
Abstract
Background:
Recently, additive fabrication has been proposed as a feasible engineering method for manufacturing of customized ankle foot orthoses (AFOs). Consequently, studies on safety, comfort and effectiveness are now carried out to assess the performance of such devices.
Objective:
Evaluate the clinical performance of customized (selective laser sintering) SLS-AFOs on eight subjects with unilateral drop foot gait and compare to clinically accepted (polypropylene) PP-AFOs.
Study Design:
Active control trial.
Methods:
For each subject two customized AFOs were fabricated: one SLS-AFO manufactured following an additive fabrication framework and one thermoplastic PP-AFO manufactured according to the traditional handcraft method. Clinical performance of both AFOs was evaluated during gait analysis.
Results:
A significant beneficial effect of both custom-moulded PP-AFO and customized SLS-AFO in terms of spatial temporal gait parameters and ankle kinematic parameters compared to barefoot gait of adults with drop foot gait are observed. No statistically significant difference between the effect of PP-AFO and of SLS-AFO was found in terms of spatial temporal gait parameters and ankle kinematic parameters.
Conclusion:
AFOs manufactured through the SLS technique show performances that are at least equivalent to the handcrafted PP-AFOs commonly prescribed in current clinical practice.
Clinical relevance
Manufacturing personalized AFOs with selective laser sintering (SLS) in an automated production process results in decreased production time and guarantees the consistency of shape and functional characteristics over different production time points compared to the traditional manufacturing process. Moreover, it reduces the dependency of the appliance on the experience and craftsmanship of the orthopaedic technician.
Background
Excessive plantar flexion due to anterior muscle insufficiency (passive drop foot) introduces significant functional deviations during gait resulting in shortened step and stride length and reduced gait velocity. 1 Prefabricated thermoplastic (polypropylene-PP, polyethylene-PE) AFOs have been widely used to manage weakness and spasticity about the ankle joint for the last three to four decades2,3 while proving their mechanical performance due to high material strength and high fatigue resistance. 4 Previous studies reported that wearing an AFO significantly changes the ankle kinematics5-7 and results in positive effects on walking velocity,8-10 stride length8-10 and cadence.8,10 Improved clinical performance, comfort and fit were achieved by manufacturing custom-fit or custom-moulded orthoses adapted to the subject needs. 11 However, the traditional manufacturing process of personalized AFOs is time consuming, relies on impression casting and is highly dependent on the experience and craftsmanship of the certified prosthetist and orthotist (CPO). 12 Additional cutting, supplementary local pressure reliefs and finishing operations may be required to fine-tune the AFO while fitting to the subject. Moreover, the characteristics of traditionally manufactured plastic orthoses are affected by parameters of the fabrication techniques (e.g. heating temperature, manual holding) which decrease the consistency over different production stages due to the amount of manual work required. 12 In consequence, undesired manufacturing variability in the quality and/or effectiveness of hand-made orthoses is introduced. 12
Additive fabrication (selective laser sintering (SLS), in particular) has been recently proposed as a feasible engineering method for manufacturing of customized prosthetic feet, prosthetic sockets, customized foot orthoses and customized ankle-foot orthoses.13-16 This technique allowed developing different manufacturing frameworks to replicate the shape and functional characteristics of existing carbon-fibre AFO or to customize shape and functional AFO characteristics under a certain degree of automation.17-18
Although the feasibility of the SLS manufacturing techniques for prosthetics and orthotics was demonstrated, studies on the safety, comfort and effectiveness of SLS orthotics are only nowadays being considered. Pallari et al. concluded that clinical performance of SLS foot orthoses manufactured for rheumatoid arthritis subjects was similar to subjects’ current prescribed customized devices in terms of the observed gait and subjective evaluation of fit and comfort. 15 Two rapid prototyped AFOs (manufactured through stereolitography technique) performed comparable to prefabricated polypropylene orthoses in a preliminary study involving one healthy subject. 19
The objective of this study was to evaluate the clinical performance of customized SLS-AFOs on eight subjects with unilateral drop foot gait. For each subject, two customized AFOs were fabricated: one SLS-AFO manufactured following an additive fabrication framework described later in this article and one thermoplastic PP-AFO manufactured according to the traditional handcrafting method. 20 Clinical performance of both AFOs was evaluated through gait analysis. The aim of this study was to compare the clinical performance of an SLS-AFO with the clinical performance of a PP-AFO in terms of spatial-temporal and kinematic gait parameters.
Methods
Participants
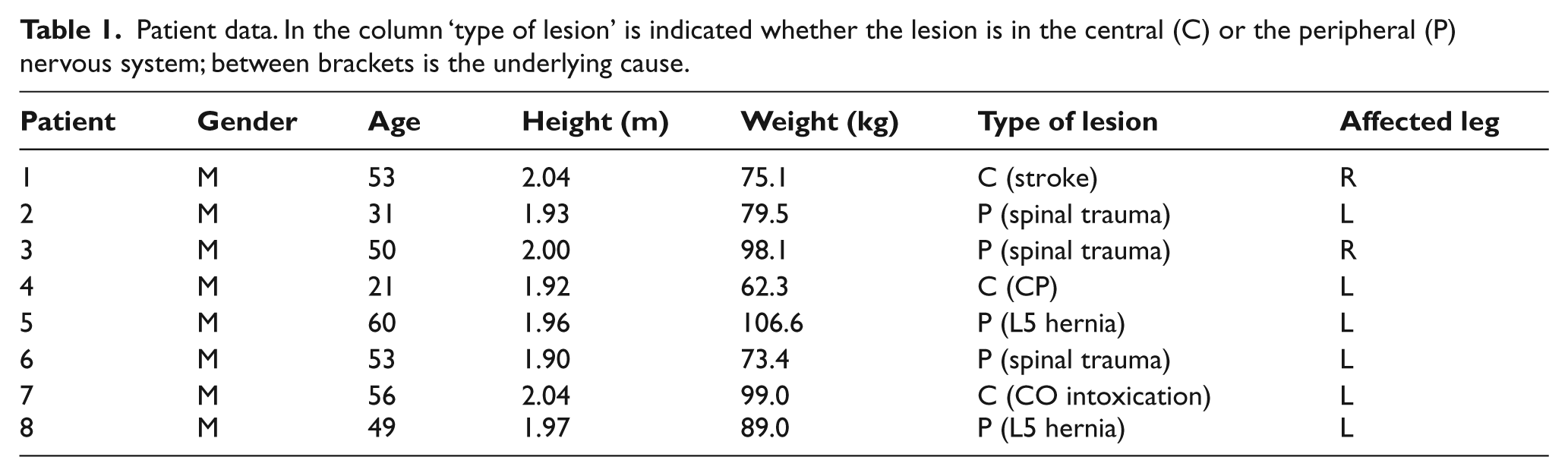
Inclusion and exclusion criteria were formulated prior to subject selection. Eight subjects with unilateral drop foot due to dorsiflexor weakness were considered for this study (age 46.6 years (standard deviation (SD) 12.5), height 1.97 m (SD 0.49) and bodyweight 85.3 kg (SD 14.2)). All subjects have been walking daily with an AFO for a period longer than 2 years. Subjects who could not walk independently (without walking aids) over 500 m and subjects with cognitive problems were not considered for the study. Following clinical evaluation, all subjects were classified in the first or second stage on the Ashworth scale 21 and therefore required moderate ankle stability. Underlying conditions leading to drop foot were stroke, cerebral palsy, L5 hernia, CO intoxication and mechanical trauma. However, gait deficiency was only due to anterior muscles weakness. Patient details are depicted in Table 1. The experimental protocol was approved by the ethical committee (B32220096061) and written informed consent was obtained from each subject prior to participation.
Patient data. In the column ‘type of lesion’ is indicated whether the lesion is in the central (C) or the peripheral (P) nervous system; between brackets is the underlying cause.
Design and manufacturing of AFOs
For each subject a custom made PP-AFO was designed and manufactured by a CPO following the traditional handcraft method: manual plaster cast and positive rectification followed by thermoforming (V!GO, Belgium). 20
The SLS AFOs were designed using the same design principles as the PP-AFOs. The complete workflow is presented in Figure 1. Initially, the cast of the subject’s leg was scanned using the Polhemus Cobra optical scanner (Polhemus, Vermont, USA), and the resulting 3D-file was imported in the STL file format into the three-matic software by Materialise NV, Leuven, Belgium. This was considered the positive on which anatomical landmarks were indicated. Further, this file was aligned and merged with a template with the same landmarks indicated. The template was a scanned foot positive in an ideally corrected position. Templates were provided by V!GO for a large range of foot sizes. The purpose of the templates is to save time in making corrections to the positive, e.g. filling gaps that might be in the plantar surface of the AFO cast, due to scanning.
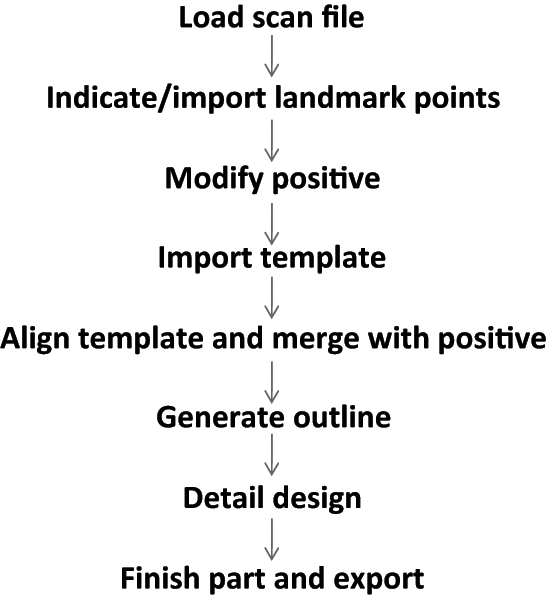
The workflow used in the computer-aided design (CAD) of the AFOs.
Once the first design of the SLS AFO was complete, it was subjected to the CPO’s assessment. Any corrections to this initial design were implemented and the revised design was subjected for another review by the CPO. This insured similar designs for both AFO types. Once this iterative process was finished, the AFO was manufactured with the SLS technique. The material used in the production was Nylon-12 with the trade name PA 2201 from EOS GmbH, Munich, Germany. The SLS machine used was a P760, also from EOS GmbH and was operated by Materialise NV in Leuven, Belgium. Once the AFO build was completed by the SLS machine, the AFOs were removed from the build, cleaned up with pressurized air, painted and coated with a Soft Touch coating and delivered to V!GO for further finishing and fitting to the subjects by the same CPO. Both PP- and SLS-AFOs for one subject are showed in Figure 2.

PP-AFO (left) and SLS-AFO (right) of one subject participating in the study.
Data collection
Gait measurements were performed at a clinical gait lab in three conditions: barefoot and while wearing the custom made PP-AFO and the custom made SLS Nylon-12 AFO. Both AFOs were provided to the subject on the day of testing, and were aligned during fitting by the same CPO. Subjects were allowed to adapt to wearing the AFOs for at least half an hour before data collection. In all cases, subjects were asked to walk at a comfortable self-selected speed along a 21.5-m instrumented Tartan track. Kinematic data were collected using the CODAMOTION system (Charnwood Dynamics Ltd, UK) with four CX1 cameras and active markers, measuring at 200 Hz. Active markers were attached on both unaffected and affected limb using a specialized wand system provided by Charnwood Dynamics Ltd. 22 For each walking condition, eight repeatable measurements which contained the full gait cycle of each limb were performed. 22 Each measurement was recorded and further used for statistical analysis.
Outcome measures and statistics
Spatial and temporal gait parameters (stride duration, stride length and stance phase duration of both the affected and unaffected limb) were calculated for each subject and each walking condition. Kinematic variables of the affected limb were calculated for each treatment condition: ankle, knee and hip angles at initial foot-floor contact; the maximum plantar flexion of the ankle and maximum knee and hip flexion angles during swing phase; ankle, knee and hip range of motion during full gait cycle.
Statistical Package for the Social Sciences (SPSS 20.0 for Windows) was used for statistical evaluation. A repeated measures analysis-of-variance was performed to determine if there were significant differences in the parameters between different walking conditions (barefoot, PP-AFO and SLS-AFO). The least-significant-difference test was performed as a post-hoc test to determine where these differences are located. Statistical significance was set at p < 0.05.
Results
Spatial and temporal gait parameters
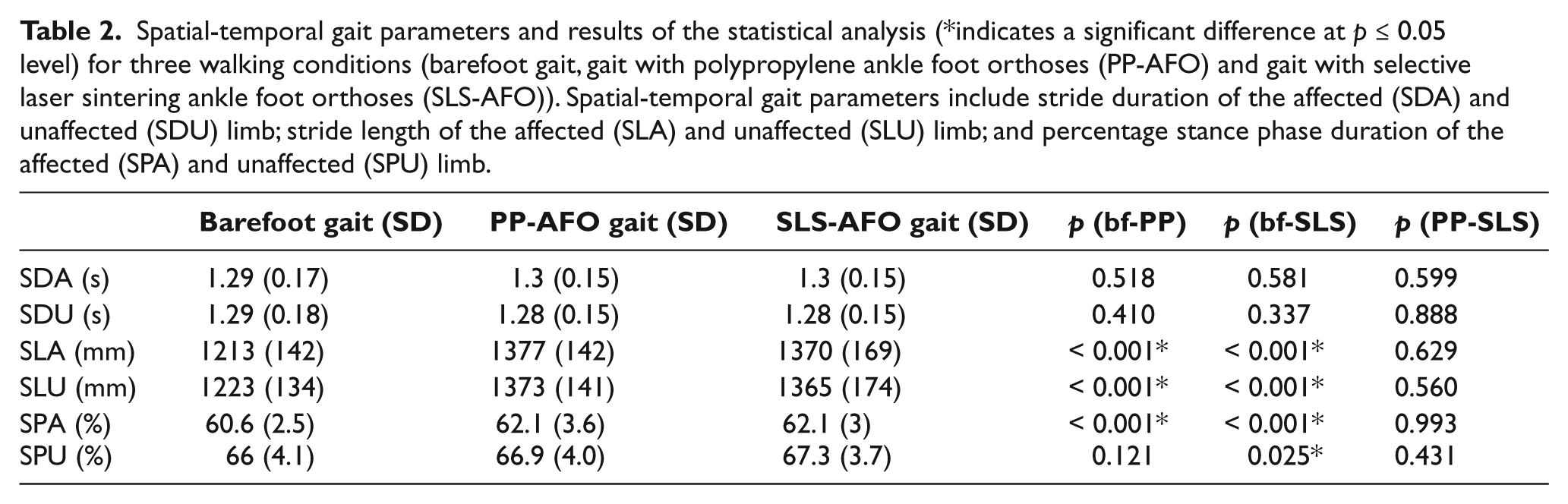
Spatial-temporal gait parameters for the three walking conditions (barefoot gait, gait with PP-AFO and gait with SLS-AFO for both affected and unaffected limb) and the results of the statistical analysis are presented in Table 2. The analysis of variance showed no significant difference in stride duration of the affected (SDA) and unaffected (SDU) limb during AFO gait when compared to barefoot walking. However, a significant increase in stride length of the affected limb (SLA) was observed while wearing both AFO-types when compared to barefoot walking: p < 0.001 when wearing a PP-AFO and p < 0.001 when wearing SLS-AFO. No significant difference in stride length of the affected limb was found between the two AFO-types (p = 0.629). Similar observations were made for the stride length of the unaffected limb (SLU). Stride length is significantly increased when comparing AFO gait to barefoot gait p < 0.001 for both PP-AFO and SLS-AFO). No significant difference in stride length of the unaffected limb was observed between the two AFO types (p = 0.560).
Spatial-temporal gait parameters and results of the statistical analysis (*indicates a significant difference at p ≤ 0.05 level) for three walking conditions (barefoot gait, gait with polypropylene ankle foot orthoses (PP-AFO) and gait with selective laser sintering ankle foot orthoses (SLS-AFO)). Spatial-temporal gait parameters include stride duration of the affected (SDA) and unaffected (SDU) limb; stride length of the affected (SLA) and unaffected (SLU) limb; and percentage stance phase duration of the affected (SPA) and unaffected (SPU) limb.
The percentage stance phase duration of the affected limb increased significantly from barefoot gait to both PP-AFO gait and SLS-AFO gait (p = 0.004). No statistically significant difference was observed between percentage stance phase duration of the affected limb for gait with the two AFO types (p = 0.993).
For the unaffected limb, the percentage stance phase duration of the gait cycle did not change significantly from barefoot gait to PP-AFO gait (p = 0.121), from barefoot gait to SLS-AFO gait there was a significant difference (p = 0.025). No statistically significant difference was found between PP-AFO gait and SLS-AFO gait (p = 0.431).
Kinematic parameters
The model used to define the kinematic gait parameters is shown in Figure 3. Positive values are given to hip flexion, knee flexion and ankle dorsiflexion. Kinematic gait parameters and results of the statistical analysis are presented in Table 3. The analysis of variance showed significant differences of ankle kinematic parameters of the affected limb between barefoot gait and PP-AFO gait and between barefoot gait and SLS-AFO gait. Ankle plantar-flexion of the affected limb at initial foot-floor contact was significantly decreased from barefoot gait to PP-AFO gait (p < 0.001) and to SLS-AFO gait (p < 0.001). No significant difference was observed between PP-AFO gait and SLS-AFO gait (p = 0.608) with respect of ankle plantar-flexion at initial foot-floor contact.
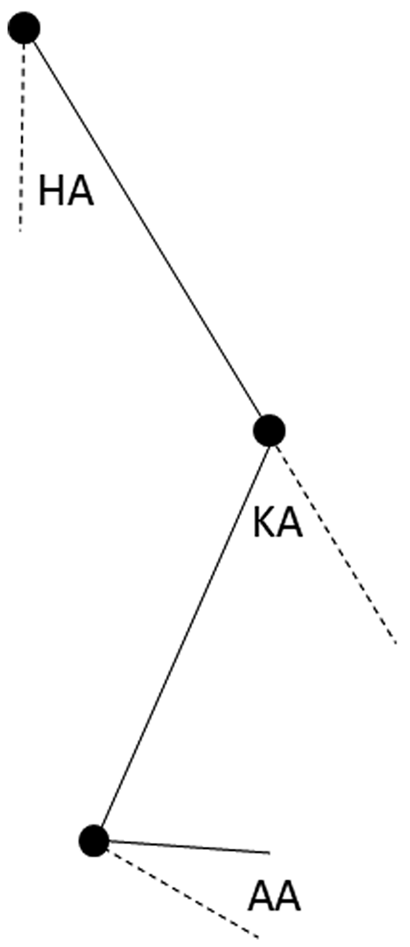
Sagittal model of a lower limb showing hip angle (HA), knee angle (KA) and ankle angle (AA). Positive values are hip flexion, knee flexion and ankle dorsiflexion.
Kinematic gait parameters of the affected limb and results of the statistical analysis (*indicates a significant difference at p ≤ 0.05 level) for three walking conditions (barefoot gait, gait with polypropylene ankle foot orthoses (PP-AFO) and gait with selective laser sintering ankle foot orthoses (SLS-AFO)). Kinematic gait parameters include ankle angle at initial foot-floor-contact (AAIC); maximum plantar flexion angle of the ankle during swing phase (AAMS); ankle range-of motion (AAR); knee angle at initial foot-floor-contact (KAIC); maximum flexion of the knee during swing phase (KAMS); knee range-of motion (KAR); hip angle at initial foot-floor-contact (HAIC); maximum flexion of the hip during swing phase (HAMS) and the hip range-of motion (HAR).
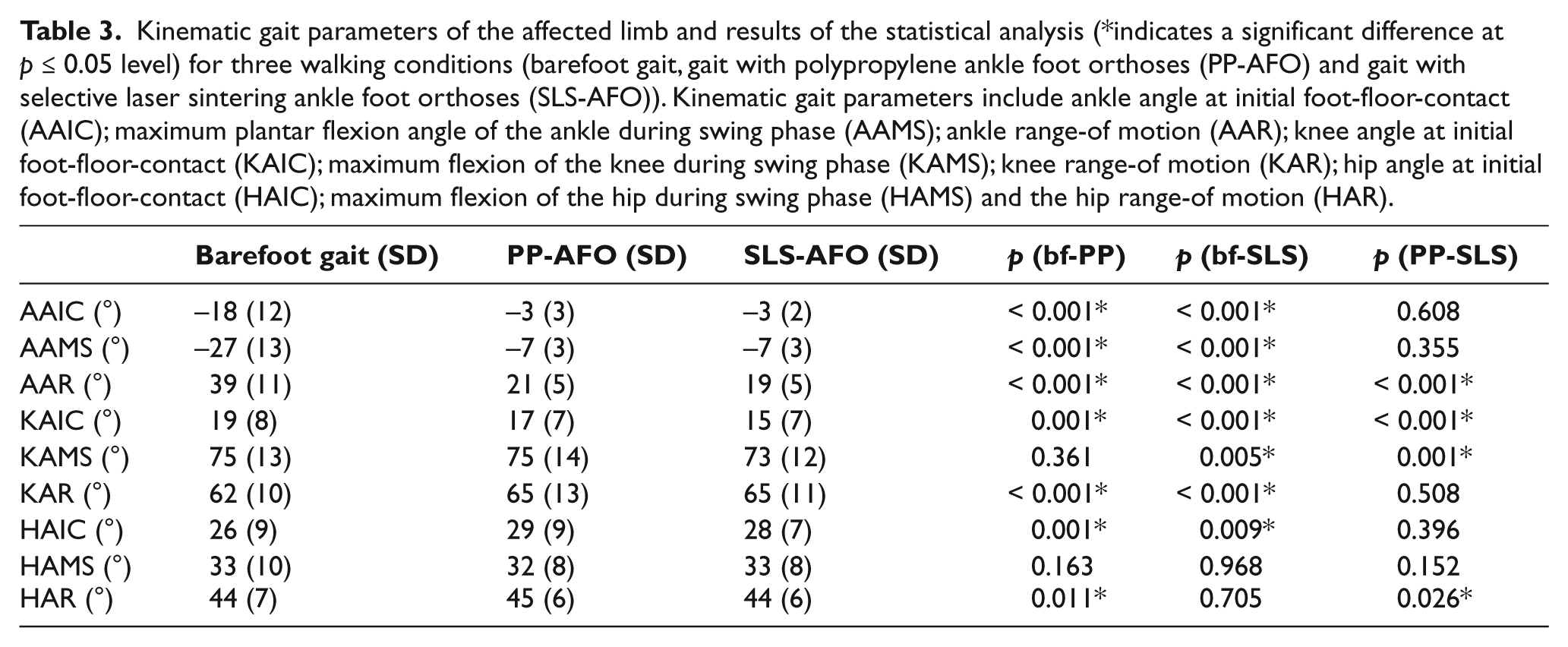
Maximum ankle plantar flexion during swing phase was significantly decreased from barefoot gait to PP-AFO gait (p < 0.001) and SLS-AFO gait (p < 0.001). No significant difference was found between PP-AFO gait and SLS-AFO gait (p = 0.355) with respect to maximum plantar flexion.
The range of motion in the ankle decreased significantly from barefoot gait to PP-AFO gait (p < 0.001) and from barefoot gait to SLS-AFO gait (p < 0.001). Different from previous parameters, a significant difference was observed between ankle range of motion during gait with the two AFO types (p < 0.001). Overall, the SLS-AFO showed a smaller range of motion.
The same parameters were investigated in knee and hip joint. Significant reduced knee flexion at foot-floor contact with a more pronounced effect of SLS-AFO gait was observed (p < 0.001); while at foot-floor contact there was an increase in hip flexion for both PP-AFO (p = 0.001) and SLS-AFO (p = 0.009) gait. At foot-floor contact, no significant difference in hip flexion between PP-AFO and SLS-AFO gait was observed (p = 0.396). During swing a significant decrease in knee flexion was observed for SLS-AFO compared to both barefoot (p = 0.005) as PP-AFO (p = 0.001) gait.
Discussion
Solid AFOs are prescribed in the treatment of multiple gait disorders. In this study subjects with passive drop foot were selected. The main functions of the orthoses are to limit excessive plantar flexion during swing to obtain sufficient toe clearance, to effectively position the foot for initial contact and to provide maximum external stability for the ankle-foot complex in all three planes of motion. 11
In this study, the clinical performance of such orthoses with a posterior shell design (leaf spring type) manufactured through SLS technique was assessed in terms of temporal-spatial and kinematic gait parameters. It was then compared to the clinical performance of the PP-AFOs.
In terms of mobility gait parameters, excessive ankle plantar flexion leads to shortened step and stride length and reduced gait velocity due to obstructed limb advancement in swing and loss of progression in stance. 1 Previous studies reported a positive effect on walking velocity,8-10 stride length8-10 and cadence8,10 in selected hemiplegic adults of a large variety of (plastic and metal) AFO types. In this study, the average stride length of the affected limb significantly increased by 13.5% (0.16 m) and by 12.9% (0.16 m) when PP-AFO and respectively SLS-AFO were used, approaching average male stride length of 1.46 m. 1 However, the duration of one gait cycle was not significantly affected by AFOs, only the stride length increased. Together with cadence, stride length has a determinant effect on gait velocity which increases with the increase of one of them in a linear and individual consistent manner. 1 Based on this rationale it can be assumed that gait velocity increased for both AFO types. The barefoot condition showed longer stance phase duration on the unaffected limb than on the affected limb; this indicates an extended weight transfer to the unaffected side to compensate for the weakness of the affected side. The application of an AFO provides external support for effective single-limb stance so that the support limb can respond with sufficient stability to the forces that act on the body. 11 In this study the mean stance time of the affected limb during barefoot walking was 60.6% of the gait cycle while with PP-AFO and SLS-AFO mean stance time increased to 62.1%.
Excessive ankle plantar flexion due to anterior muscle insufficiency (passive drop foot) introduces significant functional deviations in two of the gait tasks: (i) weight acceptance when the heel rocker is lost due to forefoot initial contact followed by passive drop foot to initiate flat foot contact and (ii) limb advancement during mid-swing when the foot is not lifted sufficiently so that toe clearance cannot be achieved. 1 These gait errors in the ankle are further reflected in the knee and hip. The lack of heel rocker results in excessive knee flexion at initial foot-floor contact and persistent knee extension during mid-stance on the affected limb while the lack of adequate ankle plantar flexion during swing induces increased hip flexion to lift the lower limb. Other compensation mechanisms to achieve toe clearance include circumduction, lateral trunk lean and contralateral vaulting. 1 Enhanced clearance can be achieved by ambulation with an AFO of appropriate design and strength: excessive plantar flexion during swing phase is limited while the ankle angle at initial contact is reduced from plantar flexion to neutral.
Previous studies have reported significant ankle plantar flexion limitation at heel strike and mid-swing with solid prefabricated plastic AFO or with Air Stirrup braces. 5 In gait of adult subjects with increased plantar flexors spasticity, walking with a Valens caliper increased ankle dorsiflexion during stance. 6 Subjects walking with a Chignon dynamic AFO made from moulded carbon fibre achieved dorsiflexion of ankle position at heel strike and in the middle of swing phase. 7 Similarly, present work revealed a significant beneficial effect of both PP-AFO and SLS-AFO on sagittal plane ankle kinematics. The ankle plantar flexion was significantly limited during initial contact and swing phases with no significant differences between the two AFO types studied. However, a significant difference of the effect of PP-AFO and SLS-AFO on ankle angle range was observed with a higher limitation of ankle excursion using the SLS-AFO. These effects are in agreement with past literature regarding ankle plantarflexion5-7 and are mainly attributable to the mechanical properties of the orthoses. Nevertheless, different materials provide different degrees of flexibility with the Nylon-12 used in the SLS system being stiffer than PP. 23 Although both materials and manufacturing methods provide sufficient mechanical resistance to plantar flexion, adding ankle moments to the gait protocol would have provided more information on the different degrees of flexibility of the different AFOs. 3 Furthermore, measuring the ankle power would give further information on the energy-storing capabilities of the different materials. 24
Burdet and colleagues observed decreased hip flexion at initial foot-floor contact when comparing the barefoot gait of hemiparetic adults to barefoot gait of healthy adults. 5 In the present study, for both AFO conditions increased hip flexion at initial foot-floor contact was observed. Furthermore, wearing an AFO resulted in decreased knee flexion at initial foot-floor contact for both AFO conditions. Lehman observed less knee flexion and less dorsiflexion for affected limbs of hemiparetic persons during swing phase, necessitating hip circumduction to achieve toe clearance. 25 While walking with the PP-AFO resulted in increased hip flexion during swing phase, walking with the SLS-AFO resulted in decreased knee flexion during swing phase. As stated previously, different materials provide different degrees of flexibility, resulting in different kinematic compensations during walking. The lack of significant effect for hip flexion during swing can be likely due to the big variety of patients, with each individual using a different compensation mechanism to achieve toe clearance while walking barefoot.
This study has some limitations. Firstly, the study has a limited number of subjects. Although statistical results are presented, extended clinical studies on a larger number of patients are needed before drawing a general conclusion and implementing these types of devices into clinical practice. However, to the authors’ knowledge, this is the first study to assess the function of AFOs produced through additive fabrication on a well-defined neuromuscular dysfunction. Previous trials evaluated the effect of rapid prototyped AFOs on healthy gait. 19 Secondly, both AFOs were provided to the subject only on the day of testing. Longer accommodation periods should be considered to assure that adaptation mechanisms remain constant during gait measurements. Thirdly, the effect of the AFO is evaluated at the fitting moment. A longer follow-up study using SLS orthoses during the activities of daily living (ADL) is advisable to assess long-term subject acceptance with respect to subject comfort and safety.
AFOs manufactured by SLS technique show clinical performances that are at least equivalent to the handcrafted PP AFOs commonly prescribed in current clinical practice. Considering the automated manufacturing process, the use of additive manufacturing techniques gives the opportunity to make the AFO production process faster, more controlled and reproducible. Average delivery time observed during this project for an SLS-AFO was three days while the average delivery time for a custom made PP-AFO was 10 days. Furthermore, since the SLS-AFO is printed from a computer-aided design, an identical reproduction of a given orthosis can be made. In literature, there is evidence to support the use of additive manufacturing for producing orthotic or prosthetic devices.13-19 However, issues related to material properties and manufacturing costs still need to be investigated before additive technologies could be considered ready for clinical use. Furthermore, it is not clear to the authors how much evidence is necessary before one can consider these manufacturing technologies ‘ready for commercial’ use. Different countries have different healthcare systems and mechanisms to bring new technology within various reimbursement systems. Not knowing which specification or standard to fulfil remains a further obstacle to clinical implementation.
Conclusion
Although recent studies have discussed the feasibility of using additive fabrication techniques to manufacture AFOs, clinical performance of these devices was not properly evaluated.17-19 The present study is the first one to (i) assess the effectiveness of SLS-AFO on drop foot gait and (ii) compare SLS-AFOs’ clinical performance to clinical performance achieved using custom-moulded PP-AFOs.
Results presented in this study indicate a significant beneficial effect of both custom-moulded PP-AFO and customized SLS-AFO in terms of spatial temporal gait parameters and ankle kinematic parameters compared to the barefoot gait of adults with drop foot gait. Furthermore, the clinical effectiveness of customized SLS-AFO is demonstrated as no statistically significant difference between the effect of PP-AFO and of SLS-AFO was found in terms of spatial temporal gait parameters and ankle kinematic parameters. It can be concluded that AFOs manufactured by SLS technique show clinical performances that are at least equivalent to the handcrafted PP-AFOs commonly prescribed in current clinical practice. Moreover, the automated production-process of SLS-AFOs results in decreased delivery time and guarantees the consistency of shape and functional characteristics over different production stages compared to the traditional manufacturing process.
Footnotes
Acknowledgements
We thank Jan Jonckers and René Willemsen of V!GO Belgium for their participation in the fabrication of the AFOs and all the test subjects for participating in the study.
Conflict of interest
None declared.
Funding
This work was funded by IWT – Flanders, [project n° 080406].