
Abstract
Study Design
Retrospective observational study.
Objectives
To evaluate 1-year clinical outcomes of vertebral body stenting (VBS) for osteoporotic vertebral fractures (OVFs) and compare its effectiveness in patients with and without poor prognostic magnetic resonance imaging (MRI) findings.
Methods
Eighty-seven patients (mean age, 79.2 years) who underwent VBS for OVF were analyzed. Those with severe vertebral body injury requiring additional posterior fixation or unsuccessful stent deployment were excluded. Outcomes included changes in pain (Numerical Rating Scale [NRS]), perioperative complications, adjacent vertebral fractures (AVF), and development of non-union or delayed vertebral collapse. Radiographic parameters—anterior vertebral height (AVH), middle vertebral height (MVH), posterior vertebral height (PVH), and vertebral angle (VA)—were assessed preoperatively, on postoperative day 1 (POD1), postoperative month 6 (POM6), and POM12. Patients were stratified based on the presence of poor prognostic MRI findings, defined as high or diffuse low-intensity signals on T2-weighted MRI.
Results
NRS significantly improved from 6.2 to 2.8 postoperatively. Cement leakage occurred without symptoms in 16% of patients. Non-union was not observed, and delayed vertebral collapse occurred without symptoms in three patients. Radiographic improvements in AVH, MVH, PVH, and VA were significant at POD1 and largely maintained at POM12. Patients with poor prognostic MRI findings showed significantly greater improvements in AVH, MVH, and VA at POD1 and POM12.
Conclusions
VBS effectively maintained vertebral height and prevented non-union and delayed collapse at 1 year postoperatively. Favorable outcomes were also seen in patients with poor prognostic MRI findings, supporting the utility of MRI as a treatment selection criterion.
Introduction
Osteoporotic vertebral fracture (OVF) is a common fragility fracture in older adults, and most cases have been considered to follow a favorable course with conservative treatment, including rest, bracing, and analgesics. 1 However, recent reports have shown that some patients experience delayed vertebral collapse, non-union, or pseudoarthrosis, leading to persistent pain, reduced activities of daily living (ADL) and quality of life (QOL), as well as neurological symptoms.2-4 Prospective studies from Japan have demonstrated that characteristic signal changes on T2-weighted magnetic resonance imaging (MRI), such as “very high intensity” or “diffuse low intensity,” are strong predictors of non-union associated with prolonged pain and progressive vertebral collapse.2,5 These findings, collectively known as poor prognostic MRI findings, have been shown to help identify patients who would benefit from early intervention using balloon kyphoplasty (BKP), with reports indicating improvements in pain, vertebral stability, and ADL/QOL at 6 months postoperatively. 6 However, BKP carries a risk of cement leakage, which can occur with a certain frequency of leakage into the intervertebral disc or extravertebral space; in rare cases, leakage into the spinal canal, intervertebral foramen, or vessels can cause serious complications.7,8 Notably, the “deflation effect” of the loss of correction due to removal after balloon dilation may lead to inadequate vertebral body repair after filling with cement. Therefore, vertebral body stenting (VBS) was developed to address these limitations. It has been suggested to be superior to BKP in preserving vertebral height and reducing the risk of cement leakage owing to the deployment of a metal stent within the fractured vertebra and injection of cement while maintaining the corrected alignment.9-11 However, reports on the medium-term outcomes of VBS remain limited, and its efficacy, particularly in patients with poor prognostic MRI findings, is yet to be fully investigated. Therefore, this study aimed to clarify the medium-term clinical outcomes of VBS and compare its efficacy between patients with and without poor prognostic MRI findings, assessing both the effectiveness of VBS and the appropriateness of its indication based on MRI findings.
Materials and Methods
This study was approved by the Institutional Review Board of the authors’ institution. VBS was performed on 118 patients (118 vertebrae) with OVF at our hospital between June 2021 and December 2023. The indication for VBS was determined through a comprehensive assessment of multiple clinical factors, irrespective of the presence or absence of poor prognostic MRI findings. These included resistance to conservative treatments (rest, bracing, analgesics), a decline in activities of daily living (ADL), and the need for early mobilization, particularly in elderly patients. Among these, 28 with severe vertebral body injuries, such as large endplate deficit type or split-type fractures, which are known to have poor outcomes with vertebroplasty alone,
12
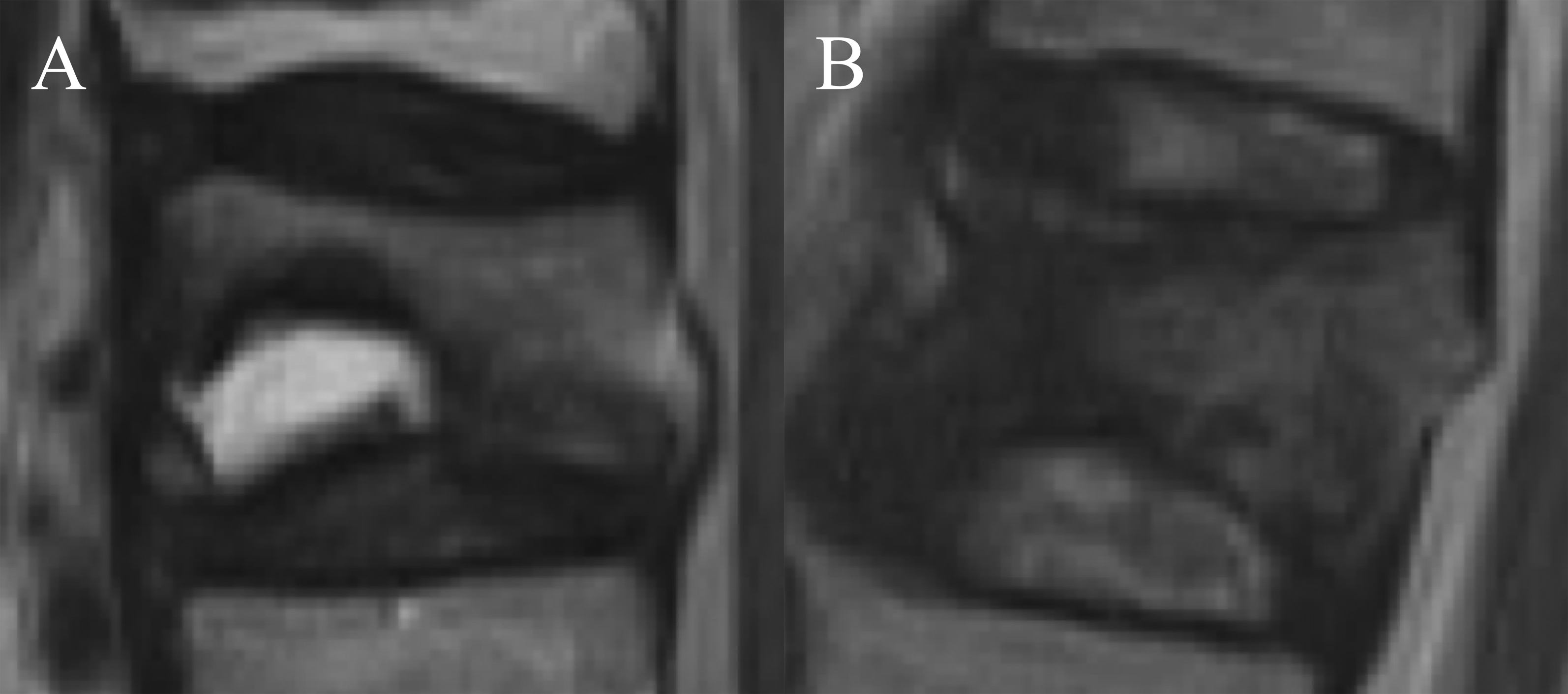
underwent additional posterior fixation and were excluded from this study. Three patients in whom stent deployment was unsuccessful and the procedure was completed with cement augmentation alone were also excluded. Consequently, 87 patients were included in the final analysis. Patient demographics and complications were assessed retrospectively. The primary outcomes included pain relief, measured using the Numerical Rating Scale (NRS); perioperative complications; adjacent vertebral fractures (AVF) within 12 months; and development of non-union or delayed vertebral collapse. Radiographic evaluation was primarily performed using supine lateral radiographs. In cases where significant spinal deformity impaired the accuracy of radiographic assessment, supplementary computed tomography images were used for reference. Anterior vertebral height (AVH), middle vertebral height (MVH), posterior vertebral height (PVH), and vertebral angle (VA) of the fractured vertebra were measured at four time points: preoperatively, postoperative day 1 (POD1), postoperative month (POM)6, and POM12 (Figure 1). At each time point, differences from the preoperative values were calculated for AVH, MVH, PVH, and VA and were expressed as ΔAVH, ΔMVH, ΔPVH, and ΔVA, respectively. MRI findings were evaluated using sagittal T2-weighted images. Based on previous reports,2,5 poor prognostic MRI findings were defined as (1) high-intensity signal changes within the fractured vertebra comparable to cerebrospinal fluid (high-intensity type) or (2) low-intensity areas occupying >50% of the vertebral body (diffuse low-intensity type) (Figure 2). Measurement of Vertebral Height and Angle on Sagittal Images. Vertebral height was assessed on sagittal images obtained from supine lateral plain radiographs or computed tomography scans. The anterior, middle, and posterior vertebral heights were defined as the height at the anterior wall (a), middle vertebral body (b), and posterior wall (c) of the vertebral body, respectively. Vertebral angle (d) was defined as the angle formed between the cranial and caudal endplates of the fractured vertebra. A: Preoperative lateral radiograph. B: Postoperative lateral radiograph Representative Poor Prognostic MRI findings. A: High-Intensity Type on T2-Weighted Imaging. B: Diffuse low-intensity type on T2-weighted imaging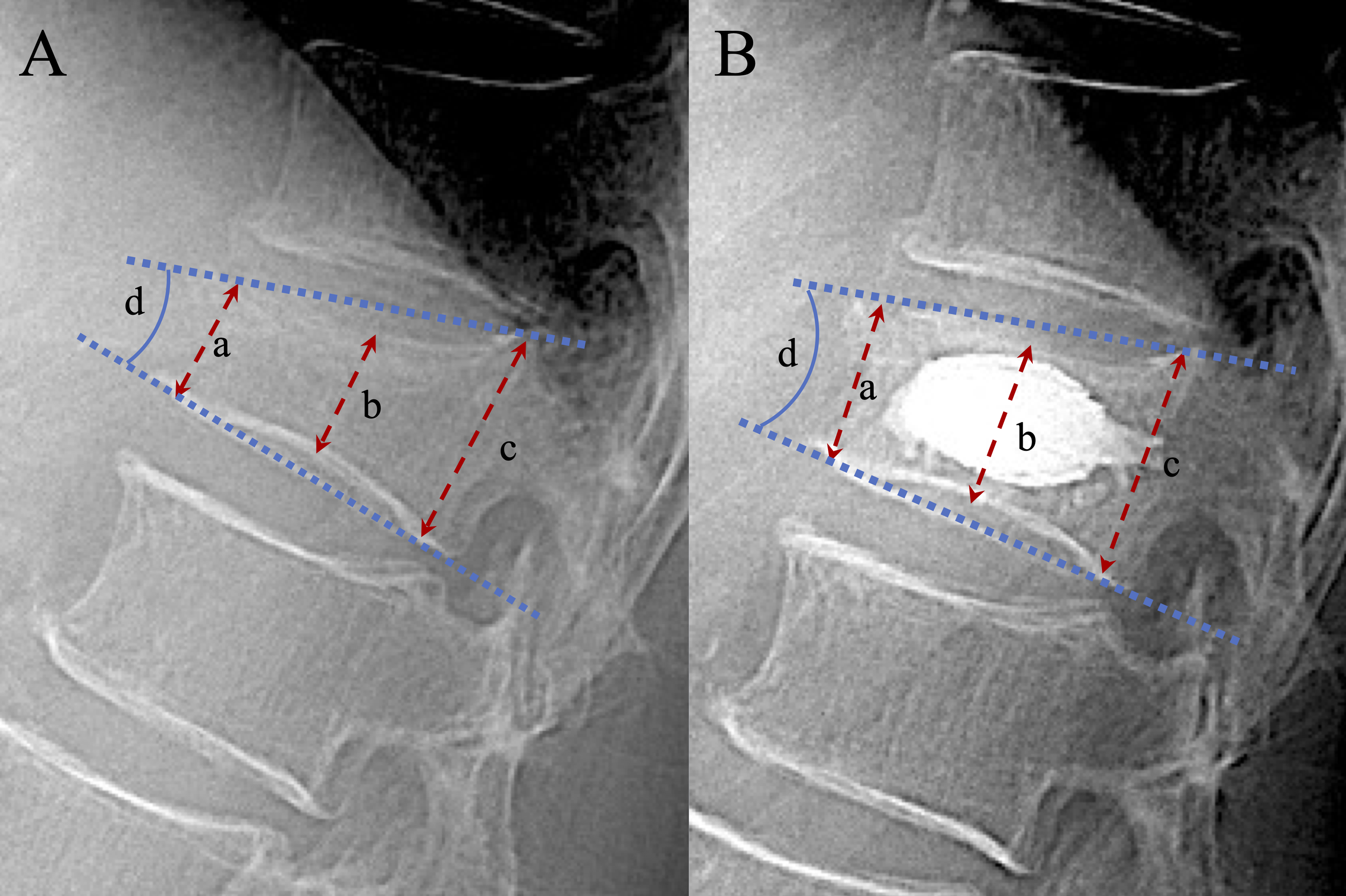
Statistical Analysis
All statistical analyses were performed using paired and Welch’s t-tests for continuous variables to identify between-group differences. Statistical data were generated using EZR software, 13 and statistical significance was set at P < .05.
Results
Baseline Characteristics, Surgical Details, and Clinical Outcomes of the Study Population
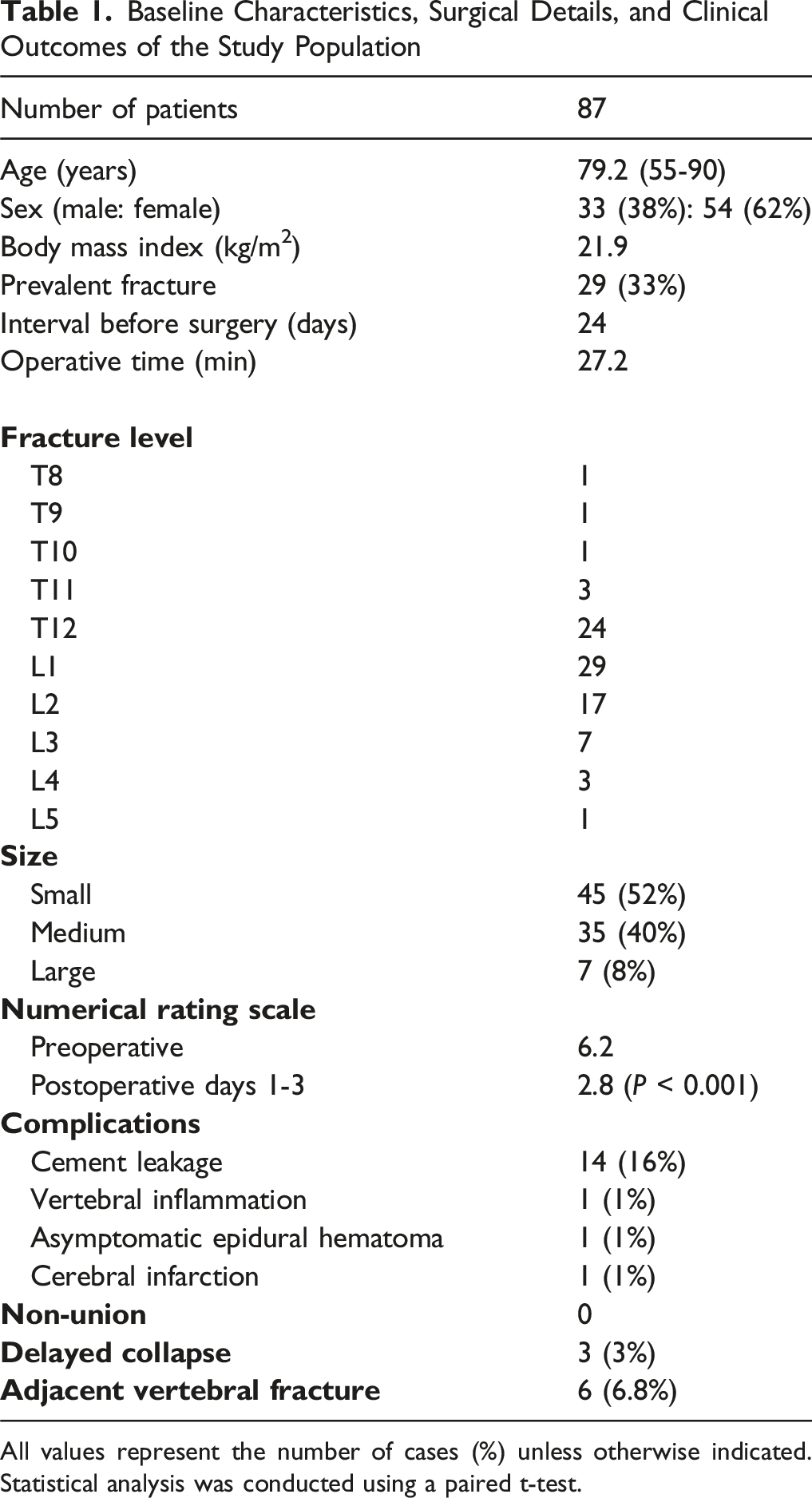
All values represent the number of cases (%) unless otherwise indicated. Statistical analysis was conducted using a paired t-test.
Radiographic Measurements of Vertebral Height and Vertebral Angle
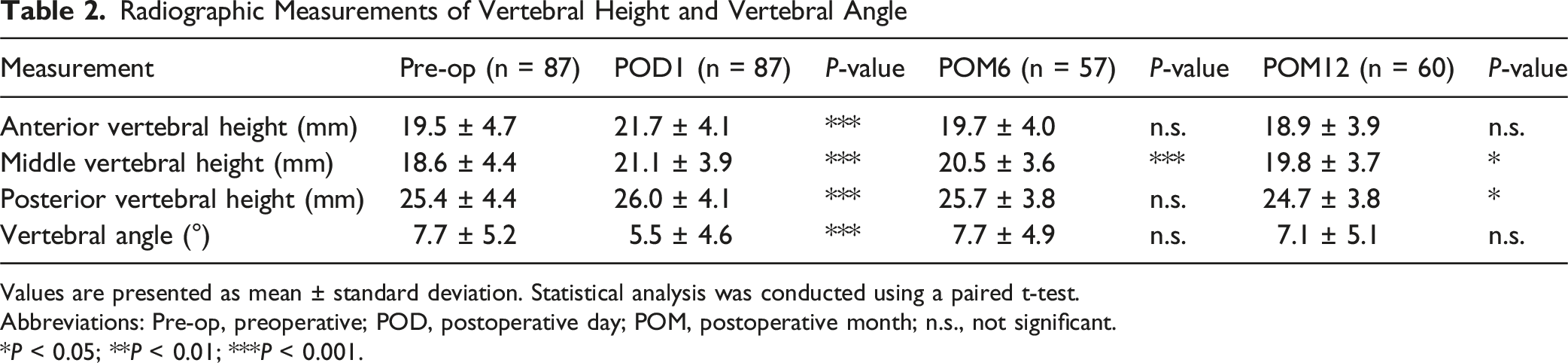
Values are presented as mean ± standard deviation. Statistical analysis was conducted using a paired t-test.
Abbreviations: Pre-op, preoperative; POD, postoperative day; POM, postoperative month; n.s., not significant.
*P < 0.05; **P < 0.01; ***P < 0.001.
Radiographic Differences Based on Poor Prognostic MRI Findings
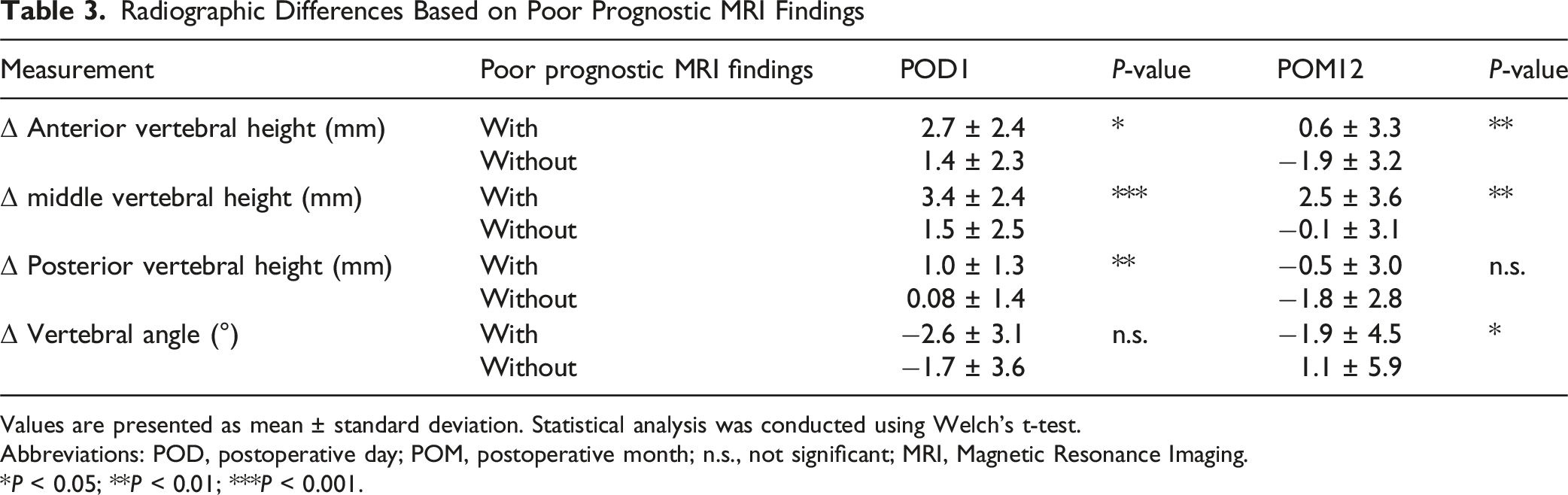
Values are presented as mean ± standard deviation. Statistical analysis was conducted using Welch’s t-test.
Abbreviations: POD, postoperative day; POM, postoperative month; n.s., not significant; MRI, Magnetic Resonance Imaging.
*P < 0.05; **P < 0.01; ***P < 0.001.
Discussion
In this study, we analyzed the outcomes of patients who underwent VBS for OVF and reported that vertebral body height was well maintained at 1 year postoperatively, with no development of non-unions or symptomatic delayed vertebral collapse. Vertebral height restoration and kyphosis correction by VBS were more effective among patients with poor prognostic MRI findings preoperatively than among those without such findings. Reports on the course of events after VBS are scarce, and, to the best of our knowledge, no reports exist on the efficacy of VBS in preventing non-union or delayed vertebral collapse in patients with poor prognostic MRI findings.
Indications for vertebroplasty in OVF have traditionally been limited to cases refractory to adequate conservative treatment. However, an increasing number of reports have recently suggested that performing vertebroplasty in the early phase of injury leads to better outcomes. In particular, among very old patients, procedures such as BKP and VBS tend to be selected with the goal of promoting early mobilization.14,15 In contrast, many OVFs improve naturally with conservative therapy, and vertebroplasty may be inappropriate for all cases considering the risks associated with surgery—perioperative complications, cement-related adverse events, AVFs, and financial cost.8,16-18 Treatment indication criteria differ depending on the surgeon, highlighting the need for establishing clear guidelines. Takahashi et al. reported that patients with residual poor prognostic MRI findings at 1 month had a poor prognosis for conservative treatment, with 62.5% experiencing non-union. 5 Hoshino et al. showed that BKP was more effective than conservative treatment in improving ADL and QOL, as well as preventing non-union at 6 months postoperatively in patients with poor prognostic MRI findings. 6 Non-union is associated with neurological deficits, chronic back pain,4,19-21 and, in some cases, progression to symptomatic delayed vertebral collapse requiring invasive surgical interventions such as anterior reconstruction.22-27 Accordingly, their prevention holds significant clinical importance. No cases developed non-union in the present study. Although all cases of delayed vertebral collapse occurred in patients with poor prognostic MRI findings, they were asymptomatic and did not require additional surgery. These findings indicate that VBS may be effective in preventing both non-union and symptomatic delayed vertebral collapse. Favorable outcomes were also observed in patients with poor prognostic MRI findings, suggesting that these MRI findings may be useful in supporting clinical decision-making. However, further comparative studies, including evaluation of preoperative vertebral instability, are needed to determine whether patients with poor prognostic MRI findings truly benefit more from VBS.
VBS was developed by the German radiologist Fürderer as a percutaneous kyphosis correction technique using intravertebral stents and was first applied clinically in 2002. 28 The balloon is expanded within the vertebral body to create space for bone cement, and the stent is implanted to prevent a loss of vertebral body height correction (deflation effect) after balloon removal and is expected to maintain vertebral body height better than BKP.29-32 Vertebral instability and intravertebral cavitation may exacerbate the deflation effect in patients with poor prognostic MRI findings. 33 In our study, greater improvements in vertebral height and VA correction were observed in this group, suggesting that the stent significantly contributed to structural support. A further advantage of VBS is its effectiveness in preventing bone cement leakage. As bone cement is injected into a cavity enclosed by the stent, the injection pressure can be kept relatively low, and the mesh structure of the stent helps prevent leakage. Additionally, the side-opening cannula allows directional control of cement filling, and the use of high-viscosity cement contributes to minimizing extravertebral leakage.10,34 According to previous reports, the cement leakage rate ranges from 20% to 51% in BKP and from 4.2% to 30% in VBS, with several studies suggesting a lower leakage rate in VBS.11,15,32,35-38 However, other reports suggest no significant difference in cement leakage between VBS and BKP, 39 indicating that factors such as patient selection, cement type, injection pressure, and bone quality need to be considered. In our study, cement leakage occurred in 16% of patients, which is comparable to the findings of previous reports, and all of them were asymptomatic. Intravertebral structural instability may increase the risk of cement leakage in patients with poor prognostic MRI findings, making VBS a rational choice from this perspective.
Radiographic evaluation demonstrated significant improvements in AVH, MVH, and PVH, as well as VA immediately after surgery. Although slight collapse progression was observed at POM6—except for the MVH—overall vertebral morphology remained stable at 12 months. In VBS, cement spread is partially limited by the presence of the stent, and vertebral height was well maintained in the middle wall because the stent is typically deployed in the central portion of the vertebral body. However, insufficient cement distribution to the anterior and posterior walls may have contributed to mild collapse in those regions. To achieve broader structural support, selecting the largest possible stent size may help enhance overall vertebral stability. Differences in outcomes depending on the selected size are a subject for future investigation. Perioperative complications were observed in three patients (3%) in this study. Although complications such as spinal cord injury, infection, embolism, and epidural hematoma have been infrequently reported in BKP,7,8 similar risks are also associated with VBS. While the overall complication rate of VBS is considered comparable to that of BKP, some studies have indicated a higher incidence of intraoperative material-related complications linked to stent deployment. 37 Therefore, vertebral augmentation requires careful surgical technique and appropriate patient selection despite being a minimally invasive and generally safe procedure.
AVF is another postoperative complication that warrants attention, whose incidence has been reported to range from 11% to 29% after BKP,15,40 and 9% to 13% after VBS.9,10 Multiple factors are believed to contribute to AVF development, including preoperative segmental kyphosis, cement leakage into the intervertebral disc, low bone mineral density, injected cement volume, patient activity level, spinal alignment, and endplate damage.9,10,12 In the present study, the incidence of AVF was 6.8%, which is lower than previously reported rates. This may be partly attributable to the exclusion of patients with severe fracture types, such as split-type fractures or large endplate deficits, resulting in a study population with relatively preserved spinal alignment. However, some studies reported no significant difference in AVF incidence between patients who underwent vertebroplasty and those treated conservatively, raising questions about the extent to which the procedure contributes to AVF development. 7 For patients identified as having a high risk for AVF based on previous literature, prioritizing appropriate osteoporosis treatment and reinforcement with external bracing may be more important than relying solely on procedural intervention.
Limitation
This study has several limitations. First, it was a retrospective observational study and did not include comparisons with conservative management or alternative procedures such as BKP, thereby precluding any direct assessment of the relative effectiveness of VBS. At our institution, VBS is used as the first-line vertebral augmentation technique, which might have introduced selection bias. Severe fracture types were deemed inappropriate for VBS alone and were treated with posterior fixation; therefore, they were excluded from this study. This exclusion may have affected our findings. All radiographs were obtained in the supine position, which may have led to overestimation of preoperative vertebral heights compared to seated imaging, particularly in cases with high instability. However, due to severe pain at the time of injury, most patients were unable to maintain a seated position, making supine imaging the most feasible and consistent method. This limitation should be considered when interpreting radiographic changes. Although vertebral body height was measured using supine lateral radiographs under standardized imaging conditions, including fixed source-to-image distance and calibrated PACS viewer, radiographic magnification error and variability in patient body size may still affect measurement accuracy. In addition, due to incomplete follow-up at certain time points, a subset of patients was not included in the longitudinal radiographic assessment. This potentioal bias should also be considered when interpreting the results.
Conclusions
This study demonstrated that VBS for OVF maintains vertebral body height even at 1 year postoperatively and may be effective in preventing non-union and delayed vertebral collapse. Favorable outcomes were also observed in patients with poor prognostic MRI findings, suggesting that these findings may support clinical decision-making regarding VBS indication.
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board of Nagoya Ekisaikai Hospital (approval number: 2022-019).
Consent to Participate
Informed consent was obtained from the patient for participation in this study using an opt-out approach approved by the IRB.
Author Contributions
All authors contributed to the study conception, design, data collection, analysis, and manuscript preparation. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.