
Abstract
Introduction
Total knee arthroplasty (TKA) is the treatment of choice for patients with advanced osteoarthritis (OA) of the knee. As one of the most common and successful orthopedic procedures, the need for TKA continually increases each year with an estimated need for 3.5 million procedures by the year 2030. 1 Despite advances in technology and improved knowledge of anatomical biomechanics, as the number of annual TKAs increase, so too does the number of revision surgeries. National registries report revision rates as high as 12% depending on the observation period. 2
Several studies have analyzed failure mechanisms for TKA in the past. According to these studies, the modes of failure included loosening, infection, instability, periprosthetic fracture, arthrofibrosis, patella-related complications, polyethylene wear, malalignment or malposition, and pain.2–5 Most studies categorized revisions as early failure (within 2 years of the primary TKA) and late failure (greater than 2 years after the primary TKA).2–4 An earlier study found infection and instability to be the most common causes of early failure while polyethylene wear and aseptic loosening were the most common causes of late failure. 6 More recent studies have demonstrated somewhat contrasting results suggesting various reasons for the most common cause of failure at each stage including instability, malalignment, extensor mechanism dysfunction, and infection as early causes; and instability, malalignment, extensor mechanism dysfunction, infection, aseptic loosening, fracture, and polyethylene wear as late causes.2–5
Within the hip replacement literature, reasons for revision have been described to evolve over time as changes in surgical technique and prosthetic design have occurred. 7 As TKA surgical techniques and prosthesis evolve, reasons for failure requiring revision surgery may also change, and continual assessment is needed.
The purpose of this review was to evaluate the causes of early and late revision TKA at a single institution and to compare those reasons with historical data on the topic.
Materials and methods
This study was deemed institutional review board exempt by the institutional clinical research committee. A retrospective chart review of all patients undergoing TKA revision by 13 board-certified surgeons at a single institution was performed. The timeline for inclusion was between January 2, 2014, and October 16, 2020. Data were collected using an administrative database for patient demographics and comorbidities including age, sex, body mass index (BMI), and race. American Society of Anesthesiologists (ASA) score was used to quantify preoperative health status.
Medical and orthopedic comorbidities were recorded and listed in Table 2. The Centers for Medicare and Medicaid Services (CMS) Hierarchical condition category (HCC) score was used to quantify comorbid health status. HCC is a risk adjustment model initially designed to quantify risk and adjust payments for Medicare Advantage patients. HCC helps communicate patient complexity by assigning risk scores to patients based on diagnosis codes and demographic factors and is calculated for risk stratification of all patients in a payer-agnostic fashion at our institution. 8
Patient comorbidities.
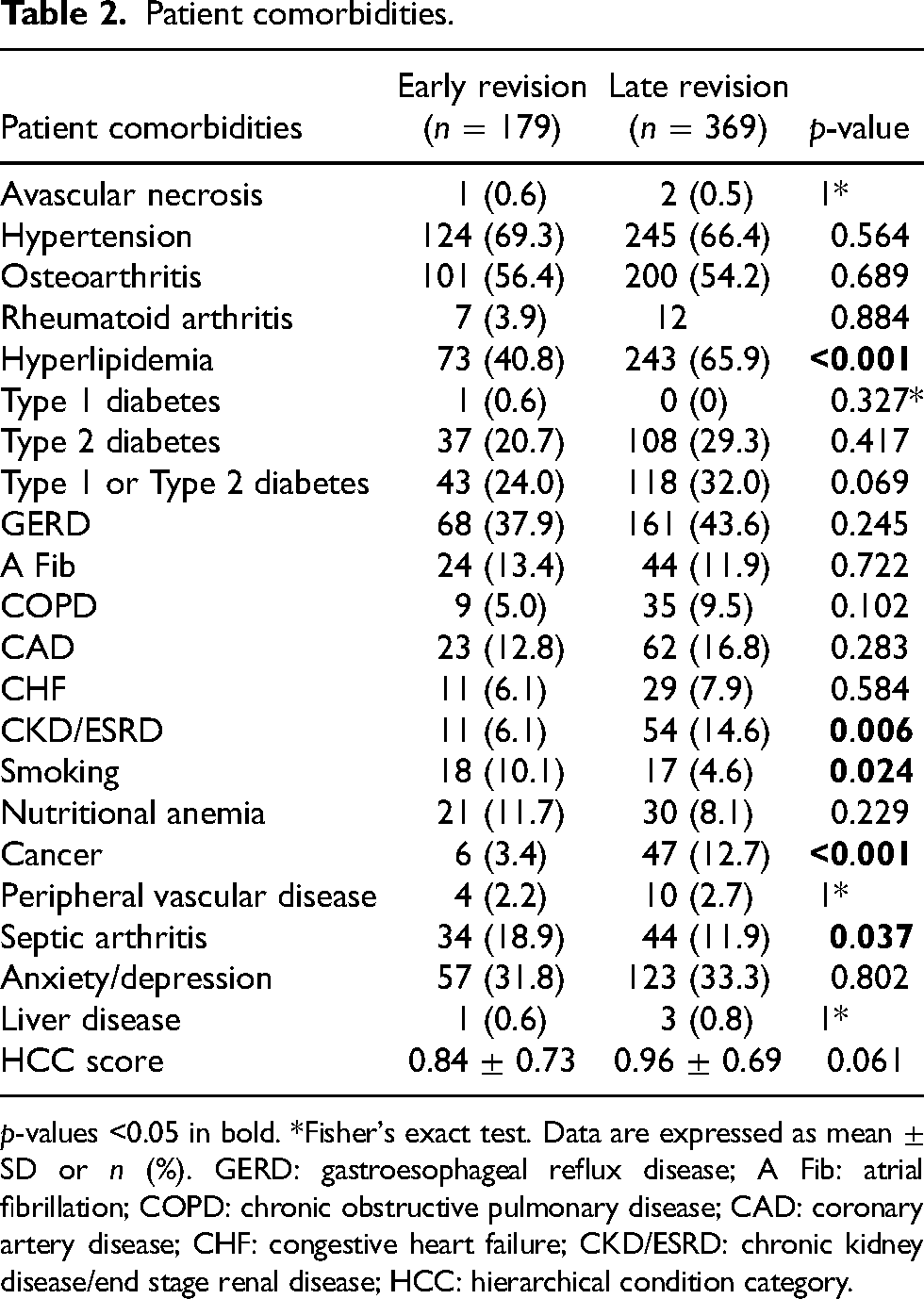
p-values <0.05 in bold. *Fisher's exact test. Data are expressed as mean ± SD or n (%). GERD: gastroesophageal reflux disease; A Fib: atrial fibrillation; COPD: chronic obstructive pulmonary disease; CAD: coronary artery disease; CHF: congestive heart failure; CKD/ESRD: chronic kidney disease/end stage renal disease; HCC: hierarchical condition category.
Perioperative protocol
All patients were cared for in a coordinated Joint Replacement Center and received education materials including written materials, preoperative medical evaluations, preoperative home exercise or outpatient physical therapy, and an education class for patients and their caregivers. Postoperatively, all patients were treated utilizing a multimodal pain management protocol which depending on patient factors included acetaminophen, oral NSAIDs, pregabalin, ketorolac, and oral opioid medications as needed. All TKA revision patients received assisted ambulation on the day of surgery when appropriate.
Study population
All patients included in this study underwent unilateral TKA revision between January 2, 2016, and October 16, 2020. Patients undergoing bilateral TKA or primary TKA were excluded from this study. A total of 548 patients met the inclusion criteria, 179 patients had a revision within the first two years following their TKA and 369 patients had a revision following two years after their TKA. There were 71 patients included in the study who had multiple revisions for a total of 155 cases and each revision was evaluated. Of these 71 patients, 55 had multiple revisions on the ipsilateral knee, while 16 had revisions of both knees.
Revision reason classification
Revision reasons were classified into nine separate categories based on information found in the patient charts, specifically the surgeon’s operative notes and consult notes. These categories include; infection (documented positive culture from joint space), loosening (documented tibial or femoral component loosening confirmed in operative note), arthrofibrosis (severe restriction in range of motion without evidence of other causes), instability (including malalignment, flexion instability, dislocation, and subluxation), periprosthetic fracture, patella-related complications (including patella fracture, avascular necrosis of patella, severe patellofemoral joint disease, quadriceps/patellar tendon rupture, patellar implant loosening, and patellar resurfacing—including unresurfaced patella conversion), polyethylene wear, pain (if no other causes were documented), and other (including wound dehiscence, recurrent hemarthrosis, severe heterotopic ossification, prepatellar bursitis, and wound drainage).
Study outcomes
Post-operative outcomes of interest included time from primary operation to revision, reason for revision, operation time, length of stay (measured in days and hours), discharge disposition, 30-day readmission, and 30-day emergency department returns. Readmissions were captured state-wide while return to emergency department were only captured for our institution.
Statistical analysis
Patients were grouped based on whether they had an early revision, within two years of TKA, or a late revision, more than two years after TKA. Statistical analyses were used to determine the impact of time to revision on postoperative outcomes for those who received a revision TKA. Univariate analysis including chi-square tests and two-sided independent samples t-tests were used to determine differences between groups. The Fisher's Exact test was performed when the assumptions of chi-square testing were not met. Multivariable logistic regression was performed to evaluate risk factors for re-revision. All statistical analyses were performed using R Studio (Version 1.4.1717© 2009–2021 RStudio, PBC). Statistical significance was assessed at p < 0.05.
Source of funding
This study did not receive any funding.
Results
Over the study period, 8013 primary TKAs were performed, and 548 patients underwent revision TKA, representing a revision burden of 6.4%. Of the 548 patients, 179 (32.7%) had an early TKA revision and 369 (67.3%) had a late TKA revision, making the burden of these revision types 2.1% and 4.3%, respectively. The primary TKA being revised was performed at an outside institution in 235 cases (43% of total revisions). Race was not significantly different as both early and late patients were approximately 73% white. Late revision patients on average were 5 years older than early patients (69.7 ± 9.6 vs. 64.6 ± 10.5, p < 0.001) and had a higher proportion of female patients (57.2% vs. 44.7%, p = 0.008). There was no difference in BMI and ASA between early and late revision patients (Table 1).
Population demographics.
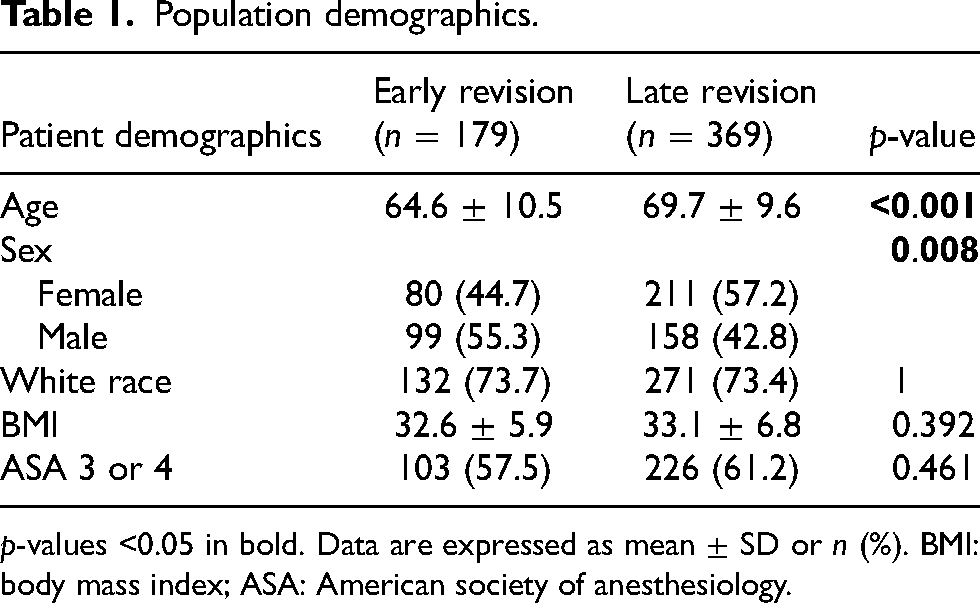
p-values <0.05 in bold. Data are expressed as mean ± SD or n (%). BMI: body mass index; ASA: American society of anesthesiology.
Across the study population, the most common reasons for revision were loosening (28.8%), infection (25.2%), and polyethylene wear (14.6%). The average time to revision for the early group was 0.87 ± 0.79 years (range, 0–2 years) and the average time to revision for the late group was 9.8 ± 5.8 years (range, 3–39 years; p < 0.001). The distribution of reasons for revision was significantly different between early and late revision patients (p < 0.001). In the early revision group, the most common reasons for revision were infection (31.3%), loosening (27.4%), and instability (10.1%). In the late revision group, the most common reasons for revision were (loosening (29.5%), infection (22.2%), and polyethylene wear (20.3%; Table 3).
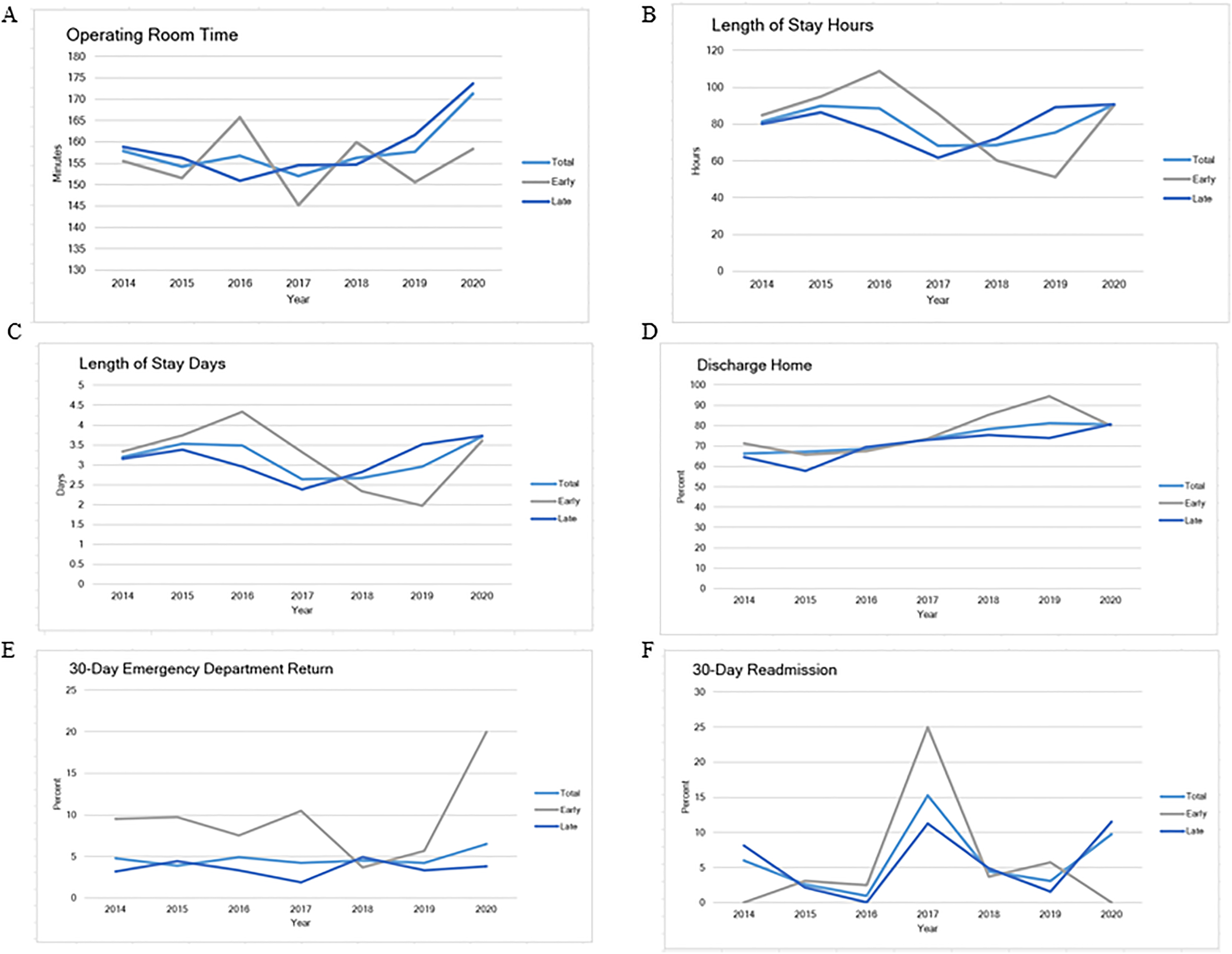
Over the study period, no statistically significant differences in hospital outcomes were observed between early and late revisions (Table 4). The average operating time was 156 min, and the average length of stay was 80 h or 3 days. Roughly 73% of patients were discharged home and 5% of patients were readmitted within 30 days and 5% returned to the emergency department within 30 days (Table 4). When evaluating trends in outcomes over time we found that operating room time, length of stay (days and hours), discharge home, and 30-day readmissions were stable over each year, however, 30-day ED returns were significantly different over time (p = 0.028; Figure 1(A) to (F)). Analysis on revision reasons in those who had 30-day ED returns demonstrated no single reason was at higher risk of return (p = 0.578; Table 5).
Percent of total early TKR by revision reason from 2014 to 2020.
Pre-op characteristics.
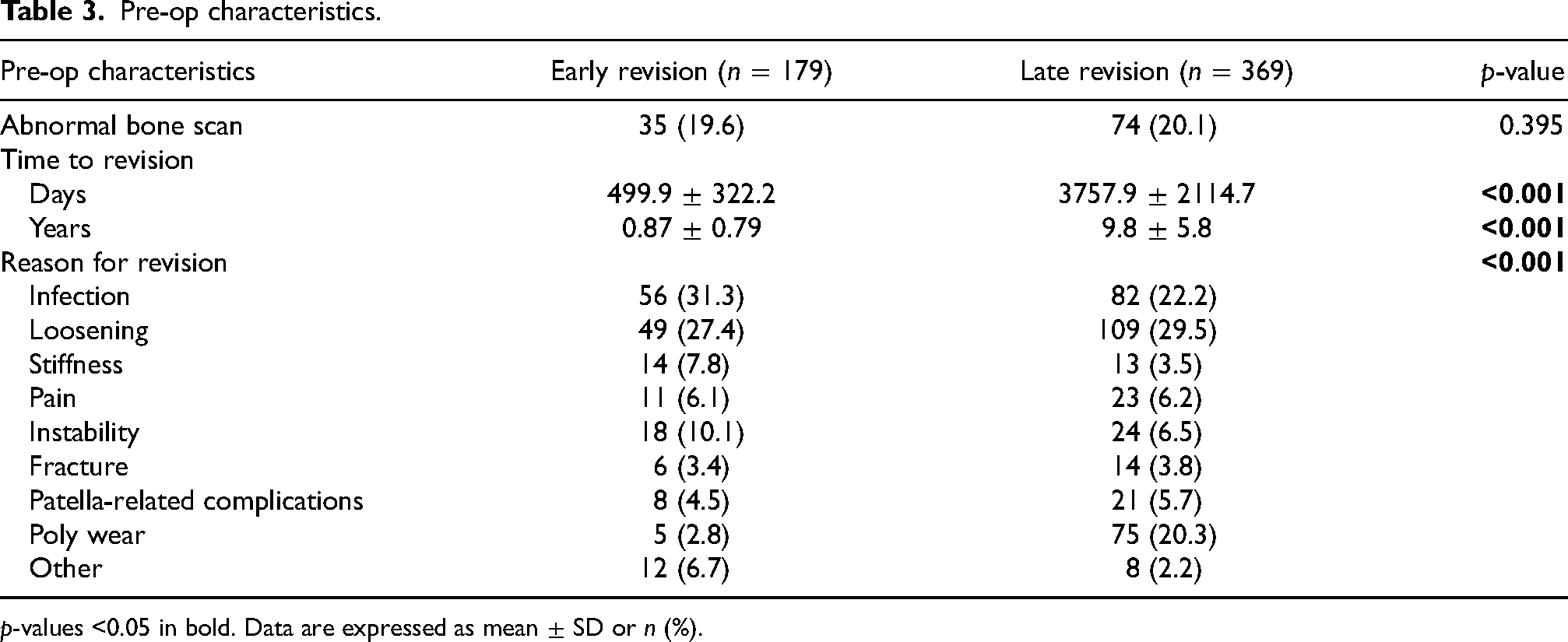
p-values <0.05 in bold. Data are expressed as mean ± SD or n (%).
Hospital outcomes.
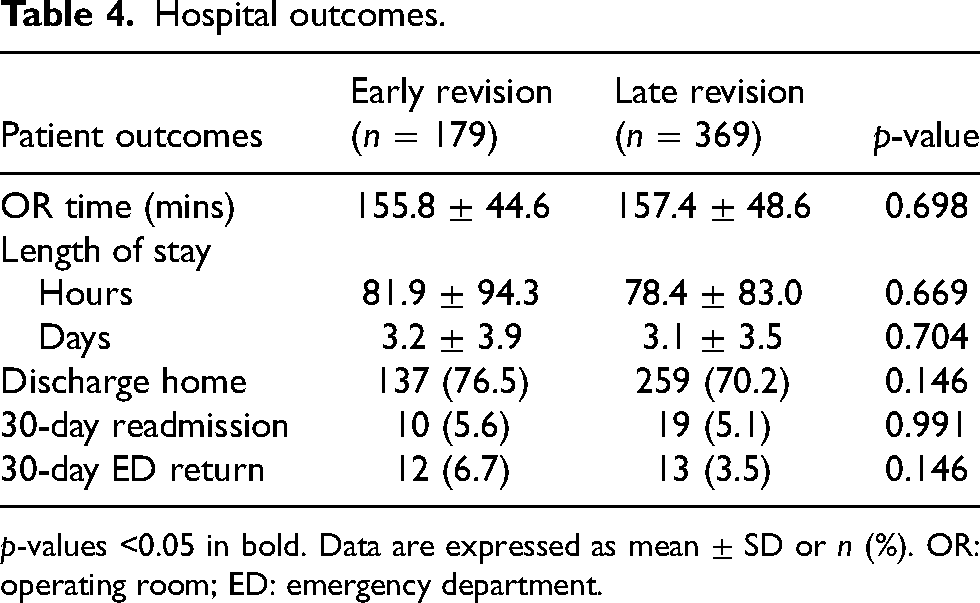
p-values <0.05 in bold. Data are expressed as mean ± SD or n (%). OR: operating room; ED: emergency department.
Regarding comorbidities, patients with late revisions were more likely to have hyperlipidemia (65.9% vs. 40.8%, p < 0.001), chronic kidney disease, or end-stage renal disease (CKD ESRD; 14.6% vs. 6.1%, p = 0.006), and cancer (12.7% vs. 3.4%, p < 0.001). Conversely, late revision patients had a lower incidence of smoking (4.6% vs. 10.1%, p = 0.024) and septic arthritis (11.9% vs. 18.9%, p = 0.037). There were no differences in avascular necrosis, hypertension, osteoarthritis, rheumatoid arthritis, type 1 or type 2 diabetes, gastroesophageal reflux disease (GERD), atrial fibrillation, chronic obstructive pulmonary disease (COPD), coronary artery disease (CAD), congestive heart failure (CHF), nutritional anemia peripheral vascular disease, anxiety/depression, liver disease, and HCC score (Table 2).
Reason for revision of early revisions with or without 30-day ED returns or reemissions.
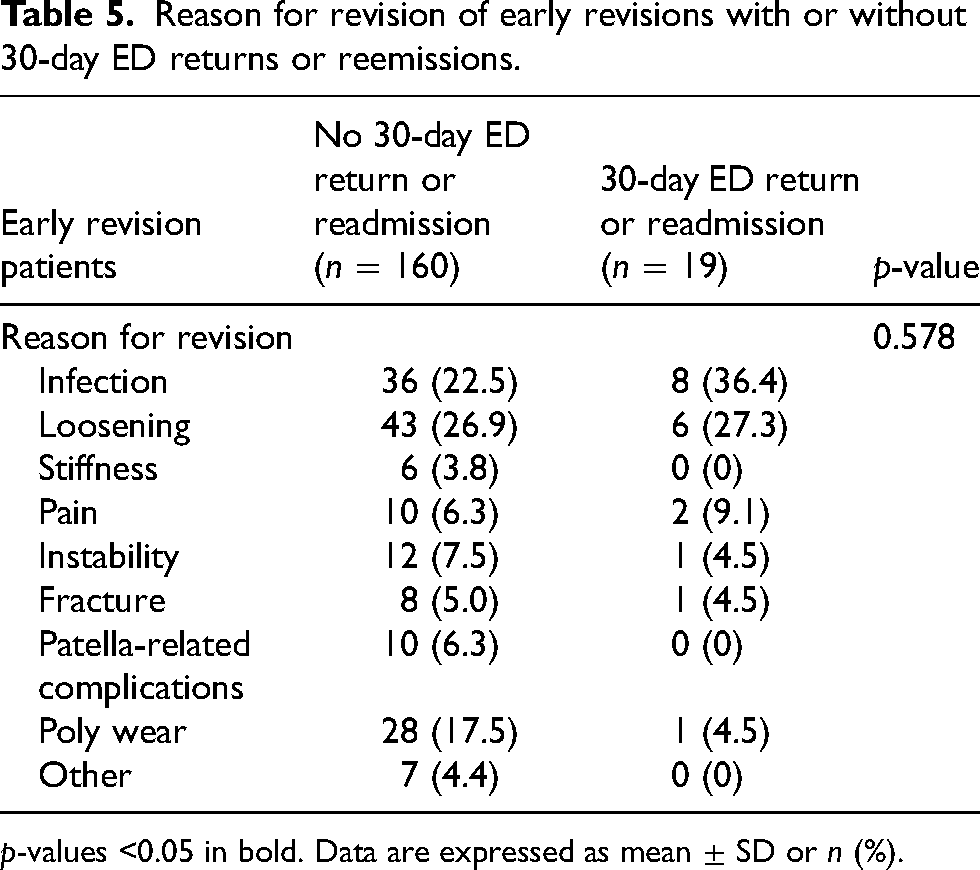
p-values <0.05 in bold. Data are expressed as mean ± SD or n (%).
Subgroup analyses were conducted to examine reasons for revision in smokers and risk factors for multiple revisions on the ipsilateral knee. Our results indicated that smoking did not increase the risk of any one type of revision reason although, smokers were more likely to have early than late revision for infection (41.7% vs. 30.4%) and more likely to have late than early revision for loosening (30.4% vs. 16.7%; Table 6). In the second subgroup analysis, seven independent risk factors for repeat revision of the ipsilateral knee were identified after controlling for other comorbidities and demographics. These included type 1 or type 2 diabetes (OR = 3.336, p = 0.002), GERD (OR = 2.203, p = 0.037), atrial fibrillation (OR = 2.984, p = 0.023), smoking (OR = 4.135, p = 0.007), cancer (OR = 5.932, p < 0.001), septic arthritis (OR = 5.852, p < 0.001), and anxiety/depression (OR = 2.814, p = 0.006; Table 7).
Pre-op characteristics and reasons for early versus late revision in smokers.
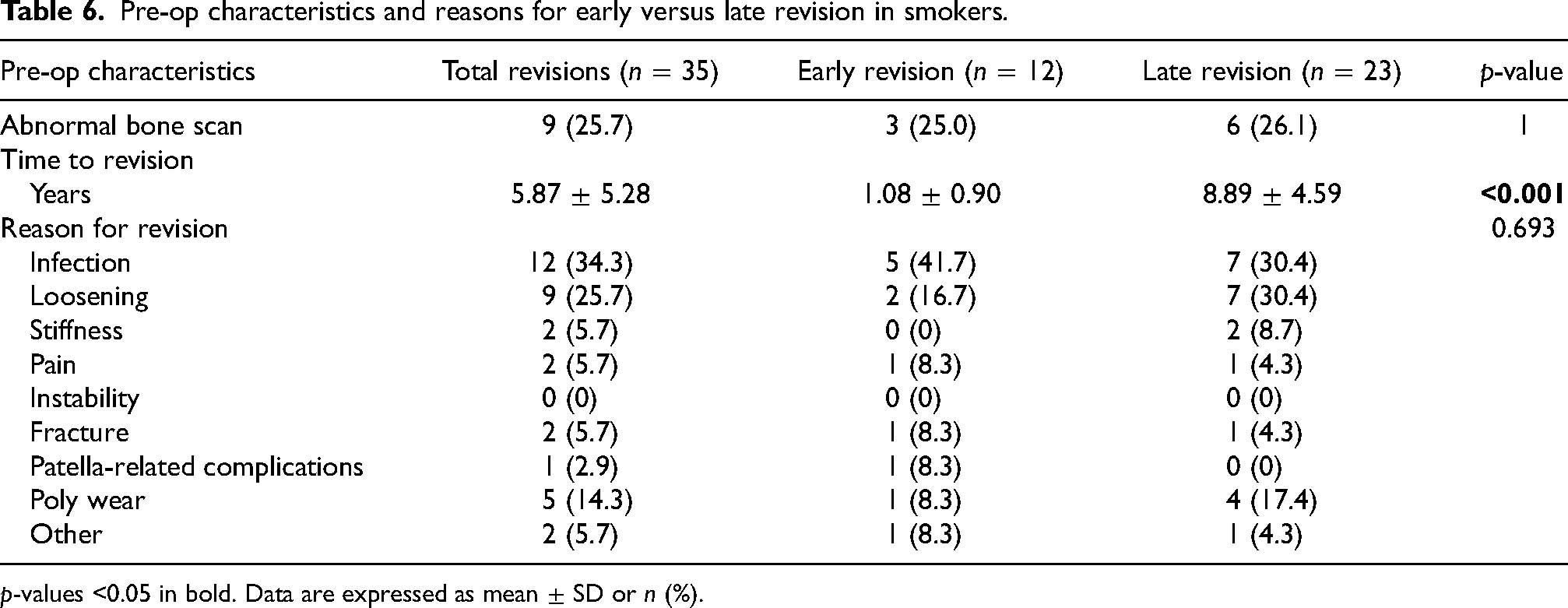
p-values <0.05 in bold. Data are expressed as mean ± SD or n (%).
Risk factors for ipsilateral re-revision.
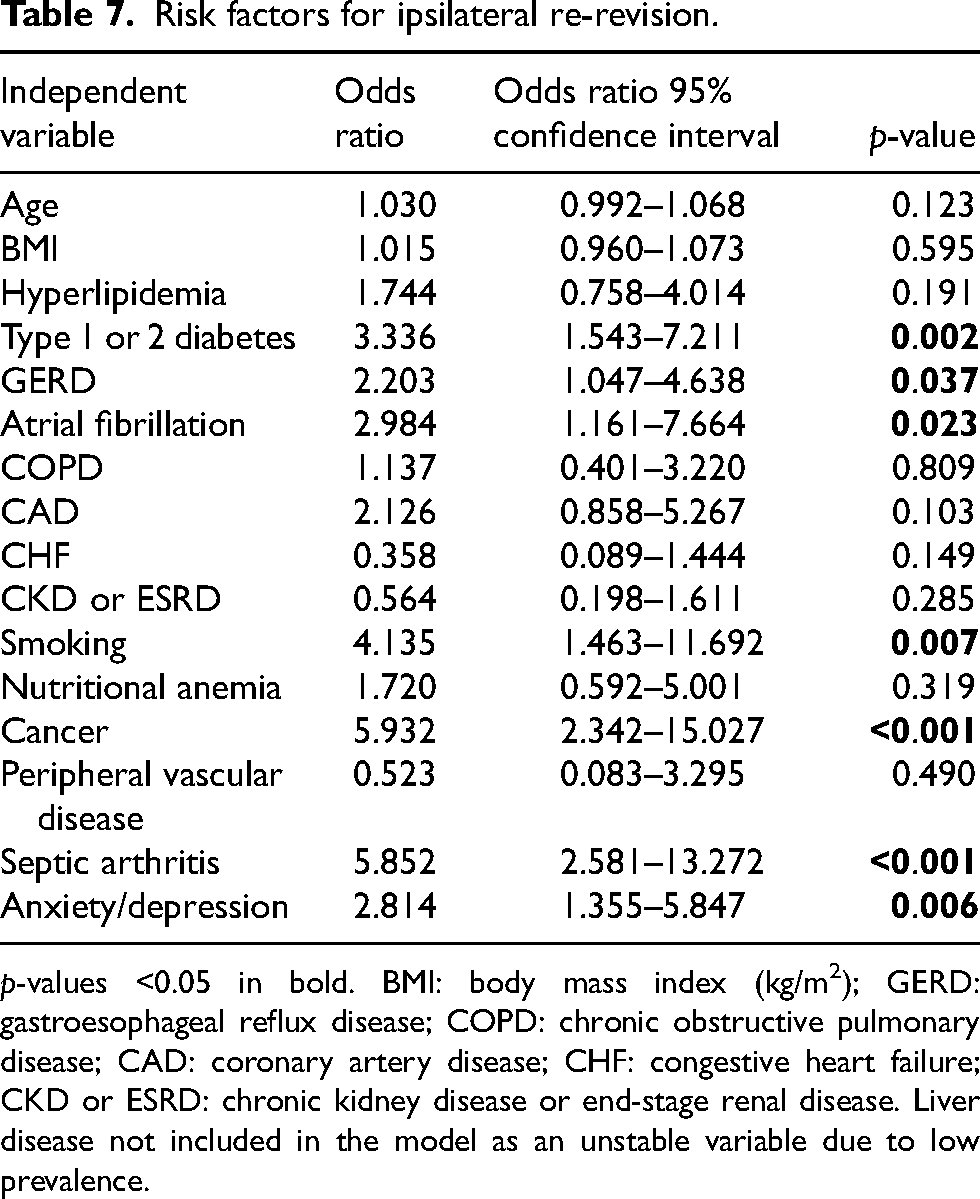
p-values <0.05 in bold. BMI: body mass index (kg/m2); GERD: gastroesophageal reflux disease; COPD: chronic obstructive pulmonary disease; CAD: coronary artery disease; CHF: congestive heart failure; CKD or ESRD: chronic kidney disease or end-stage renal disease. Liver disease not included in the model as an unstable variable due to low prevalence.
Discussion
Overall, revision rates after primary TKA are low with a 10-year revision risk of approximately 5% although the absolute number of revisions are increasing due to the growing number of TKAs performed annually. 3 In this study, TKA failure was broken down into early and late failure. Of 548 patients, 179 (32.7%) had revision due to early failure while 369 (67.3%) had revision due to late failure. On average, early failures occurred at roughly 1 year while late failures occurred at roughly 10 years. We found the top causes of early failure were infection, loosening, and instability while the top causes of late failure were loosening, infection (22.2%), and polyethylene wear. Patients with earlier failure were more likely to be smokers, perhaps related to the increase risk of infection in this group. The role of infection is not disputed as a leading cause of revision; however, other causes have less consistency as a leading contributor across the literature.
At our institution, the revision burden, defined as the number of revisions divided by the total number of revision and primary arthroplasties performed over a period of time, 9 was 6.4% over the study period. While revision burden is a crude measure that can be influenced by multiple factors, it is commonly used as benchmark that can be compared across institutions and registries. In 2021, an overall TKA revision burden of 9.2% was reported in the American Joint Replacement Registry, with a 2020 burden of 7.3% reported in the Australian Orthopaedic Association National Joint Registry. 9 While the current study does not aim to evaluate TKA survivorship, the finding that our observed revision burden is similar to those reported in national registries provides context for our results and suggests they may serve as valid external benchmarks for other institutions.
Our findings describing reasons for revision differ somewhat from the previously published literature. Mathis et al. reported that instability and patellofemoral and/or extensor mechanism insufficiency were the most common causes of both early and late failure. 2 Although we found instability to be the third most common cause of early failure, only 6.5% of patients had late failure due to instability. Additionally, patellofemoral and/or extensor mechanism insufficiency were combined into the “Patellar Complications” category which only accounted for 4.5% and 5.7% of the early and late failures respectively. This difference may be related to the fact that 86% of the patients evaluated by Mathis et al. were referred to a specialized knee center after primary TKA was performed at another institution. 2 Meanwhile, 57% of the patients included in this study had their primary TKA performed at our institution and because of this, our results may be more reflective of the revision trends of the general population. In 2002, Sharkey et al. found infection (25.4%) and instability (21.2%) to be the most common causes of early failure while polyethylene wear (44.4%) and loosening (34.4%) were the most common causes of late failure. 6 However, in their 2014 update, Sharkey et al. found infection (early: 37.6%; late: 21.9%) and loosening (early: 22.8%; late: 51.4%) to be the most common causes of both early and late failure with the incidence of polyethylene wear significantly reduced at 4.3% of late failures. 4 The difference regarding polyethylene wear may be associated with the advancements seen in second-generation polyethylene technology. 10 This finding is different from our own as we found polyethylene wear to be responsible for 20.3% of late failures. Additionally, Thiele et al. reported polyethylene wear to be responsible for 18.5% of late failures in their 2015 study where they further broke down “time to failure” into three categories; early (<1 year postoperative), intermediate (1–3 years postoperative), and late (>3 years postoperative). 5 Similar to our study, Thiele et al. reported infection (26.8) and instability (23.9%) as the most common causes of early failure, although they found malalignment (18.3%) was the third most common cause whereas we demonstrated loosening to be in the top three. 5 In a more recent study, Postler et al. found infection to be the most frequent cause of revision overall with 51.3% of early revisions and 26.8% of late revisions associated with this cause. 3 Loosening, arthrofibrosis, and extensor mechanism injury followed infection as the top cause of revision accounting for 9.2% of revisions each. Regarding late revisions, loosening, and periprosthetic fracture accounted for 23.7% and 18.8%, respectively. 3 Although there is variation across the published literature, there is a common theme that infection is one of the overall leading causes of revision.
The differences within the literature regarding revision causes may be related to the differences in the patient populations studied as many studies involved cases that were referred to the institution because of their complexity. In a retrospective case–control study, Blanco et al. demonstrated risk factors such as obesity, diabetes, and ASA grade were statistically significant related to TKA periprosthetic joint infection (PJI). 11 Because obesity is a modifiable risk factor, and diabetic control can be improved, it may be possible to mitigate these risks and potentially reduce the rate of PJI. In our study, we found a higher incidence of smoking in those that had early revision. Because infection was the leading cause of early revision, it is likely that the smoking status of these patients played a role in their infected joint as smokers have a 1.8 times higher risk of infection in the first year after total joint surgery. 12 Blanco et al. also found that requirement of blood transfusion after TKA was also statistically significant related to PJI. 11 Although transfusion rates for patients undergoing TKA are relatively low around 3.2%, this is still a factor that can be improved. 13 Over the years, transfusion rates have been reduced through more stringent transfusion guidelines, enhanced protocols, and advancements in pharmaceuticals and bleeding control devices. 13 Other surgical factors associated with PJI are operative time and tourniquet time, with longer times increasing the risk. 11 Overall, these are areas that deserve more attention as they are factors that could be better controlled which would ultimately reduce the risk of PJI.
Loosening was another leading cause of revision across multiple sources and as such, it is important to focus on ways to reduce the incidence of loosening to decrease the overall incidence of revisions in the future. A number of factors related to component loosening have been described in the literature including but not limited to implant design, type of cement, cement technique, coronal alignment, and polyethylene design.14–18 Each of these factors are somewhat modifiable and with improvements in technology and technique it is possible loosening due to these causes could be avoided. Van Hamersveld et al. demonstrated loosening occurred more often in cementless implants without hydroxyapatite coating or highly porous metal. 18 When considering cement, the use of high-viscosity cement was associated with an increased risk of revision due to loosening compared to low-viscosity cement. 14 However, the use of cement, in general, does not seem to play a role as Pacoret et al. demonstrated no difference in tibial component survival rate between cemented and cementless fixation with a minimum 5-year postoperative follow-up. 17 With regard to coronal alignment, conflicting conclusions have been reached. In a study of 1151 knees with an average follow-up of 8 ± 4 years, Lee et al. concluded that varus malalignment greater than 3 degrees from neutral mechanical alignment was associated with greater rates of aseptic loosening. 16 Conversely, Parratte et al. evaluated 15-year survivorship of 398 primary TKAs and found that a postoperative mechanical axis of 0° ± 3° did not improve implant survival, thus calling the dichotomous definition of aligned versus malaligned into question. 19 Lastly, patients receiving highly cross-linked polyethylene were less likely to require revision due to loosening when compared to those receiving conventional polyethylene. 15
Trends over time for each perioperative outcome were also evaluated and demonstrated stable outcomes over time with the exception of 30-day ED return which was significantly different. Considering this, we evaluated reasons for the revision of ED returns but these results showed there was no specific revision reason that increased the risk of returns. Given the variability in ED return rates and lack of a specific identifiable risk factor for ED returns, it is critical that patients undergoing higher-risk revision procedures be provided with comprehensive education and access to resources such as nurse navigators to reduce potentially avoidable ED returns.
This study is not without limitations. First, we utilized a large timeframe of inclusion, which may have introduced inconsistencies as the implant designs, materials, and surgical techniques used all likely had improvements introduced over time. Second, there were 71 patients included in the study who had multiple revisions for a total of 155 cases and each revision was evaluated. These cases may have impacted our results. In our subgroup analysis, we identified seven independent risk factors of ipsilateral re-revision, some of which may be modifiable with medical and lifestyle management. This interesting finding suggests further study into the efficacy of programs aimed at optimizing patients to mitigate risk of re-revision is warranted. Next, the reasons for revision were determined via review of the operative notes so there may have been inconsistencies how surgeons classified failure. Lastly, infection in our study was defined by positive cultures in the joint space not by utilization of additional standardized measures such as the Musculoskeletal Infection Society criteria. A strength of this study is that 57% of patients had a revision where the primary surgery was done at our institution so full details of both operations were available which differs from other studies who had a majority of their revisions referred from other institutions.2,4,5
Conclusion
This study demonstrated the main causes for revision at a high-volume orthopedic joint replacement center. The most common reasons for revision were infection, loosening, instability, and polyethylene wear. Early revisions were more likely to be related to infection, while later revisions were more likely to be for loosening. These results suggest that the reasons for revision are constantly evolving and need to be reassessed periodically to improve patient outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.