
Abstract
Study design:
randomized, double-blinded, clinical trial.
Background:
Low back pain is one of the commonest disorders affecting the back. The literature reflects how over time excessive pronation of the foot has become to be recognized as linked to chronic low back pain, and how the problem can evolve for the better with the use of compensating foot orthoses.
Objectives:
The main objective of this study is to answer the question of whether the use of a certain type of custom-made foot orthosis alleviates low back pain.
Material and methods:
In a sample of 51 participants with excessive subtalar pronation and chronic low back pain (43 women and 8 men), the effect of custom-made foot orthoses in low back pain was studied. The study design was a randomized, double-blinded, clinical trial with two groups: experimental, treated with the custom-made foot orthoses, and control, treated with a placebo. Low back pain was evaluated by a visual analog scale for pain and Oswestry’s Disability Index Questionnaire for lower back pain at two moments—on the day of inclusion in the study and after 4 weeks of treatment.
Results:
The evolution of the low back pain showed significant differences in the experimental group, showing a significant reduction of pain and disability (p < 0.001, visual analog scale; p < 0.001, Oswestry’s Index).
Conclusions:
In the sample studied, the use of custom-made foot orthoses to control foot pronation had a short-term effect in reduction of perceived low back pain.
Clinical relevance
If subtalar joint hyperpronation plays a fundamental role in the pathomechanics of lower limb, and this can facilitate the development of low back pain, then controlling the abnormal mobility of subtalar joint by means of foot orthoses should improve this symptom. This article could help solve this controversy.
Background
Lower back pain (LBP) is one of the most common clinical disorders in the general population. It is estimated to affect 80% of the population at some point in their life. 1 The first episode occurs between 20 and 40 years of age,1,2 and the prevalence is high at ages from 30 to 60 years old.3,4 Despite its high incidence, there is no clear consensus on its etiology. One possible cause is abnormal foot function. Abnormal subtalar pronation, that is, pronation that occurs in an excessive way or when this joint would have to be supinating, causes increased internal rotation of the tibia and femur, and anterior inclination of the pelvis. This increases tension in the muscles of this region and rotation of the lumbar vertebrae during gait. 5 The presence of excessive calcaneal eversion generates internal rotation of the hips, and may consequently trigger increased pelvic anteversion and lumbar hyperlordosis. 6 Therefore, the foot posture can affect pelvic alignment and the position of the spine.6–8 Excessive calcaneal eversion, in association with other factors, should be taken into account when evaluating imbalances in the lower back. 8
Foot orthoses are often recommended as a treatment to control excessive subtalar and midtarsal pronation during the stance phase of gait. Although their mechanism of action on LBP is still not fully clear, several studies have found marked improvement in LBP after the use of different type of orthoses.5,9 The effect of the custom-made foot orthoses used in this study to improve LBP has not been evaluated previously, to the extent of the authors’ knowledge. The main objective of this study was therefore to evaluate the relationship between controlling excessive foot pronation by means of these custom-made foot orthoses and the evolution of LBP. The null hypothesis was that the level of LBP expressed by the experimental group after using the orthoses did not differ from the level of LBP expressed by the control group after the use of the placebo treatment.
Methods
Participants
A randomized, double-blinded, clinical trial was designed for this study. Seventy-one people were initially assessed for eligibility. Eleven persons were excluded: three subjects because of previous back surgery, two women because of pregnancy, and the remaining people because they were under medical analgesic treatment. The original sample consisted of 60 participants (51 women and 9 men), 34 corresponding to the experimental group and 26 corresponding to the control group. By the end of the follow-up period, there was a loss of nine participants who left the study for unknown reasons (four participants), medical treatment for LBP during the follow-up period (two participants), or because it was impossible to contact them (three participants), five from the experimental group and four from the control group (Figure 1). Of the 51 final participants, 43 were women and 8 were men, with a mean age of 40.63 ± 14.63 years. The sample consisted of patients from the Podiatric Clinical Area of the University of Seville, in the period from February 2009 to March 2011. The inclusion criteria were as follows: Foot Posture Index (FPI-6) indicating at least one pronated foot (i.e. ≥ +6), 10 presence of chronic nonspecific LBP, and age range of 18–65 years.1,2 The exclusion criteria were as follows: serious illness, pregnancy, previous back or lower extremity surgery, currently under medical or physiotherapy treatment for LBP or some foot pathology, and leg length discrepancy >5 mm. 11 All the patients gave their written informed consent for participation in this study. This study follows the guidelines from the CONSORT statement and was approved by the Experimental Ethics Committee of the University of Seville.
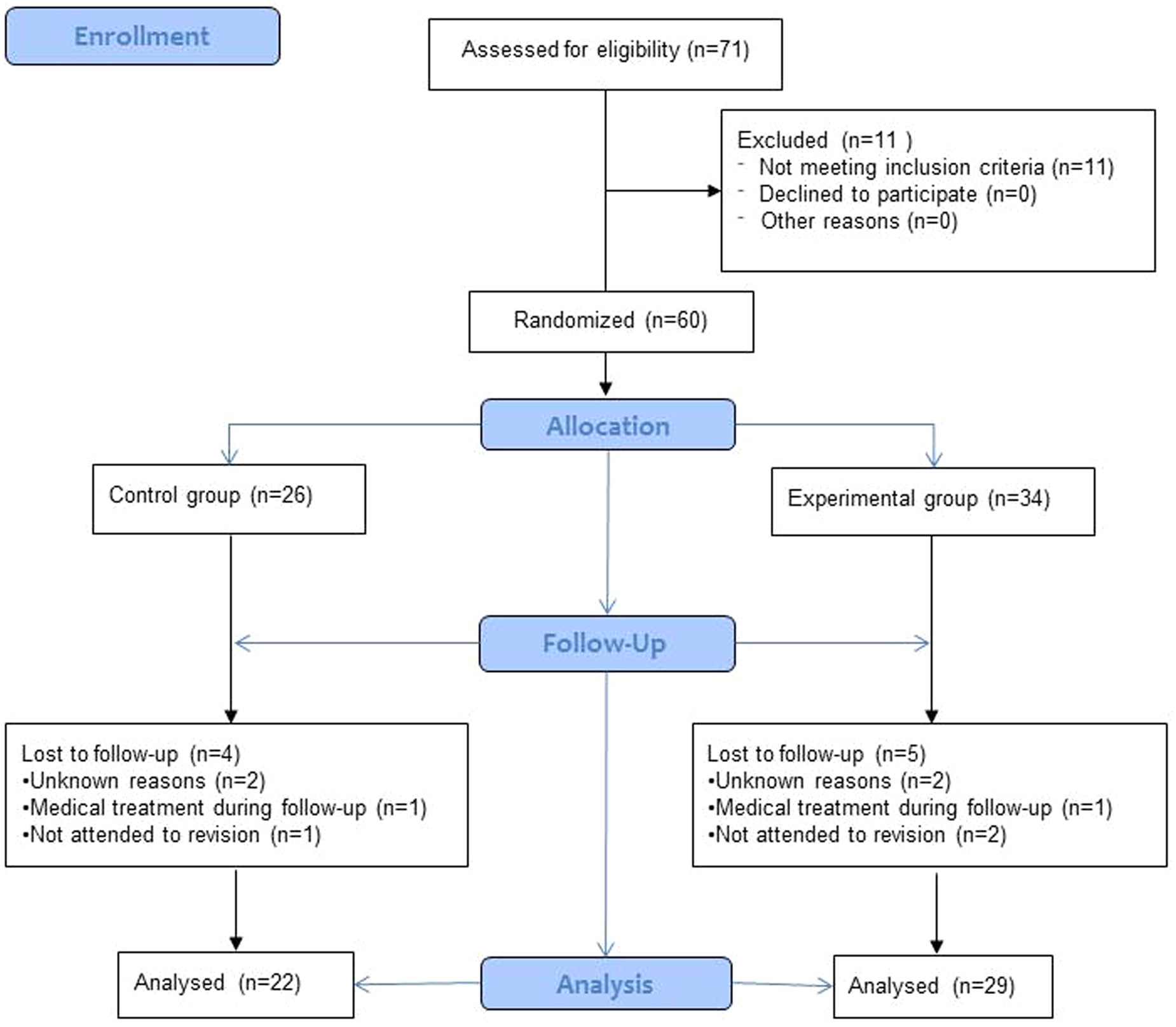
Flow diagram.
Procedure
On the day the patients came to the Podiatric Center, they underwent a routine biomechanical lower limb examination to determine whether they were candidates for treatment with foot orthoses. Participants were subjects with chronic LBP who attended the center seeking professional treatment for their feet, and if during the biomechanical examination, the clinician observed that they had an FPI-6 of ≥ +6, they were proposed to participate in this study. If patients refused to take part in this research, they were treated anyway. FPI-6, a method validated and recommended by various authors as a useful complementary tool for evaluating foot disorders, was also measured.10,12–14 The FPI-6 is a clinical tool aimed at quantifying the degree to which a foot can be considered in a pronated, supinated, or neutral position. Some studies have previously provided evidence for the validity of the FPI-6 as a clinical instrument for use in screening studies, as demonstrated good internal construct validity including good individual item fit and good overall fit to the model. 15 The FPI-6 scores predicted 64% of the variation in the static ankle/subtalar position during double-limb quiet standing, and 41% of the variance in ankle/subtalar position at midstance phase of gait. 16 Moreover, a recent publication states that the FPI-6 scores and individual components of the FPI-6 show strong statistical relationships to dynamic measures. 17 This test was always performed by the same investigator (A.C.M.), a podiatrist with 18 years of experience in making biomechanical examinations, who followed Redmond et al.’s 10 recommendations of completing at least 30 FPI-6 before making the measurement for some type of study. Participants were randomly allocated to each group by a collaborating investigator (P.V.M.) tossing a coin. The principal investigator was blind as to which group each participant had been allocated. Two types of foot orthosis was fabricated for each participant, custom-made foot orthoses and placebo. The control arm was given placebo foot orthoses and the experimental arm was given experimental foot orthoses. The treatment in each case (experimental/control) was administered by a collaborating investigator (P.V.M). The participants were also blind since it was not explained to them which kind of treatment was being studied. They were each informed that, whichever the treatment they had been administered during the study, at the end of the study they would receive the foot orthoses best suited to them. Moreover, the participants were instructed not to receive any other medical, podiatric, or physiotherapy treatment during this study, and avoid taking self-medication, and if any of these conditions are not met, they had to inform the researchers in order to be excluded from the study.
The dependent variable, chronic LBP, was measured using a 100-mm visual analog scale (VAS), which is considered to be a reliable method. 18 This measurement was complemented with Oswestry’s Disability Index Questionnaire for Lower Back Pain that provides information on the disability due to LBP and its impact on 10 daily activities, each of which is scored on five possible responses to give a disability percentage. 19 These measures of perception of back pain were assessed for each patient at the moment of inclusion in this study, and after 4 weeks of using the treatment. The follow-up time of 4 weeks was chosen in accordance with indications given in previous studies.9,20–22 The second assessment was performed by a collaborating investigator (P.V.M) to maintain the blinding of the principal investigator. A comparison of the initial and the final values was carried out.
Fabrication of the foot orthoses
The selection of the foot orthoses employed in this study was related to clinicians’ preference, as this type of orthotics are frequently used in the Podiatric Clinical Area of the University of Seville. After the biomechanical examination, phenolic foam molds were made of the patient’s feet under weight-bearing conditions. The patient’s foot was manipulated before being introduced into the phenolic foam so as to place the subtalar joint in the neutral position and the forefoot plantar plane parallel to the floor. The negative phenolic foam molds were filled with liquid plaster to obtain a positive mold of the foot on which to make the foot orthosis. The design and materials of the custom-made foot orthoses were the same for each individual in the experimental group. All the foot orthoses were made with polypropylene of 3-mm thickness from the heel to just behind the metatarsal heads, covered with a 2-mm-thick polyethylene foam layer of 35-shore-A hardness from the rearfoot until surpassing the distal part of the toes. A 3-mm-thick polypropylene sheet was heated to 180°C until it became transparent (after 2–3 min) for application in the vacuum press forming the orthosis. The following marks were painted onto the orthosis to guide the removal of the spare material: a calcaneal line parallel to the dorsal surface of the positive cast and 10–15 mm above the support surface level, one point just below the navicular tuberosity representing the maximum height of the orthosis on the medial side, and a distal line joining the points just proximal to the metatarsal heads and ending at the proximal edges of the first and fifth metatarsal heads. The spare material was removed by means of a polishing machine. Then, the 2-mm-thick polyethylene foam sheet was adhered to the upper surface of the molded polypropylene (Figure 2).

Foot orthoses applied to the experimental group.
For the control arm, a flat, 1.9-mm-thick insole was made of polyester resin as placebo treatment, adjusting it to the size of the foot and fitting it into the participant’s shoes, but not adapting it to the positive mold. The intention was not to alter the patient’s normal function (Figure 3).

Placebo treatment applied to the control group.
When the orthoses were finally applied to the patient, their definitive adjustment to the foot was made and the patient was asked to walk with them for a few minutes so as to report any discomfort or incidence. After any further necessary adjustments and once the patient stated that they felt comfortable, the adaptation was taken as being concluded. Instructions were given to the participants for wearing the foot orthotics for, at least, 8 h/day.
Data analysis
This study was designed to detect changes with an effect size greater than 0.8 (large effect size) for a contrast of pre- and post-test measurements on the same sample, assuming type I and type II errors of 0.05 and 0.2, respectively. The GPower 3.1.0 software package (Franz Faul, Universität Kiel, Kiel, Germany) was used to calculate the minimum sample size from these design values, giving a value of 21 participants per group. We assumed 15% loss during follow-up, so that a final total of 60 participants were recruited, 30 per group.
The data were analyzed with the SPSS software package (SPSS Science, Chicago, IL, USA). To analyze the intra-observer reliability of the measurements of the FPI-6, the intraclass correlation coefficient (3,1) was calculated on the basis of 10 feet selected at random from the sample and measuring FPI three times at a separation of 1 week between measurements.
The Shapiro–Wilk test applied to these data suggested that the Student’s t-test for paired samples should be used to compare each group’s expression of LBP between the initial moment and the end of the follow-up period.
The initial homogeneity of the dependent variable (the perceived pain) with respect to the experimental or control group was confirmed using Student’s t-test for independent samples. Other verifications made of homogeneity between the two groups were as follows: age (using Student’s t-test for independent samples), body mass index (BMI), and FPI-6 (using the Mann–Whitney U-test), and sex (using Pearson’s chi-squared test). Moreover, Student’s t-test for independent samples was employed to analyze differences in LBP between both groups independently at the end of the follow-up.
The effect size was calculated as Cohen’s d using the formula: (Mean 1 − Mean 2) / ([SD1 + SD2]/2), in which the value of d is positive if the difference between the means is in the predicted sense. This parameter classifies the effect size as small if d ≥ 0.20, medium if d ≥ 0.50, and large if d ≥ 0.80. Differences were considered to be statistically significant if p < 0.05.
Results
The intraclass correlation coefficient for FPI-6 was greater than 0.90, indicating that the methods used gave measurements with acceptable reproducibility (intraclass correlation coefficient for the right FPI-6: 0.997, 95% confidence interval (CI): 0.987–0.999 and intraclass correlation coefficient for the left FPI-6: 0.988, 95% CI: 0.953–0.997).
The control group consisted of 22 participants (20 women and 2 men) aged 19 to 64 years (mean 42.05 ± 15.17 years), and the experimental group consisted of 29 participants (23 women and 6 men) aged 18 to 64 years (mean 39.55 ± 14.38 years) Table 1 presents the mean, standard deviation, 95% CI, median, and interquartile range of the LBP for the two groups at the two moments of measurement.
Mean, SD, 95% CI, median, and interquartile range of low back pain measured on the VAS and Oswestry scale for each group at the beginning and end of the follow-up period.
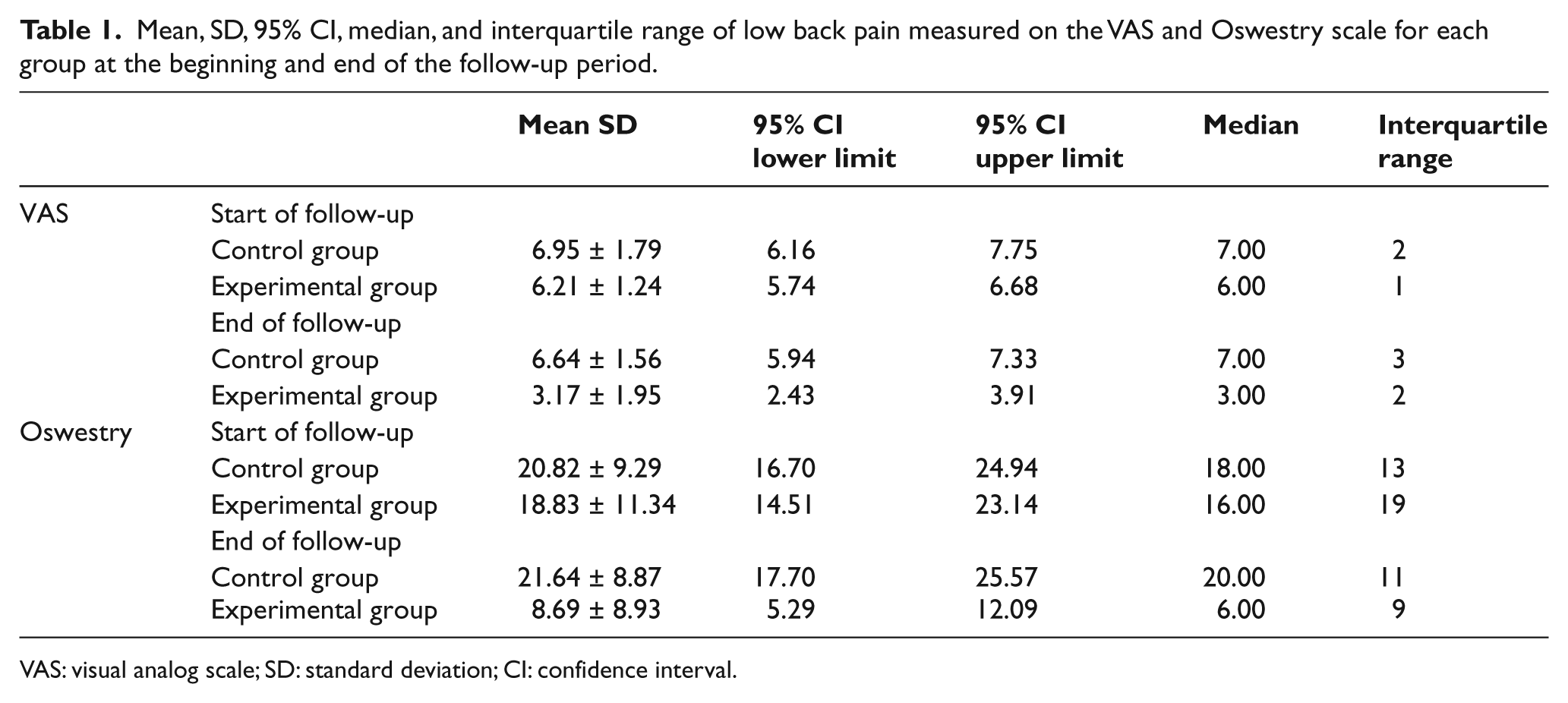
VAS: visual analog scale; SD: standard deviation; CI: confidence interval.
Homogeneity was not rejected in terms of age, BMI, sex, and FPI-6 (age: p = 0.552; BMI: p = 0.555; sex: p = 0.259; left foot FPI-6: p = 0.563; and right foot FPI-6: p = 0.953). A priori, therefore, the two groups were homogeneous and hence comparable (Table 2).
Mean, standard deviation, and p-value of sex, age, BMI and FPI for each group.

BMI: body mass index; FPI: Foot Posture Index.
In the initial exploratory analysis, the two groups were found to be also homogeneous in terms of the dependent variable as measured on both scales (p = 0.083 for VAS and p = 0.506 for Oswestry); therefore, no significant differences between the two groups were observed at the beginning of this study. However, at the end of the follow-up, there were significant differences in LBP between both groups (p < 0.001 for both scales).
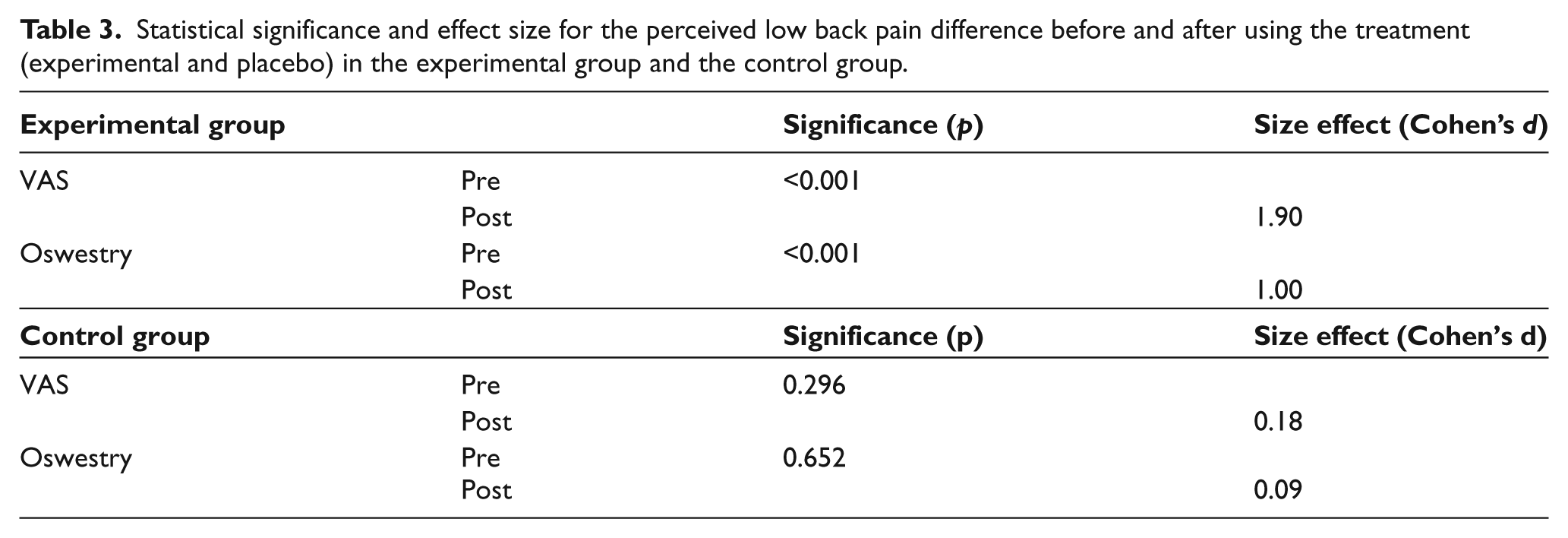
The measurements made at the end of the follow-up suggest that the experimental group showed significant improvements in self-reported LBP before and after the use of the orthoses, with the effect size being large (Table 3). One also observes in this table that in the control group, there were no significant differences following the use of the placebo insoles, and the effect size was small. These data suggest that a diminution of perceived LBP was related to the use of the custom-made foot orthoses, as the control group did not show such an improvement.
Statistical significance and effect size for the perceived low back pain difference before and after using the treatment (experimental and placebo) in the experimental group and the control group.
Discussion
The results showed that, while LBP did not disappear completely when the foot orthoses were applied for 4 weeks, it did improve significantly (p < 0.001). The study’s null hypothesis may therefore be rejected. The large effect size obtained in the comparisons suggests that it is highly likely that these effects also occur in the general population.
This study has certain limitations as, that is, the shortness of the follow-up time period, chronic LBP is not always permanent and more often recurrent with episodic flare-ups of varying duration. A longer duration of the follow-up would provide stronger evidence—the authors would note, however, that this has been the time used in previous similar studies.21,23 Another limitation could be that none of the spinal parameters that describe the spino-pelvic compensation mechanisms such as pelvic tilt and sacral slope, nor their potential influence in lumbar lordosis, were monitored; this could be an explanation for the incomplete relief of symptoms observed. Only excessive foot pronation was considered, although the authors maintain that it is not the only factor leading to LBP, as there may well be other factors that influence LBP that have not been taken into account in this study. Finally, the authors also accept that there were a major number of experimental losses in this study. These losses, however, were basically evenly divided between the experimental and the control groups (5 vs 4, respectively), so the authors do not think that this significantly influenced the results.
Excessive foot pronation has previously been considered to be a risk factor for LBP.6,8,21,24–27 During the contact phase of gait, the initial impact produces a reaction force from the ground causing an external torque that leads to subtalar joint pronation, knee flexion, and internal rotation of the lower limb.6,25,26 Excessive occurrence of this pronation leads to pelvic misalignment and lumbar hyperlordosis.8,27,28 Various studies describe how foot orthoses can influence this cascade of movements that induce problems at other levels.29–32 Novick and Kelley 33 find that treating excessive foot pronation with polypropylene foot orthoses improved not only the function of the foot but also the entire kinetic chain of the lower limb and back. Landsman et al. 21 find that foot orthoses can alleviate LBP after 4 weeks of use (VAS measurements). Cambron et al. 5 evaluated LBP (VAS and Oswestry scale measurements) over the course of a controlled clinical trial of 12-weeks duration. They observed an improvement in LBP after 6 weeks of use in the experimental group while the control group showed no significant changes. The results of this study seem to be consistent with all these studies.
The literature review of Sahar et al. 34 evaluated studies published until 2008 that examined the appropriateness of using insoles to prevent or treat LBP, excluding studies in which the foot orthoses were designed to treat leg-length discrepancies. They concluded that there was strong evidence that insoles were not effective for the prevention of back pain, and that the current evidence on insoles as treatment for LBP did not allow any conclusions. They therefore stressed the need to conduct more clinical trials to determine the effectiveness of their use in treating LBP.
The results for the experimental group indicate LBP improvement as measured on both scales due to the use of custom-made foot orthoses, even though the pain was not totally eliminated. Nonetheless, they also point to the advisability of including a biomechanical examination of the foot and leg in the protocol of evaluating and treating LBP. This could help reduce the health-care costs and workforce absenteeism resulting from patients suffering from LBP in addition to improving their quality of life. The authors must remind that other risk factors for LBP have not been included in this work, and they obviously have to be taken into account in those protocols.
Conclusion
The results of this study suggest that alteration of foot type toward a lower FPI-6 using custom-made foot orthoses seemed to reduce LBP. The orthoses employed reduced the VAS scale and Oswestry Index values in participants with excessive subtalar pronation in a 4-week follow-up period, although they did not totally eliminate this symptom. The differences observed and their effect size suggest that the same findings are likely to hold at the population level.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.