
Abstract
Background:
Although the majority of total knee arthroplasty cases have good outcome and survival, some arthroplasty eventually required revision. While early outcomes of revision knee arthroplasty are well reported, there is relatively fewer literatures reporting on the longer term outcome of revision knee arthroplasty. This study aims to review the outcome of revision knee arthroplasty for a longer term, and also make comparison between the two common indications for revision arthroplasty of infection and aseptic loosening.
Methods:
This study reviews all total knee arthroplasty revision performed at a single center over a 11 year period. Of the 48 cases found, 35 cases not lost to follow-up had a mean follow-up duration of 10.6 years (SD 2.9) for aseptic loosening, and 10.1 years (SD 2.6) for infection. Data of initial arthroplasty, revision arthroplasty, demographics, follow-up outcome were obtained, analyzed and compared.
Results:
Revision arthroplasty due to infection had more cases that required use of varus/valgus constraints (p ∼ 0.008) and extensile surgical exposure of quadriceps snip (p ∼ 0.005) compared to aseptic loosening. The survival at 10 years for this study is 91% overall (aseptic loosening 93.3%, infection 89.3%). Infection cases had significant initial improvement for range of motion (p ∼ 0.001) and use of walking aid (p ∼ 0.04) at post-operation 1 year, but no significant differences between the infection and aseptic loosening cases at 5 years and 10 years follow-up. Comparison between the two groups on other factors including initial arthroplasty, operative details, demographics, post-operative details and X-rays showed no statistically significant difference.
Keywords
Background
Total knee arthroplasty (TKA) has become a common surgical procedure in treatment of advance osteoarthritis for pain relief, improvement of function, quality of life and patient satisfaction. 1 –3 Survivorship for the majority of total knee arthroplasty had been reported as excellent. 4,5 However, a portion of primary knee arthroplasty were complicated with conditions which resulted in removal of arthroplasty and revision surgeries. 6,7 The reasons for revision of knee arthroplasty had varied across different literatures. 8 –13 The prevalence of knee arthroplasty revision was projected to be increasing. 14 Meanwhile, the cost and undesired clinical outcome of revision knee arthroplasty had also been reported as significantly higher than primary knee arthroplasty. 15 –17 In order to slow down the rising number of knee arthroplasty revision, many had advocated preventive measures for knee arthroplasty revision, especially for infection. Some measures involves the identification and management risk factors prior to primary knee arthroplasty. 18 –21
On the other hand, it is important to avoid complications in revision knee arthroplasty, and also determine the longer term prognosis of the procedure. According to literature, knee arthroplasty revision had been reported as an effective procedure. 15,22 Risk of failure in revision arthroplasty are mostly due to infection, 13,15 followed by stiffness, extensor mechanism problems, fractures and loosening. 23 However, a relatively fewer literatures are available reporting on the longer term outcome revision knee arthroplasty. 24 –26 We thus wish to add to the currently available literature. This study retrospectively review the experience with revision knee arthroplasty in the author’s center (a regional hospital in Hong Kong) to report on long-term outcome, survival and compare the outcome in accordance to indication of revision.
Methods
Data collection was first obtained utilizing the Clinical Data Analysis and Reporting System (CDARS) of the Hong Kong Hospital Authority. A list of all cases with the operative procedure quoted as “knee arthroplasty revision” in the author’s center from January 2004 to December 2014 were retrieved. Only cases with operation for revision of one or more components in a total knee arthroplasty were included. Cases excluded were exchange of polyethylene insert and conversion from Uni-compartmental knee arthroplasty.
Information obtained and analyzed for each case included: patient demographics, information of the initial knee arthroplasty, operative records, X-rays, laboratory test results, histological reports, and follow-up documentation. The cause of revision that was documented by the surgeon on the operation records were reviewed together with further post-operative information available.
Data for continuous values were described by means, standard deviations and range. Data of categorical values were described in absolute and relatives frequencies. Comparison was made between the two main groups of indication revision of infection and aseptic loosening. Statistical analysis was performed using Prism version 8.0 by GraphPad Software, Inc. Intergroup differences in continuous data were analyzed with two tailed t-test. Categorical values were analyzed with Fisher’s Exact test. Inter-observer for X-ray assessment were reviewed with kappa coefficient. Survival analysis was performed using Kaplan–Meier method with the aid of Excel Microsoft Inc. Statistical significance was determined as present with P-value 0.05 or less.
During the timeframe from January 2004 to December 2014, the reporting system found 56 cases with procedure coding of revision knee arthroplasty. Out of these cases, six of them had only received operation for infection with arthrotomy, debridement and exchange of polyethylene insert with retention of original tibial and femoral components. One case only had a revision of patellar polyethylene for patella-femoral joint pain issue. Another one case had removal of implant with replacement by a cement spacer for chronic infection, which had subsequent died from chest infection before a further revision knee arthroplasty could be implanted. A final 48 cases which had undergone operation of revision for one or more components of a total knee arthroplasty was included in this review.
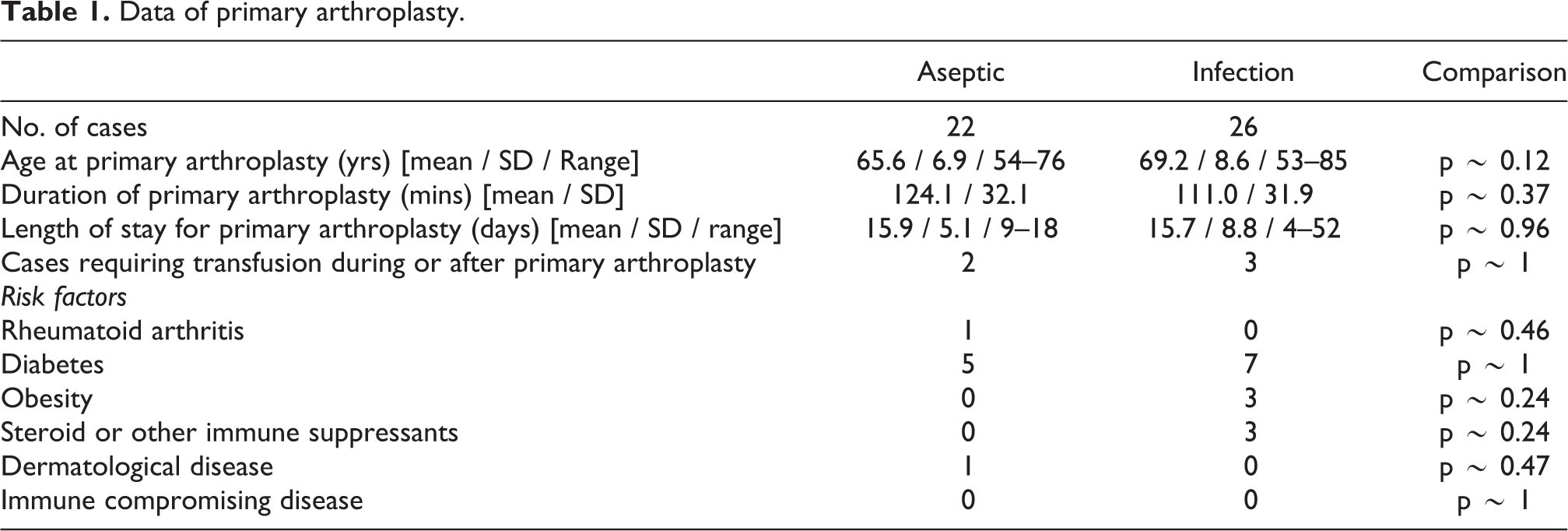
Among the 48 cases of revision knee arthroplasty, 22 cases were due to aseptic loosening, and 26 cases were due to infection. Comparison were performed between cases for indication for revision surgery, mainly in two groups the “Aseptic Loosening group” and the “Infection group.” Comparison that were made includes information of prior primary arthroplasty, risk factors for infection, data of revision operation, and details during post-operative follow-up. As for comparison of the revision operation, the final revision operation was accounted for comparison in the infection cases. No difference was noted between the data of primary arthroplasty between the two groups (Table 1).
Data of primary arthroplasty.
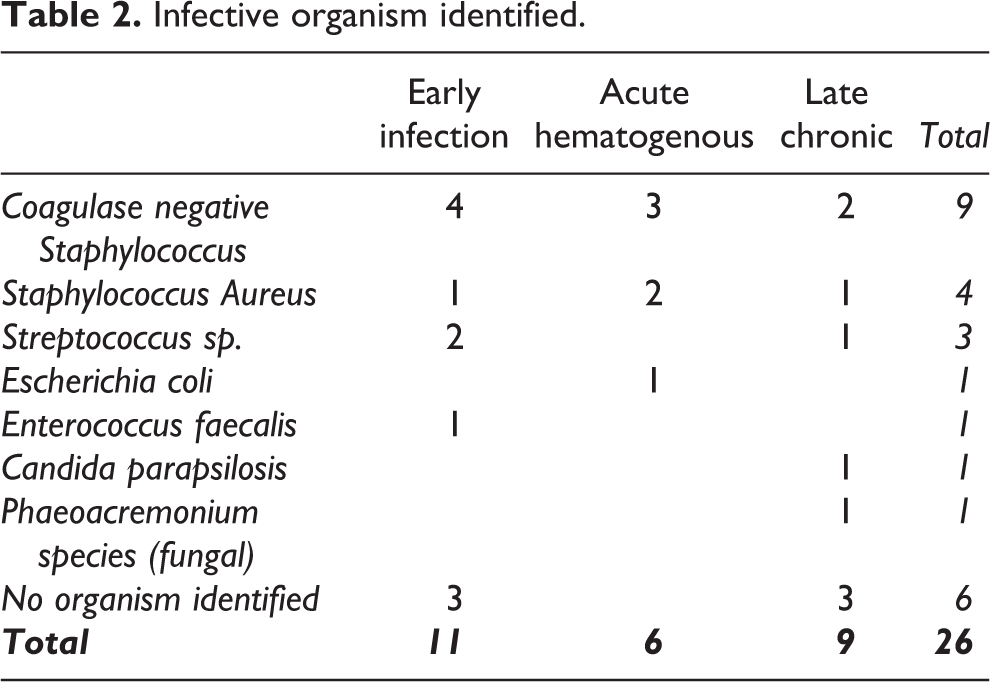
For the 26 infection cases: 15 cases had two-staged operation of removal of implant, replaced with antibiotic loaded cement spacer, then after a long course of antibiotics and infection had cleared up, received subsequent re-implantation with revision arthroplasty implant. 9 cases had implant removal, placement of antibiotic loaded cement spacer, long courses of antibiotics, repeated once or more additional operation debridement with exchange of cemented spacer, prior to re-implantation of revision knee arthroplasty after infection was deemed as cleared up. Two cases had one stage revision with subsequent course of prolonged antibiotics. All revision arthroplasty implantation for infection cases were performed with prerequisite that after an antibiotic free period of proximally 2 months, cases had no residual clinical features of infection, normalized serum white cell and inflammatory markers, and intra-operative frozen section showed less than 5 inflammatory cell count per high power field. Infective Organism identified were predominately gram positive cocci (Table 2).
Infective organism identified.
There are no significant difference in the data of initial primary knee arthroplasty between the 2 groups in terms of age, gender, pre-morbid risk factors, duration of primary knee arthroplasty, duration of inpatient stay, and transfusion rate (Table 1).
Revision operation for infection cases generally occurred earlier than aseptic loosening cases. This is evidenced by aseptic loosening cases had received their primary knee arthroplasty for a long duration before removal (mean 107.8 months, SD 50.8 months) compared to infection cases (mean 33.2 months, SD 39.1 months) (p < 0.0001). Even with early infection cases excluded (mean 52.9 months, SD 41.1 months), the duration of implanted primary arthroplasty in aseptic loosening cases was still significantly longer (p ∼ 0.0001).
The mean duration of follow-up for all cases was 9.1 years (SD 3.62). Eventually 13 cases, four cases in the aseptic loosening group and nine cases in the infection group, were lost to follow-up. There was no significant difference in the number of case lost to follow-up between the two groups (p = 0.3288). Reasons for lost to follow-up include 10 cases of death, two case of defaulting appointment, and one case referred to another hospital. Of the remaining 35 cases, average duration of follow-up was 10.6 years (SD 2.91) for aseptic loosening group, and 10.1 years (SD 2.60) for infection group. 45 (93.8%) cases had a minimal of post-operation 5 years follow-up, and 25 cases (52.1%) had at least 10 years follow-up after the operation
Results
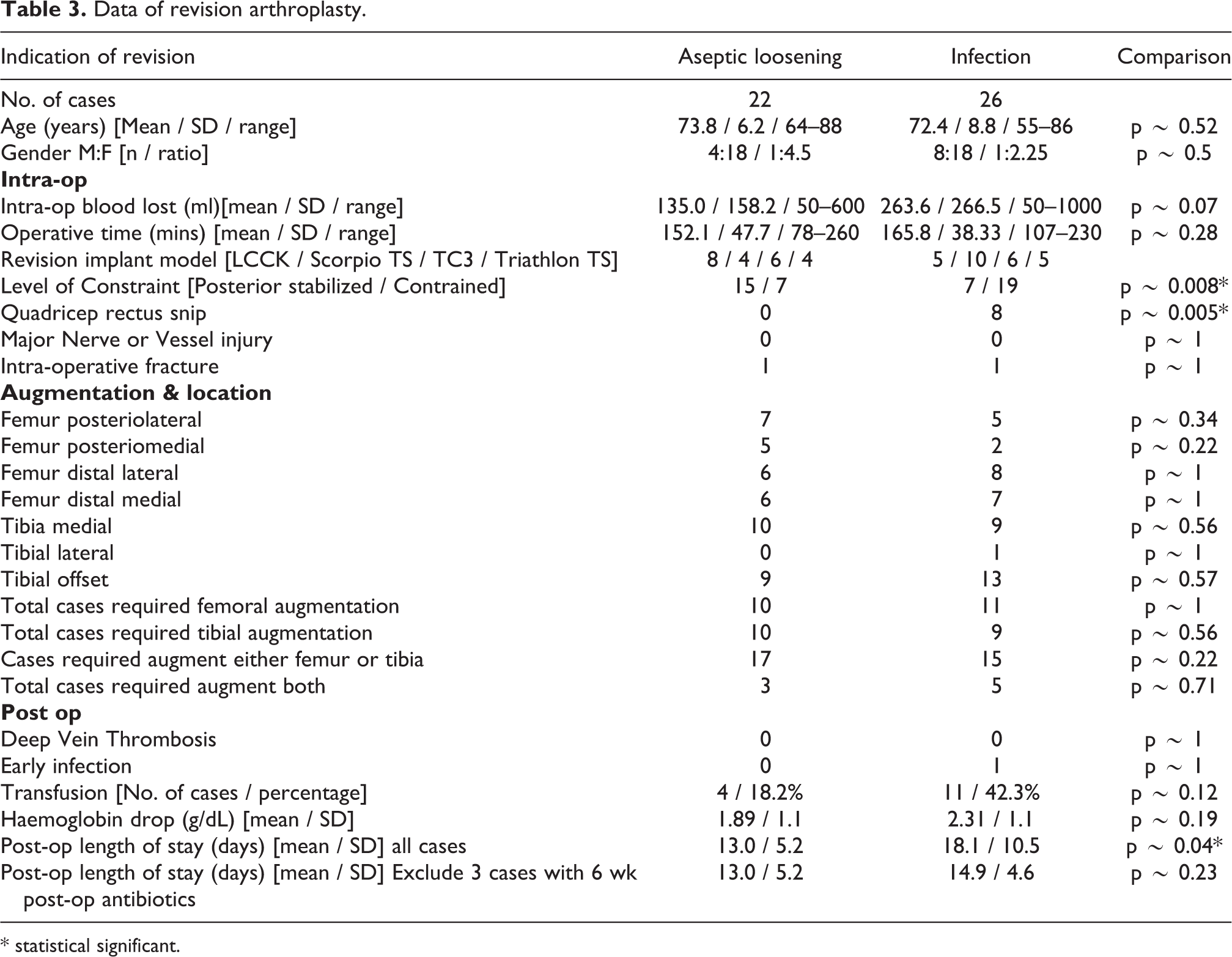
There is a significance more cases with higher level of constraint used for infection cases (19 constrain, 7 Posterior stabilized) compared to aseptic loosening cases (7 constrain, 15 posterior stabilized) (p ∼ 0.008). Condylar constrain systems used included Legacy Constrained Condylar Knee by Nexgen, Total Stabilization system by Stryker, and TC3 by Depuy (Table 3).
Data of revision arthroplasty.
* statistical significant.
More infection cases required “quadriceps rectus snip” intra-operatively for exposure (8 cases), compared to none in the aseptic loosening group (p ∼ 0.005).
Intra-operative blood lost of infection group seems higher than that of aseptic loosening group, this difference was just short of statistical significance (p ∼ 0.06). Post operative transfusion also appeared higher for the infection group (11 cases, 42.3%) than the aseptic loosening group (4 cases, 18.2%), but also short of statistical significance (p ∼ 0.12). Post-operative haemoglobin drop was also not significant between the two groups (Table 3).
Operative time of revision operation for aseptic loosening group (mean 152.1 minutes, SD 47.7 minutes) and infection group (mean 165.8 minutes, SD 38.3 minutes) showed no significant difference (p = 0.28). There was no significance difference in the number of implant augmentations used both in total and for individual locations. Prevalence of intra-operative fracture, post-operative deep vein thrombosis, and early infection was low and had no significant difference between the two groups. The post-operative length of stay for infection group was significantly longer (mean 18.1 days, SD 10.5 days), compared to aseptic loosening group (mean 13.0 days, SD 5.15) (p ∼ 0.04). However, there was 3 cases of infection group case that required six more weeks of antibiotics due to positive intra-operative culture that reported after revision operation. After excluding these three cases from the infection group (mean 14.9 days, SD 4.6 days), there was no significant different in the post-operative length of stay compared to aseptic loosening group (p ∼ 0.22) (Table 3).
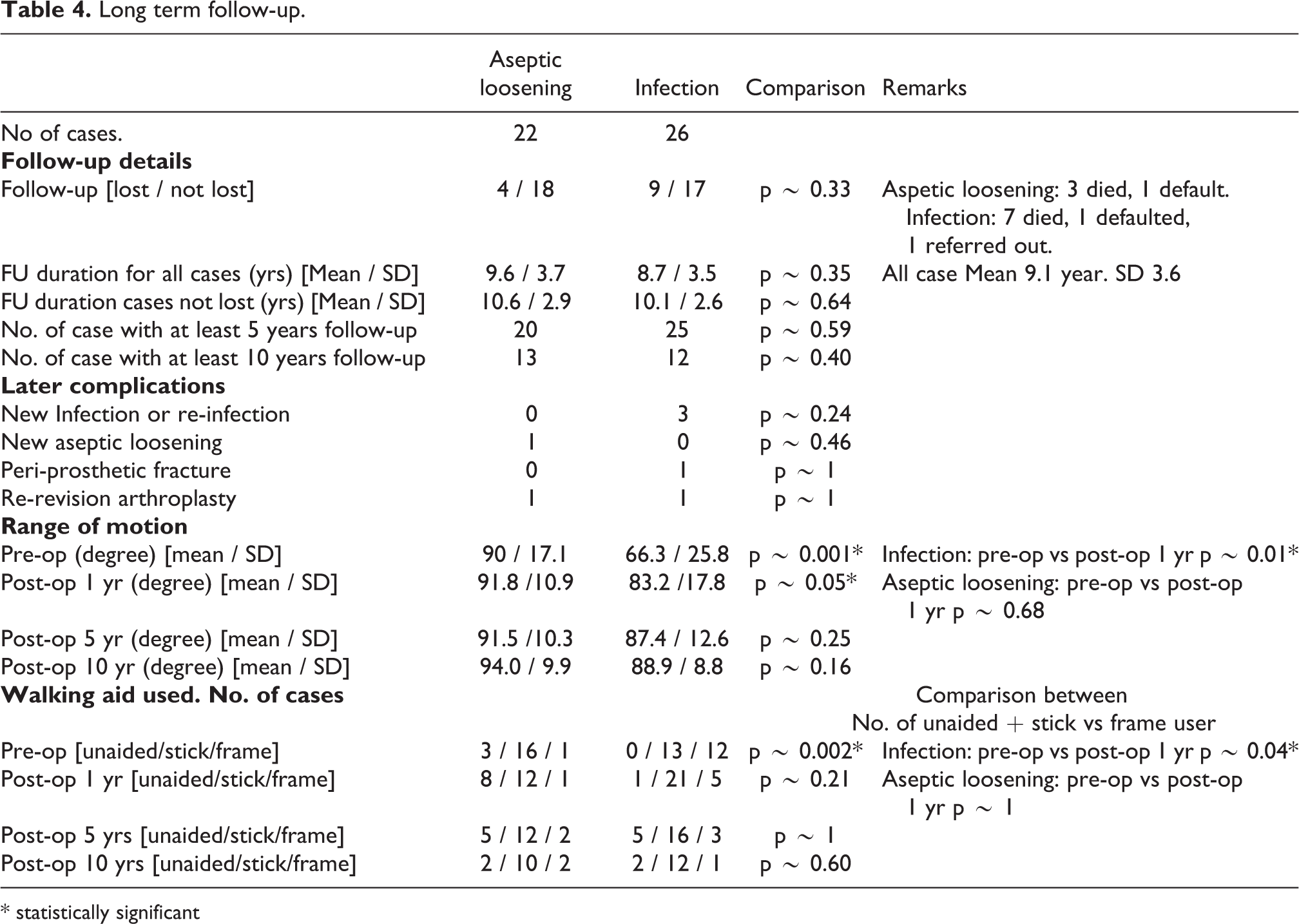
At 10 years follow-up, the rate of late complications was generally low. The overall survival of the revision arthroplasty in this series was 91% at 10 years, with aseptic loosening group at 93.3% and infection group 89.3% (Figure 1). In the infection group, three cases had new occurrence of infection. One was a severe early infection resulted in sepsis requiring above knee amputation of the limb at 6 months after the revision arthroplasty. Another had a late chronic infection after 9 years, requiring removal of implant replaced with antibiotic-load cement spacer, and repeated debridement with exchange of cement spacer due to questionable clearance of infection. One more with acute hematogenous infection 4 years after revision, which was treated operatively with arthrotomy, debridement and exchange of insert. One case had aseptic loosening after 7 years requiring re-revision. Other longer term issues including peri-prosthetic fracture and stiffness were low (Table 4).
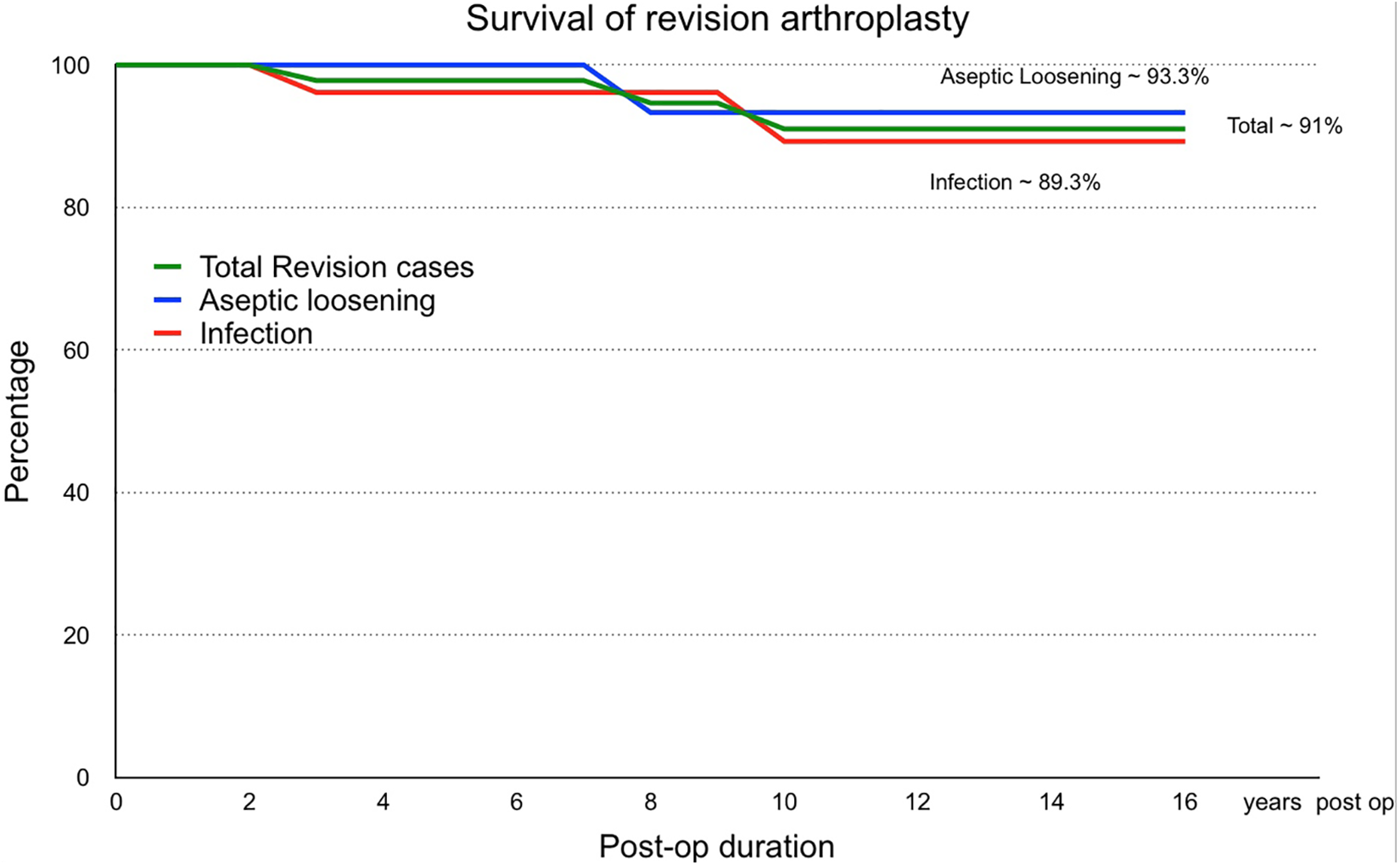
Survival of revision arthroplasty.
Long term follow-up.
* statistically significant
Range of motion (ROM) in the infection group pre-operatively (mean 66.3 degrees, SD 25.8 degrees) was significantly less than the aseptic loosening group (mean 90.0 degrees, SD 17.1 degrees)(p ∼ 0.001). At post-operation 1 year, the ROM of the infection group had largely improved to mean of 83.2 degrees (SD 17.8 degrees) (p ∼ 0.01). This could be attributed by the use of cement spacer in the treatment of infection prior to the revision arthroplasty. In contrast at 1 year after operation, the aseptic loosening group have a better range of motion 91.8 degrees (SD 10.9 degrees) compared to infection group (p ∼ 0.05), but not no significant improvement of ROM compared to pre-operation (p ∼ 0.68). There was no significant difference in ROM between the two groups by 5-years and 10-years follow-up (Table 4).
The use of walking aid was documented both in pre-operation, at post-operation 1 year, 5 years and 10 years. Pre-operatively, there was significantly more patients in the infection group requiring frame for mobilization compared to the aseptic loosening group (p ∼ 0.002). At 1 year post-operation, the use of walking frame significantly less patients in the infection group compared to their pre-operative mobility (p ∼ 0.04). Meanwhile, no significant difference in the use of aid at post-operative 1 year, 5 years and 10 years was noted between infection and aseptic loosening groups (Table 4).
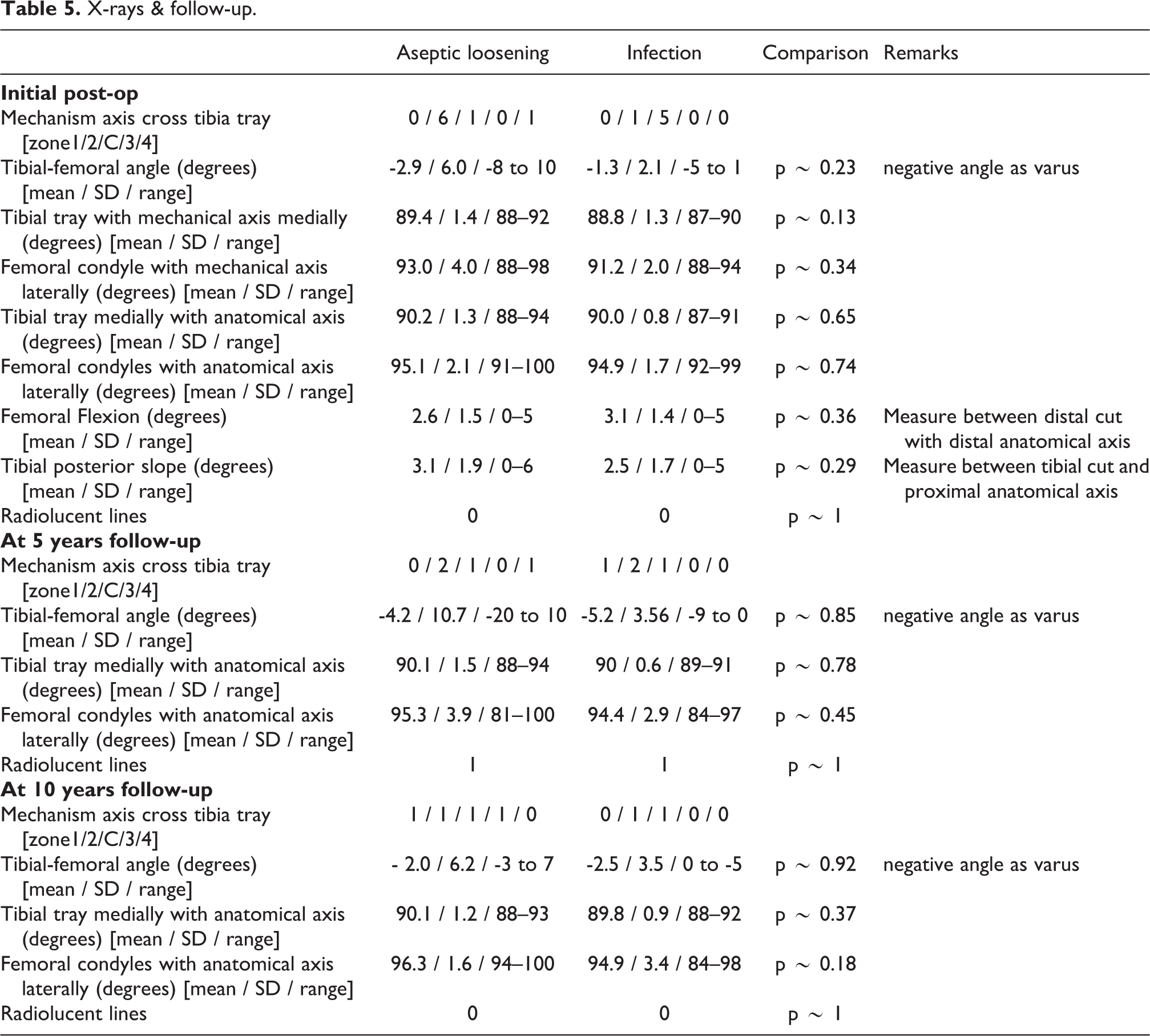
Comparison of X-rays between the infection and aseptic loosening groups at early post-operation, 5 years follow-up and 10 years follow-up showed not significant difference (Table 5).
X-rays & follow-up.
Discussion
In this study, there are significantly more cases among the infection group to require varus/valgus constrain implants (19 constrain, 7 Posterior-stabilized) compared to aseptic loosening group (7 constrain, 15 posterior stabilized) (p ∼ 0.008). This finding maybe attributed by the process of infection and repeated operative debridement resulting in medial–lateral laxity. Another postulated explanation could be due to bone lost in the infection or debridement processes. However, this postulation was not supported by the lack of significant difference in the used of augmentation between aseptic loosening and infection cases (Table 3).
Intra-operative extra exposure technique by quadriceps rectus snip was significantly more in infection cases (8 cases), than none in the aseptic loosening group (p ∼ 0.005). This could be attributed by a smaller pre-operative range of motion in the infection group. Abdel et al. 27 series stated approximately 10% of knee revision cases had quadriceps snips, demonstrated the use of snips were associated to lower range of motion pre-operatively, and fortunately no significant increase in complication compared with standard approach.
For complications of revision arthroplasty, van Rensch et al. 26 also reported 29% of case had complications with 15% requiring surgery, but there was no significant relation in complication rate to indication of arthroplasty. In this series, the number of late complications up till 10 years follow-up were generally low. Overall survival seems acceptable in this series at 10 years 91%, with aseptic loosening group 93.3% and infection group 89.3% (Figure 1). Kim and Park 25 series of 114 knees and mean follow-up of 7.2 years using the LCCK, had even claimed an extremely good survival of 96% at 19.2 years. Ro et al. 28 reported that septic revision was associated to poorer clinically outcome, though not an independent risk factor, but associated to independent risk factors including bone lost, repeated surgeries, and persistent infections (Table 1).
Range of motion (ROM) pre-operatively was smaller in the infection group (mean 66.3 degrees, SD 25.8 degrees) compared to the aseptic loosening group (mean 90.0 degrees, SD 17.1 degrees)(p ∼ 0.001). But at 1 year post-operation, infection group ROM had significantly improved (mean 83.2 degrees, SD 17.8 degrees) (p ∼ 0.01). The use of antibiotic loaded cement spacer in the treatment of infections was suggested to be the reason. On further follow-up, no more significant difference in ROM could be demonstrated between the two groups (Table 4). Contrarily, van Rensch et al. 26 reported significant improvement of ROM post-operatively for septic loosening group and malposition group at 2 years and 7.5 years follow-up.
As for use of walking aid, significantly more patients in the infection group required frame for mobilization pre-operatively compared to the aseptic loosening group (p ∼ 0.002). This could be attributed by the presence of antibiotic load cement spacer, repeated surgery for infection, prolong hospitalization prior to revision, and stiffness. This postulation are strengthened by the finding that the use of walking frame had significantly decreased patients in the infection group at 1 year post-operation (p ∼ 0.04). For mobility at longer term, there was no significant difference in the use of aid at post-operative 5 years and 10 years (Table 4). van Rensch et al. 26 too reported similar knee society function score around at 7.5 years of follow-up.
The indication of revision had varied across literatures. While Insall et al. 8 in the 1980s attributed the most common causes as malalignment, ligamental imbalance and patella complications, recent literatures in the likes of Postler et al., 13 Fahad Hossain et al., 15 Koh et al., 29 and Khan et al. 21 had identified infection and aseptic loosening as the main reasons knee arthroplasty revisions. In this study, the most common reason of revision arthroplasty was infection (26 cases, 54.2%), followed by aseptic loosening (22 cases, 45.8%). In line with the reported impression that majority of earlier revisions cases were due to infection, while a most of later revisions were due to aseptic loosening, this series revealed the duration of primary knee arthroplasty implanted in infection cases had a shorter duration of primary knee arthroplasty implantation (mean 33.2 months, SD 39.1 months) than to aseptic loosening group (mean 107.8 months, SD 50.8 months) (p < 0.0001).
In terms of age, Pedersen et al. 9 had noted that revision risk decrease with increasing age on the Danish Registry. Castagnini et al. 12 stated that younger patients had a high loosening rate. In this study, no significant difference was found data of initial primary knee arthroplasty between infection group and aseptic loosening in terms of age, gender, pre-morbid risk factors, duration of primary knee arthroplasty, duration of inpatient stay, and transfusion rate. Jämsen et al. 18 had stated risk factors for failures in primary arthroplasty included male gender, rheumatoid arthritis & fracture around the knee. Pitta et al. 7 had identified pre-operative risk factors for Total knee arthroplasty failure as history of drug abuse, deformity, usage of constrained implant, post-traumatic arthritis and younger age. This study had attempted to analyze some of these factors, along with length of stay, operative time in primary arthroplasty, and blood transfusion. However, we were unable to demonstrate statistically significant difference for such factors in relation with infection or revision. In another study from a center with similar demographics, a longer operative team in the initial arthroplasty is related to subsequent revision arthroplasty. 30
In a recent local study, Siu et al. 31 stated that gram positive Staphylococcus was most common infective organism. Similarly in this study, infective organism identified were predominately gram positive cocci (Table 2). Therefore, effective preventive measures and treatment with emphasize on prevention of infection by gram positive cocci.
Conclusion
Comparison between infection and aseptic loosening in revision knee arthroplasty revealed a higher proportion of use of varus/valgus constraints (p ∼ 0.008) and extensile surgical exposure in form of quadriceps snip (p ∼ 0.005) for infection cases. For longer term follow-up, the survival at 10 years seems acceptable at 91% overall (aseptic loosening 93.3%, infection 89.3%) and long term complications were generally low. While there were initial improvement for infection cases in terms of the range of motion (p ∼ 0.001) and use of walking aid (p ∼ 0.04) at post-operation one year, there are no differences between the two groups at 5 years and 10 years follow-up. Comparison between the two groups on other factors including demographics, initial arthroplasty, operative details, post-operative details and X-rays showed no statistically significant difference.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.