
Abstract
Background and aim:
Microprocessor-controlled prosthetic knees have gained increasing popularity over the last decade. Research supports their provision to address specific problems or to achieve certain rehabilitation goals. However, there are yet no agreed protocols or prescribing criteria to assist clinicians in the identification and appropriate selection of suitable users. The aim is to reach professionals’ agreement on specific prescribing guidelines for microprocessor-controlled prosthetic knees.
Technique:
The study involved multidisciplinary teams from the Inter Regional Prosthetic Audit Group, representing nine Prosthetic Rehabilitation Centres in the South East England region. We used the Delphi technique with a total of three rounds to reach professionals’ agreement.
Discussion:
The prescribing guidelines were agreed and will be reviewed and updated depending on new research evidence and technical advances.
Clinical relevance
This project is highly useful for professionals in a clinic setting to aid in appropriate patient selection and to justify the cost of prescribing microprocessor-controlled prosthetic knees.
Background and aim
Microprocessor-controlled knees (MPKs) are a category of prosthetic knee components, which have gained increased popularity in recent years. They can be a vital, necessary and important means to improve rehabilitation outcomes and quality of life. There is an increasing variety of commercially available MPKs; nevertheless, they all share some basic features and functionalities that set them apart from non-MPKs. Evidence currently supports the use of MPKs showing specific improvements in safety, energy requirements and long-term cost-effectiveness. 1 MPKs, however, come at relatively high initial and ongoing costs compared to other categories of prosthetic knees, and appropriate patient selection is key to justify those implications. Manufacturers of prosthetic components highlight the main benefits of components with little emphasis on contraindications or suitability details. The lack of national or international prescribing policies for most prosthetic components results in variable prescribing practices between different centres and creates an urgent need to agree on a unified approach. In a publicly funded health-care system, it is important to adopt a clear, uniform and fair approach to prescribing practices across the board. Furthermore, prescribing MPKs is associated with significant financial implications making provision increasingly harder to justify especially in light of continued improvements of non-MPK components. Current published evidence provides guidance in relation to the specific benefits of using an MPK, but prescribing guidelines that regulate the provision of MPKs in England are yet to be agreed. We used professionals’ consensus in our evidence-based decision-making to produce these guidelines. It is assumed that current clinical practices are influenced by published scientific evidence in addition to the practicalities and limitations of prescribing within a clinical setting.
The aim of this study is to produce prescribing guidelines for MPKs through professional consensus based on current published research evidence.
Technique
A Delphi technique was used by contacting multidisciplinary teams at the nine Prosthetic Rehabilitation Centres in the South East England. Delphi may be characterised as a method for structuring a group communication process so that the process is effective in allowing a group of individuals, as a whole, to deal with a complex problem. 2 The Delphi technique is a structured technique, originally developed as a systematic, interactive forecasting method, which relies on expert’s opinions where experts answer questionnaires in two or more rounds. A facilitator provides an anonymous summary of the experts’ opinions from the previous round as well as the reasons they provided for their judgments. Thus, experts are encouraged to revise their earlier answers in light of the replies of other members of their panel. During this process, the range of the answers will decrease and the group will converge towards agreement. 2
We followed the outlines of pharmacological prescribing guidelines to include suitability criteria, indications and contraindications. The results of each Delphi round were circulated in writing and presented at a meeting with the involved professionals. The multidisciplinary teams in all the nine participating centres included rehabilitation medicine physicians, physiotherapists, occupational therapists and prosthetists. Agreement between professionals within a centre was reached and the overall result was forwarded to the investigator. Professionals were asked to support their suggestions and replies with current published evidence. Research shows a significant improvement in reducing stumbles and falls3,4 and a significant reduction in energy requirements of walking.5,6 A reduction in contralateral limb loading 7 and a significant improvement in joint kinetic symmetry 8 suggest reduced wear and tear of the contralateral limb. Other benefits such as improvements in activity, reduced cognitive demands for walking, improved environmental obstacle negotiation, enhanced user satisfaction and quality of life were reported in a comprehensive systematic review. 9 Previous systematic reviews reported similar findings in relation to safety, energy efficiency and cost-effectiveness 4 in addition to quality of life and improved activity. 10
The first Delphi round probed current prescribing practices, reflecting different professionals’ views. This included open questions to formulate the guidelines under five headings: Suitability, Minimum Requirements, Main Indications, Relative Indications, and Contraindications. Feedback from the first Delphi round was used to modify the format of the guidelines to include four main headings: Definitions, Suitability Criteria, Indications and Contraindications. All items received through the first round were sent out for consultation and scoring in the second round, with each item rated as a percentage of agreement according to the number of suggestions it received in the first round.
The second round amalgamated similar items and produced the core guidelines for rating and feedback. Professionals were encouraged to rate agreement with each item and provide comments. Feedback was then used to modify, delete or add items, and the guidelines were further amended and submitted for consultation through the third round.
By the start of the third round, most items had already achieved 100% agreement and the rest had 80% or more agreement. Comments were invited to make further improvements to one suitability criteria item, five indication items and two contraindication items. These were modified and sent for rating and feedback in the third Delphi questionnaire along with the agreed items. Following feedback from all centres, one of the indications was deleted as it was thought to be already included in other items, and the rest of the items were further modified. The final results were presented at a meeting and members were given a 6-week period to provide any final feedback or comments. The agreed definitions and guidelines are listed in Table 1.
The agreed definitions and guidelines.
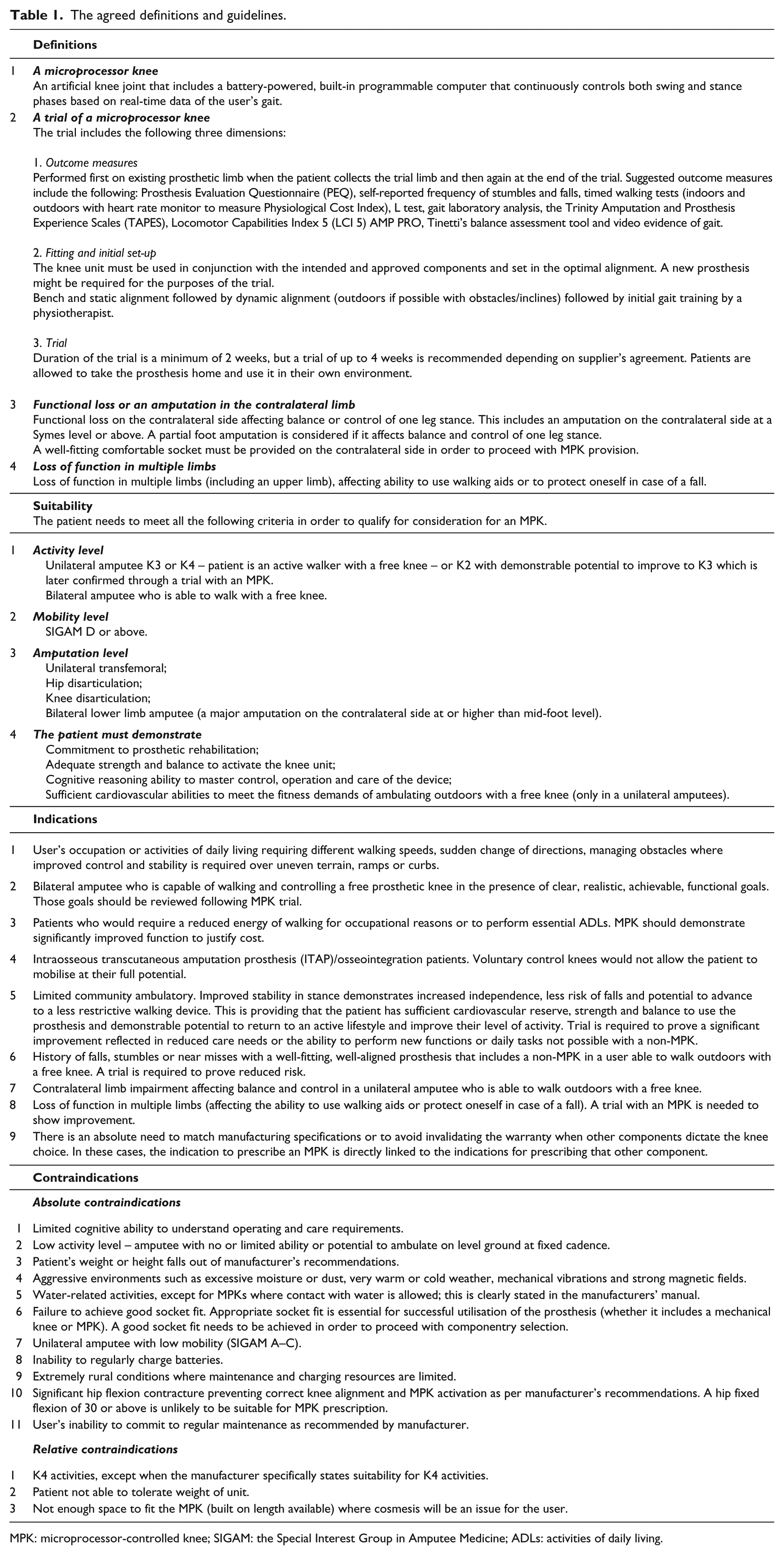
MPK: microprocessor-controlled knee; SIGAM: the Special Interest Group in Amputee Medicine; ADLs: activities of daily living.
Discussion
The agreed guidelines reflect the current prescribing practices and views of a large sample of rehabilitation teams in the South East England. These views were informed by published research evidence of the advantages and shortfalls of MPKs. The professionals’ academic knowledge is balanced by the practical constraints of prescribing in a clinical setting under strict budgetary limitations. Our work highlighted significant differences in practice between professionals in different centres, which often made it difficult to reach full agreement on certain items. This also exposed a gap between what professionals aspire to provide for their patients and what is practically and financially possible. There is great variability in professionals’ familiarity with MPKs due to the existing postcode lottery of provision that we are trying to address. In general, those in centres with less experience in prescribing MPKs tended to be more inclusive in their indications as they had higher expectations compared to professionals more familiar with prescribing MPKs. Many agreed that using an MPK would hold a degree of functional benefit in a large percentage of users. However, provision ultimately depends on defining the smallest improvement that could still be deemed as meaningful in the context of the goal-setting process and affordable within the health-care system. There is an obvious need for further health economic studies to define the quality-added life years (QALYs) of using MPKs within the national health-care system in England. The cost of an MPK component is only one aspect of its health economy impact, which needs to be considered in view of the long-term cost savings that include prevention of injuries and reduced medical- and social-care needs. We therefore expect that the indications for prescribing MPKs might need to be more or less inclusive within the context of different health-care systems.
Our study was limited to the opinions of the available professionals in the South East England based on their experience of the relative costs and performance of current components and rehabilitation practices. These indications should be reviewed in the future in light of changes to the short- and long-term costs of MPK components and changes to health-care and social-care systems.
Key point
This article presents core MPK prescribing guidelines as agreed by multidisciplinary team members in nine prosthetic centres in England. The prescribing guidelines are influenced by technological advances of MPK components in addition to health-care and social-care structures.
Footnotes
Acknowledgements
We would like to acknowledge the members of the Inter-Regional Prosthetic Audit Group in the Southeast of England (IRPAG) who contributed to the Delphi process. We are also grateful for Dr Pria krishnasamy’s significant contribution at the initial stages of this project.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.