
Abstract
Background:
An ankle–foot orthosis using an oil damper is designed to enable natural movement of the ankle joint. Wearing an ankle–foot orthosis using an oil damper has been demonstrated to assist the first rocker in stroke patients, but its effect on their gait when not wearing it is unclear.
Objectives:
To determine the effect of use of ankle–foot orthosis using an oil damper on the gait of stroke patients with hemiparesis when not wearing the ankle–foot orthosis.
Study design:
Crossover study.
Methods:
The gait of eight stroke patients in the chronic phase when not wearing an ankle–foot orthosis was measured, using a three-dimensional motion analysis system, before using the ankle–foot orthosis using an oil damper and then without and with using the ankle–foot orthosis using an oil damper after 3 weeks of use. Differences in gait were compared between the three measurement conditions.
Results:
Use of ankle–foot orthosis using an oil damper significantly decreased preswing time and significantly increased the positive ankle joint power in stance when not wearing the ankle–foot orthosis using an oil damper.
Conclusions:
These changes indicate the promising therapeutic effects of ankle–foot orthosis using an oil damper use and suggest the ankle–foot orthosis using an oil damper’s potential as a therapeutic device.
Clinical relevance
After 3 weeks of use of an ankle–foot orthosis using an oil damper, which assists the first rocker, the gait of stroke patients in the chronic phase when not wearing the ankle–foot orthosis using an oil damper was improved. Preswing time was significantly decreased and positive ankle joint power was significantly increased. The ankle–foot orthosis using an oil damper, which assists the first rocker function with natural movement of the ankle joint during gait, has the potential to improve the gait of stroke patients after immediate-term use.
Background
The gait of stroke patients is characterized by decreased walking speed, asymmetry, increased energy cost, foot drop, and insufficient muscle activity in stance.1–5 To overcome these problems, and especially to compensate for the insufficient muscle activity in stance and maintain clearance in swing, wearing an ankle–foot orthosis (AFO) is clinically useful, and many studies have shown the positive effects of their use. Most of these studies have compared gait with and without AFO use, 6 gait with AFOs of different design,7–9 or alignment of the AFO with footwear. 10 The results of these studies indicate that wearing an AFO can positively affect gait speed, temporal and distance factors, and joint kinematics and kinetics of the ankle and knee joints, but the effects of AFO use on gait when not wearing an AFO have not been shown.
Besides AFO use, another conventional treatment to improve foot drop in stroke patients is functional electrical stimulation (FES), which is designed to elicit ankle dorsiflexion during the swing phase of the paretic limb by stimulating the peroneal nerve for an adequate duration of the gait cycle. 11 Prolonged use of FES has resulted in better dorsiflexion in the swing phase and, in some cases, physiological improvements such as increased muscle strength and increased joint range of motion (ROM).12,13 Furthermore, walking speed can be increased even when the device is turned off.14,15 Such changes are referred to as a therapeutic effect. Everaert et al. 16 compared changes in walking speed and the physiological cost index (PCI) after 6 weeks of FES and AFO use in a randomized controlled trial involving 93 stroke patients. They found that both the FES and AFO had significant orthotic and therapeutic effects, but the FES had a larger therapeutic effect, and stated that one of the reasons for the AFO’s smaller therapeutic effect was the restriction placed on ankle joint movement during gait with conventional AFOs.
Most conventional AFOs restrict ankle joint movement during gait in order to stabilize the ankle joint in stance and maintain clearance in swing. However, a dual carbon fiber spring AFO (CFO) that was specially designed to allow natural movement of the ankle joint during gait was shown to produce a significantly larger ankle ROM during push-off compared to the common posterior leaf-spring AFO. 17 The CFO assisted the first and second rocker functions but did not improve the third rocker. With the goal of improving rocker function, an AFO using an oil damper (AFO-OD) was developed to assist the first rocker during gait. 18 The mechanical joint of the AFO-OD has a larger ROM than conventional AFOs, moving to plantar flexion with resistance and into dorsiflexion freely. An improvement of gait with the use of the AFO-OD has been shown in previous studies,19,20 but its effect on the gait when not wearing the device has yet to be demonstrated. To this end, this study aimed to determine the effect of AFO-OD use on the gait of stroke patients when not wearing the device. In our previous study comparing stroke patients’ gait before and after short-term AFO-OD use, temporal and distance factors as well as peak plantar flexor moment in stance were all found to be significantly improved after 3 weeks of use. 20 We regarded these changes as suggestive of the therapeutic effect of AFO-OD use. Thus, in this study, we tested the hypothesis that the AFO-OD would show a therapeutic effect by improving the temporal and distance factors and peak plantar flexor moment of stroke patients when not wearing the AFO-OD.
Method
Features of the AFO-OD
An AFO-OD (GaitSolution Design; Kawamura Gishi, Osaka, Japan) that was originally developed to assist the first rocker function was used in this study (Figure 1). The mechanical features of the AFO-OD are described in detail elsewhere.18,21 A schematic illustration of the gait assistance provided by the AFO-OD is shown in Figure 2. The device assists the first rocker function by the resistive force generated by an oil damper attached to the ankle joint. It assists insufficient eccentric contraction of the dorsiflexors to prevent abrupt landing of the forefoot and pulls the shank forward in the loading response. The mechanical joint of the AFO-OD moves freely to dorsiflexion, which means that the AFO-OD does not offer any assistance for plantar flexor in the second rocker function. The AFO-OD generates resistance to prevent excessive plantar flexion of the ankle joint in the third rocker and swing phase.
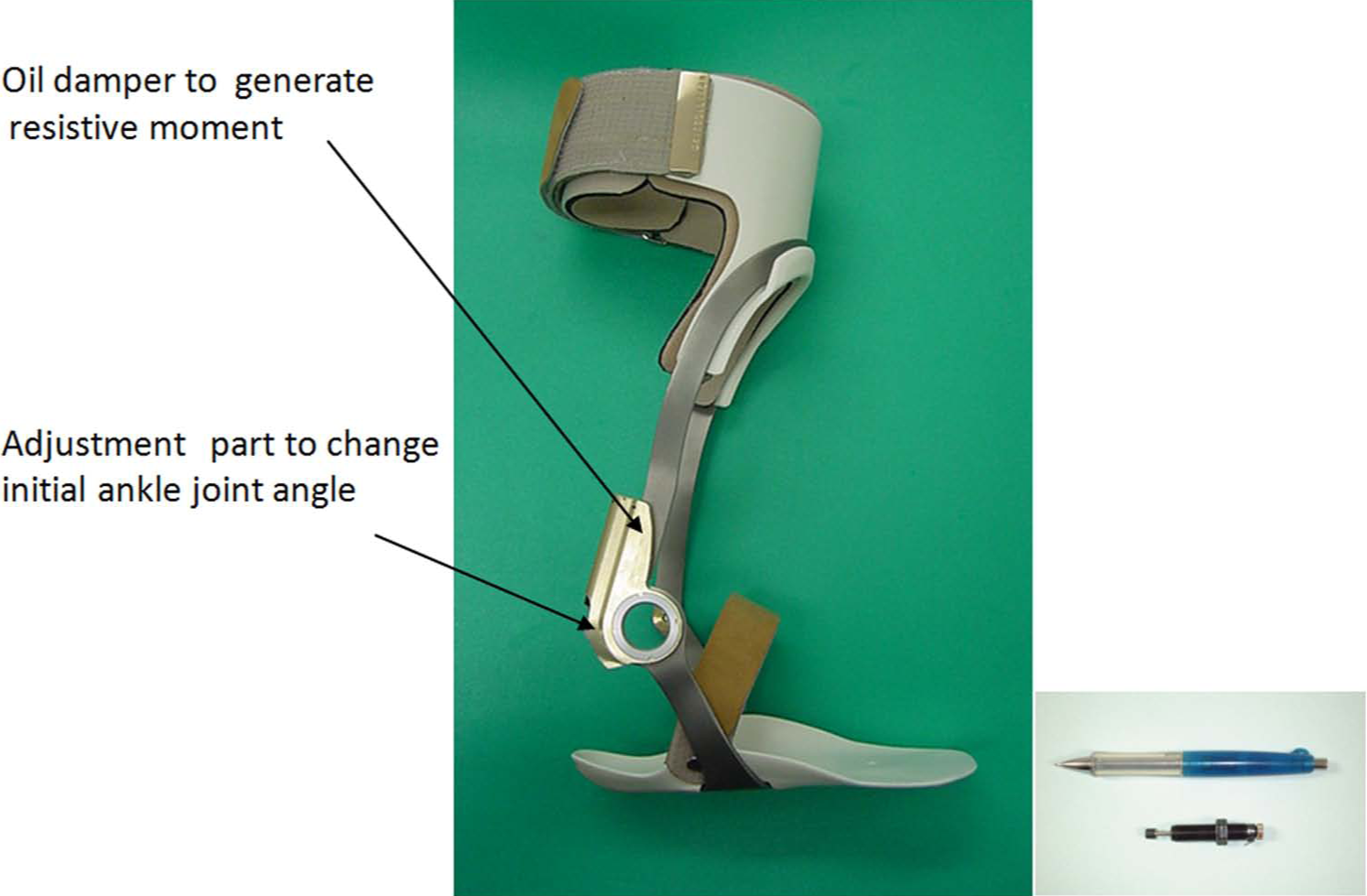
Structure of the ankle–foot orthosis using an oil damper (AFO-OD) used in this study.
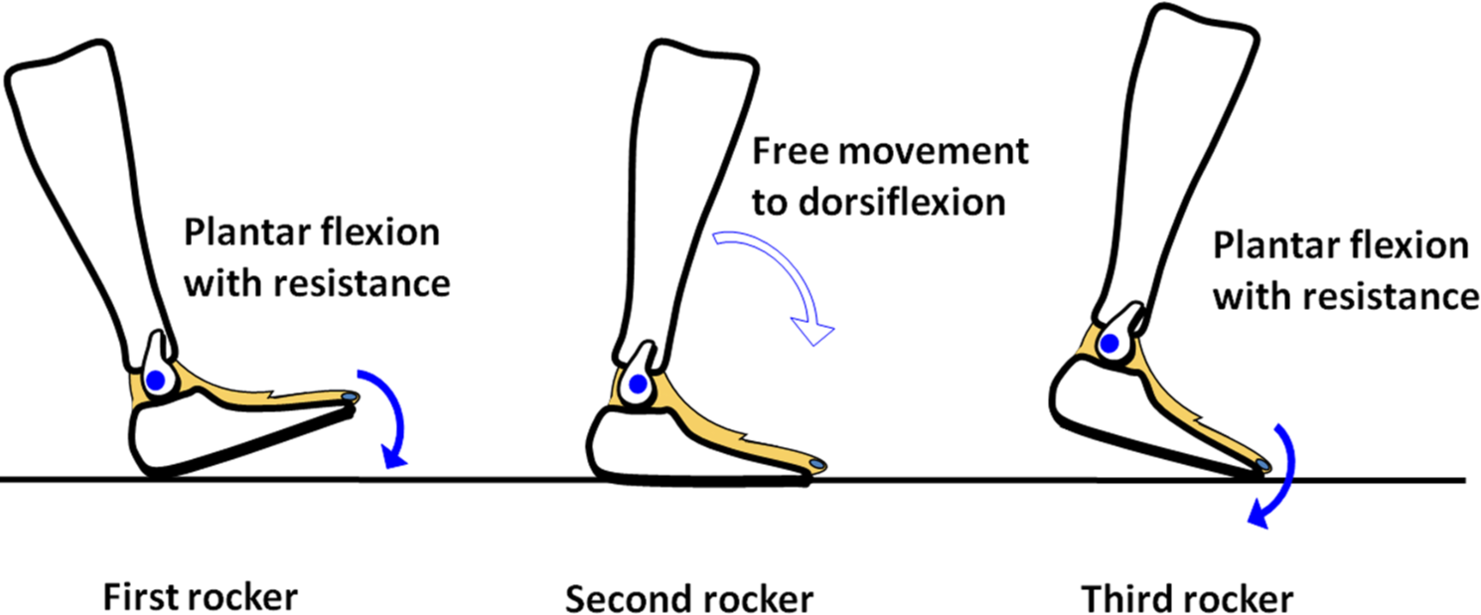
Schematic illustration of the effect of using the AFO-OD.
Patients and study protocol
Patients and the study protocol were the same as those in our previous study. 20 Briefly, eight stroke patients (five men, three women; mean age = 55.2 years) in the chronic phase with hemiparesis participated. Their clinical profiles are shown in Table 1. Patients were assigned as A–H according to walking speed, with Patient A being the fastest and Patient H the slowest. All patients attended one to three 20-min sessions per week in a general rehabilitation program run by physiotherapists before participating in this study. Walking speed was almost constant, as determined on the 10-m walk test.
Patient profiles.
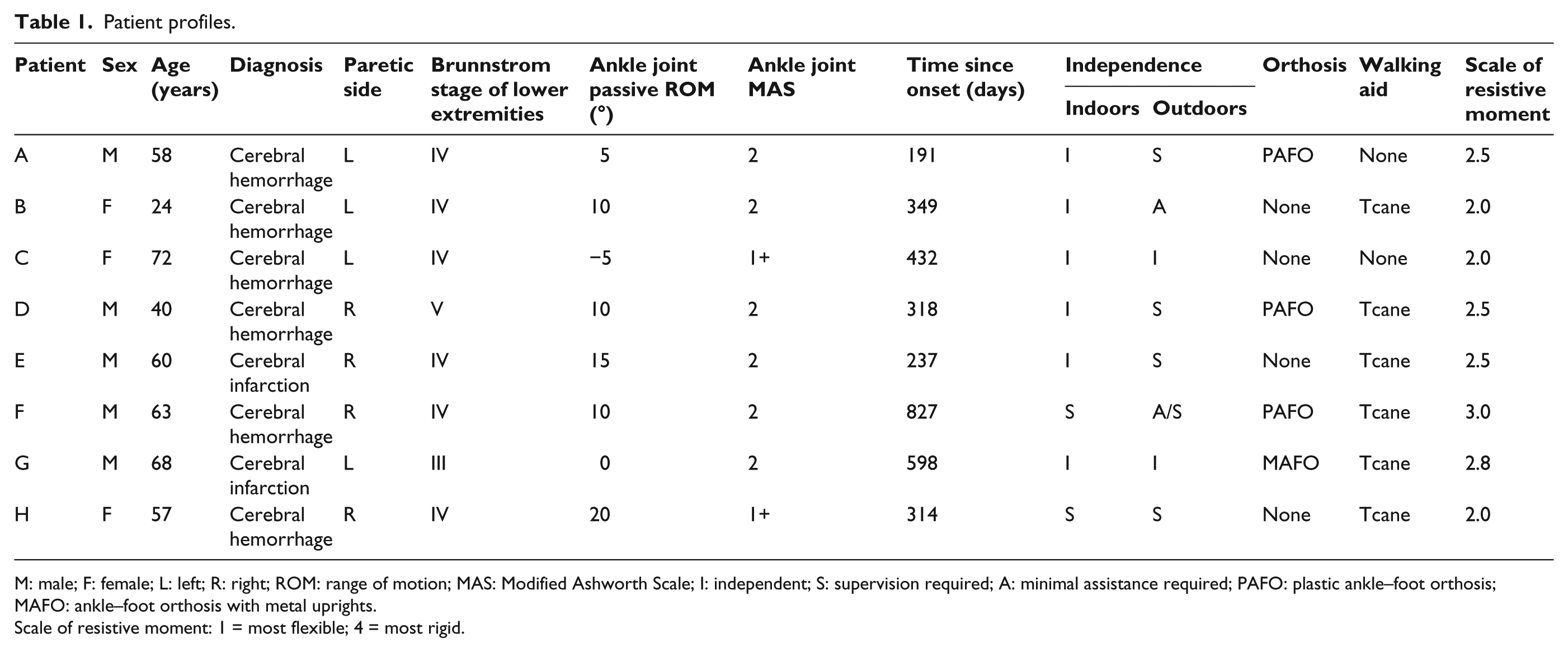
M: male; F: female; L: left; R: right; ROM: range of motion; MAS: Modified Ashworth Scale; I: independent; S: supervision required; A: minimal assistance required; PAFO: plastic ankle–foot orthosis; MAFO: ankle–foot orthosis with metal uprights.
Scale of resistive moment: 1 = most flexible; 4 = most rigid.
Gait was measured using a three-dimensional (3D) motion analysis system (10 Vicon MX cameras (Oxford, UK) and 6 AMTI force plates (Watertown, USA)). A total of 16 reflective markers were attached to the body and the trajectory of markers and the force plate data were measured at a sampling frequency of 100 Hz. Patients wore their own shoes in all measurements. First, gait with shoes but without an AFO was measured at the patient’s preferred walking speed. Measurements were repeated until five steps of the affected limb on the force plates were obtained. The patients then started using the AFO-OD. The magnitude of the resistive moment and the initial ankle joint angle of the AFO-OD were tuned by orthotists to each patient’s condition according to the physiotherapist’s observation and the patient’s opinion. The tuning of the resistive moment was made to achieve smooth foot contact during loading response. The initial joint angle was adjusted so that the resistive moment started to generate from the ankle joint angle on initial contact. The initial ankle joint angle was neutral for all patients. The scale of the resistive moment in each patient is shown in Table 1. The resistive moment of AFO-OD was tuned in the range of 1 (most flexible) to 4 (most rigid), but actual resistive moment was unknown because it depended on the speed of compression of the damper during gait.
When the patients were comfortable with the tuned AFO-OD, they started using it for 3 consecutive weeks. During this 3-week period, they wore the AFO-OD daily, and while wearing it, they continued to participate in their regular 20-min gait training sessions one to three times per week run by the physiotherapists. After 3 weeks, gait without the AFO-OD and then with it were measured following the same protocol. Thus, data on the patients’ gait were obtained in three conditions: without an AFO before use of the AFO-OD, without the AFO-OD after 3 weeks of use, and with the AFO-OD after 3 weeks of use.
All procedures were approved by the local ethics committee of Seiai Rehabilitation Hospital and were consistent with the Declaration of Helsinki. Informed consent was obtained from all patients prior to their participation in the study.
Data processing
The trajectory of markers and the force plate data were low-pass filtered by a second-order Butterworth filter with a cutoff of 6 Hz. An inverse dynamic model was employed and in each condition the following parameters were determined (Table 2): temporal and distance parameters; lateral sway of the center of gravity; peak value of the anterior/posterior component of floor reaction force; peak value of the joint angles and the internal joint moments of the ankle, knee, and hip joints; and negative and positive peak power around the ankle joint. Data on floor reaction force, joint angle, joint moment, and power were obtained for the paretic limb. Joint moment was normalized by the height and weight of each patient, and power and floor reaction force were normalized by body weight.
Median and interquartile range for gait parameters of the three walking conditions (n = 8), and results of statistical analysis.
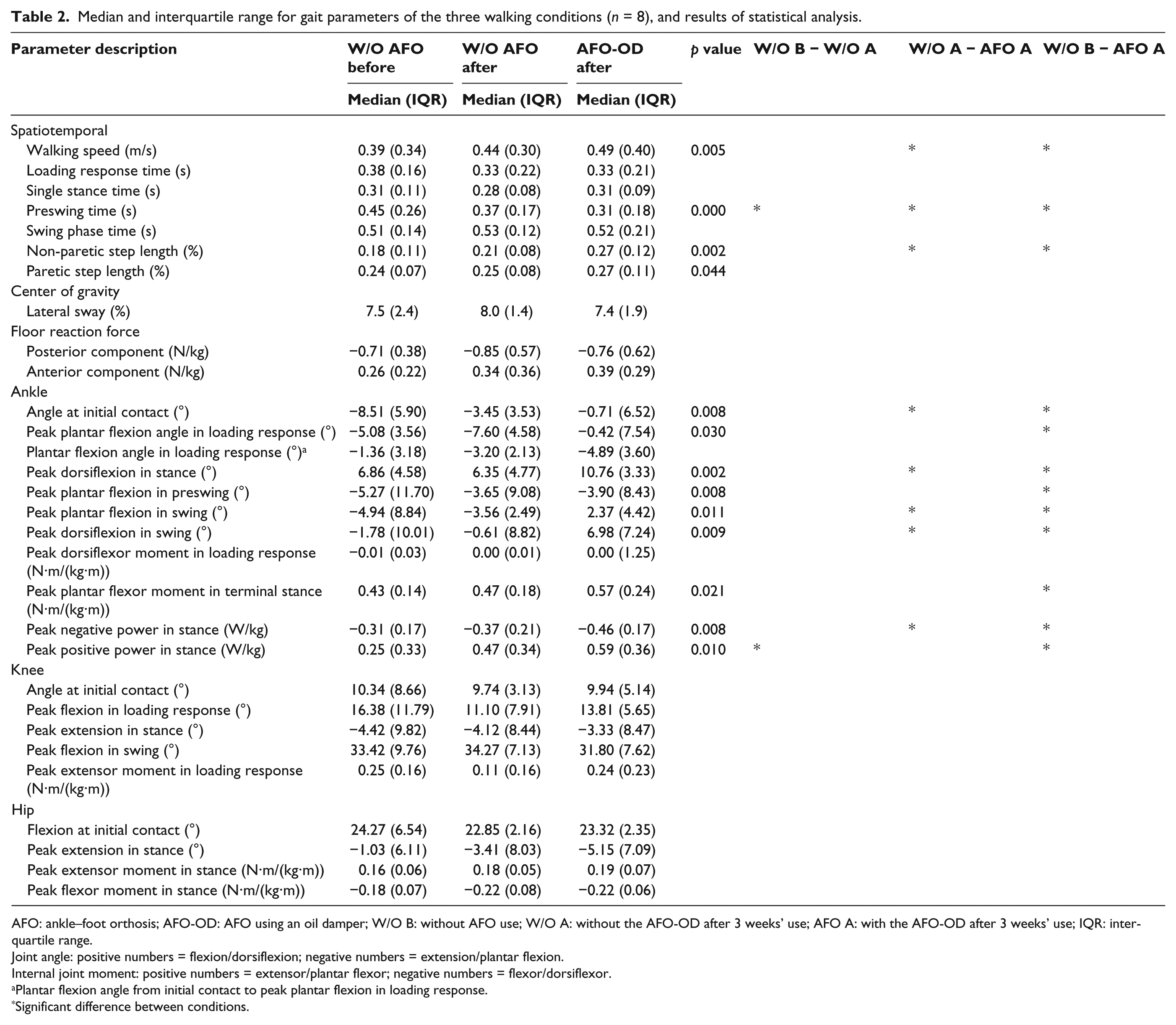
AFO: ankle–foot orthosis; AFO-OD: AFO using an oil damper; W/O B: without AFO use; W/O A: without the AFO-OD after 3 weeks’ use; AFO A: with the AFO-OD after 3 weeks’ use; IQR: interquartile range.
Joint angle: positive numbers = flexion/dorsiflexion; negative numbers = extension/plantar flexion.
Internal joint moment: positive numbers = extensor/plantar flexor; negative numbers = flexor/dorsiflexor.
Plantar flexion angle from initial contact to peak plantar flexion in loading response.
Significant difference between conditions.
Statistical analysis
The gait parameters were determined and averaged for at least five gait cycles in each of the three experimental conditions. To exclude the effect of outliers in this small test group, nonparametric statistical analyses were performed. First, Friedman’s analysis was performed to determine whether there was a significant difference between the three conditions. If a significant difference was found, then further comparisons were made between walking (1) without an AFO before AFO-OD use, (2) without an AFO-OD after 3 weeks of use, and (3) with the AFO-OD after 3 weeks of use. Bonferroni’s correction was applied to reduce the likelihood of obtaining false-positive results. Statistical significance was established at a p value of 0.05 for Friedman’s analysis, and it was adjusted by the number for post hoc comparisons. SPSS version 21 for Windows was used for all statistical analyses.
Results
Figure 3 shows representative results of a single gait cycle in the case of Patient B (Table 1). For each of the three conditions, ankle joint angle is shown in Figure 3(a), ankle joint moment in Figure 3(b), and ankle power in Figure 3(c). The ankle joint angle was more dorsiflexed in swing phase when the patient walked with the AFO-OD after 3 weeks of use. The joint moment was shown as the internal joint moment with positive plantar flexor moment. The smallest values of peak plantar flexor moment in late stance and negative power in mid stance were seen during gait without an AFO before AFO-OD use and these values had both increased after 3 weeks of AFO-OD use. The peak positive power in late stance was small during gait before use of the AFO-OD and was largest during gait after 3 weeks of use without using the AFO-OD, although it was decreased when using the AFO-OD.
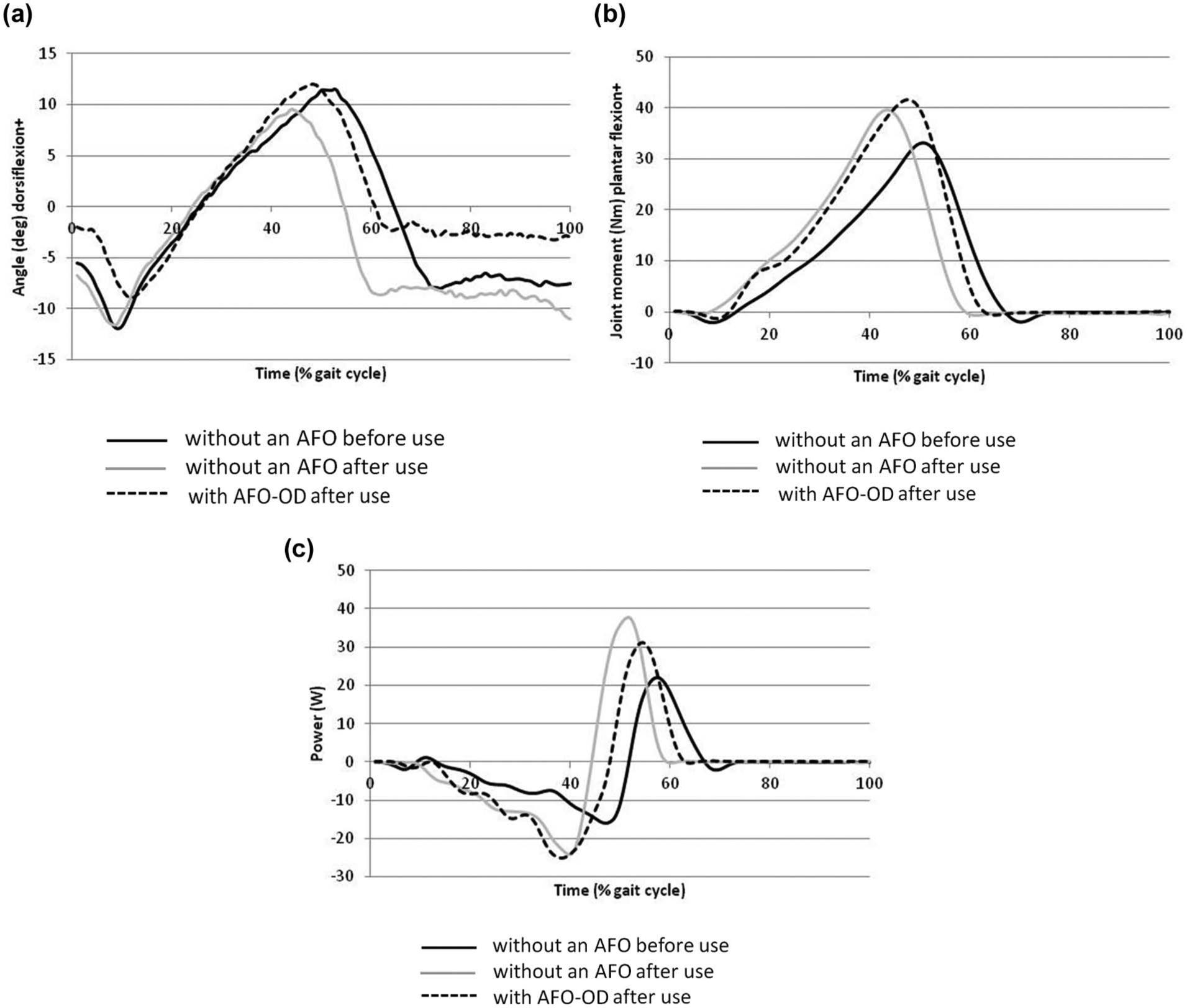
Representative gait parameter results of a single gait cycle for Patient B under the three conditions of AFO use: (a) ankle joint angle, (b) ankle joint moment, and (c) ankle joint power.
Gait data from the eight patients and the results of statistical analysis are shown in Table 2. Friedman’s analysis showed significant differences in temporal and distance parameters as well as ankle joint angle, moment, and power. The change in the ankle joint angle was a direct effect of AFO-OD use. Differences in gait parameters, calculated by pairwise comparison, for without an AFO before AFO-OD use (W/O B) and without the AFO-OD after 3 weeks of use (W/O A) suggested a therapeutic effect of the AFO-OD (Table 2, left column, W/O B − W/O A). Differences in gait between without and with the AFO-OD after 3 weeks of use showed an orthotic effect (Table 2, middle column, W/O A − AFO A). Moreover, combined effects were seen (Table 2, right column, W/O B − AFO A). Most of the differences found showed orthotic and combined effects. In terms of the therapeutic effect, preswing time was significantly decreased and peak positive power was increased when walking without the AFO-OD after 3 weeks of use. A comparison of gait without an AFO before AFO-OD use and without the AFO-OD after 3 weeks of use revealed increases in walking speed, non-paretic step length, peak plantar flexor moment in terminal stance, and peak negative power, although these changes were not significant.
Results of the parameters for which AFO-OD use suggested a therapeutic effect are shown for the eight patients in Figure 4. Preswing time was markedly decreased in most patients without using the AFO-OD after 3 weeks of use. In addition, peak positive ankle power was increased without using the AFO-OD after 3 weeks of use in most patients, but was decreased during gait with the AFO-OD in some patients.
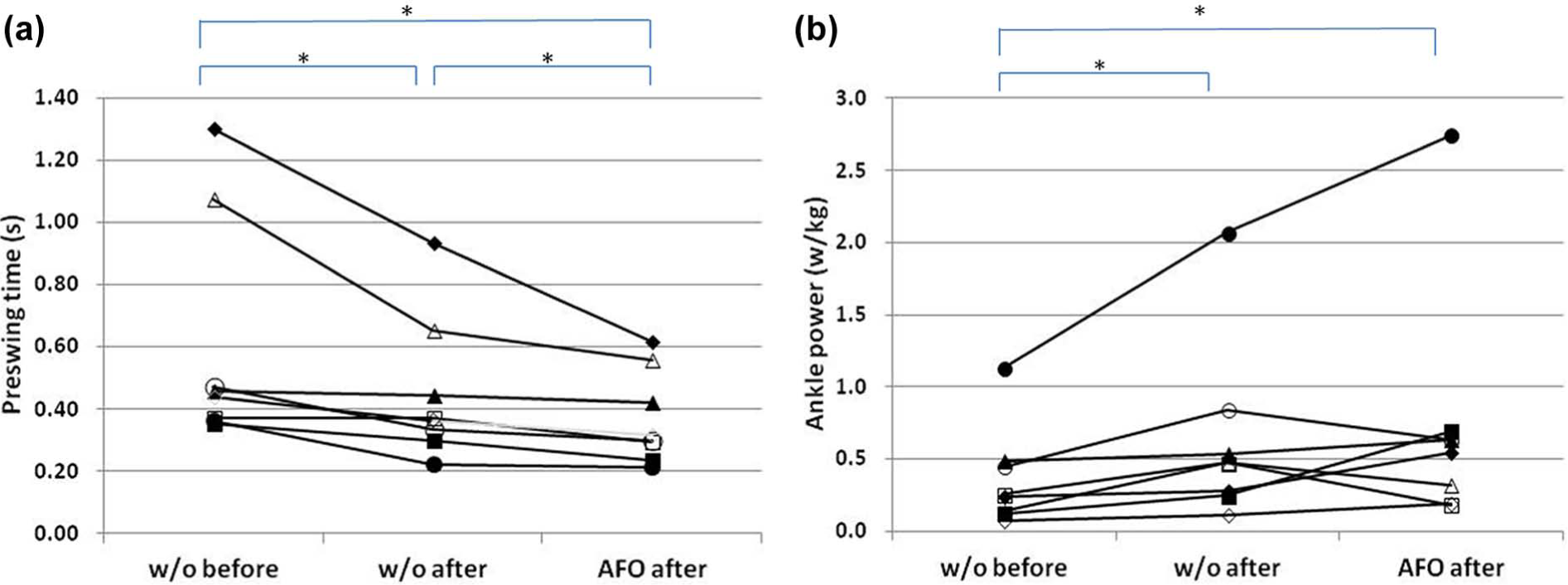
Change in (a) preswing time and (b) positive ankle joint power in stance under the three experimental conditions in Patients A–H.
Discussion
Statistical analysis revealed that the orthotic effect was larger than the therapeutic effect following immediate-term use of the AFO-OD. This result is in agreement with that of a previous study. 16 In terms of the therapeutic effect, walking speed, non-paretic step length, peak plantar flexor moment in stance, and peak negative power in stance were all increased but not significantly. However, preswing time was significantly decreased and peak positive power was significantly increased during gait without the AFO-OD after immediate-term use. Thus, the hypothesis was partly supported by the results obtained in this study.
Many studies employing gait analysis in stroke patients have shown prolonged preswing time.1,22,23 Preswing is the period from the initial contact of the non-paretic limb to foot off of the paretic limb. In clinical practice, many patients experience difficulty with foot off of the paretic limb in late stance. Kramers de Quervain et al. 24 found that preswing time was prolonged in those patients with the slowest walking speed. From the results of this study (Figure 4(a)), preswing time was largely decreased after 3 weeks of AFO-OD use even when not wearing the device during gait. The amount of decrease was large in patients with a slow walking speed, namely, Patients F and G. Some patients including Patients F and G showed more upright posture of the trunk after 3 weeks of AFO-OD use even when they walked without an AFO. A previous study on the effects of AFO-OD use found that 99 stroke patients responded by questionnaire that the upright trunk posture was one of the main improvements they noticed from using the AFO-OD. 21 Improved trunk posture might mediate the reduced preswing time; however, there are no quantitative data to support this speculation at this time.
A possible therapeutic effect, but no orthotic effect, was observed for peak positive power. In previous studies, decreased power was one of the characteristics of stroke patients’gait.1,25 Power is calculated by multiplying joint moment and joint angular velocity during gait. The positive power in late stance is related to the internal plantar flexor moment of the ankle joint and the joint angular velocity to plantar flexion in preswing. After 3 weeks of AFO-OD use the peak plantar flexor moment was slightly increased in our patients. Joint angular velocity to plantar flexion is related to the ROM from peak dorsiflexion to plantar flexion at the end of the stance phase. It is also affected by the preswing time. The preswing time was decreased in all patients, as shown in Figure 4(a). However, ROM in preswing was affected by wearing the AFO-OD because the AFO-OD offered resistance to plantar flexion in order to prevent foot drop in the swing phase. This is the reason for peak positive power increasing in some patients (Patients A, C, E, G, and H) but decreasing in other patients (Patients B, D, and F) when they walked with the AFO-OD, as shown in Figure 4(b).
The AFO-OD was developed to assist the first rocker function, but the therapeutic effects of wearing the AFO-OD were found in late stance in this study. The oil damper assists the eccentric contraction of the dorsiflexors in loading response to facilitate smooth loading on the paretic limb. The ankle joint of the AFO-OD moves freely to dorsiflexion to allow natural movement of the ankle joint of the paretic limb in stance. Due to this function, in our previous study, we found peak plantar flexor moment was increased in stance when patients wore the AFO-OD. 20 These results indicate the possibility of using the AFO-OD as a therapeutic device but not one that can substitute for the insufficient function seen in stroke patients. However, since the mechanism of increasing the plantar flexor moment has not been clarified, further research is necessary to provide an evidence-based explanation.
Patients in the chronic phase of stroke participated in this study. Generally, such patients have difficulty improving their gait during short-term rehabilitation programs. In this study, all patients continued to receive general rehabilitation from physiotherapists at the same frequency as they did before participating in this study. Nevertheless, gait changes were observed in just 3 weeks. Thus, gait training using the AFO-OD, which moves to plantar flexion with resistance and dorsiflexion with no resistance, might facilitate natural movement of the ankle joint during gait. Another AFO that facilitates natural ankle joint movement during gait is the dynamic AFO. Nolan et al. 26 measured the gait of a single patient with stroke-related hemiplegia when wearing a dynamic AFO and found that the hip joint movement was markedly affected by wearing the device. This study found no changes in hip or knee joint kinetics or kinematics, probably because of the variation that comes with a larger number of participants.
The limitations of this study were the small number of patients, with variation in their profiles, and the lack of a control group. Further research with a larger number of patients and a control group is therefore necessary to explore the generalizability of these findings and to determine the characteristics of patients suitable for AFO-OD use. Another limitation concerned the factors affecting the therapeutic effect. We asked patients to maintain their usual level of activity during the 3-week study period but did not actually measure this. Thus, the therapeutic effect suggested in this study may have included increased activity levels due to motivation about participating in the study. Furthermore, the 3-week use of the AFO-OD is likely not long enough to produce a sustained therapeutic effect. Longer term effects of AFO-OD use in patients’ daily life should be studied to clarify the therapeutic and orthotic effects of using the device.
Conclusion
To explore the potential therapeutic effect of use of the AFO-OD, which facilitates natural movement of the ankle joint angle, the gait of eight stroke patients was measured, using a 3D motion analysis system and force plates, without an AFO before using the AFO-OD and then both without and with the AFO-OD after 3 weeks of use. An orthotic effect was found for increased walking speed, step length, dorsiflexed ankle joint angle, and peak plantar flexor moment in stance. Comparison of gaits without an AFO before and after 3 weeks of use revealed that preswing time was significantly decreased and positive ankle joint power was significantly increased after its use. These results suggest the AFO-OD’s potential as a therapeutic device.
Footnotes
Conflict of interest
None declared.
Funding
The research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.