
Abstract
Background:
Knee arthroplasty is an efficient solution for osteoarthrosis in amputees. However, because of overload on the implant, it is apparently more subject to failure than in the non-amputated population. The aim of this case report is to show a failure of primary total knee arthroplasty contralateral to transfemoral amputation that required revision involving a tissue bank because of severely compromised knee bone. Surgical strategies, rehabilitation, and postoperative care for the operated limb and the contralateral prosthesis were demonstrated.
Case description and methods:
A 60-year-old patient with early failure of total knee arthroplasty contralateral to transfemoral amputation underwent arthroplasty revision in which a graft from a tissue bank was used. After the revision, prosthesis length adjustment and exercise therapy were fundamental to the rehabilitation.
Findings and outcomes:
The patient progressed well after the revision of the arthroplasty, with increases on the Knee Society Score and 36-Item Short Form Health Survey scales.
Conclusion:
Knee arthroplasty in amputees should be planned differently to that of the general population. For the procedure to be successful, there should be greater attention to implant stability, equalization of leg length, and a postoperative regimen including muscle strengthening and range of motion exercises to achieve the required knee flexion.
Clinical relevance
This case report is important because it presents a challenging case of a unilateral transfemoral amputee with failed arthroplasty over the years in the contralateral limb. To our knowledge, such a case has not been described in the scientific literature. It would be helpful for surgeons and rehabilitation professionals to chart out a treatment protocol and also to prevent premature failure of the joint.
Background
The incidence of knee-joint osteoarthrosis in the contralateral limb for amputees is much greater than in the general population (20% vs 2%), 1 with similar values for transfemoral, transtibial, and knee desarticulation. With increasing life expectancy among the population, arthroplasty has been used for this group of patients to seek improvements in lower-limb function, mobility, knee pain, and quality of life, which become further impeded because of amputated limb and greater energy expenditure while walking.2–6
However, the greater mechanical demands on the implant, due to the greater loading placed on the healthy limb knee in amputees, such as increased power generation during stance and extensor moments and power absorption at toe-off, may lead to higher rates of early failure and revision of the implant. 7
In this case report, we present an occurrence of failure of primary total knee arthroplasty contralateral to transfemoral amputation that required revision involving a tissue bank because of severely compromised tibia bone. We demonstrate the surgical strategies, rehabilitation, and postoperative care for the operated limb and the contralateral prosthesis.
Case description and methods
The patient was a 60-year-old male who was involved in a road traffic accident 20 years previously. He sustained compound fractures of the left tibia and fibula, subsequently developed necrotizing fasciitis of the lower leg, and eventually underwent a transfemoral amputation.
After the infection had been treated and the residual stump had healed, a prosthetic limb appropriate for transfemoral amputation was fitted, consisting of a quadrilateral encasement, monocentric self-locking knee, and solid ankle cushion heel (SACH) foot.
The patient used the prosthesis approximately 10 h a day, walking without any assistive devices such as canes or crutches. He started to use a cane 15 years after the amputation due to right-knee pain. Until this time, he was able to walk without distance limitations, doing around 2 km within a single period and going up and down stairs without restrictions. Apart from the amputation, the patient had no other health issues.
The patient progressed with degenerative osteoarthrosis of the right knee, with great varus instability and lateral subluxation of the tibia. At the age of 56 years, he presented flexion contracture of 20° with varus tibiofemoral angle of 25° and significant pain, which caused functional impairment with regard to day-to-day activities. At that time, primary total arthroplasty was performed on his right knee, with extensive medial release, sacrificing of the posterior cruciate ligament, and lateralization of the tibial component for correction of the bone defect (Figure 1).
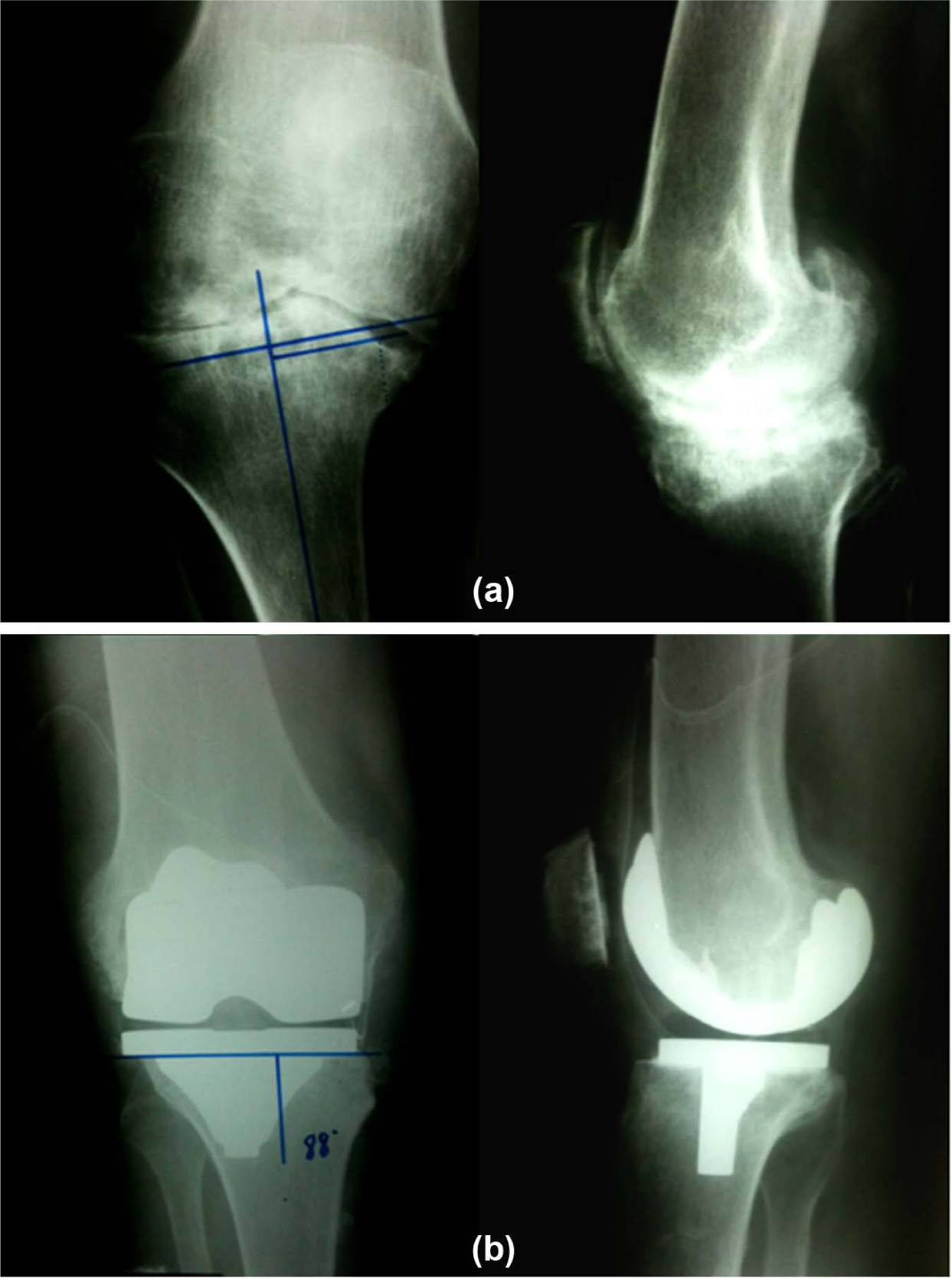
Radiographs in front and lateral views of the right knee (a) before and (b) after primary total knee arthroplasty.
After this procedure, the left-leg prosthesis was increased in length to match the length of the operated leg and adapt it to walking. The standardized postoperative rehabilitation at our institution consists of passive, assisted-active, and active exercises to gain range of motion, focused in gaining full extension and at least 90° of flexion in the first days after surgery. Surgery followed by gait training 2 days after surgery, progressing from a walking frame to a cane and to no walking aides when patient comfort allows, normally 6 weeks after surgery. Progressive muscle strengthening is performed from the first day after surgery, especially for the quadriceps, hamstrings, and hip abductors and extensors, starting with isometric exercises for the quadriceps and hip extensors and slowly initiating resistance exercises to knee extension. When these exercises are pain free, resistance is added as tolerated. 8
One year after the primary arthroplasty, the patient developed gradual varus instability and loosening of the tibial component. This led to a major anteromedial bone defect in the right knee (Figure 2).
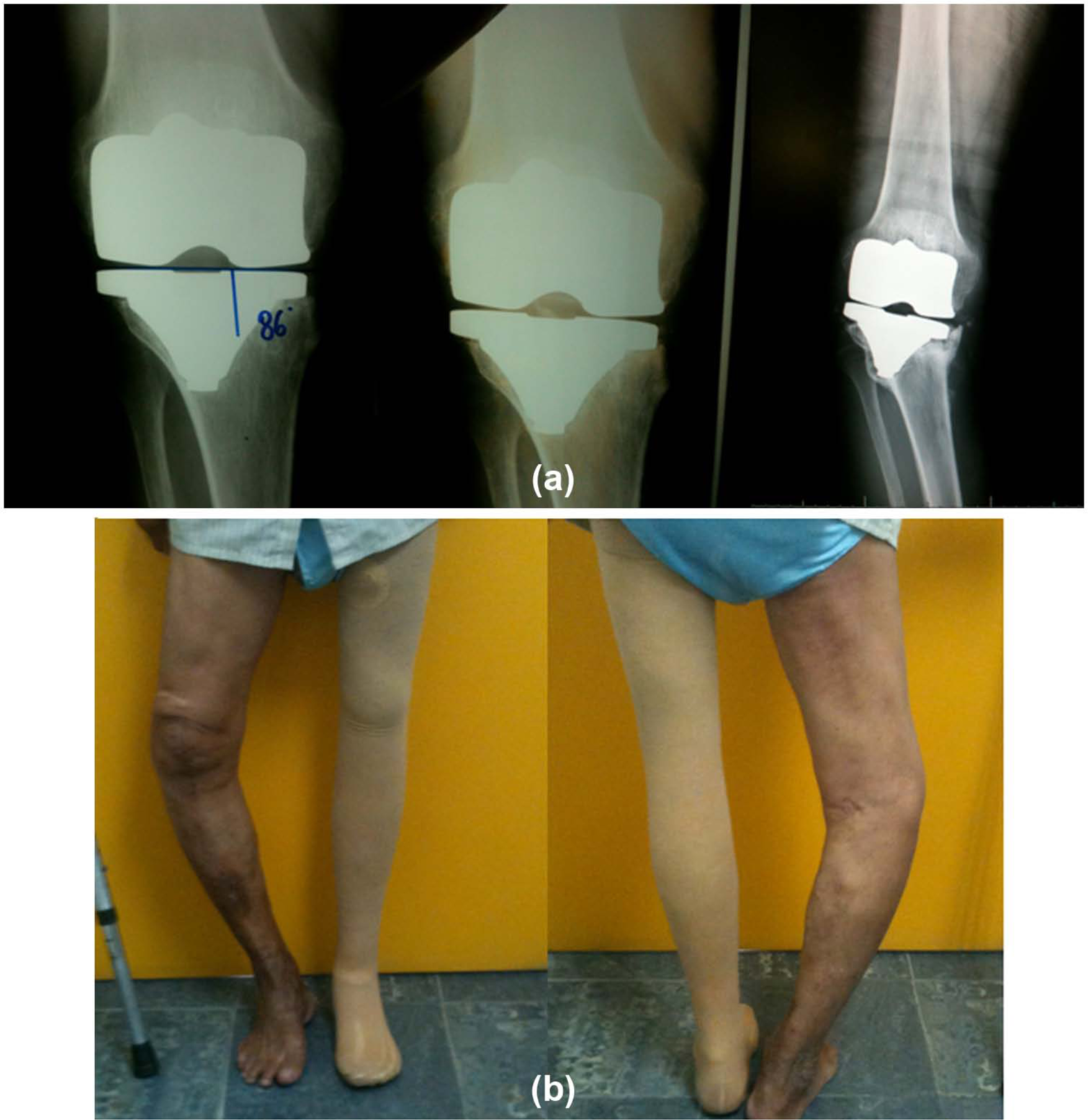
(a) Anteroposterior radiographs on the patient’s right knee with progressive varus deviation of the tibial component over the course of 3 years of follow-up and (b) clinical photos of the patient in front and back views, with right leg showing marked varus due to failure of total arthroplasty on the right knee.
Throughout the development of the instability, the patient continued to walk with the aid of crutches. He never used the wheelchair and he used the prosthesis on the contralateral limb. Despite the tibial bone defect, the patient had range of motion of 115°.
It was decided to revise the right-knee arthroplasty using a structured graft from a tissue bank in order to correct the bone defect, align the limb, and restore the patient’s ability to function.
In planning the revision of the arthroplasty, use of a proximal tibial component from a tissue bank was arranged, in order to fill the bone defect, along with femoral and tibial arthroplasty components with nails, for better stabilization. This technique is already used for this kind of deformities in non-amputated patients, but there are no scientific data available to describe this in contralateral above-knee amputees.
The revision of the arthroplasty was performed using a pneumatic tourniquet of 300 mmHg and a trans-quadriceps access route, complemented with an oblique access via the vastus lateralis muscle. 9 After debridement and collection of material for culturing, it was observed that there was a significant anteromedial cavity and peripheral defect in the proximal right tibia, which was classified as Anderson Orthopaedic Research Institute (AORI) type III, which means deficient methapyseal bone with bone loss compromising a major portion of the condyle or plateau. 10 Bone cuts were made in the femur, and the proximal tibia was prepared with a cut 2 mm below the lateral plateau. The femoral and tibial medullary canals were milled and prepared for the nails of the revision components to be inserted.
The tibial implant was cemented into the tissue-bank graft, the nail of the implant was cemented into the patient’s tibial metaphysis and diaphysis, and good stability was achieved. The femoral component was cemented with an intramedullary nail in order to increase the stability of the revision implant (Figure 3).

(a) Clinical photo during operation for revision of total knee arthroplasty using proximal tibial material from a tissue bank and cementation of the tibial component, with nail initially in the homologous tibia and subsequently in the patient’s tibia; (b) clinical photos of the patient in front and back views and radiographs of the right knee in front and lateral views, after total knee arthroplasty using proximal tibial material from a tissue bank.
During the immediate postoperative period, as a result of the surgery, there was a lengthening of the operated side by 4 cm, which necessitated an adjustment of the amputee prosthesis in order to equalize the leg lengths. The continual suction drain was removed on the first postoperative day, and a motor rehabilitation program, similar to the first arthroplasty surgery, was immediately instituted, with gains in range of motion, progression of weight-bearing, and muscle strengthening. Because of the long time taken for integration between the tissue-bank graft and the host bone, the progression of weight-bearing was slower than in conventional revisions, and it was decided to maintain partial weight-bearing with a walking frame for 12 weeks. The progression to a cane and to no walking device took four more weeks and was done as the patient tolerated.
Six months after surgery, Knee Society Score (KSS), a knee scale which evaluates intensity of pain, range of motion, stability in the anterior–posterior and medial–lateral axes, flexion deformities, and contractures and alignment ranging from 0 to 100, was taken, and a 36-Item Short Form Health Survey (SF-36) questionnaire, which is a short form measure of generic health status in the general population consisting of eight domains, which are physical functioning, physical role functioning, bodily pain, general health perceptions, vitality, social role functioning, emotional role functioning, and mental health, was administrated. Ethical approval was obtained from our institution scientific committee, and informed consent was obtained for this case report.
Findings and outcomes
The revision of the arthroplasty in this patient with contralateral amputation was seen to be successful. Adequate preoperative planning was fundamental to the success of the procedure. The range of motion of the operated knee, which had been a total of 115° of flexion and extension, was found to have been restored 6 weeks after the operation (Table 1). The patient was able to walk without the aid of crutches or a walking frame 4 months after the operation. The progression of weight-bearing was slower than in conventional cases because of the slower integration of the allograft. The KSS was 24 before the operation and increased to 85 in the sixth month after the operation.
Range of motion in degrees preoperatively and immediately, and 1 and 6 months postoperatively.

Table 2 shows the scores for the SF-36 questionnaire and demonstrates that there were improvements in all the domains after the surgery. Vitality, social role functioning, and emotional role functioning were the most improved domains.
Preoperative and 6 months postoperative SF-36 scores for a patient who underwent revision of total knee arthroplasty.
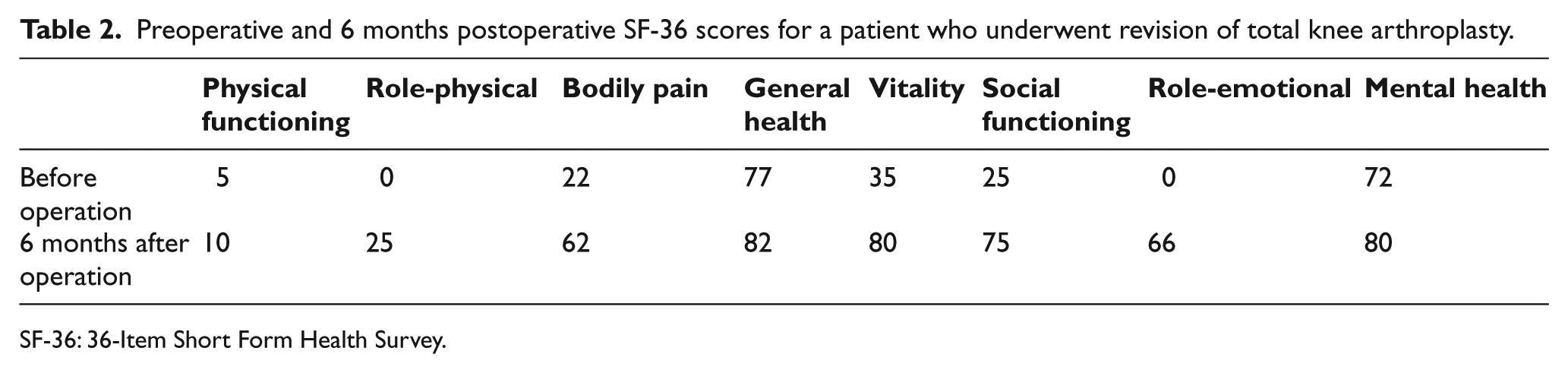
SF-36: 36-Item Short Form Health Survey.
Discussion
Patients who undergo amputations due to trauma while still young are subject to developing early arthrosis and undergo arthroplasty and revisions of arthroplasty earlier than is usual. Thus, strategies for preventing arthrosis in this population are almost mandatory. 11
The strategy of lateralization of the tibial component also needs to be commented on. In amputees, even after arthroplasty, weight-bearing continues to be distributed unequally between the legs because of postural adaptations, such that the replaced joint continues to receive more load. This increases the chance of failure of the arthroplasty. 12 One solution that might be more efficient would be to initially use a nail in the tibial and femoral components so as to increase the stability of the components and diminish the chances of failure, thus reserving the option of transferring the tibial base for non-amputated patients.
The rehabilitation for the patient advanced slowly because of the overload in the knee as a result of contralateral amputation, especially the gait training and progression to independent walking. Normally, patients are able to walk without walking aides approximately 6 weeks after total knee arthroplasty. Even though this was probably not the reason for failure, it is important to progress slower in this kind of patients to avoid potential problems.
In this case, the presence of difference in size of prosthesis compared to the healthy limb cannot be fully disregarded, which leads to greater weight-bearing on the contralateral limb. Friberg 13 showed that 70% of limbs with prostheses fitted were shorter than a healthy non-amputated limb, with Gaunaurd et al., 14 even with advances in technique and rehabilitation, reporting 57% being shorter. Such situations give rise to postural imbalance, with a tendency toward knee flexion during a large proportion of the gait cycle, along with varus, in an attempt to centralize the steps at the center of rotation of the body. 15 In the case of our patient, this would have led to weakening of the lateral structures and failure of the tibial component with varus deviation.
The tissue-bank material was used because of the severity of tibial bone defect not being suitable for unstructured graft or metal wedges to achieve stability of the component, 10 and also to increase the bone stock, should another procedure become necessary in the future. An unconventional endoprosthesis was also not used although it reduces the duration of surgery and does not require tissue-bank material, and there are higher chances of complications associated with it, higher chances of mechanical failures in the long term, and also non-preservation of the bone stock for possible new procedures in the future and higher rate of medium- and long-term mechanical failure. 16
During the immediate postoperative period, and before gait training and postural reeducation is started, it is fundamental to adjust the length of the prosthesis. This situation is best assessed by means of panoramic frontal radiographs with weight-bearing. Rigorous adjustment to equalize the length of the prosthesis with that of the non-amputated leg is imperative as otherwise it would lead to imbalance while walking and overloading of the knee implant. There will also be kinematic alterations to other joints, particularly those of the axial skeleton. 17
The incidence of amputation in the United States is around 100,000 per year. 18 With such high incidence and the high probability of development of osteoarthritis as a result of prosthetic leg, there is a trend toward increasing number of joint replacements in patients with amputations and, consequently, increasing number of arthroplasty revisions. Special care should be taken among amputees regarding the strategies for surgical procedures and postoperative rehabilitation care in order to avoid early failure of the procedure and impairment of the quality of life among this population.
So far we have not found any previous studies or reports on arthroplasty failure among amputees. Further studies should be conducted in order to assess the causes of failure in this population to prevent this problem.
Conclusion
Total knee arthroplasty among patients with a contralateral amputation is subject to failures. A careful operative technique aiming toward greater stability of the components and rehabilitation strategies involving equalization of leg lengths are important for the procedure to be successful.
Footnotes
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.