessions.
The second, survey phase of the wider study allowed more specific insight into the teaching methods that were common across the institutions and others that were more distinctive. Table 2 shows instructor responses to prompts regarding the use of specific teaching strategies in teaching theoretical material. The Chi-squared statistic on Table 2 indicates no significant difference between instructors from developed regions (Oceania, Northern Europe, and North America) and those from developing ones (South Asia and the Middle East). The number of responses in the “Strongly disagree” was extremely small and those responses have been consolidated into “Disagree” on the following tables. The instructor responses in Phase 2 reflect some unease with the results of the documentary analysis from Phase 1. For example, Phase 1 indicated considerable use of lectures but Phase 2 suggests that instructors are ambivalent about this, with almost twice as many doubting its effectiveness.
Strategies for teaching theoretical classes (based on Phase 2 survey).
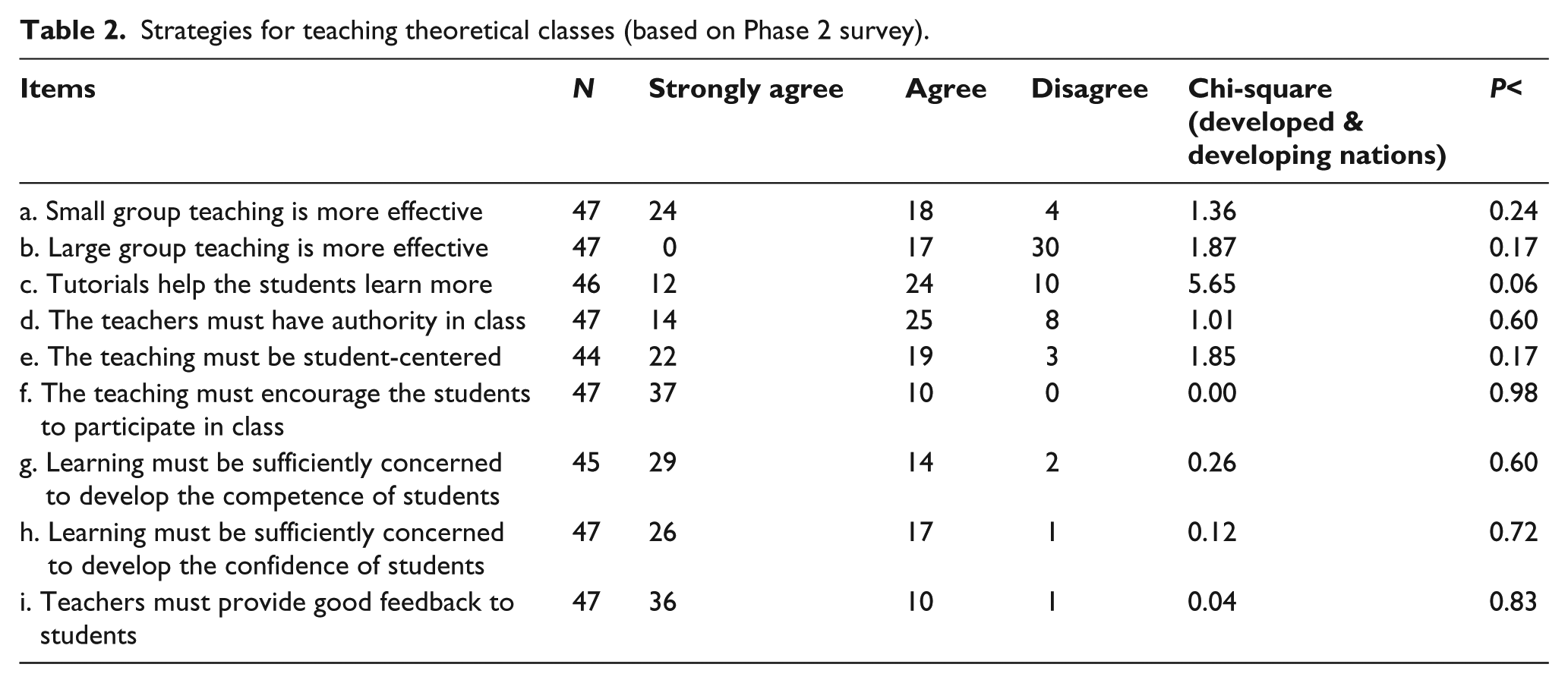
The more illuminative results of the Phase 3 Delphi study indicated more support for large group teaching of theoretical material (Item b on Table 2). There was only moderate consensus in viewing it as less effective than other approaches (Median = 5 and Agreement = 61.5%), although one expert instructor commented that this method “is good for giving the basic, small groups for developing individual skill set.” This position garnered slightly more agreement (Median = 5 and agreement = 69.2%), but there was a higher consensus regarding the importance of small group teaching (Median = 5 and Agreement = 84.6%) among these Delphi participants.
Phase 1 indicated that prosthetics and orthotics programs usually apply similar methods for teaching the technical part of prosthetics and orthotics in practical and clinical classes. These include observation, workshop practice, laboratory and online practical education, and clinical training. The initial curriculum analysis indicated that most (7 out of the 10) included observation of clinical and workshop practice and site visits in their programs, but such observation differed in purpose and form. Three programs from the Middle East and South Asia placed emphasis on student process diaries and another asked that they record their analysis of the design and fabrication process. Two programs from North Europe claimed to use workshop subjects to motivate students to ask questions about the profession and society and to develop their professional curiosity and critical thinking.
Almost all programs involve student workshop manufacture of prosthetic and orthotic devices. However, two programs from North Europe and South Asia require that students record everything that they do during this period in their workbooks, and one program from North Europe emphasizes quality assurance and seeks to develop student skills through EBP. Table 3 provides more details extracted from the survey study and indications of difference between programs located in developed and developing nations.
Strategies for teaching practical classes (based on Phase 2 survey).
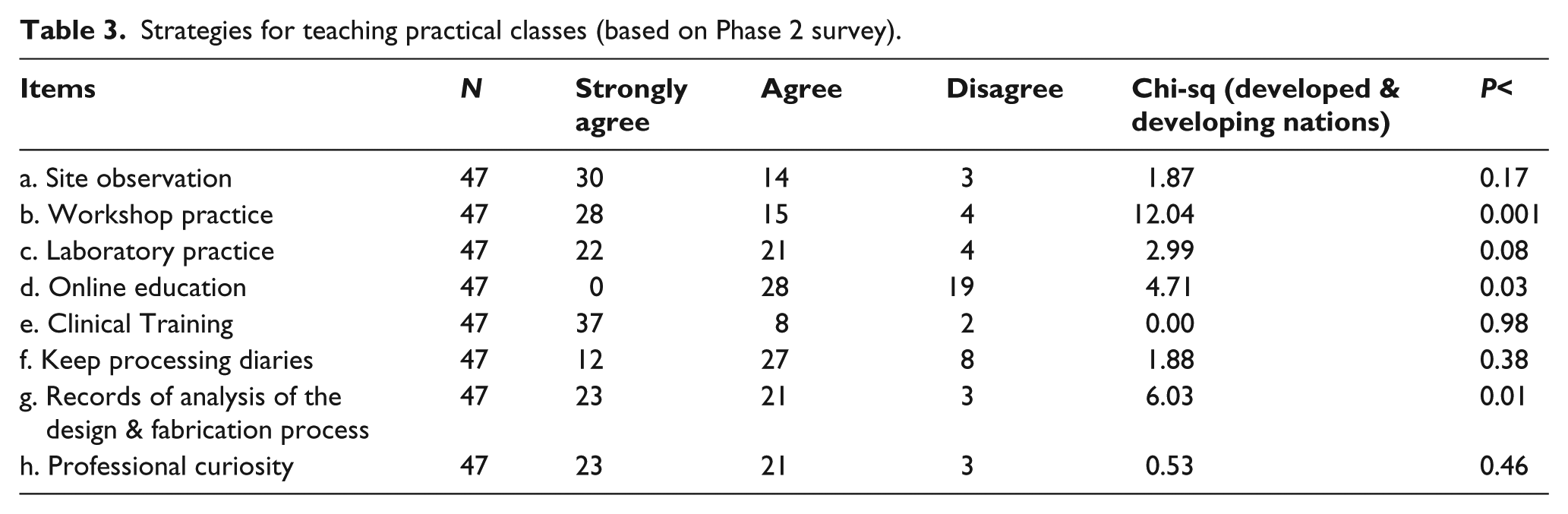
Table 3 indicates that instructor response regarding the teaching of practical material varied according to the level of development of the region within which they worked (see Items b, d, and g). Instructors from developing countries placed more stress on workshop practice, records of analysis of the design and fabrication process, and online practical education than developed nations.
Although the panel of experts in the Delphi study agreed that clinical training is one of the most important parts of practical teaching (Acceptance = 6 and Agreement = 84.6%), “Site observation” could not achieve even moderate consensus (Acceptance = 5 and Agreement = 58.3%). There was moderate agreement with the importance of both workshop practice and laboratory practice (Acceptance = 5 and Agreement = 76.9% for both) and results from the expert panel reiterated the Phase 2 regional variation regarding online practical education (Acceptance = 4 and Agreement = 53.8%).
Clinical training provides students with direct contact with clients, so it is unsurprising that all documentation placed stress on independent student positive interaction with patients during clinical training. Moreover, clinical training provides an opportunity for students to integrate scientific subjects and the theory of prosthetics and orthotics with practice as they evaluate their practical experience in real environments. Clinical placement may be seen as the most important part of prosthetics and orthotics education and it exists in all programs, in various forms, and for differing lengths of time. The results of Phase 1 of this study showed that half of 10 programs allocate either their final year or final half year to clinical placement. Such placements may divide prosthetics from orthotics or combine both. However, there did not appear to be general consensus across the 10 programs regarding the appropriate time for beginning clinical training. Table 4 shows the results of responses to Phase 2 questions regarding this important issue.
Strategies for teaching clinical training (based on Phase 2 survey).
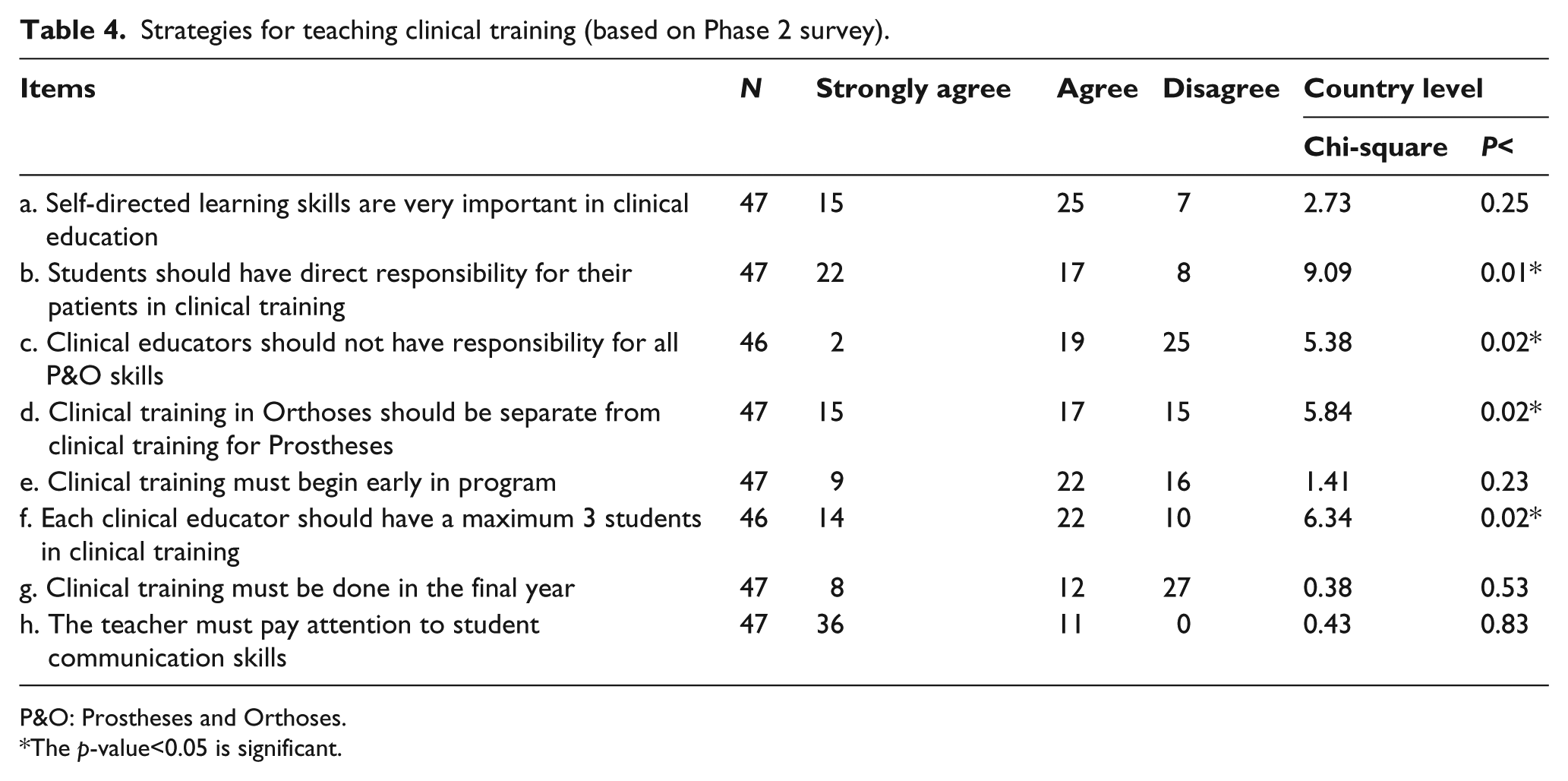
P&O: Prostheses and Orthoses.
The p -value<0.05 is significant.
Instructors from developing nations more strongly favored increased student responsibility for their patients. This group of instructors also preferred increased educator responsibility (see Table 4). It seems that instructors from more developed nations more strongly emphasize student responsibility for independently acquiring clinical skills. The results of the Delphi phase showed that most expert instructors agreed that students are responsible for their own learning and development of their professional skills, but this remains problematic as the item could only achieve moderate acceptance and agreement (Median = 5).
Similarly, instructors from developing countries (78.8%) favored separation of clinical training in prosthetics from orthotics clinics, but 57.1% of instructors from developed countries did not agree. There appears to be a lack of consensus between instructors from institutions in regions with different degrees of development. These differences fall into areas of student responsibility for their own learning, use of PBL, function of workshop practice, and clinical placements (the role of online resources, responsibility for clinical supervision, and separation of prosthetics from orthotics placements).
Discussion
Each program employed different strategies, approaches, and methods to teach the essential disciplinary sciences. Teacher-centered strategies for teaching theoretical material emerged more positively from this study than may have been expected. Lectures may be supported by other approaches, such as class websites, tutorials, group work, presentations, and multidisciplinary group working, to form a blended teacher-centered approach. 8 There has, nonetheless, been some apparent movement from traditional lecture-based, teacher-centered practices to more interactive student-centered approaches within prosthetics and orthotics programs, although only moderate consensus was achieved in the Delphi study concerning teacher-centered approaches as being less effective. Such student-centered approaches appear to be widely advocated within allied health education, as some authors indicate that students in a PBL program read more text books and more library resources and texts are needed than for traditional programs.12,20 This approach might be an appropriate response to rapid technological and healthcare changes and increase the competency of students in the domains of critical thinking, technical, and communication skills. 21 However, the number of prosthetics and orthotics programs which employ student-centered approaches appears small. Greater consensus emerged during the Delphi study, but this may be a response to reports of its effectiveness. 22 These expert instructors do not appear to be confident about the impact of PBL on learning outcomes and this echoes ambivalence within the literature.12,15,20,23 It may be that the expertise of these instructors did not extend to experience with PBL. This limitation of the study could be overcome by deliberate recruitment of expert instructors with experience of the approach, although the reticence of this group may reflect a wider attitude. However, that would be a useful topic for a later study.
This panel of expert instructors agreed that client contact at the beginning of study may motivate the students to better understand theoretical subjects, as Manogue et al. 8 earlier recommended for dental students.
Instructors from developing countries paid greater attention to workshop practice and online practical education than instructors from developed nations. They were also much more positive about the possibilities of online practical education for practical teaching in their nations, in line with some other authors who believe that online education is useful for students. Somewhat surprisingly, instructors from developed countries were less enthusiastic.24–26 Consensus was not achieved about the use of online practical education for better understanding of practical courses during the Delphi phase, which revealed a similar range of views concerning the use of computer software. Although it seems to be a feature of many programs, the majority of instructors accepted this method only for instruction in practical skills previous to real practice, stating that clinical activity and client contact have more impact than the virtual environment. However, instructors from developing countries relied more on student-produced records than did those from developed nations, which may be related to low numbers of patients for practical training and the consequent need for students to write and review reports of their own practical activities.
Professional curiosity forms a foundation for self-directed learning, which is necessary for clinical training and student problem solving during patient management. Clinical training was considered very important as a practical teaching method and observation from sites followed it in terms of instructor priority. The students have direct contact with clients and responsibility to manage the patients during clinical training, and clinical educators may employ various learning strategies, such as solving problems and encouraging lifelong learning. Problem solving may lead to EBP, which is seen by some as one of the most important issues to emerge in rehabilitation. 27 Other prosthetics and orthotics authors have suggested that curricula and assessment methods should be modified to train the students for critical thinking, which will be useful either in making appropriate decisions in clinical practice or in responding to rapid changes in information.28,29
The results show that instructors from more developed nations more strongly emphasize student responsibility for independently acquiring clinical skills than those from developing nations. The results of the Delphi phase also showed that most experts agreed that students are independently responsible for their own learning and development of professional skills. Instructors from developing nations may prefer to educate their students in their university, under the closer supervision such a location allows, instead of during clinical training which happens off campus and with associated problems of quality control.
There were some limitations to this study, such as institutional policies that prohibited access to their curricula or review of some curricula that would have otherwise been available and language of communication, all of which contributed to some restriction on the number of programs whose instructors could participate in the study. The possibility of expert bias raised by this restriction has already been mentioned. However, the main aim of teaching and educating in any discipline and institution is to increase the professional competence and confidence of its graduates, and the teaching and learning approaches presented above could well form components of EBP in allied health professions. 30
Conclusion
A number of themes emerge from the results of this investigation of the priorities that expert prosthetic and orthotic instructors place on different teaching methods. Perhaps, most fundamental is the extent to which students are responsible for their own learning. Instructors working in developed nations saw students as bearing much responsibility for their own learning, even in clinical contexts, while those from developing nations placed greater responsibility on them for the quality of the devices that they fabricated for patients and the general quality of care that they offered.
This difference expressed itself in the priority given to different methods. Traditional patterns of lecture, tutorial, and workshop were present in all regions, although these expert instructors seemed quite aware of their shortcomings and of the impact that institutional facilities have upon instructor choice of teaching methods. Student-centered approaches were broadly supported, although PBL was less common than might have been expected from the general health sciences literature.
Regional differences in locus of responsibility also surfaced with respect to clinical teaching, with instructors from developing nations being more likely to see its function as revolving around skill development, while those from developed nations looked for emerging student critical thinking as a result of work in prosthetic and orthotics clinics.
This difference in the locus of responsibility for learning seems to underlie many of the priorities expressed by these expert instructors. Where the student is seen as more responsible, methods are chosen over which the instructor has less control. Where the instructor is seen as more responsible, methods which allow that responsibility to be more effectively managed seem more important.
Contemporary discussions can sometimes obscure the actual state of instructional practice. The research reported in this article provides data for one area of health science education. This data may be useful as a baseline from which important and fruitful changes can be encouraged. The next step would be to involve student priorities and outcomes in the exploration of current teaching practices in orthotics and prosthetic education. Hunt et al. 6 urged that the curriculum designer consider the relation between the teaching and learning processes, recognizing that, while educators attempt to teach scientific materials and professional skills, the amount of learning is determined by students. This seems true, wherever the instructor or institution places the locus of responsibility.
Footnotes
Acknowledgements
This article emerged from the first author’s doctoral study, which was carried out under ethical approval from the University of Newcastle, Australia (Approval Number H-350-1206). We would like to thank the institutions and expert prosthetics and orthotics instructors whose participation made this study possible.
Author contribution
All authors contributed equally in the preparation of this article.
Conflict of interest
The authors report no conflict of interest and they are responsible for the content and writing of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.