
Abstract
Background: Patellofemoral pain is one of the most common disorders affecting the knee. Forefoot varus and excessive subtalar pronation can be associated with patellofemoral pain. Foot orthotics may produce an improvement in symptoms.
Objectives: The aim of this study was to test whether patellofemoral pain is improved after four weeks of using custom-made foot orthoses.
Study Design: Clinical trial without control group.
Methods: Twenty-one subjects with patellofemoral pain were given custom-made foot orthoses (2-mm thick polypropylene and 4-mm thick polyethylene foam liner of 45 shore A hardness). Patellofemoral pain was evaluated with a visual analogue scale before applying the treatment, and at two weeks and four weeks follow-up. At the two-week check-up, a forefoot varus posting was added to the orthoses.
Results: Improvements in patellofemoral pain was significant in all comparisons: initial pain with pain at the two-week check-up (P<0.001), initial pain with pain at four weeks (P<0.001), and pain at two weeks with pain at four weeks (P<0.001). The effect size was large in all comparisons.
Conclusion: For the participants in this study, the custom-made foot orthoses were found to be an effective conservative treatment to reduce the symptoms of patellofemoral pain.
Clinical relevance
As foot orthoses are a conservative, simple and low-cost treatment, the improvement in symptoms represents major benefits for the patients with patellofemoral pain themselves, and for the public health system since it could reduce the costs deriving from other more complex treatments, such as surgery or prolonged periods of rehabilitation.
Background
Patellofemoral pain is one of the most common disorders affecting the knee and may affect up to 25% of the population. 1 It usually represents a major problem especially in active adolescents or young adults, or subjects with intense sports activity. It is a disorder with a wide range of symptoms, as persistent retropatellar pain, accentuated pain climbing or descending stairs, after a period of prolonged sitting, squatting down, crepitation of the joint or feeling of instability. 2
Despite its high incidence, there is no clear consensuson what are the causative mechanisms leading to this common problem. Explanations have been as diverse as changes in the Q angle, imbalances in the periarticular soft tissues of the knee, quadriceps weakness, vastus muscle imbalance, or bone abnormalities.2–4 Misalignment of the patellofemoral system is present in most of these theories either as a primary problem or as a result of some other alteration in the lower limb. This misalignment may not be caused solely by local mechanical problems of the joint, but may also result from excessive subtalar pronation which may alter normal tibial rotation in the stance phase of gait, leading to biomechanical defects in the patellofemoral mechanism.5–7 Tiberio stated that compensatory femoral internal rotation due to increased subtalar pronation may cause compression of the lateral aspect of the patella on the lateral femoral condyle. 8 Fourteen of the 16 individuals with patellofemoral pain who participated in the Johnston and Gross study had forefoot varus, 2 an alteration which often leads to compensatory subtalar pronation.9,10 Late excessive rearfoot eversion during the stance phase of gait increased the internal rotation of the lower limb in a study carried out by Souza et al., 7 and this could have been related to patellofemoral pain as an overuse lesion.
Foot orthoses are often recommended as a treatment to control excessive pronation of the subtalar and midtarsal joint during the stance phase of gait. Although the mechanism by which they act on the mechanics of the knee is not clearly understood, numerous studies have shown a marked improvement in patellofemoral pain with their use.2,5,11–15 Various types of foot orthoses have been studied to check their effectiveness in knee pain. These consist of simple lateral or medial wedges added to footwear,16–18 or standard 19 or custom-made foot orthoses, 2 all yielding a diversity of results.
The overall objective of the present study was to test the effectiveness of one type of custom-made foot orthosis in reducing patellofemoral pain. Secondary objectives were: to check what type of forefoot alignment existed in the patellofemoral pain patients who participated in the study, and to check whether they experienced a greater improvement when a forefoot posting was introduced into the foot orthoses. The null hypotheses tested in the study were: (i) the foot orthoses led to no reduction in patellofemoral pain; (ii) patients with patellofemoral pain have no tendency to present forefoot varus deformity; and (iii) the forefoot varus posting did not enhance the relief of the patellofemoral pain.
Methods
Subjects
Twenty-one subjects with patellofemoral pain, six women and 15 men, mean age 26.57±11.05 years, participated in the study. They had presented at the Podiatric Clinical Area of the University of Seville seeking professional consultation in the period January 2009 to May 2011. The subjects were considered suitable candidates for orthotic intervention if they met the following criteria: retropatellar or peripatellar pain caused by at least two activities from among running, walking, hopping, squatting, stair climbing, kneeling or prolonged sitting; duration of symptoms longer than six weeks; pain of insidious onset; pain unrelated to trauma; worst pain in the previous week of at least 30 mm on a 100-mm visual analogue scale (VAS); and pain elicited by patellar palpation, patellofemoral joint compression, or resisted isometric quadriceps contraction with knee slightly flexed. 15 Exclusion criteria were: musculoskeletal disorders of the knee different than patellofemoral pain; previous surgery on the knee; neurological lower limb disorders, knee pain treated with drugs, foot orthoses, or rehabilitation.
This work was in accordance with the protocol and followed the ethical and humane principles of research. Written informed consent for participation and publication, including publication of photographs of participants, has been obtained. The study was approved by the Research Ethics Committee of the University of Seville.
Procedure
On the day, the subjects came to the center they underwent a routine biomechanical examination to check whether they were candidates for treatment with foot orthoses. The mobility of the forefoot was measured with the individual supine on the examination table, the subtalar joint in neutral position by means of palpating talar head on the medial and lateral aspect of the foot, and placing the rearfoot in a position in which the head of the talus was equally perceptible on both sides. 20 Then, with the free hand, the forefoot was placed in maximum supination, i.e. until the moment prior to perceiving motion of the rearfoot. This position was maintained while the hand holding the rearfoot rested it carefully on the table so as not to change the forefoot position, and then placed a universal, two-armed goniometer with one arm parallel to the edge of the table and the other parallel to the plantar plane of the metatarsal heads. To measure the forefoot pronation, the procedure was the same except for putting the forefoot in maximum pronation (Figures 1 and 2).
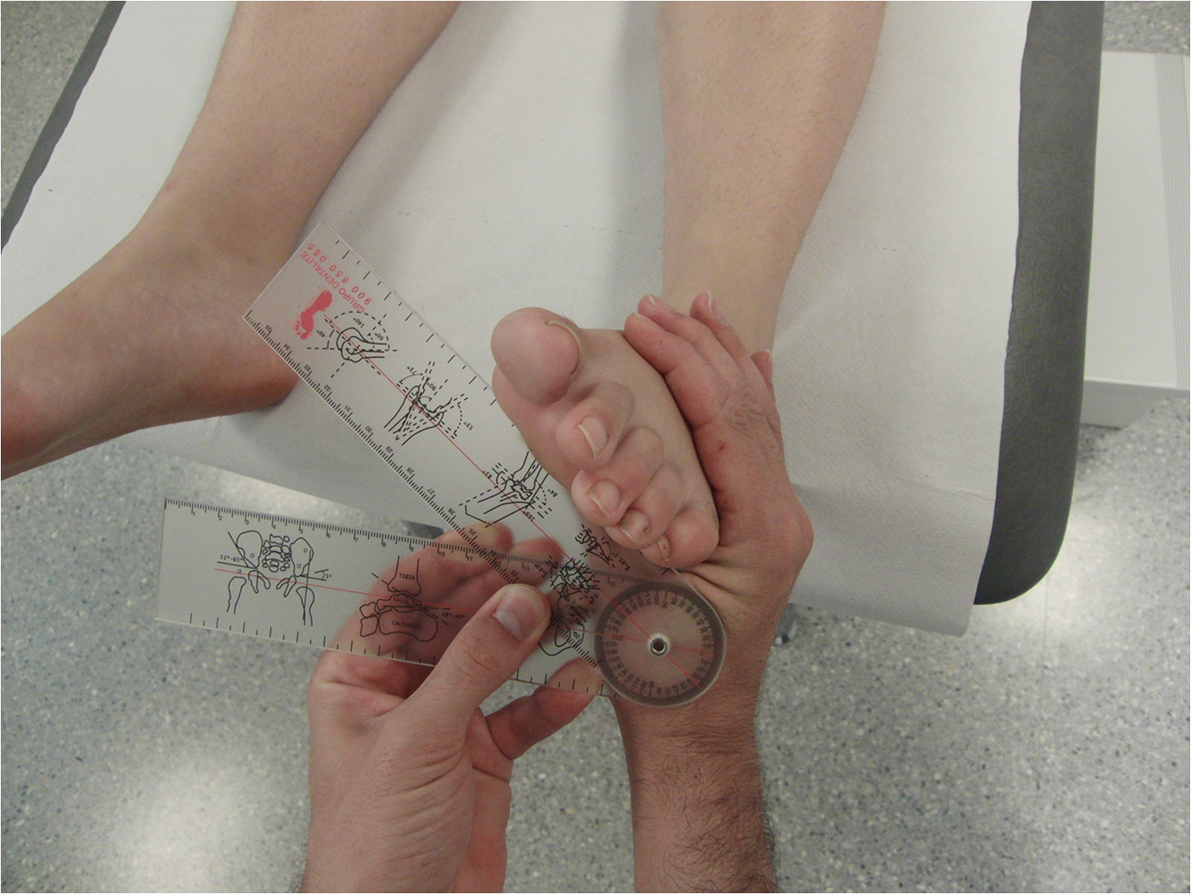
Method of measurement of forefoot supination.
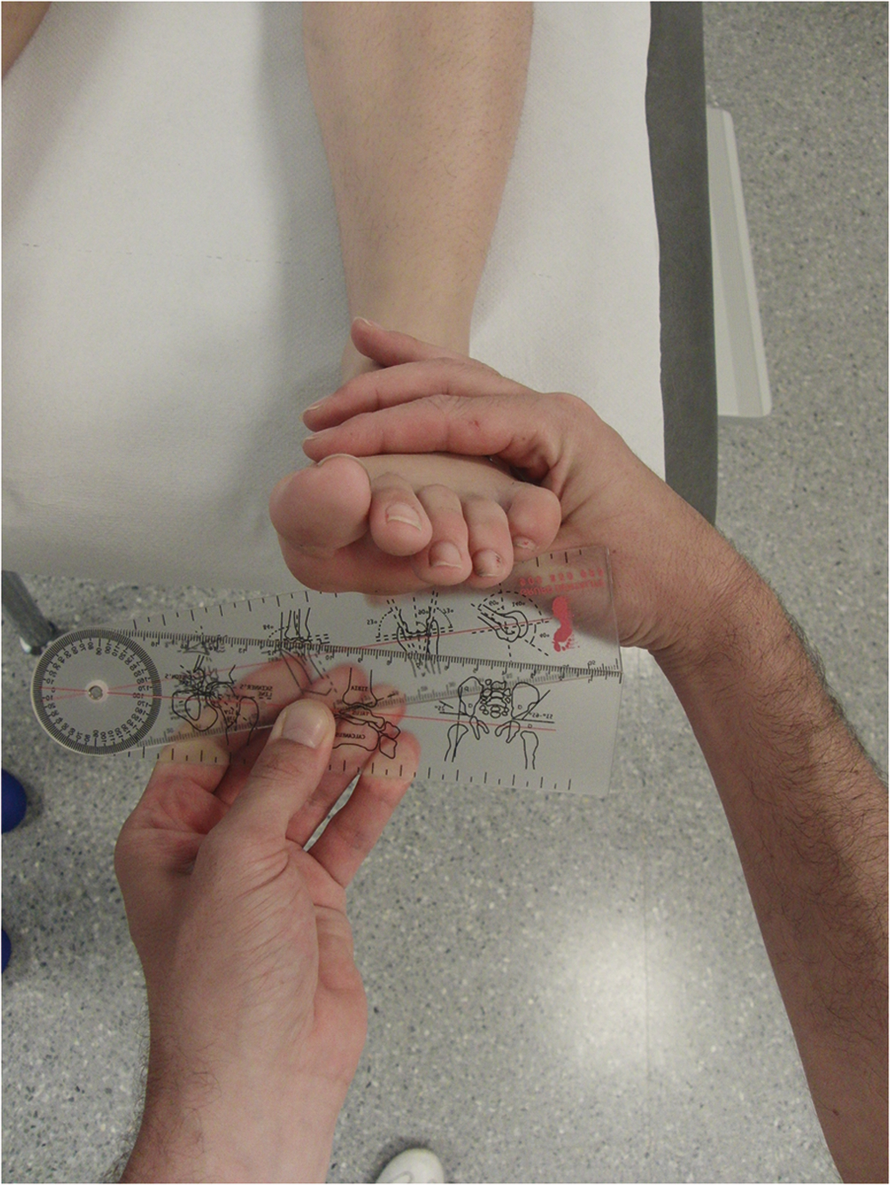
Method of measurement of forefoot pronation.
Once the foot orthoses had been made, and just before starting to use them, the patient was asked to mark the pain perceived in the last week on a 100-mm VAS (measurement 1–M1). The participant was asked to return after two weeks of use, to score the pain level perceived during the last three days on the same scale (measurement 2–M2), and a forefoot varus posting was added. After two weeks of using the foot orthoses with forefoot posting, the patient returned to the center and was again asked to indicate the pain perceived during the last three days (measurement 3–M3). The VAS is considered to be one of the best methods for estimating the intensity of pain, and has been reported to be a valid measure to detect clinical changes in pain perception in subjects with patellofemoral pain. 21
Fabrication of the foot orthoses
After the biomechanical examination, molds were made of patient’s feet under weight-bearing conditions with phenolic foam. The patient’s foot was manipulated before being introduced into the phenolic foam to place the subtalar joint in the neutral position and the forefoot plantar plane parallel to the floor. The negative molds of phenolic foam were filled with liquid plaster to obtain a positive mold of the foot on which to make the foot orthosis. All the foot orthoses were made with polypropylene of 2-mm thickness from the heel to just behind the metatarsal heads, covered with a 4-mm thick polyethylene foam layer of 45 shore A hardness from the rearfoot until surpassing the distal part of the toes.
The positive plaster cast was placed into a vacuum with the plantar surface upwards. A 2-mm thick polypropylene sheet was heated up to 180 degrees, until it became transparent (two to three minutes), for vacuum press forming the orthosis. Some marks were painted on the orthosis in order to remove the spare material. These marks were the following: a calcaneal line parallel to the dorsal surface of the positive cast and 10–15 mm above the support surface level; one point just below the navicular tuberosity, representing the maximum height of the orthosis on the medial side; and a distal line joining the points just proximal to the metatarsal heads and ending at the proximal edges of the first and fifth metatarsal heads. The spare material was removed by means of a polishing machine. Then, the 4-mm thick polyethylene foam sheet was adhered to the upper surface of the molded polypropylene (Figure 3).

Custom-made foot orthosis used in this study.
In the present study, the measurement of the mobility of the forefoot was used to decide the thickness of the forefoot posting that was added to the foot orthosis. It was applied 1-mm thickness per 10 degrees of difference in favor of supination movement compared to that of pronation as measured for the forefoot with the subtalar joint in neutral position. For example, an individual with 40 degrees of supination and 10 degrees of pronation would have a forefoot posting of 3 mm. The forefoot posting was also polyethylene foam of 45 shore A, and extended from the distal part of the polypropylene layer to the line corresponding to the subdigital space of the foot, leaving only the pads of the toes without support on the posting (Figure 4).

Medial posting added at two-week revision.
When the orthoses were finally handed over to the patient, their definitive adjustment to the foot was made, and the patient was asked to walk with them for a few minutes so as to report any discomfort or incidence. After any further necessary adjustments, and once the patient stated that they felt comfortable, the adaptation was taken as being concluded.
Data analysis
The study was designed to detect changes with an effect size greater than 0.6 (medium effect size) for a contrast of pre- and post-test measurements on the same sample, assuming type I and type II errors of 0.05 and 0.2, respectively. With these design values, the GPower 3.1.0 software package (Franz Faul, Universität Kiel, Germany) was used to calculate the minimum sample size, which was found to be 19 participants. We assumed 10% loss during follow-up, so that a final total of 21 subjects were recruited.
Data were analyzed with the SPSS package (SPSS Science, Chicago, Illinois). To analyze the intra-observer reliability of the measurements of the mobility of the forefoot, the intraclass correlation coefficient (3,1) was calculated, using 12 feet that were selected at random from the sample, and measuring pronation and supination twice at a separation of one month between each measurement. The Shapiro–Wilk test applied to the data showed the distribution to be normal in the first and second pain measurements, but not in the third. It was therefore decided to use Student’s t-test for paired samples to compare M1 with M2, and the non-parametric Wilcoxon test to compare M3 and M1, and M3 and M2. We calculated Cohen’s d to estimate the effect size, using the formula: (Mean 1 – Mean 2)/([SD1 + SD2]/2), where the value of d is positive if the difference between the means is in the predicted sense. This parameter classifies the effect size into small if d = 0.20, medium if d = 0.50, and large if d is greater than or equal to 0.80. Differences were considered to be statistically significant if P<0.05.
Results
The value of the intraclass correlation coefficient was 0.95 and 0.94 for supination and pronation of the forefoot, respectively. These coefficients can be considered very high, so that the reproducibility of the measurements is acceptable with the technique used.
The study included 21 participants. They all attended the two-week check-up (second measurement of patellofemoral pain–M2). The four-week revision (third measurement of patellofemoral pain–M3) was attended by 20 participants, so that the loss by the end of the study was of about 5% of the sample. The cause for this participant’s failure to attend was unknown. In the sample studied, there was a mean forefoot inversion of 36.5 ± 10.4 degrees (range 25 to 60 degrees), and a mean eversion of 6.1 ± 5.8 degrees (range 0 to 20 degrees). The thickness of the forefoot posting was 3 mm in 16 cases, 4 mm in four cases, and 5 mm in one case.
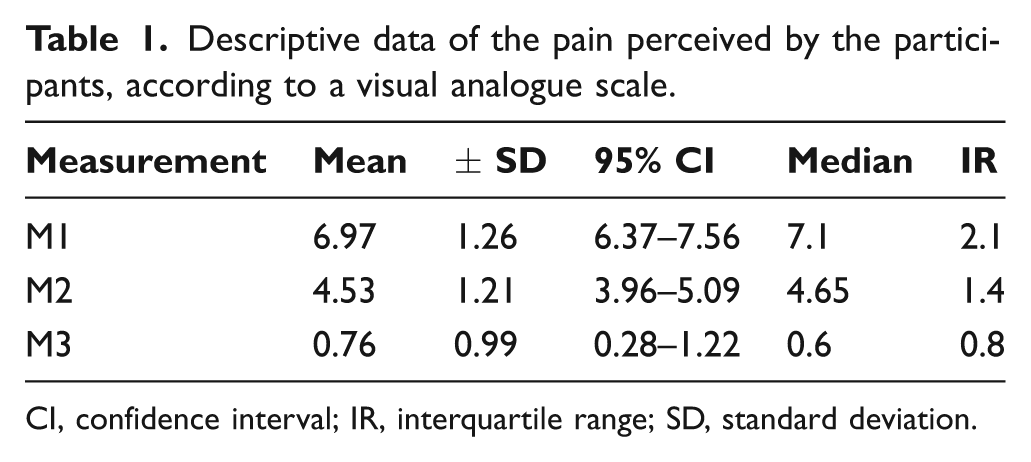
The descriptive values of patellofemoral pain obtained on the VAS for the three measurements (M1–M3) are given in Table 1, and Table 2 lists the P-values for each of the comparisons, and Cohen’s d for the effect size. Figure 5 shows the evolution of the symptoms in the sample subjects. It can be observed that the differences were significant in all three comparisons, and that the effect sizes of the changes were large.
Descriptive data of the pain perceived by the participants, according to a visual analogue scale
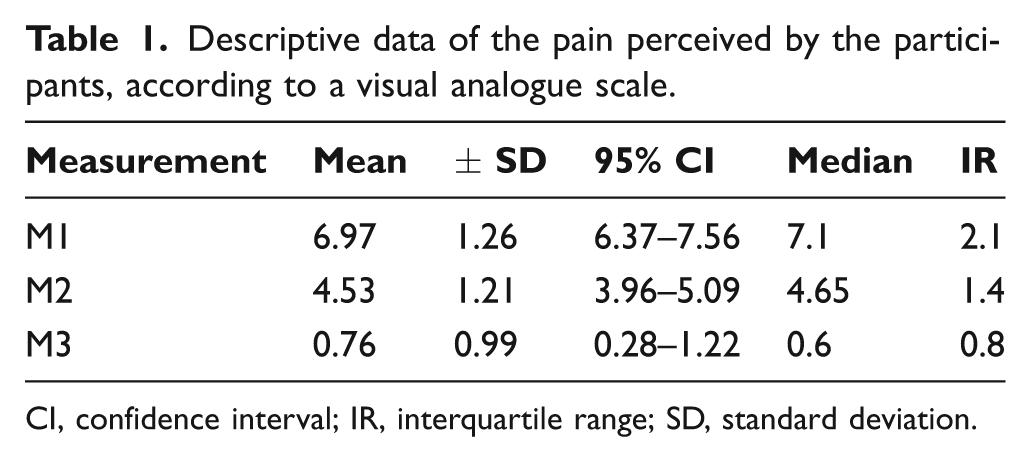
CI, confidence interval; IR, interquartile range; SD, standard deviation.
Statistical significance of the comparisons and the corresponding effect sizes
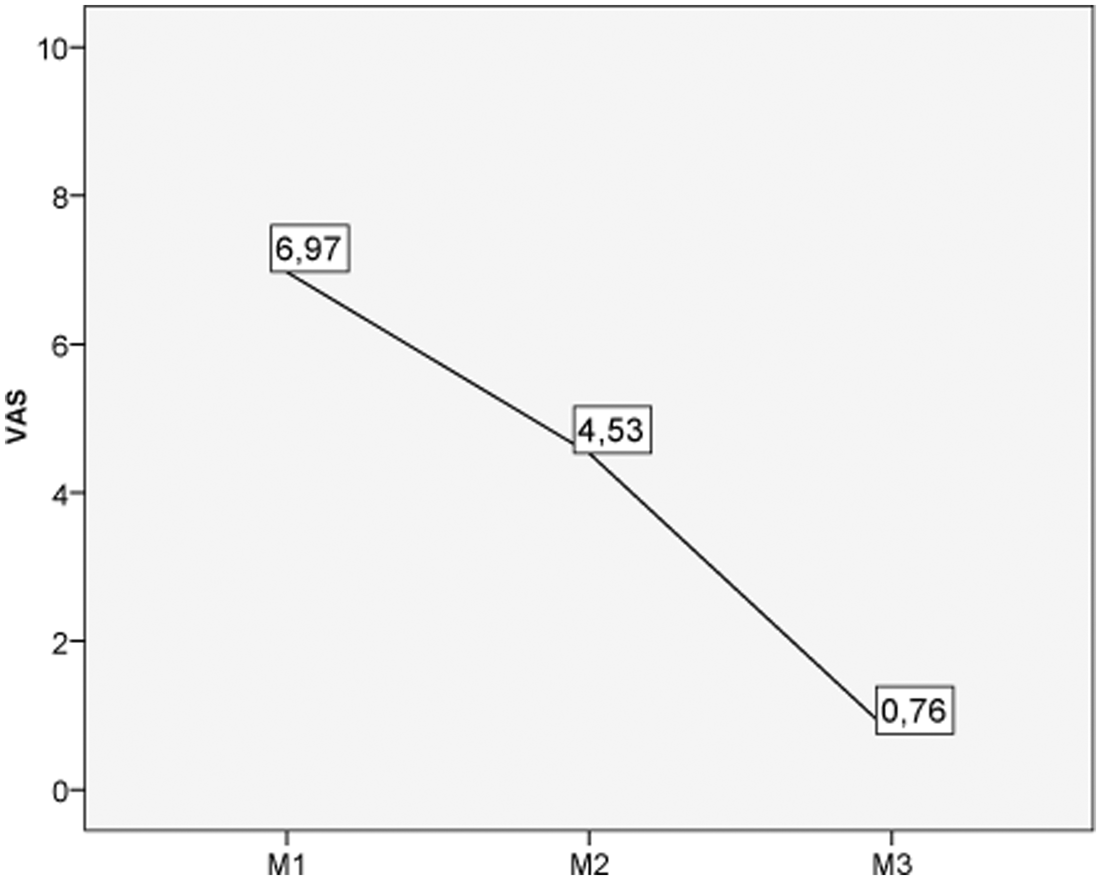
Values of the visual analogue scale before treatment (M1), at the two-week revision (M2) and at the four-week revision (M3).
Discussion
The results of this work have shown that the proposed conservative treatment reduced patellofemoral pain considerably in the participants. In addition, it was observed that the individuals with patellofemoral pain in this study tended to present forefoot varus, and that compensating this defect with a forefoot posting provided even greater reduction in pain. The results therefore allow us to reject the null hypotheses set out at the beginning of the study.
Before discussing the results, some aspects of the present work that might help improve future studies conducted in this line of research should be highlighted. The first aspect that could have added to the quality of the study would have been the inclusion of a control group together with the design of a randomized clinical trial to compare their results with those of the experimental group. This was not done in the present case because the patients came of their own accord to the Podiatric Clinical Area of the University of Seville for treatment, and, following their biomechanical examination, in all cases they were considered amenable to treatment with foot orthoses. Another limitation was that the participants wore the foot orthoses for only four weeks. Depending on the nature of the musculoskeletal injury, tissue can take longer to heal. 22 If the orthosis contributes to the ability of damaged tissue to heal then this process was just starting. Nevertheless, in a study in which similar foot orthoses were applied to evaluate their effect on reducing low back pain over a period of eight weeks, it was found that the greatest improvement was after two weeks of use, that there continued to be improvement until four weeks, following which there was stabilization without there being any return of increased pain. 23 A study by Trotter and Pierrynowski also found a great improvement in the first three weeks of using custom-made foot orthoses. 12 The maneuver measurement for forefoot movement could also be considered as a potential limitation. The measurement of the forefoot alignment with respect to the rearfoot is usually done using a technique that was described in 1986 by Smith et al. 24 We believe, however, that the procedure used in the present study provides more information on the function of the forefoot. Unlike the technique proposed by Smith et al., the present procedure yields information on the amount of supination performed by the entire forefoot and also on the amount of pronation. Debrunner and Hepp explain that the examination of the forefoot has to be done while holding the rearfoot firmly to block it, and then perform the forefoot supination and pronation, whose normal values according to those authors, are 35 degrees and 15 degrees, respectively. 25 This technique provides information on the relationship between the two movements, since a subject’s forefoot capable of 30 degrees supination and 15 degrees pronation is quite different from one capable of 30 degrees supination but 0 degrees pronation. During the propulsive phase of gait, the center of pressure should move from the lateral zone of the sole of the foot to the medial zone in response to the forefoot pronation driven by muscles that are particularly active at this stage, such as the peroneus longus and peroneus brevis. 26 The limitation of pronation of the forefoot could cause this mechanism not to develop normally, forcing pronation of the subtalar joint to compensate the deficit of load on the medial zone of the forefoot. Nonetheless, the technique used in the present work showed high levels of intra-tester reliability.
There is increasing evidence that treatment of forefoot varus with foot orthoses is effective in reducing patellofemoral pain. The present results in particular suggest that such treatment reduces the pain in cases in which the forefoot presents a movement of increased inversion. On average, the inversion observed in the participants was six times greater than the eversion, a higher ratio than that proposed by some authors as normal. 25 We would argue that this alteration of the forefoot causes it to function as a forefoot varus deformity. Similar results have been reported by other workers. Johnston and Gross examined the effect of foot orthoses on the quality of life of patients with patellofemoral pain, and added forefoot varus posting to 80% of their sample. 2 They showed improvement in pain, stiffness and physical activity after using foot orthoses for two weeks and in the follow-up after three months of use. 2 Eng and Pierrynowski found that the subjects who formed the group with patellofemoral pain in their study had a mean (±SD) of 12.4 (±3.7) degrees of forefoot varus. 5 They observed that the use of soft foot orthoses for eight weeks, together with a program of isometric exercises for the quadriceps muscle, reduced patellofemoral pain more than the exercise program alone. Saxena and Haddad examined 102 subjects of whom nearly 90% were diagnosed with patellofemoral pain, retropatellar dysplasia, or chondromalacia patellae, and needed to add forefoot varus posting in 91.2% of the cases, which led them to suggest that there might be a correlation between forefoot varus deformity and patellofemoral pain. 11 At other times, rather than forefoot varus, it has been excessive subtalar pronation which has been associated with patellofemoral pain.13,15,27 It should be noted that one of the compensation mechanisms of forefoot varus in gait is increased subtalar pronation.9,14,28
All these studies point to the existence of a strong functional relationship between the foot and knee. Pronation of the subtalar joint and flexion of the knee cause internal tibial rotation in a weight-bearing position. This internal tibial rotation occurs because the knee begins the stance phase of gait in an almost fully extended position, and then flexes to cushion the impact together with subtalar pronation. 6 Under normal conditions, these movements change to the midstance phase of gait, in which the knee begins to extend and the subtalar joint begins to supine. However, when the subtalar pronation is excessive or prolonged in time, for example because it is needed to compensate high forefoot inversion, 28 the external rotation of the tibia may be delayed. Tiberio calls this situation a ‘biomechanical dilemma’ for the knee joint, and it may be the source of patellofemoral problems since the movements of the patella are influenced by tibial rotation. 8 In the first degrees of flexion, the patella is looser, less pressed against the femur, thus allowing more movement, 29 and changes may be produced in the normal position of the patella on the femur. These changes may cause patellofemoral problems that can be controlled with the use of foot orthoses.
There might be several reasons why foot orthoses are effective in decreasing patellofemoral pain. One is that foot orthoses to control subtalar pronation would diminish internal tibial rotation in the late midstance and propulsive phases of gait, thus mitigating the ‘biomechanical dilemma’ referred to by Tiberio. 8 If the subtalar joint pronates during heel-off and push-off, the mechanics of the knee may be affected by changes in tibial rotation. When the knee is extended during gait, the tibia has to undergo external rotation. Subtalar pronation, however, forces internal tibial rotation. Foot orthoses would reduce this conflict. A second reason is that the Q angle would acquire a more physiological position with the use of foot orthoses, since increased or decreased Q angles would both result in areas of excessive pressure of contact of the patella on the femur. 30 A third reason would be that foot orthoses contribute to a more centralized position of the patella with respect to the femoral condyles, 31 possibly because of their effect on the rotations in the frontal and transverse planes of the tibia on the femur. Therefore, the reaction forces of the patellofemoral joint would be more evenly distributed between the two condyles. 5
Conclusions
The results of the present study suggest that custom-made foot orthoses, fabricated with 2-mm thick polypropylene and a 4-mm thick polyethylene foam liner of 45 shore A, reduced the patellofemoral pain in the participants. In most cases the improvement was increased by adding forefoot varus posting to the orthoses, since it was observed that the participants presented increased movement of inversion of the forefoot relative to that of eversion.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.