
Abstract
Objective
To compare the kinematic effects of two widely-used prefabricated ankle–foot orthoses (AFOs), the Dyna Ankle (DA) and UD Flex (UD), on the gait cycle of patients with hemiplegia due to cerebral palsy or acquired brain injury.
Methods
This was a retrospective cohort study involving 29 patients. Gait analysis results were assessed under three conditions: barefoot, with the DA, and with the UD. Friedman tests and post hoc analysis with Bonferroni correction were performed to assess differences between the three conditions.
Results
The DA significantly improved ankle dorsiflexion during the mid-swing phase, making it more effective in correcting foot drop compared with the UD (DA: 2.28°, UD: 0.44°). Conversely, the UD was more effective in preventing knee flexion during the loading response (DA: 28.11°, UD: 26.72°).
Conclusions
The DA improved ankle dorsiflexion during the swing phase significantly more than that with the UD in patients with hemiplegia. Compared with the DA, the UD more effectively prevented increased knee flexion during the loading response. The choice to prescribe these orthoses should consider individual patient characteristics.
Keywords
Introduction
Patients with cerebral palsy (CP) and brain injuries frequently present with gait abnormalities owing to muscle weakness and spasticity.1–3 Gait impairments in the affected limbs result in abnormal kinematic characteristics and temporospatial asymmetries.4,5 Functional walking is a common rehabilitation goal in patients with CP and stroke because it is closely related to activities of daily living and a patient’s social life.6,7 Conventional rehabilitation therapy is performed to correct pathological gait patterns; however, lower extremity orthoses are widely-used to further correct gait abnormalities and improve walking efficiency.8–12
When prescribing ankle–foot orthoses (AFOs), it is important to carefully consider the available options, which can vary in terms of articulation, material, price, and whether they are prefabricated or custom-made. 13 Among the various types of AFOs, the Dyna Ankle® (DA; Ottobock HealthCare GmbH, Duderstadt, Germany) and the UD Flex® (UD; Advanfit Inc., Kumamoto, Japan) are widely used because they are prefabricated, light, easy to wear, and cost-effective.
Although the DA and UD are frequently-used prefabricated orthoses, few studies have compared the effectiveness of these orthoses to correct gait abnormalities.14,15 The DA has a posterior AFO design, while the UD has an anterior AFO design. On the basis of this information, we hypothesized that the DA would improve ankle dorsiflexion during the swing phase more significantly than that with the UD, while the UD would be more effective in preventing increased knee flexion during the stance phase compared with the DA. Furthermore, we hypothesized that the two orthoses may have different effects depending on the motor grade of the ankle. To investigate these hypotheses, we performed a retrospective study to assess the kinematic impact of the two orthoses on the gait patterns of patients with hemiplegia due to cerebral palsy or acquired brain injury. Furthermore, we performed a stratified analysis on the basis of ankle motor grade.
Materials and methods
Study population
We retrospectively collected data for patients with hemiplegia who visited the Rehabilitation Medicine Center of Yonsei University College of Medicine, Seoul, Korea, between January 2007 and December 2009. This study was approved by the Institutional Review Board of Severance Hospital, Yonsei University Health System, Seoul, Korea (2020-0706-002). Owing to the retrospective nature of the study, the review board waived the need to obtain informed consent. Furthermore, all identifiable patient information has been removed from the article. The reporting of this study conforms to the STROBE guidelines. 16
The inclusion criteria were as follows: 1) patients with CP or acquired brain injury who visited our Department of Rehabilitation Medicine with a complaint of gait impairment and 2) patients who underwent gait analysis under the following conditions: barefoot, with the DA, and with the UD. The exclusion criteria were patients with other neurological deficits, such as peripheral nerve injury, Parkinson’s disease, or multiple sclerosis. Figure 1 is the study flowchart.
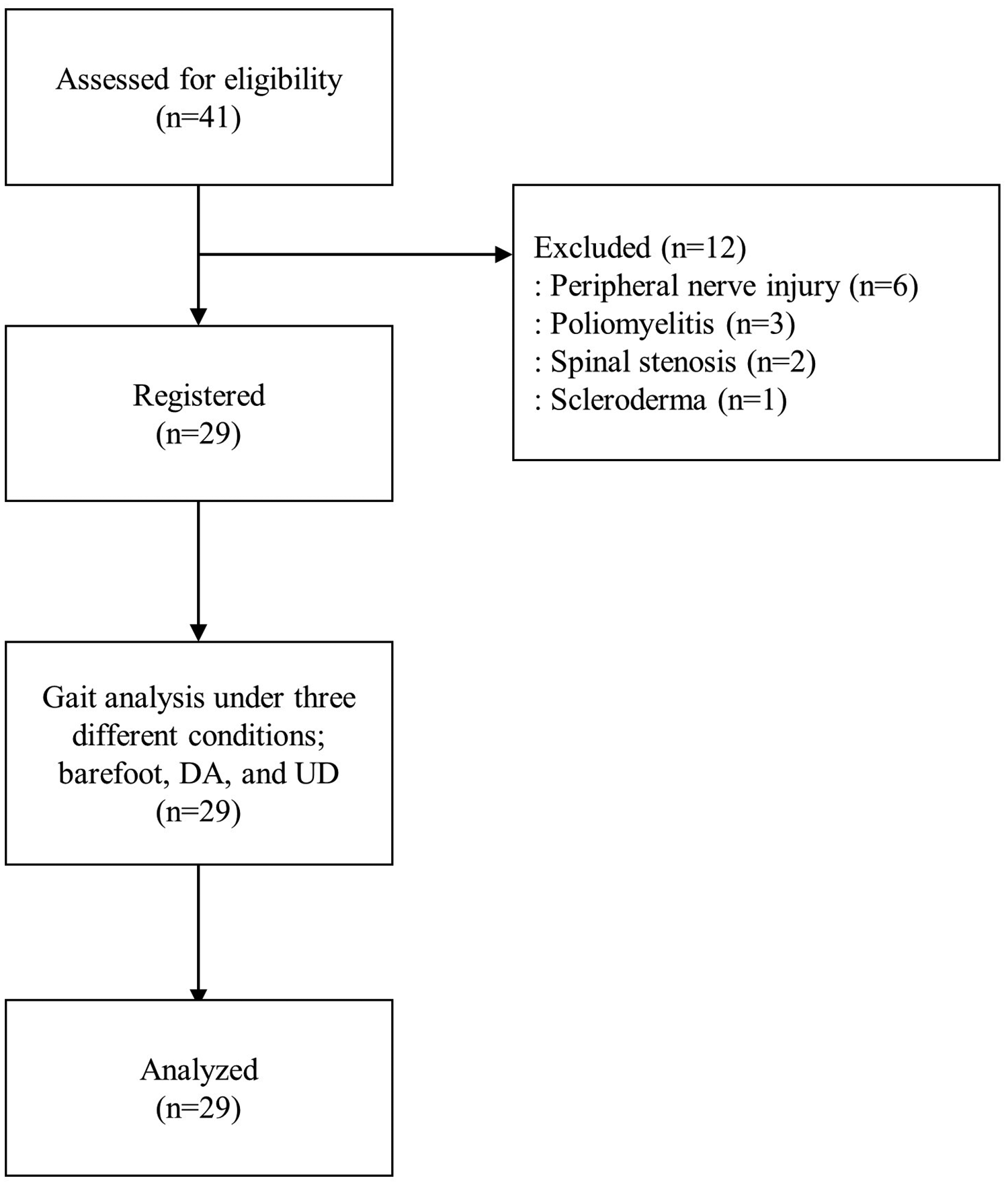
Study flowchart.
Procedure
A three-dimensional motion analysis system (Vicon Motion Systems, Ltd., Oxford, UK) was used to measure the gait performance of each affected limb. This system comprises six infrared-sensitive cameras to track fixed markers through space. Fifteen passively reflective markers were attached to each participant, as follows: sacrum, and bilaterally on the anterior superior iliac spine, thigh, lateral knee, tibia, lateral malleoli, second metatarsal head, and heel (Figure 2). All participants’ movements were video-recorded from the frontal and lateral views. Temporospatial data, namely cadence, stride time, stride length, step time, step length, speed, and foot off, were collected. Kinematic data, namely pelvic tilt angle, hip flexion/extension, knee flexion/extension, and ankle dorsiflexion/plantar flexion, were also collected. Kinematic data were plotted using Polygon software (Oxford Metrics, Yarnton, UK).

Placement of the 15 markers attached to each participant, as follows: sacrum, and bilateral anterior superior iliac spine, thigh, lateral knee, tibia, lateral malleoli, second metatarsal head, and heel.
Gait analysis was performed in a gait analysis laboratory equipped with a 10-m walkway at our rehabilitation center under three conditions: 1) barefoot walking, 2) walking while wearing the DA, and 3) walking while wearing the UD (Figure 3). The gait speed was set at the participant’s usual walking speed. During a single gait analysis session, three trials were performed; 120 steps was considered valid. The order of performing the gait analysis for each participant for the three conditions was randomly assigned. The degrees of anterior pelvic tilt, hip flexion, knee flexion, and ankle dorsiflexion were presented as positive values, while the degrees of posterior pelvic tilt, hip extension, knee extension, and ankle plantar flexion were presented as negative values. All gait analysis results were stored in the gait analysis laboratory database at our center, and the researchers accessed the database directly to extract the data.
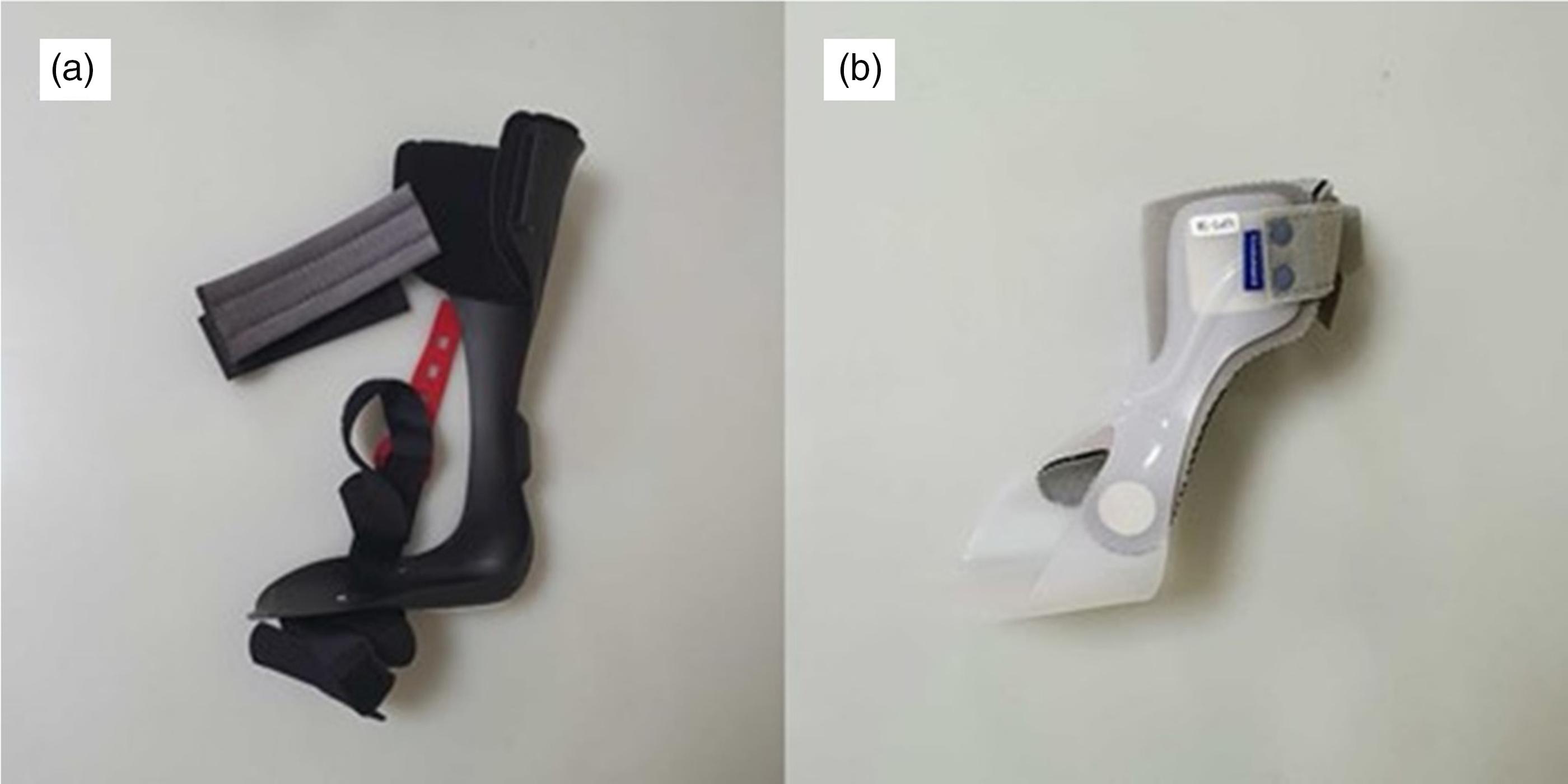
Lateral image of the Dyna Ankle (a) and UD Flex (b).
Statistical analysis
Simple descriptive statistics were used to characterize the samples and distributions of the variables. Data are presented as median (lower quartile, upper quartile) for variables such as age, and the kinematic data. To compare each participant’s performance under the three conditions (barefoot, and while wearing the DA or the UD), kinematic data were analyzed using the Friedman test. The results were considered significant at p < 0.05. Post hoc tests were performed using the Wilcoxon signed-rank test. For multiple comparisons, we verified the adjusted p-values of the post hoc test results using Bonferroni correction. A stratified analysis of gait kinematics was also performed for the three conditions on the basis of the motor grade of the ankle dorsiflexors, which was determined using the manual muscle test. 17 In this test, grade 3 is assigned when there is full range of anti-gravity joint movement. Consequently, the stratified analysis was categorized on the basis of a threshold of grade 3, dividing the data into ankle dorsiflexor motor grade ≥3 and <3 groups. All statistical analyses were performed using SPSS software version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Data for 41 individuals were assessed for eligibility; 12 were excluded, leaving 29 registered participants. All excluded individuals were capable of independent walking and able to understand instructions for the gait analysis. However, these individuals were excluded owing to the presence of other neurological deficits (n = 12: 6 with peripheral nerve injuries, 3 with poliomyelitis, 2 with spinal stenosis, and 1 with scleroderma).
The 29 participants who met our selection criteria comprised 18 men and 11 women, with a median age of 31.0 (20.0, 41.0) years. The median height of the participants was 165.0 (160.0, 173.0) cm, and the median weight was 64.0 (51.0, 72.0) kg. Of these participants, 10 were individuals with CP and 19 had acquired brain injury (10 with brain tumor, 5 with stroke, 2 with traumatic brain injuries, 1 with encephalitis, and 1 post-lobectomy). Fourteen patients had right hemiplegia, and 15 had left hemiplegia. The ankle dorsiflexor grades were as follows: 9 individuals had grade 1, 3 had grade 2, 12 had grade 3, and the remaining 5 had grade 4. The ankle plantar-flexor grades were as follows: 4 participants had grade 1 or 2, 13 had grade 3, and the remaining 8 had grade 4. Four participants were taking anti-spastic medication at the time of gait analysis, while 25 were not taking any medication. The median modified Barthel Index (MBI) score was 100 (90.0, 100.0). The median Functional Independence Measure (FIM) score was 123 (109.0, 126.0). For the locomotion item within the FIM, the median score was 13.0 (10.0, 14.0) (Table 1).
Participants’ characteristics.

Values are presented as median (lower quartile, upper quartile) or as number (%).
Analysis of temporospatial and kinematic data under the three different conditions
Temporospatial parameters, specifically cadence and stride time, exhibited significant differences according to the Friedman test results (both, p = 0.040) (Table 2). However, the post hoc Wilcoxon signed-rank test did not reveal significant differences between the conditions.
Comparison of spatiotemporal and kinematic data between barefoot, Dyna Ankle, and UD Flex conditions.

Values are presented as median (interquartile range).
For post hoc tests, the p-values were verified using Bonferroni correction.
B, barefoot; DA, Dyna Ankle; UD, UD Flex. *p < 0.05.
The Friedman test showed significant differences between barefoot, DA, and UD conditions for hip flexion at initial contact (p = 0.021), maximal knee flexion during the loading response (p = 0.001), maximal ankle dorsiflexion during stance (p < 0.001), ankle dorsiflexion during mid-swing (p < 0.001), ankle dorsiflexion during terminal swing (p < 0.001), and maximal ankle plantar flexion during push-off (p < 0.001). The post hoc Wilcoxon signed rank test results revealed no significant differences between the three conditions for hip flexion at initial contact. Significant differences were observed between barefoot and DA and between DA and UD for maximal knee flexion during the loading response (p = 0.001 and p = 0.004, respectively) and maximal ankle dorsiflexion during stance (p = 0.018 and p = 0.026, respectively); however, no significant differences were observed between barefoot and UD. Ankle dorsiflexion during mid-swing also showed significant differences between barefoot and DA, between barefoot and UD, and between DA and UD (p < 0.001, p = 0.003, and p = 0.029, respectively). Significant differences between barefoot and DA and between barefoot and UD were observed for ankle dorsiflexion during terminal swing (both, p < 0.001) and maximal ankle plantar flexion during push-off (both, p < 0.001).
Stratified analysis of participants with ankle dorsiflexor motor grades ≥3
There were no significant differences for the temporospatial parameters according to the Friedman test results. However, these results revealed significant differences between barefoot and DA, and between barefoot and UD for ankle dorsiflexion during mid-swing (p = 0.001), ankle dorsiflexion during terminal swing (p < 0.001), and maximal ankle plantar flexion during push-off (p = 0.001) (Table 3). The post hoc Wilcoxon’s signed-rank test revealed significant differences between barefoot and DA and between barefoot and UD for ankle dorsiflexion during mid-swing (p = 0.015 and p = 0.019, respectively), ankle dorsiflexion during terminal swing (p = 0.004 and p = 0.007, respectively), and maximal ankle plantar flexion during push-off (p = 0.004 and p = 0.002, respectively). No significant differences were observed between DA and UD.
Comparison of spatiotemporal and kinematic data between barefoot, Dyna Ankle, and UD Flex conditions in participants with ankle dorsiflexor motor grade ≥3.

Values are presented as median (interquartile range).
For post hoc tests, the p-values were verified using Bonferroni correction.
B, barefoot; DA, Dyna Ankle; UD, UD Flex. *p < 0.05.
Stratified analysis of participants with ankle dorsiflexor motor grades <3
Temporospatial parameters, specifically cadence and stride time, indicated significant differences according to the Friedman test results (both, p = 0.046) (Table 2). However, the post hoc Wilcoxon signed-rank test results did not indicate significant differences between the conditions.
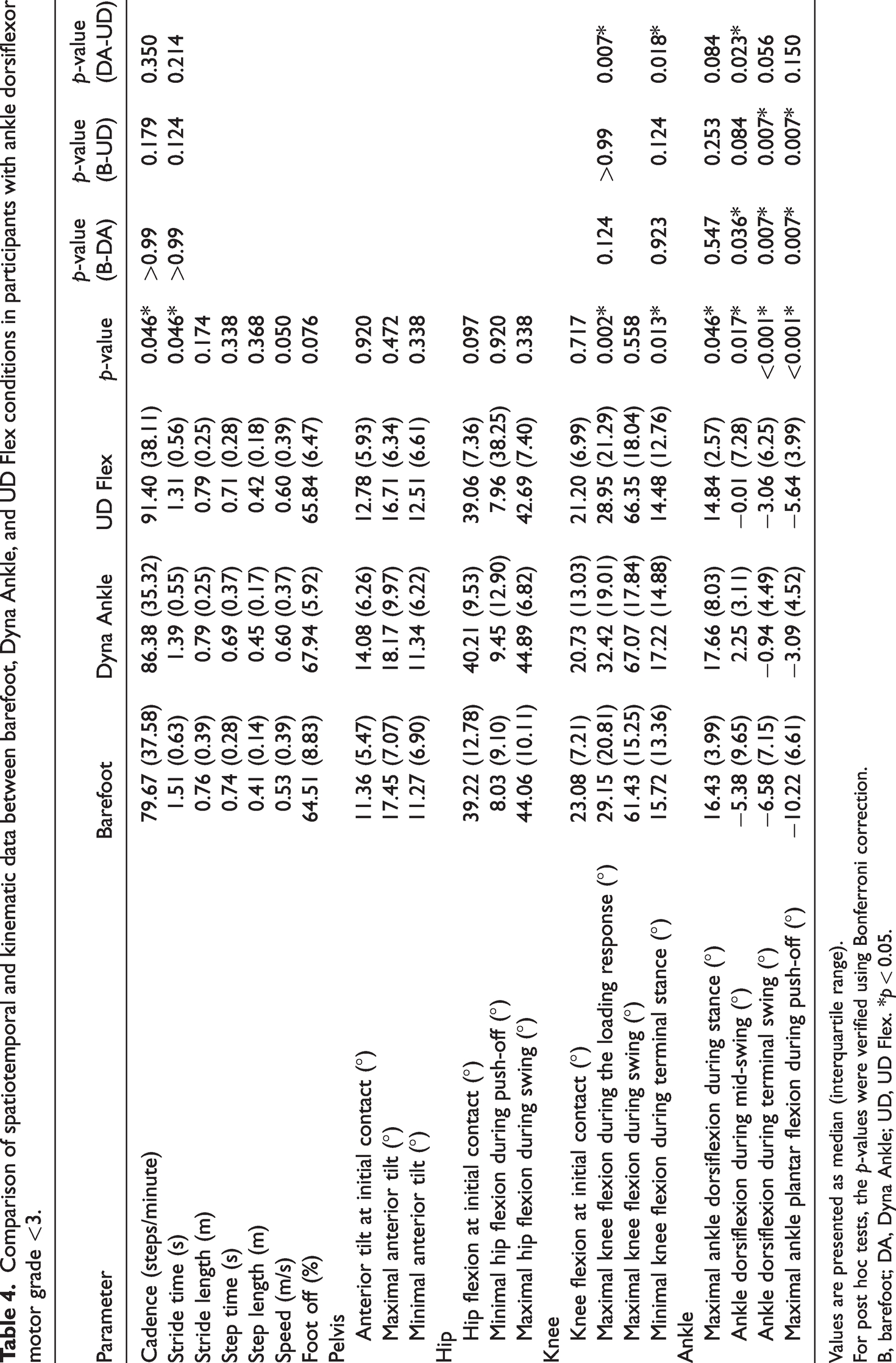
The Friedman test results indicated significant differences between barefoot, DA, and UD in maximal knee flexion during the loading response (p = 0.002), minimal knee flexion during terminal stance (p = 0.013), maximal ankle dorsiflexion during stance (p = 0.046), ankle dorsiflexion during mid-swing (p = 0.017), ankle dorsiflexion during terminal swing (p < 0.001), and maximal ankle plantar flexion during push-off (p < 0.001) (Table 4). The post hoc Wilcoxon signed rank test results revealed significant differences between DA and UD for maximal knee flexion during the loading response (p = 0.007) and minimal knee flexion during terminal stance (p = 0.018), but no significant differences were observed between barefoot and DA or between barefoot and UD. Moreover, no significant differences were observed for maximal ankle dorsiflexion during stance. Although significant differences were observed between barefoot and DA and between DA and UD for ankle dorsiflexion during mid-swing (p = 0.036 and p = 0.023, respectively), no significant differences were observed between barefoot and UD. Similarly, although significant differences were observed between barefoot and DA and between barefoot and UD for ankle dorsiflexion during terminal swing (both, p = 0.007) and maximal ankle plantar flexion during push-off (both, p = 0.007), no significant differences were observed between DA and UD.
Comparison of spatiotemporal and kinematic data between barefoot, Dyna Ankle, and UD Flex conditions in participants with ankle dorsiflexor motor grade <3.
Values are presented as median (interquartile range).
For post hoc tests, the p-values were verified using Bonferroni correction.
B, barefoot; DA, Dyna Ankle; UD, UD Flex. *p < 0.05.
Discussion
This study compared two widely-used AFOs, the DA and the UD, and provided information for the prescription of prefabricated AFOs in patients with hemiplegia. We analyzed temporospatial and kinematic data collected under three different conditions (barefoot, DA, and UD) and revealed significant differences. The DA improved ankle dorsiflexion significantly during the swing phase, making it more effective in correcting foot drop compared with the UD. In comparison, the UD was more effective in preventing knee flexion during the loading response compared with the DA. Stratified analysis on the basis of ankle dorsiflexor motor grade revealed distinct patterns of differences.
Patients with ankle dorsiflexor weakness often have insufficient toe clearance during the swing phase, which is a main cause of falls. 18 Not only do patients with CP and acquired brain injury experience motor weakness disturbance, but most also present with spasticity on the affected side. 19 Hamstring spasticity often leads to knee flexion during weight-bearing, which is associated with jump gait and crouch gait. 20
AFOs can improve the walking ability of patients with hemiplegia by providing a beneficial effect on the kinematics of the knee and ankle. 21 AFOs can also prevent foot drop during early stance, swing, and push-off phases. 21 Furthermore, AFOs aid in facilitating weight-bearing on the affected leg by increasing the excursion of the center of pressure forward over the stance foot, enhancing knee movements during the stance phase. 21 Consequently, AFOs contribute to a reduction in energy expenditure during walking. 21
The DA is a prefabricated AFO with dynamic AFO characteristics, providing greater compliance in the sagittal plane and allowing for some ankle movement. The DA is constructed from polyvinyl chloride material, with a distal footplate thickness of 1.3 mm. The footplate length is situation at the metatarsal head, with an ankle angle set at 90 degrees, and the shank angle to the floor is 0 degrees. The trim line of the DA is located posterior to the malleolus, making the ankle motion relatively free. The DA is made of polypropylene and can be modified slightly with heat, and there are four size options. Prevention of ankle supination during jumping is better when using the DA compared with other tested orthoses and barefoot. 22 Additionally, the DA has the advantage of being safe, comfortable, and easy to handle. 22 Although the DA was designed for ankle sprains or ligament injury, it can also be used by people with ankle motor weakness, especially neurologic weakness of the ankle dorsiflexors and evertors, as this orthosis holds the ankle in moderate pronation and dorsiflexion. There have been attempts to apply dynamic AFOs similar to the DA in patients with hemiparesis, and these attempts have shown immediate improvements in stance and gait parameters. 14
The UD is another type of prefabricated plastic AFO designed to be worn at the front of the foot, with a completely open heel. The UD is constructed from polypropylene material and has a distal footplate thickness of 1.5 mm. The footplate length is situated just behind the metatarsal head, with an ankle angle set at 90 degrees, and the shank angle to the floor is 0 degrees. The UD is indicated for patients with foot drop due to mild foot deformity, stroke, or spinal cord injury. The UD is also used to relieve pain and prevent foot deformation after tendon reconstruction operation. 15 The open heal of the UD has the advantage of allowing users to receive ground reaction feedback, resulting in a more natural way of walking.23,24 Additionally, the UD is ultralightweight, and the weight varies depending on size and ranges from 55 to 115 g. The UD can be placed easily with one hand, which is advantageous for patients with hemiplegia. As the UD provides 5 degrees of ankle dorsiflexion, it can be helpful for ankle motor weakness, especially ankle dorsiflexor weakness. 15 In 2009, Bae et al. showed a significant effect of the UD to assist ankle dorsiflexion during the swing phase compared with the non-UD group. 24
Because both orthoses are designed to provide slight ankle dorsiflexion, they can help improve foot clearance in patients with ankle dorsiflexor weakness. In this study, we aimed to compare the kinematic effects of the DA and UD on the gait cycle of patients with hemiplegia, specifically those diagnosed with CP or acquired brain injury. Previous studies found that, for the post-stroke hemiplegic gait, a posterior AFO is superior to an anterior AFO in improving rear-foot dorsiflexion throughout the entire gait cycle. 25 Furthermore, a posterior AFO increased knee flexion during the stance phase. 26 In our data analysis, we observed no differences in the effects of the DA and UD on pelvis and hip kinematics, or temporospatial parameters. However, knee flexion in the loading response differed between the three conditions in the post hoc test. Bae et al. reported no difference in peak knee flexion in barefoot and UD conditions during the loading response, which was similar to the findings in our study. 24 However, our study revealed a significant difference with the DA compared with the other two conditions; knee flexion increased during the loading response when participants wore the DA. Excessive knee flexion during weight-bearing can lead to abnormal gait patterns, such as jump gait or crouch gait. 20 In the case of the UD, knee flexion did not increase compared with walking barefoot. Therefore, it may be advisable to choose the UD over the DA for patients exhibiting abnormal gait patterns with significant knee flexion during stance, especially during the loading response. During the stance phase, maximal ankle dorsiflexion increased when participants wore the DA compared with walking barefoot. However, compared with walking barefoot, wearing the UD did not lead to any difference in maximal ankle dorsiflexion during the stance phase. This result is also consistent with the results in Bae et al.’s study. 24
During the mid-swing phase, ankle dorsiflexion improved with both orthoses. Bae et al. reported a significant increase in peak ankle dorsiflexion with the UD during the swing phase. 24 However, in our study, ankle dorsiflexion improvement was most pronounced with the DA, indicating that the DA provided the most effective correction for foot clearance. During terminal swing, ankle dorsiflexion increased with the use of both orthoses, with no difference in the extent of increase between them. In summary, the DA provided significantly better dorsiflexion correction during the swing phase. Therefore, for individuals in whom reduced foot clearance is a primary contributor to abnormal gait patterns, choosing the DA over the UD may be preferable.
During push-off, the use of an orthosis significantly restricted ankle plantar flexion compared with walking barefoot. Both the DA and the UD limited ankle plantar flexion during push-off, with no significant difference in ankle plantar flexion between the two orthoses.
The effects of the two orthoses varied by the motor grade of the ankle dorsiflexors. For patients with substantial ankle dorsiflexor strength (grade ≥3), the application of either orthosis had no effect on the pelvis, hip, or knee. Ankle dorsiflexion during mid-swing, ankle dorsiflexion during terminal swing, and maximal ankle plantar flexion during push-off showed significant differences compared with walking barefoot, for both orthoses; however, no difference in effects was found between the two orthoses. Thus, neither the DA nor the UD influence joints other than the ankle, and no differences were found between the orthoses’ effects on the ankle.
For patients lacking ankle dorsiflexor strength (grade <3), using either orthosis influenced the knee and ankle. With respect to knee joint kinematics, differences were observed in knee flexion during the loading response and terminal stance between the two orthoses. Similar to the initial analysis, knee flexion was greater during the loading response when the DA was used compared with the UD. An interesting observation was the significant difference in knee flexion during terminal stance, which was more pronounced with the DA compared with the UD. This suggests that excessive knee flexion is apparent when the DA is used compared with UD. During the swing phase, ankle dorsiflexion was significantly corrected when the DA was used compared with the UD. In contrast, the UD showed some correction in ankle dorsiflexion during terminal swing compared with walking barefoot; however, there was no effect during the mid-swing phase.
When prescribing AFOs, such as the simple prefabricated products, the DA and UD, to correct abnormal gait patterns in patients with hemiplegia, the patient’s characteristics must be considered. In participants with substantial ankle dorsiflexor strength, neither orthosis had any effect on the pelvis, hip, and knee, although an improvement in foot drop was observed with both orthoses. However, no difference between the two orthoses was found; thus, either orthosis can be selected in these patients. When there is a lack of ankle dorsiflexor strength, both orthoses had an impact on both the knee and ankle. As a result, a decision must be made with respect to which aspect requires focus during the stance phase (excessive knee flexion) and swing phase (foot clearance). If the primary goal is to correct foot clearance, the DA may be preferable, while, if excessive knee flexion is the concern, the UD may be preferable.
This study has several limitations. First, this was a retrospective study. Second, only 29 individuals participated in the study, and the diagnoses were heterogeneous. Therefore, further studies with large sample sizes are necessary. Third, spasticity of the lower extremity can influence gait kinematics; however, although we performed a subgroup analysis on the basis of spasticity, we did not verify the spasticity of each patient. In addition to spasticity, numerous factors can influence gait patterns, such as proprioception, skeletal deformity, body weight, and social factors. Therefore, we must consider potential confounding factors in a future study. Fourth, we performed a gait analysis barefoot to evaluate indoor activity, and barefoot assessments may be difficult to apply to outdoor activities. Fifth, fatigue after brain injury, which can be associated with poor functional outcome and mobility, was not assessed in this study. Finally, because this study involved highly functional patients with an FIM locomotion score of 13.0 (10.0, 14.0), it is difficult to generalize our findings to all patients with hemiplegia. In our future prospective study, a subgroup analysis using multiple factors, such as spasticity and gait analysis while wearing shoes, will be performed with a larger sample size than that in the current study. Additionally, we plan more precise evaluation through gait analysis using statistical parametric mapping.
Conclusions
The DA and UD have different effects in patients with hemiplegia. The DA improves ankle dorsiflexion during the swing phase much more compared with the UD, in patients with hemiplegia. However, the UD induces less knee flexion compared with the DA during the loading response. No significant difference was found between the two orthoses for pelvic and hip kinematics during the overall gait cycle. In the stratified analysis, both orthoses exhibited similar effects in patients with substantial ankle dorsiflexor strength. In patients with a lack of ankle dorsiflexor strength, both orthoses had distinct effects on the knee and ankle. Therefore, it may be advisable to prescribe orthoses by considering a patient’s clinical characteristics, such as ankle dorsiflexor strength, as well as gait abnormalities, such as excessive knee flexion during the stance phase and foot drop, in patients with hemiplegia. This study provides unique information on the prescription of prefabricated AFOs.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241233514 - Supplemental material for Comparison between prefabricated ankle–foot orthoses, Dyna Ankle and UD Flex, in patients with hemiplegia
Supplemental material, sj-pdf-1-imr-10.1177_03000605241233514 for Comparison between prefabricated ankle–foot orthoses, Dyna Ankle and UD Flex, in patients with hemiplegia by Su Ji Lee, Tae Yong Kim, Kyung Min Kim and Sung-Rae Cho in Journal of International Medical Research
Footnotes
Acknowledgement
The authors thank Medical Illustration & Design (MID), which is part of the Medical Research Support Services of Yonsei University College of Medicine, for providing excellent support with the medical illustrations.
Author contributions
The paper was co-authored by SJL, TYK, KMK and SRC. SRC contributed as the corresponding author. SJL, TYK, and KMK contributed equally to data analysis and interpretation. All authors participated in writing and editing the manuscript.
Data availability statement
The datasets used and/or analyzed in this study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Korean Fund for Regenerative Medicine (KFRM) [grant numbers 21C0715L1, 21A0202L1), funded by the Ministry of Science and ICT and the Ministry of Health & Welfare, Republic of Korea; and the Korean Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea [grant number H122C1588].
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.