
Abstract
Background:
User feedback about grasping force and hand aperture is very important in object handling with myoelectric forearm prostheses but is lacking in current prostheses. Vibrotactile feedback increases the performance of healthy subjects in virtual grasping tasks, but no extensive validation on potential users has been performed.
Objectives:
Investigate the performance of upper-limb loss subjects in grasping tasks with vibrotactile stimulation, providing hand aperture, and grasping force feedback.
Study design:
Cross-over trial.
Methods:
A total of 10 subjects with upper-limb loss performed virtual grasping tasks while perceiving vibrotactile feedback. Hand aperture feedback was provided through an array of coin motors and grasping force feedback through a single miniature stimulator or an array of coin motors. Objects with varying sizes and weights had to be grasped by a virtual hand.
Results:
Percentages correctly applied hand apertures and correct grasping force levels were all higher for the vibrotactile feedback condition compared to the no-feedback condition. With visual feedback, the results were always better compared to the vibrotactile feedback condition. Task durations were comparable for all feedback conditions.
Conclusion:
Vibrotactile grasping force and hand aperture feedback improves grasping performance of subjects with upper-limb loss. However, it should be investigated whether this is of additional value in daily-life tasks.
Clinical relevance
This study is a first step toward the implementation of sensory vibrotactile feedback for users of myoelectric forearm prostheses. Grasping force feedback is crucial for optimal object handling, and hand aperture feedback is essential for reduction of required visual attention. Grasping performance with feedback is evaluated for the potential users.
Keywords
Background
Myoelectric forearm prostheses are being developed as a replacement for missing hands due to amputation or congenital reduction defects. However, only 64% of the fitted myoelectric forearm prostheses are used by their owners on a daily basis, 1 which is caused by, among other reasons, the limited functionality of the prosthesis and the lack of sensory feedback.1,2 In a workshop with a representative sample of myoelectric forearm prosthesis users, information about grasping force and hand aperture was cited as the most important feedback for a prosthesis user. 3 Common methods to provide the artificial feedback noninvasively are through electrotactile, mechanotactile, or vibrotactile stimulation of the skin.4,5 Although mechanotactile stimulation is, in terms of feedback performance, the most promising because of the modality-matching,4,6 recent emphasis is mostly on vibrotactile stimulation due to the miniaturization of the stimulators. 7 The focus of most studies on vibrotactile user feedback is about grasping force feedback, which is provided through a single C2 tactor (miniature vibrotactile stimulator),8–11 a single coin motor,12,13 or an array of coin motors. 14 In another study, the use of a single C2 tactor and that of an array of coin motors were compared. 15
Although feedback about hand aperture was also indicated to be very important, 3 only a few studies evaluating hand aperture feedback have been found. Electrotactile stimulation to provide hand aperture feedback has been tested, both noninvasively by stimulating the skin 16 and invasively by direct nerve stimulation. 17 In a recent study, an array of C2 tactors on the waist was used to provide vibrotactile feedback about several hand configurations. 18 A comparison between electrotactile and vibrotactile stimulation to provide hand aperture feedback, specifically by using an array of stimulators, has been performed as well. 19 Another approach is the use of skin stretch feedback to provide proprioceptive information, which was shown in some cases to be superior over vibrotactile feedback.20,21
In short, most studies on grasping force and hand aperture feedback showed an increase in grasping performance when feedback is provided, but there is no consensus on the optimal stimulation method. Only in around half of the aforementioned studies were the feedback methods evaluated on amputees, and the number of subjects in these studies was relatively low (1–6 amputees).
Several studies have compared the sensitivity of the residual limb of amputees with that of the healthy limb, but there is no consensus on the similarity between these sensory thresholds. 22 Older studies reported a better spatial acuity at the residual limb, specifically lower touch and two-point discrimination thresholds and lower errors in point localization, and this was explained by the reorganization of the central sensory mappings after amputation.23,24 However, more recent studies on healthy subjects suggested that the differences in spatial acuity are more likely to be caused by differences in the amount of attention given to the stimulation site. After amputation, the attentional resources are spread over a smaller body area and may therefore result in a better spatial acuity.25,26 Other studies found no differences in tactile detection thresholds, specifically two-point discrimination, force discrimination, and vibration thresholds, between the amputated and sound limb22,27 or between the sound limb and the reinnervated skin after targeted reinnervation.28,29 Higher tactile and two-point discrimination thresholds were only found at the scar tissue. 22 Furthermore, the sensitivity did not change over time, except for some stabilization toward normal values at the scar tissue. 30 To our knowledge, no studies have been performed on sensitivity abnormalities in subjects with congenital transradial reduction defects.
Based on the reviewed literature, it is currently not known how amputees or subjects with congenital upper-limb defects would perform in vibrotactile feedback experiments compared to healthy subjects. Therefore, in this study, subjects with a transradial amputation or congenital reduction defect were evaluated in their performance on a set of virtual grasping tasks when vibrotactile grasping force and hand aperture feedback are provided.
Methods
Subjects
Subject characteristics are summarized in Table 1. Subjects with upper-limb loss were recruited by rehabilitation physicians at the local rehabilitation center. Subjects were included if (1) they had no prior experience with vibrotactile stimulation, (2) they did not suffer from severe skin or sensory problems on the residual limb, (3) they were able to understand the tasks, and (4) they were able to control the virtual setup with their sound arm. Every subject was briefed about the study beforehand via an information letter and all gave informed consent. The study protocol is approved by the local medical ethical committee (Medisch Ethische ToetsingsCommissie Twente).
Summary of the subject characteristics.
C: cosmetic prosthesis; M: myoelectric prosthesis; B: body-powered prosthesis; No: no visual and no vibrotactile feedback.
Mean values and standard deviations are given.
Materials
Two vibrotactile stimulation methods were used to provide feedback: amplitude and position modulation. A C2 tactor (Engineering Acoustics Inc., Casselberry, FL, USA) was used to provide the amplitude modulated vibrotactile stimulation. The C2 tactor (3 cm diameter and 0.5 cm height) was activated at 250 Hz, corresponding to the resonance frequency of the tactor and the frequency at which the main mechanoreceptors in the forearm skin, the Pacinian corpuscles, are most sensitive. An array of eight coin motors (1 cm diameter and 0.3 cm height) was used to provide the position modulated vibrotactile stimulation. The activation voltage of the coin motors (iNEED (HK) Limited, Shenzhen, China) was kept constant at 2.5 V, which corresponds to a stimulation frequency of between 50 and 100 Hz depending on the specific skin characteristics. The coin motors and C2 tactor were both attached to the skin by double-sided tape rings (EEG Kleberinge; GVB-geliMED KG, Bad Segeberg, Germany).
Grasping force feedback
Grasping force feedback was provided either through a single C2 tactor placed on the residual limb or through an array of eight coin motors placed around the forearm. The coin motors were placed 3 cm distal to the elbow and equally distributed around the arm, resulting in inter-stimulator distances of 3.1 ± 0.3 cm. Each of the eight discrete grasping force levels that could be applied by the subjects was related to the activation of one of the eight coin motors. Activation of the most dorsal coin motor corresponded to the lowest grasping force level, and with increasing force, the activation shifted around the arm. The C2 tactor was placed on the dorsal side of the forearm, halfway between the elbow and the tip of the residual limb. In this case, the eight discrete grasping force levels were related to eight different amplitude levels ranging from 1 to 4.5 V with an increment of 0.5 V, with 1 V corresponding to the lowest force level.
Hand aperture feedback
Hand aperture feedback was provided through an array of eight coin motors. Each of the eight possible discrete hand aperture levels, ranging from a fully opened to a fully closed hand, was related to the activation of a particular coin motor. Two orientations of the array, transversal and longitudinal, were investigated. For the transversal orientation, the coin motors were placed around the forearm in a similar arrangement to that for the grasping force feedback. The most dorsal stimulator corresponded to the fully opened hand, and for each decrease in hand aperture, the activation shifted to the next stimulator around the arm. For the longitudinal orientation, the coin motors were placed on the dorsal side of the forearm with the same inter-stimulator distance as for the transversal orientation. Activation of the most distal coin motor was related to the closed hand and that of the most proximal coin motor to the fully opened hand.
Virtual setup
A virtual setup was created in LabView (LabView 2010 SP1; National Instruments, Austin, TX, USA) to show an opening and a closing hand for the hand aperture feedback experiments (see Figure 1(a)) and a hand holding an object for the grasping force experiments (see Figure 1(b)). The hand aperture and the grasping force were controlled by the subjects through mouse scrolling, with forward scrolling being linearly related to the closing of the hand or the increasing of grasping force. The gain between the degree of mouse scrolling and the resulting change in hand aperture or grasping force was randomized per object. Furthermore, the “clicks” that are normally felt when scrolling were also removed to exclude any information that can be used to link the degree of mouse scrolling to the resulting hand aperture or grasping force. For the hand aperture feedback experiments, a virtual circular object, which had to be grasped by the subjects, was displayed between the thumb and the index finger. Eight different object sizes were simulated and presented in random order, with up to a total of 40 objects per task. Each discrete level of hand aperture was related to a particular object size and consequently to the activation of a particular coin motor. For the grasping force feedback experiments, eight different object weights were simulated, corresponding to the eight discrete grasping force levels necessary to successfully hold the object. The weight of the object was visually represented by the color of it.
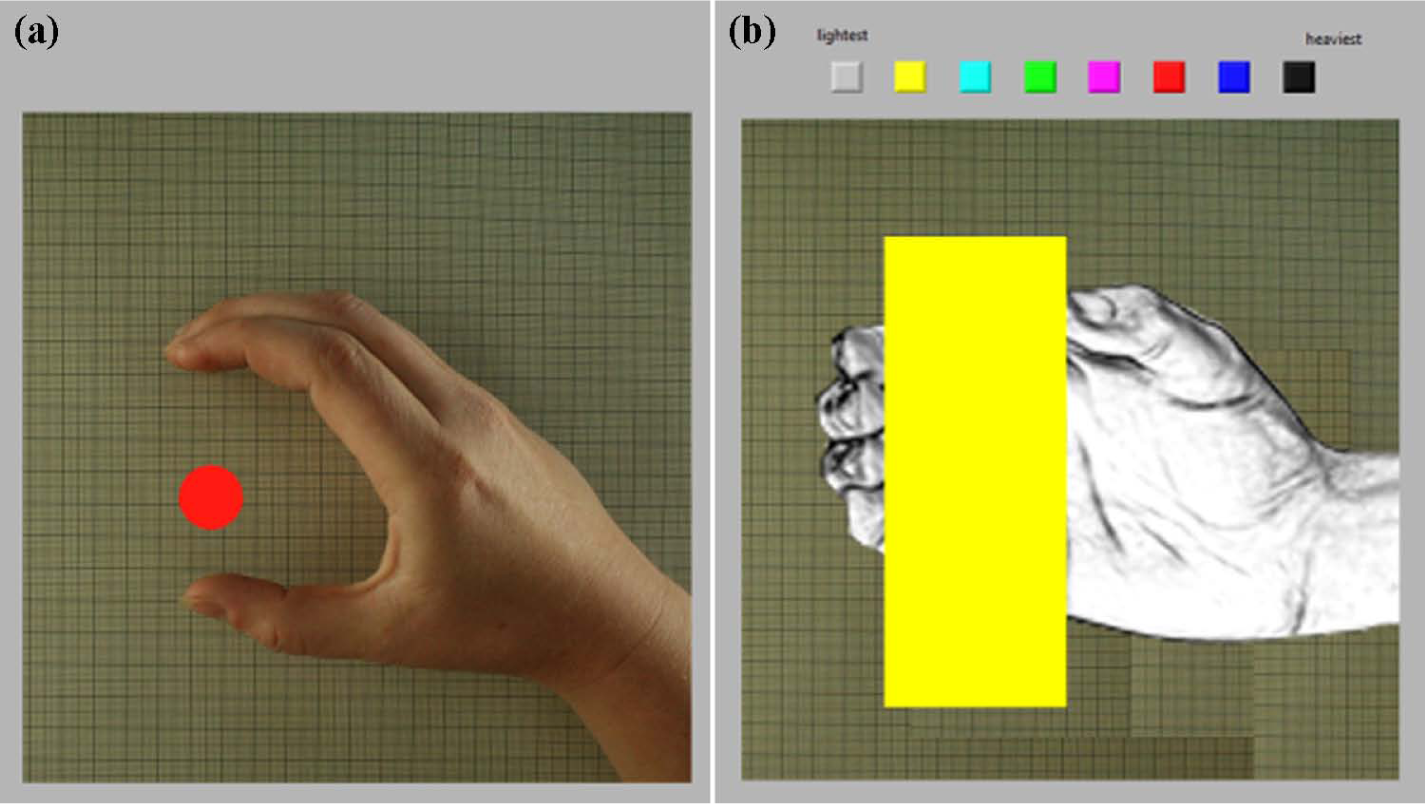
Virtual representation of a grasping hand and objects with varying sizes and weights, used for (a) hand aperture feedback experiments and (b) grasping force experiments.
Protocol
Subjects were seated behind a laptop showing the virtual setup. Subjects controlled the mouse with their sound hand, while feedback was provided to their residual limb.
The grasping force feedback experiments consisted of a training (20 objects) and an experimental session (40 objects). In both sessions, feedback was provided via the C2 tactor and the coin motor array. Subjects were asked to apply the appropriate grasping force by scrolling the mouse. After 2 s of displaying the object, the result was shown visually in the form of a squeezed object when the force was too high or a dropped object when the force was too low. If the applied grasping force was correct, the next object was shown. Otherwise, the same object was shown again but with a maximum of five attempts. During the experimental session, the result of the applied grasping force was hidden and the subjects were asked to apply the right grasping force as fast as possible and within 3 s, after which the next object was shown.
For the hand aperture feedback experiments, two sessions for each array orientation were performed: during the first session, the virtual hand and the object were shown throughout the whole task, while for the second session, the hand was not shown at all and the object was only shown for 0.5 s. The first session, which is referred to as the visual-feedback session, allowed the subject to learn the relationship between coin motor activation and the level of hand aperture. During the second session, the subjects had to rely on the vibrotactile feedback only, thus simulating situations where visual feedback is not available.
The order of the array orientations and the feedback configurations was randomized for each subject to compensate for possible learning effects. A control measurement without any feedback was performed after each feedback experiment.
Statistical analysis
Based on the required hand apertures and grasping forces, the percentages of correct hand apertures and grasping forces were calculated. Furthermore, the percentages of hand apertures and grasping forces deviating maximally one level were calculated. The latter percentages were used to provide another measure of accuracy, one that does not depend on the exact localization or amplitude perception of the stimulus. The last set of results used in the analysis was the task duration of each subject, which was calculated by summing over all objects, the time taken to reach the final hand aperture or grasping force level. Repeated-measures analysis of variance (ANOVA) tests, with a significance level of 0.05, were used to evaluate the differences between the feedback configurations.
Comparison with healthy subjects
The results were compared with the outcomes from two separate studies on the performance of healthy subjects in virtual grasping tasks with vibrotactile hand aperture 19 and grasping force feedback. 15 In comparison with the protocol of this study, there were two differences: (1) for healthy subjects, the coin motors were equally distributed between the elbow and the wrist and were not placed on the upper arm; and (2) healthy subjects controlled the mouse with their dominant (computer) hand and feedback was delivered to the same arm. The results for subjects with upper-limb loss and for healthy subjects were compared via unpaired samples t-tests.
Results
Grasping force feedback
The percentages of correct grasping forces and the percentages of grasping forces deviating maximally one force level from the required force were calculated and presented in Figure 2(a).
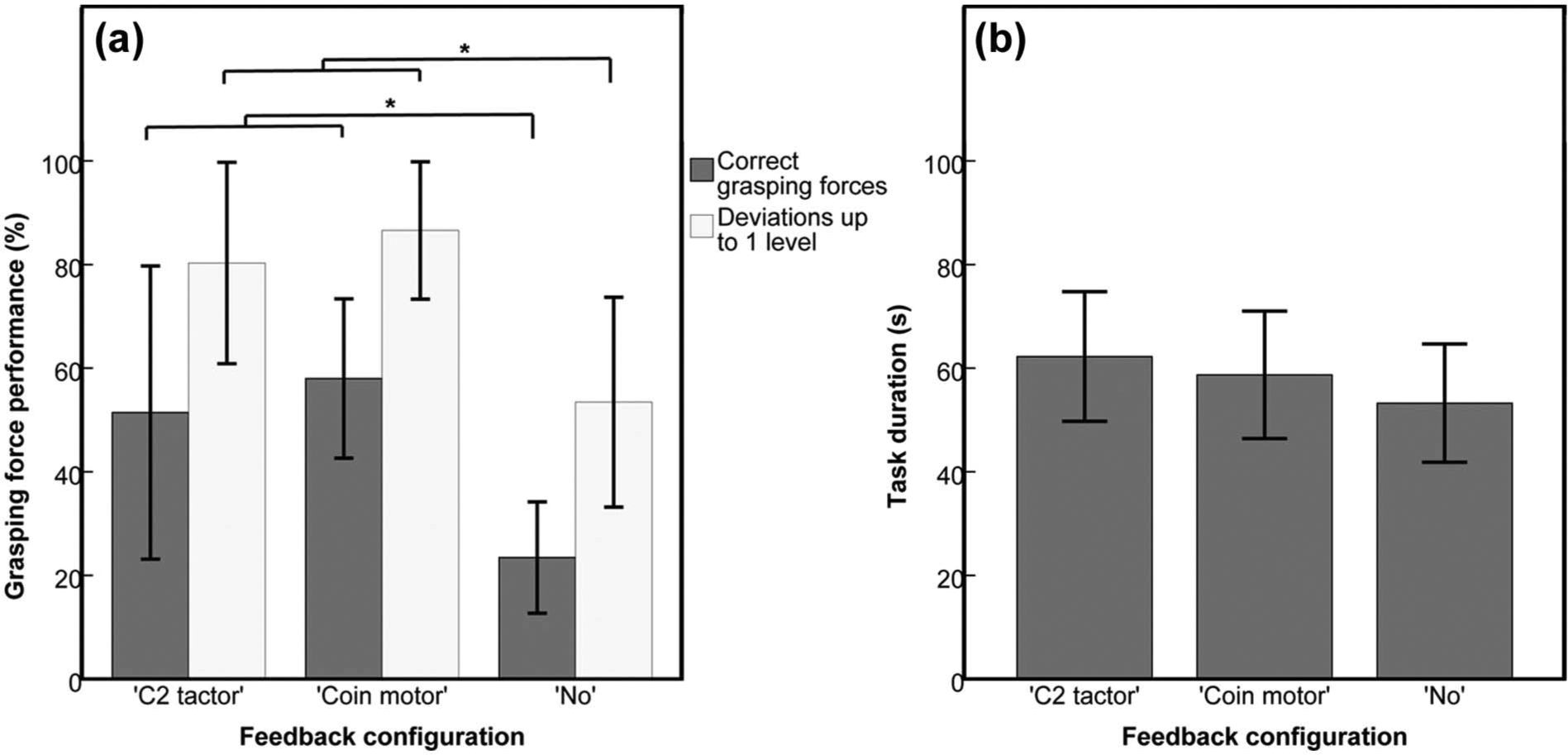
(a) Mean percentages of correct grasping forces and percentages of grasping forces deviating maximally one level and (b) mean task durations.
Repeated-measures ANOVA was performed to evaluate the differences in grasping performance between the two vibrotactile feedback conditions and the control condition with no feedback. The percentages of correct grasping forces as well as the percentages of grasping forces deviating up to one level differed significantly between the two feedback configurations (p < 0.001). Therefore, Bonferroni-corrected (p-values/3) post hoc paired samples t-tests were performed to evaluate these differences. No significant differences between the two vibrotactile feedback configurations were found (p-values > 0.05), but with vibrotactile feedback, the percentages of correct grasping forces and the percentages of grasping forces deviating maximally one level were significantly higher compared to those with no feedback (p-values between ≤0.001 and 0.002). No significant differences in task duration between the three conditions were found (p = 0.107), as shown in Figure 2(b).
Hand aperture feedback
The mean percentages of correct hand apertures and the mean percentages of hand apertures deviating maximally one level from the required aperture were calculated for each feedback configuration and are shown in Figure 3(a). Configurations are named according to the presence or absence of visual feedback (“YV” for visual feedback and “NV” for no visual feedback) and to the array orientation used (“T” for transversal and “L” for longitudinal).

(a) Mean percentages of correct hand apertures and percentages of hand apertures deviating maximally one level and (b) mean task durations.
Repeated-measures ANOVA showed that the percentages of correct hand apertures, the percentages of hand apertures deviating maximally one level, and the task durations differed significantly between the five feedback configurations (p-values < 0.001). Bonferroni-corrected post hoc paired samples t-tests were performed to further evaluate these differences. A comparison between the transversal (“NVT”) and longitudinal (“NVL”) orientation did not show a significant difference for both percentages (p-values > 0.5). For both orientations, the combined visual and vibrotactile feedback condition resulted in significantly higher performance scores than the vibrotactile feedback–only condition (p-values < 0.001). The percentages of correct hand apertures were significantly higher for the vibrotactile feedback–only condition than that for the no-feedback condition (p = 0.04 for both orientations), which was also the case for the percentages of hand apertures deviating maximally one level (p = 0.008 for the transversal and p = 0.024 for the longitudinal orientation).
Task durations did not differ significantly between the two array orientations (p-values > 0.4) and between the combined visual and vibrotactile feedback and the vibrotactile feedback–only conditions (p-values of 1). When using vibrotactile feedback only via a transversal-oriented array, the task duration did not differ significantly from that when using no feedback (p = 0.102), but for the longitudinal-oriented array, a marginal increase in task duration was found (p = 0.046) as shown in Figure 3(b).
Comparison with healthy subjects
The results from both studies on healthy subjects15,19 were combined with the results from this study and are presented in Figures 4 and 5. Unpaired samples t-tests showed that the percentages of correct grasping forces for subjects with upper-limb loss using the coin motor configuration were significantly lower (p = 0.011) than that for healthy subjects, but no significant differences were found in the other results for the grasping force feedback experiments. When visual feedback was provided simultaneously with vibrotactile hand aperture feedback, healthy subjects scored significantly better on both outcome parameters (higher percentages and lower task durations, with p-values between 0 and 0.038). Task durations were only significantly higher for subjects with upper-limb loss compared to those for healthy subjects (p = 0.039) when using a longitudinal-oriented array.
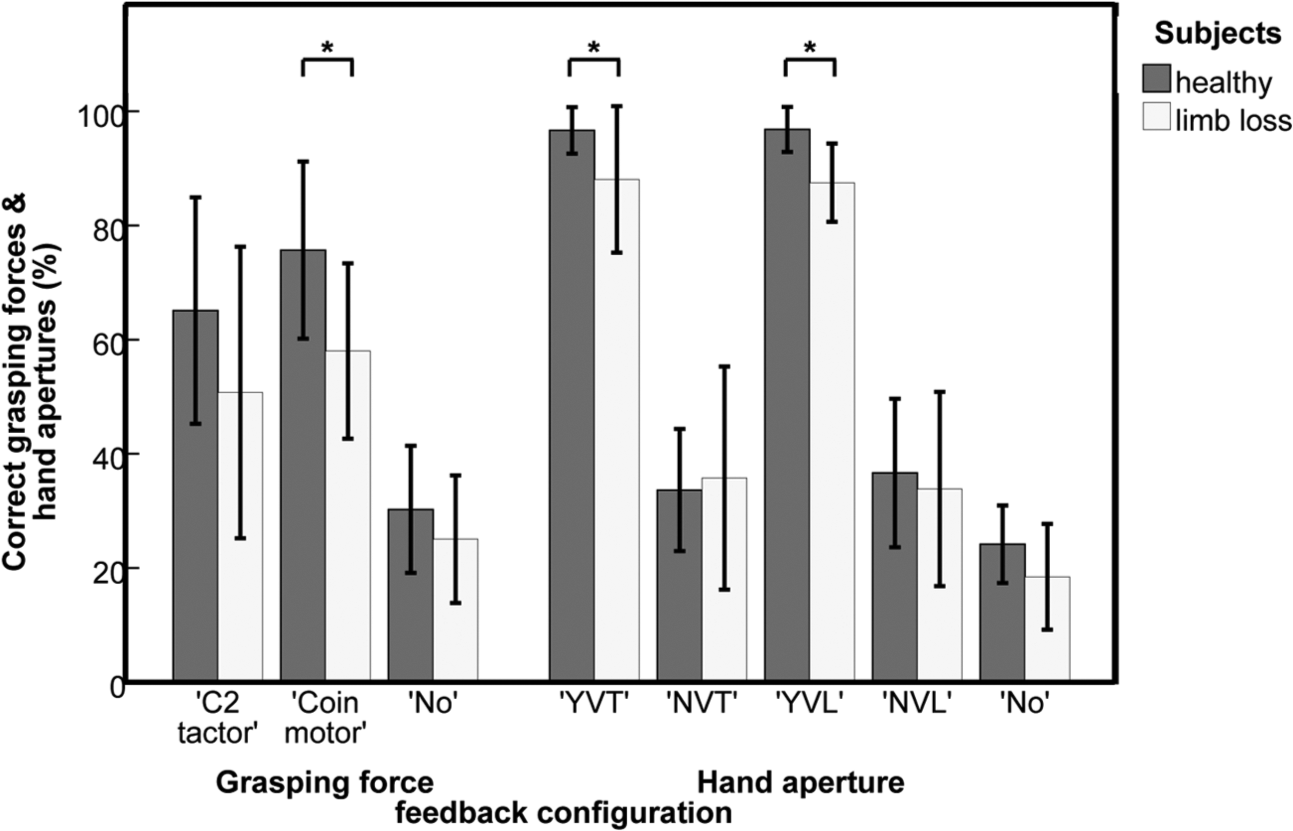
Comparison of percentages of correct grasping forces and hand apertures between healthy subjects and subjects with upper-limb loss.
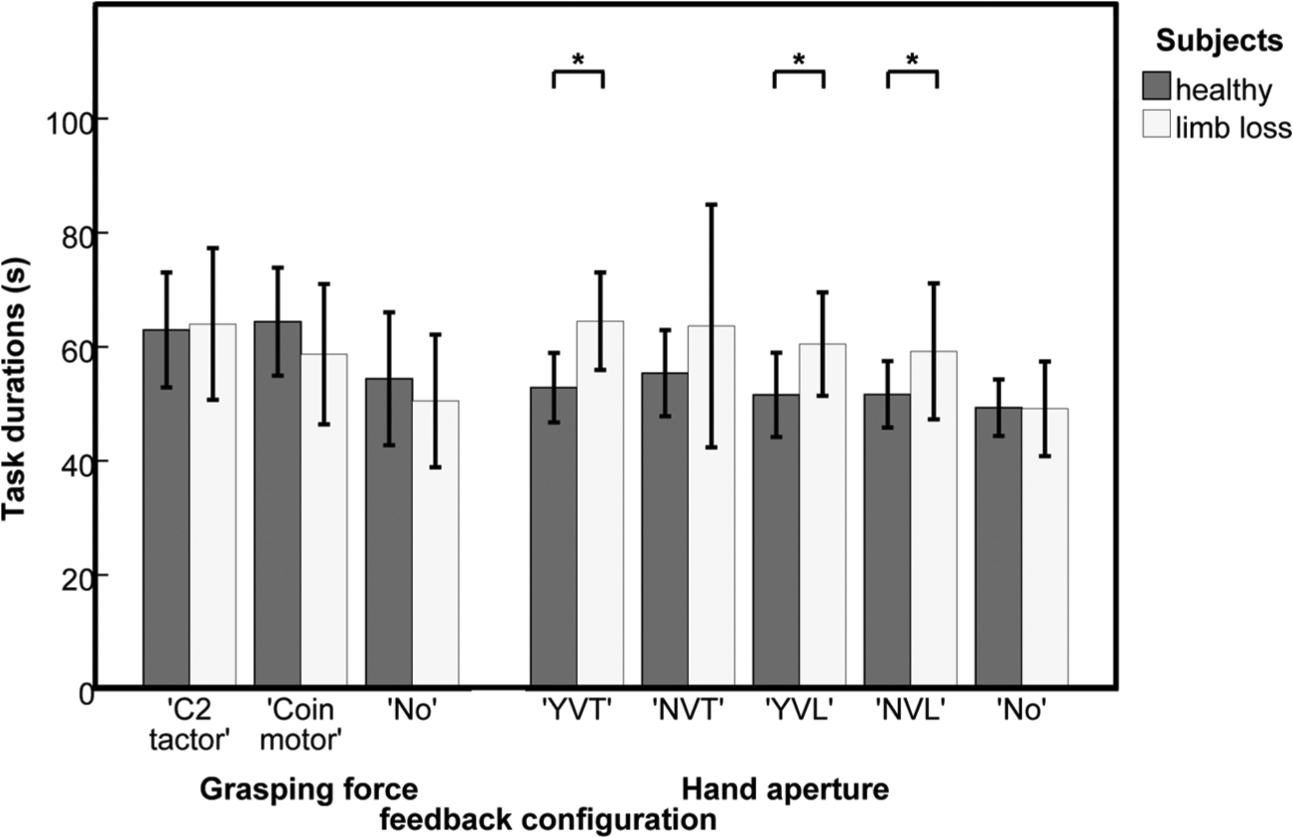
Comparison of task durations between healthy subjects and subjects with upper-limb loss.
Discussion
Grasping force feedback
The addition of vibrotactile grasping force feedback significantly increased the percentages of both the correct grasping forces and the grasping forces correct within one level compared to those without the addition of feedback. Therefore, it was concluded that the vibrotactile grasping force feedback could be interpreted by the amputee and congenital defect subjects. In the literature, positive results in relation to the vibration amplitude of a C2 tactor tothe applied normal force have been reported already. 8 However, this study was also performed with healthy subjects, using a completely different setup. Other studies, using frequency modulation of a single coin motor, 9 a C2 tactor 10 or an array of coin motors, 14 did not show an increase in performance compared to situations without vibrotactile force feedback. None of these studies included measurements on subjects with upper-limb loss. The only study on subjects with upper-limb loss, which involved the use of a single coin motor with its frequency related to the grasping force, showed better control in grasping forces when feedback is provided. 13
Two grasping force feedback configurations were compared in our study because the best configuration could not be determined from existing literature. The C2 tactor was selected because it is commonly used in experimental studies and the local increase in vibration amplitude would be most intuitively related to the localized sensation of pressure at the skin. The array of coin motors was selected because it showed promising results in a previous study on hand aperture feedback and is relatively cheap to implement. 19 No significant differences in grasping performance between the two configurations were found in our study. It should be investigated in future studies which feedback method can be best combined with hand aperture feedback and with EMG (electromyographic) control of the prosthesis.
Hand aperture feedback
When only vibrotactile feedback was provided, the percentages of correct hand apertures were around 35%, which is not very high, especially if compared to those when additional visual feedback was provided (percentages of around 90%). However, the percentages increase to around 75% if the percentages of hand apertures deviating maximally one level were considered. Furthermore, even for the percentages of correct hand apertures, the results for the experiments with only vibrotactile feedback were significantly better compared to those with no feedback, which shows that vibrotactile hand aperture feedback can be useful in situations where the prosthesis is out of view. Task durations were not significantly longer for the vibrotactile-only feedback situation compared to those for the no-feedback and visual-feedback situations, which indicates that the interpretation of vibrotactile feedback did not require significantly more time.
The comparison between the transversal and longitudinal array orientations did not show any significant differences in the performance measures, except for a marginal increase in the task duration for the longitudinal orientation in comparison with that for the no-feedback situation. In studies by Green 31 and Cody et al., 32 better localization performances were found for transversal-oriented arrays, which were explained by the asymmetric shape and orientation of the receptive fields of the mechanoreceptors with smaller diameters in the transversal direction. However, localization performance can also be increased when stimulators are placed near bony landmarks, 33 as was the case for the longitudinal orientation (stimulators over the elbow joint and near the end of the residual limb). Stimulators were placed on the upper arm with equal inter-stimulator distances for both arrays. The mean inter-stimulator distance was around 3 cm, which is just within the range of the spatial acuities found for the forearm (2–3.5 cm), 34 thus making it nearly impossible to reach perfect performance in identifying the correct hand apertures. The number of stimulators placed on the upper arm depended on the length of the residual limb, but on average four stimulators were placed on the upper arm. An advantage of the transversal array is that it can be completely incorporated in the prosthesis, but two possible disadvantages are the interference with the electrodes needed for the prosthesis control and the limited amount of space available in the prosthesis socket, both of which should be investigated in future studies.
Comparison with healthy subjects
In the hand aperture feedback experiments, healthy subjects showed higher performance with visual feedback, which is probably caused by their greater exposure to computers and to experimental studies, the latter of which was totally new for the subjects with upper-limb loss. The slightly higher task durations for subjects with upper-limb loss could have been caused by the higher age of the subjects, because reaction times decrease with increasing age. 35 Furthermore, in a study by Stevens and Choo, 34 it was shown that spatial acuity diminishes with aging. However, these differences in spatial acuity may have been counteracted in this study by the improvement in the spatial acuity of amputees which was reported in other studies.23,24
Beforehand, it was not possible to predict how subjects with upper-limb loss would perform in vibrotactile feedback experiments in comparison to healthy subjects, because there is no consensus on possible sensitivity differences. Our study showed that these differences, even if present, did not influence the usefulness of vibrotactile feedback, because the performance results for subjects with upper-limb loss were highly similar to those of healthy subjects.
Methodological considerations
To be able to compare the results of this study with the results from the previous studies on healthy subjects, the same virtual setup was used. This setup had been designed to ensure that the natural sensory pathways of the healthy subjects were blocked. The “clicks” from the mouse scroll were removed and the gain relating the mouse scrolling to the hand aperture or grasping force was randomized to eliminate any clues about the hand aperture or grasping force. The success of this method was demonstrated by the low percentages of correct hand apertures and grasping forces in the no-feedback situations, which were around guessing level.
In this study, the virtual hand was controlled by the sound arm, while feedback was provided to the residual limb. Mouse scroll control was used to enable a comparison of the results from this study with those from previous studies on healthy subjects.15,19 In these latter studies, feedback was provided to the same arm used to control the virtual hand, which could have contributed to some differences in performance. EMG control of the virtual hand was excluded from these studies because preliminary tests showed that EMG control required a long training period and resulted in a high variability in the grasping performance between different subjects. However, in future studies, with a shorter protocol and a longer training period, it should be investigated whether EMG control influences the interpretation of vibrotactile feedback. Furthermore, it is preferable to evaluate the various feedback configurations in real-life grasping tasks with upper-limb loss subjects using a myoelectric prosthesis.
Conclusion
Vibrotactile grasping force feedback and hand aperture feedback both improve the performance of subjects with upper-limb loss in virtual grasping tasks, as shown by the higher percentages of correct grasping forces and correct hand apertures. No significant differences in grasping performance were found between the various feedback configurations. It should be evaluated in future studies which feedback configurations are optimal when combining the two feedback methods in one system and when performing daily-life grasping tasks with a real myoelectric prosthesis.
Footnotes
Acknowledgements
The authors would like to thank Jeroen Olsman and Hans Konter for their help with the recruitment of amputee and congenital defect subjects and Nick Fung for his critical review of the grammar.
Conflict of interest
None declared.
Funding
This work was supported by the Ministry of Economic Affairs and the Province of Overijssel within the Pieken in de Delta (PIDON) initiative, under grant PID082035/1.6.1b.