
Abstract
Background:
Foot pain decreases individuals’ ability to perform daily activities. Insoles are often prescribed to reduce the pain which, in turn, may promote return to normal activities.
Objectives:
To evaluate the effects of insoles on foot pain and daily activities, and to investigate the relationship between individuals’ satisfaction with insoles and actual use of them.
Study design:
A 4-week pre–post intervention follow-up.
Methods:
Brief Pain Inventory, International Physical Activity Questionnaire and Lower Extremities Functional Status were used as outcome measures. Client Satisfaction with Device was used in the follow-up.
Results:
A total of 67 participants answered the questionnaires (81% women). Overall, a reduction in Pain Severity (p = 0.002) and Pain Interference (p = 0.008) was shown. Secondary analyses revealed a significant effect only in women. No changes in daily activities (Walking, p = 0.867; Total Physical Activity, p = 0.842; Lower Extremities Functional Status, p = 0.939) could be seen. There was no relation between Client Satisfaction with Device measures and duration of insole use. A difference in sex was shown; women scored higher than men on Pain Severity.
Conclusion:
Insoles reduce pain and pain interference with daily activities for women with foot pain. Satisfaction with the insoles is not a predictor of actual insole use. The effect of insoles on activity performance needs further study.
Clinical relevance
This study provides evidence for prescribing insoles to people with foot pain. Nonetheless, insoles are not enough to increase their physical activity level in the short term. Satisfaction with insoles and duration of use are not correlated and cannot be inferred from each other.
Background
Pain in weight-bearing joints limits individuals’ physical functioning and ability to perform daily activities.1,2 This pain is often the outcome of structural deformities such as flat foot, or cavus foot. In workers with structural deformities of the foot and whose occupations include standing or walking for a long time, pain reduction is an important goal. 3 In particular, a reduction in walking is typically the major effect of foot pain on physical activity (PA).4,5 In order to reduce the pain, insoles are often prescribed. An important question is how effective the insoles are for reducing foot pain and, as a consequence, for increasing daily activities.
Insoles have a direct mechanical effect on the foot during weight-bearing, by supporting it and keeping it in alignment, thus distributing pressure over the entire plantar surface. 6 The insoles can also have indirect effects on more proximal joints in the body, such as in the knees and the back. One of the most common reasons for prescribing insoles is to enhance functioning by reducing non-specific pain in the foot, leg or lower back. Reduction of pain has been shown to improve performance of daily activities such as work and recreational activities.7,8 Many studies have focused on the biomechanical and physiological responses to insoles in patients with low back pain, 9 rheumatoid arthritis 10 or osteoarthritis. 11 In another study, the effect of insoles on non-specific foot pain and work satisfaction was investigated. 12 Although there seems to be an inverse relation between pain and daily activities, the effect of insoles on pain and daily activities is not clear. Specifically, there is a gap between the clear-cut diagnoses in scientific studies and the often unspecific pain of unknown origin met by professionals in clinical practice. Therefore, there is a need to investigate if the clinical practice to prescribe insoles to people with unspecific foot pain is supported by scientific evidence.
It can be hypothesized that the use of the insoles is related to what the user thinks about various aspects of the insoles, including their comfort and appearance. 13 However, only one study reports on this topic, 14 and there are no studies covering the specific relationship between satisfaction and actual use. Thus, the aims of this study were to evaluate the effects of insoles on foot pain and daily activity, and to investigate the relation between satisfaction with the insoles and actual use in individuals with foot pain.
Methods
The fitting of insoles is an established intervention for people with foot pain and, although no strong scientific evidence exists, there is clinical evidence for the effect. In order not to prolong the pain for the clients by allocating some of them to a control group, an uncontrolled pre–post intervention survey design was chosen. The data were collected on two occasions: when the participants came to the clinic before first-time fitting of insoles – or, in the case of previous users, before refitting of insoles – and again after 4 weeks of use.
Participants and procedure
The participants were patients referred to the Department of Prosthetics and Orthotics at Örebro University Hospital, Örebro, Sweden. Data were collected prospectively between 30 August 2010 and 31 January 2011. The inclusion criteria were as follows: (1) foot pain, (2) aged 18 years or older and (3) able to speak Swedish. Exclusion criteria were as follows: (1) pain due to a systemic disease, (2) use of orthosis other than insoles or (3) earlier surgery in lower extremities. During the data collection period, 75 individuals completed the first survey. At the follow-up, 8 patients failed to return the questionnaires. Hence, 67 participants (81% women) with foot pain were included in this study (Table 1). Out of these, after 4 weeks of insoles use, 22 participants had been using analgesic and/or anti-inflammatory medications (e.g. paracetamol and diclofenac) to relieve pain, 1 physiotherapy intervention, 1 reported no such medication use and 43 answers were missing.
Participants’ demographic data.
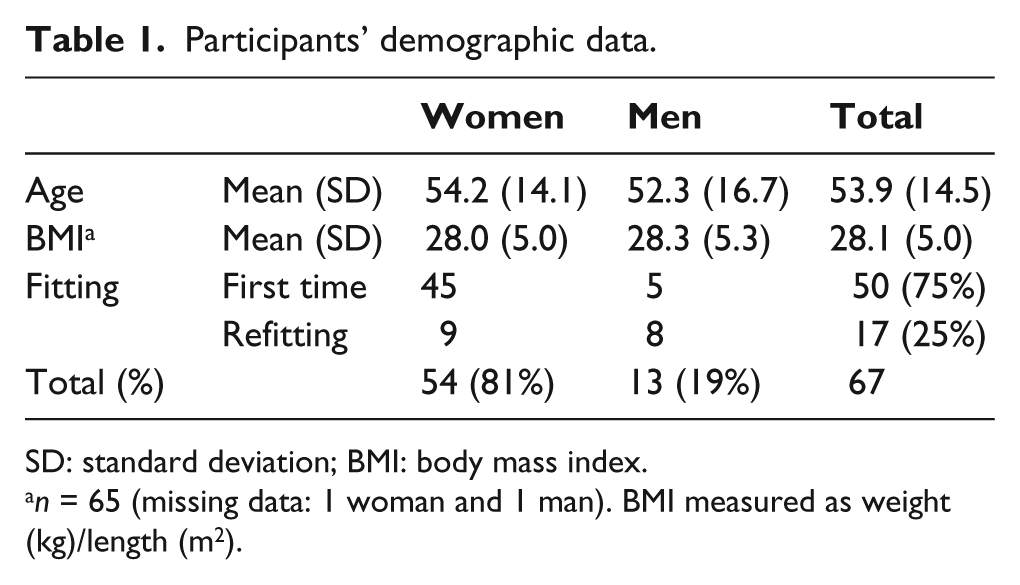
SD: standard deviation; BMI: body mass index.
n = 65 (missing data: 1 woman and 1 man). BMI measured as weight (kg)/length (m2).
At the time of the clinic appointment, according to the normal procedure, the prosthetist–orthotist examined the patients’ clinical status, chose a type of insoles, accommodated the insoles to the patient’s shoes and checked the comfort and fit before the patient left the clinic. A total of 36 participants were prescribed custom-made insoles (27 from casting, 9 from footprint) made of ethylene vinyl acetate (EVA). A total of 30 participants were prescribed off-the-shelf insoles (29 made of EVA and 1 pair made of carbon fibre). For one participant, type of insoles data were missing. The EVA insoles had a medial arch support and a heel cup. Some insoles were modified (wedges, metatarsal pads, etc.) depending on the patient’s complaints. The EVA insoles had different hardness: 2 pairs were hard (Shore A: 50–55), 4 pairs were soft (Shore A: 35–40) and 56 pairs were intermediate (two layers of EVA of different hardness; Shore A: 20–45 and 50–55). Three participants’ EVA insoles data were missing.
The questionnaires were prepared and placed in the patient’s folder before the clinic appointment. At the time of the visit, the patient was given oral and written information about the study. After giving written consent, the participants were asked to complete three questionnaires. During the same appointment, the certified prosthetist–orthotist completed a participant checklist. After 4 weeks of insole use, the participants received the questionnaires again, this time by mail, and were asked to complete and return them in the prepaid envelope provided. A reminder was sent if the questionnaires had not been returned after 2 weeks.
Questionnaires
Brief Pain Inventory
The Brief Pain Inventory (BPI) is a multidimensional pain questionnaire that has demonstrated validity for use in the evaluation of chronic pain.15,16 All items are rated on a numerical scale from 0 (no pain/no interference) to 10 (worst possible pain/complete interference). The data were handled and scored as recommended according to a three-factor model, which includes the Pain Severity dimension and two subdimensions of the Pain Interference dimension: Activity (4 items) and Affective (3 items). 17 This model was chosen as it represents pain better than the two-factor model, in which Pain Interference is treated as a single factor. 18 The first question in BPI and the medication effect questions were omitted because no study has investigated their psychometric validity. 17
International Physical Activity Questionnaire–Short Form
The International Physical Activity Questionnaire (IPAQ) was developed and validated for studying PA in individuals aged from 15 to 69 years 19 and has also been adapted for elderly people. 20 In IPAQ, three categories of activities are reported: Vigorous, Moderate and Walking activities. These three categories are combined in one total PA score. The Walking category has earlier been investigated separately for reliability and validity. 21 Hence, because foot pain was expected to affect walking, in addition to the total PA score, this category was analysed and reported separately. The data were processed and analysed according to the IPAQ guidelines 19 with one exception: if the participant skipped one or two items of IPAQ or answered ‘I don’t know’, these responses were treated as missing instead of excluding the participant. This approach has been used previously for the Swedish IPAQ reference data. 20 Physical activity was reported as minutes per day in three categories, each representing different intensity in metabolic equivalent turnover (MET): Vigorous = 8 METs, Moderate = 4 METs and Walking = 3.3 METs. 19 The minutes per week of physical activity in each intensity category was multiplied by the number of METs for that category, and the sum of these three measures, that is, MET min/week, was used as the output unit.
Orthotics and Prosthetics Users’ Survey
The Orthotics and Prosthetics Users’ Survey (OPUS) is a self-report instrument that has been validated for users of prostheses and orthoses.22,23 Two OPUS modules modified in a previous study 23 were used in this study: Lower Extremities Functional Status (LEFS; 27 items) and Client Satisfaction with Device (CSD; 9 items), both rated on 4-point Likert scales. 23 The LEFS and CSD modules have demonstrated good test–retest reliability (intraclass correlation coefficient = 0.96 and 0.82, respectively) and are recommended for repeated measurements of patients over time. 24 In this study, six new items were added to raise the ceiling of CSD. 23 Three of them were adopted from existing instruments: ‘My device is effective (corresponds to my needs)’, 25 ‘I can use my device without being bothered by perspiration’ and ‘My device is easy to use’. 26 The other three items were constructed based on clinical experience: ‘I can use the shoes and clothes I want to when I use my device’, ‘I am satisfied with the size of my device’ and ‘I can use my device in all contexts I want to’. The nine old and six new CSD items were analysed according to the Rasch rating scale model. Items with an information-weighted (infit) or outlier-sensitive (outfit) mean square >1.4 in combination with an infit or outfit z standardized ≥ 2.0 were considered to misfit the Rasch model. 27 One item (‘I can use my device without being bothered by perspiration’) demonstrated misfit and was thus omitted. The remaining 14 items were used in this study.
The BPI, IPAQ and LEFS were used at both the initial and follow-up data collection, and the CSD was used only at the follow-up. Eight certified prosthetist–orthotists contributed to the data collection, by completing a checklist for each participant, including information about type of insole and insole-fitting history (first time or refitting).
In addition, a short demographic questionnaire was given to the participants, asking about body length and weight, to calculate the body mass index (BMI).
Ethics
The study was approved by the Regional Ethical Review Board, Uppsala, Sweden. All participants gave informed consent to the research and to publication of the results.
Statistical analysis
The IPAQ datasets were reported as continuous data by converting raw data to MET minutes (MET·min/week) according to the IPAQ guidelines, 19 but, as the IPAQ datasets were non-normally distributed (skewed to the left) and the BPI datasets were ordinal, non-parametric statistics were used for analyses and description of these data. The LEFS measures were converted to OPUS units on a scale from 0 to 100 by using Winsteps Rasch-analysis software, version 3.70.0.3, with the item difficulties and rating scale structures anchored based on the results from a previous study. 23 Similarly, the CSD measures were converted to OPUS units. Hence, parametric statistics were used for analyses and description of these data.
To detect any possible effect of insoles on pain and daily activities, Wilcoxon matched pairs signed-rank test and paired-samples t-test were used. To determine any potential differences according to sex, Mann–Whitney test was used. Two-sided p-values < 0.05 were considered statistically significant. Linear regression analysis was performed to describe the relation between participant’s satisfaction with insoles (independent factor) and the duration of insole use (dependent factor) according to CSD. The statistical analyses were conducted using SPSS 15.
Results
A total of 67 clients participated in the study. There were no statistically significant differences in age and BMI between men and women (p = 0.780; p = 0.880). Most of the participants had received insoles for the first time (p < 0.001; Table 1), but there were no statistically significant differences in BPI scores between clients with first time or refitting of insoles, neither before (p = 0.195–0.988) nor after (p = 0.094–0.539) using the insoles.
After 4 weeks of insole use, the analysis of all participants’ data showed a significant improvement (i.e. lower scores) on all three factors (Pain Severity and the Activity and Affective subdimensions of Pain Interference) of the BPI (Table 2). Women demonstrated significant improvement on all BPI factors except on the ‘worst pain’ item (p = 0.119). Men, on the other hand, did not show statistically significant improvement on any of the dimensions (Table 2). Women scored higher than men on Pain Severity, both before (p = 0.043) and after (p = 0.003) using the insoles.
Median (inter-quartile range) of pain severity and pain interference before and after fitting of insoles for clients with non-specific pain in lower extremities overall and according to sex.
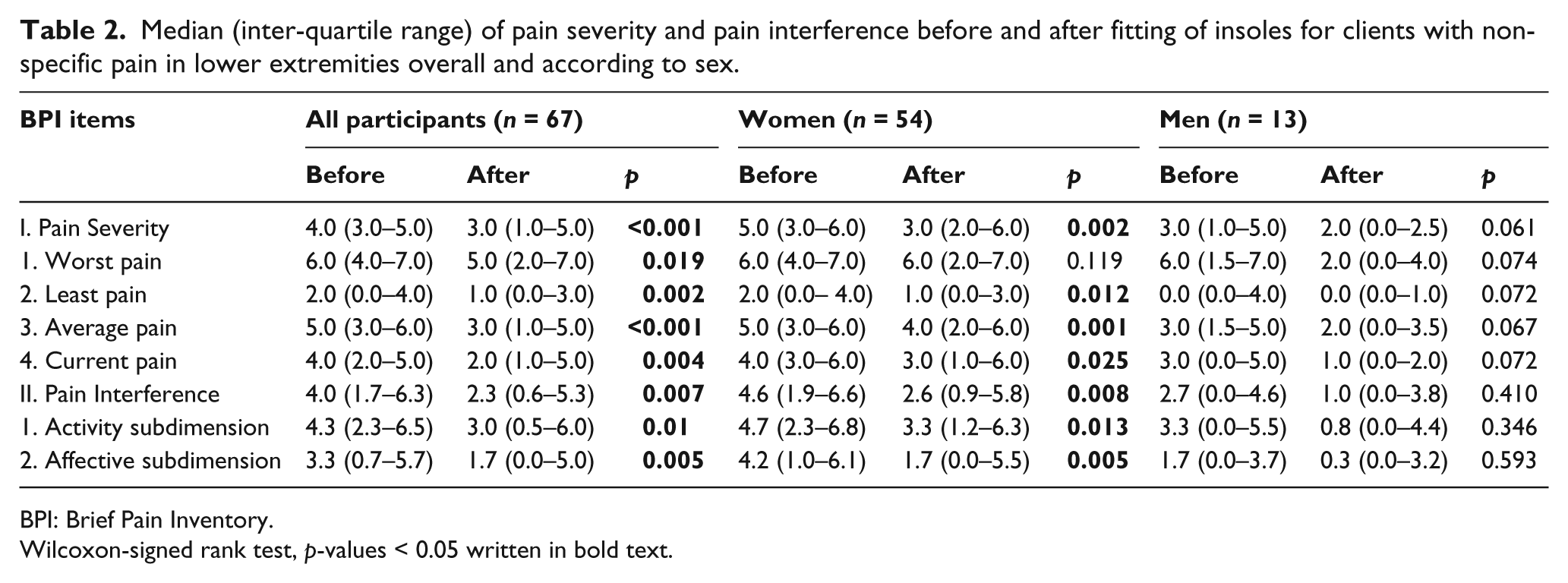
BPI: Brief Pain Inventory.
Wilcoxon-signed rank test, p-values < 0.05 written in bold text.
There were no statistically significant effects of the insoles on Total PA score or on the subcategory Walking, as measured by IPAQ (Figure 1). The median score for Total PA was 2384 MET·min/week before using insoles and 1425 MET·min/week after 4 weeks (p = 0.842). The median score for Walking was 891 MET·min/week before and 693 MET·min/week after using the insoles (p = 0.867).
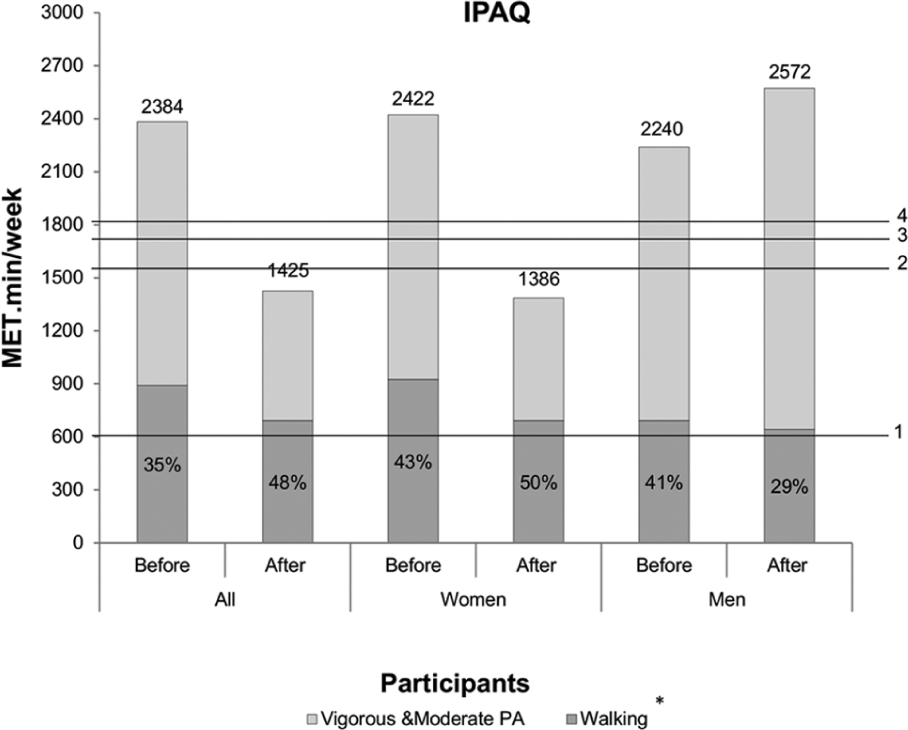
Median of physical activity and percentage of walking as measured by IPAQ.
Furthermore, there was no significant effect of insole use on ease of performance of daily activities as measured by LEFS (mean 57.1 for both before and after using insoles; p = 0.939). The mean duration of insole use was 6.5 h/day and the mean CSD value was 64.2 units. The duration of insole use and CSD values presented a very weak positive correlation (Pearson’s r = 0.2), and the linear regression was very low and not statistically significant (p = 0.122, R2 = 0.04 (95% confidence interval (CI): −0.20 to 1.64; Figure 2).
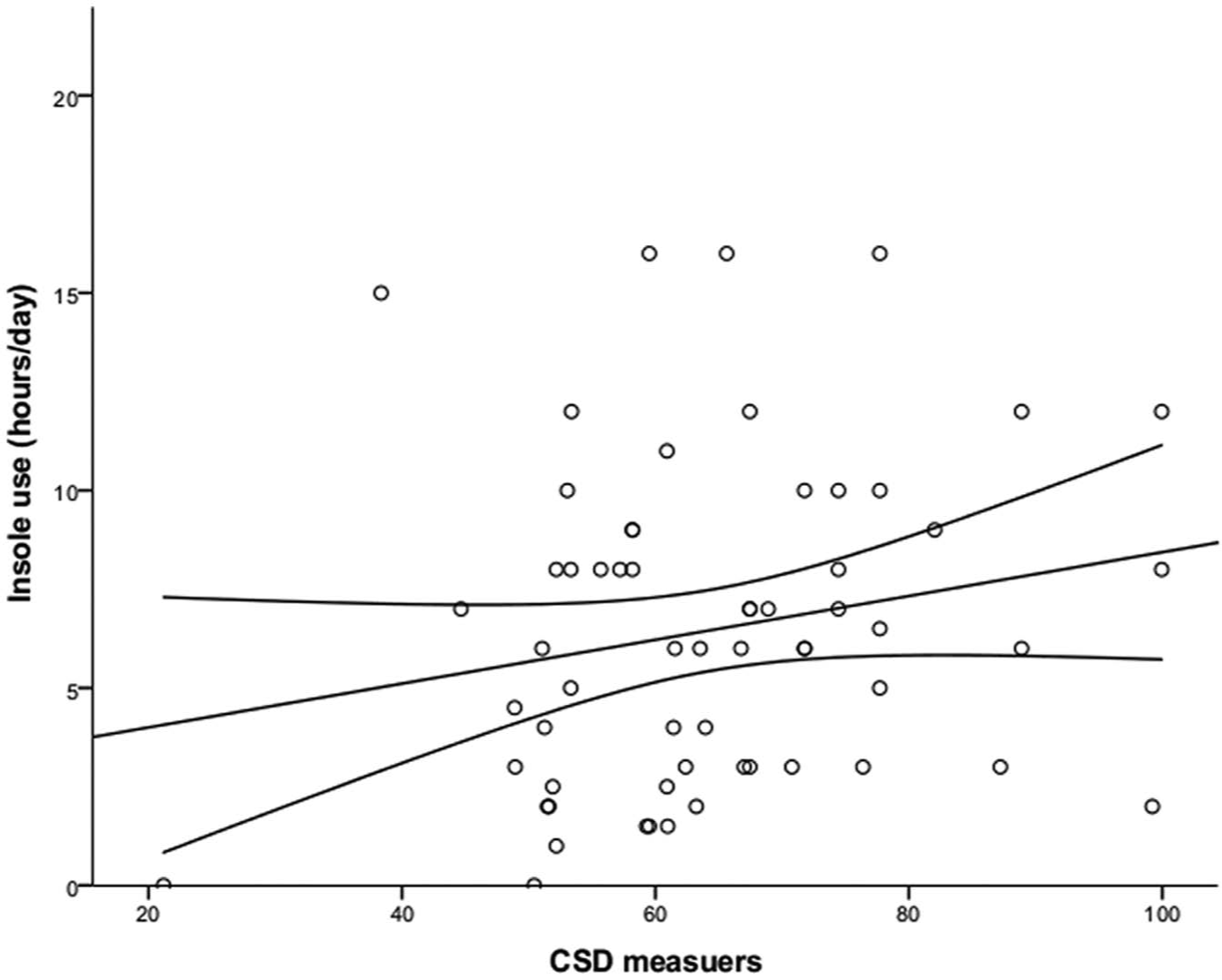
Relation between CSD units and duration of insole use. R2 = 0.04, p = 0.122, (95% CI: −0.20 to 1.64).
Discussion
This study shows that the clinical practice of treatment with insoles in women reduces pain severity and the negative impact of pain on daily activities and mood. These are important results, given that foot pain is prevalent and insoles are a common intervention. Importantly, the effects of insoles do not differ between individuals who are fitted with insoles for the first time and those who are refitted with insoles.
Surprisingly, the participants did not significantly increase their PA level (IPAQ) or their capacity for daily activities (LEFS), not even for women who reported a positive effect of insoles on pain interference with daily activities (BPI). This may have several explanations. First, pain may not have had a significant effect on PA level in this sample from the beginning; compared to the IPAQ reference data, the PA level in the sample was normal, 28 and the average participant met the World Health Organization recommendations for physical activities, that is, 600 MET·min/week. 29 Another explanation may be that PA levels are typically lower during the cold months of the year,30,31 and the fact that the weather was getting colder during the study period may have acted as a barrier for participants to increase their PA level. Furthermore, the follow-up period may have been too short to register any changes in PA level and capacity for daily activities. Pain reduction may not be a sufficient stimulus for individuals to increase their PA level; additional changes may be needed to alter established habits.
Analysis of how satisfaction influences the use of insoles was based on the assumption that if you are satisfied with a device, you will use it more. This assumption was not supported by the results and may indicate that the relationship between satisfaction and use is more complex. Some individuals may use insoles because they provide them with something useful, such as pain relief, while still not being very satisfied with them.
The effect of insoles on foot pain varied across the sample. There was a difference according to sex, showing that women had a significant reduction in all three BPI factors, whereas men did not report any significant reduction. It is important to note that the initial median values of BPI in Table 2 were low for males, which may give explanation for the non-significant results for men. These differences may be related to that the number of men was small and may have weakened the power to detect changes of pain among men. Another factor is the pain severity; this may be related to the fact that women had higher initial pain levels, which is in accordance with earlier studies. 32 The insole-fitting history was not an important factor for reduction of pain severity (the positive effects of insoles were the same); this is surprising, since a lower effect could be expected for those participants who already had insoles. The beneficial effect of refitting insoles could be due to the existing insoles being worn out or ill-fitting. This should encourage clinicians to refit clients with insoles even if the first fit has not been successful.
Although a control group would have improved the quality of the study, an uncontrolled study design was chosen based on ethical considerations. Despite this limitation, the study results have added further evidence for the role of insoles in reducing foot pain and for the level of support they provide in the performance of daily activities for people with foot pain. The major limitation in this study is its small sample size and the uneven distribution of participants based on sex. This limitation may explain why there were no significant differences in PA level between women and men in this study, as has been shown in other studies. 33 The use of subjective methods to evaluate PA level and foot functional status may be another limitation by increasing the probability of overestimation34,35 and recall problems. 36 However, by using repeated measures from the same sample, these limitations were presumably present in both the pre- and post-intervention data, which should reduce the impact of any reporting bias on the results.
In general, the results of this study provide additional knowledge on the effect of insoles on foot pain and will help to strengthen clinical decisions. Further studies should recruit more participants to increase the power of the study and should include a longer follow-up period as well as use objective methods to assess insoles effect and PA level.
Conclusion
Fitting insoles for women with foot pain appears to reduce the severity of pain and pain interference with daily activities. Based on the findings of this study, the reduction in pain severity is present in both first-time users and those refitted with insoles. The effect of insoles on activity performance needs further study. Duration of insole use cannot be predicted by users’ satisfaction alone.
Footnotes
Acknowledgements
We thank the participants and the staff at the Örebro University, Örebro, Sweden. We thank Anita Hurtig-Wennlöf, Associate Professor, School of Health and Medical Sciences Örebro University, Örebro, Sweden, for help with IPAQ, and the Centre for Rehabilitation Research, Örebro County Council, Örebro, Sweden, for providing research facilities for this project.
Conflict of interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.