
Abstract
Background:
Daily changes in the shape and size of the residual limb affect prosthetic socket fit. Prosthetic socks are often added or removed to manage changes in limb volume. Little has been published about how persons with transtibial amputations use socks to manage diurnal changes in volume and comfort.
Objectives:
To investigate prosthetic sock use with a customized, self-report questionnaire.
Study design:
Cross-sectional survey.
Methods:
Persons with transtibial amputation reported number, thickness, and timing of socks used over a 14-day period.
Results:
Data from 23 subjects (16 males and 7 females) were included. On average, socks were changed less than once per day (0.6/day) and ply increased over the day (4.8–5.5 ply). Subjects wore prostheses significantly longer (15.0–14.1 h, p = 0.02) and changed socks significantly more often (0.6/day–0.4/day, p = 0.03) on weekdays compared to weekends. Participants were also divided into two subgroups: those who used socks to manage limb volume and those who used socks for socket comfort. Sock use did not differ (p > 0.05) between subgroups.
Conclusions:
Sock changes are infrequent among persons with lower limb loss. Initial, verbal reports of sock use were often inconsistent with data measured by logs. Tools (e.g. sock logs or objective instruments) to better understand sock-use habits among persons with limb loss are needed.
Clinical relevance
Knowledge of prosthetic patients’ sock use may help practitioners enhance volume management strategies or troubleshoot fitting issues. Results showed that subjects generally added socks to account for volume loss, and end-of-day sock thickness frequently exceeded 5 ply. Use of sock logs in clinical practice may facilitate improved residual limb health.
Background
Fluctuations in the circumference and volume of a residual limb are common for persons with transtibial (below knee) amputation. 1 Changes in size and shape of the limb affect prosthetic socket fit and can cause discomfort, gait instability, and skin issues for a prosthetic user. 2 Although the most substantial changes in the size and shape of a residual limb occur during the first 4–6 months and small changes may continue for up to 12–18 months after amputation, 3 diurnal (i.e. daily) volume changes occur even after this postoperative recovery period. 4 The degree of diurnal volume fluctuation varies by individual,5,6 but factors such as socket fit, suspension method, and physical activity are believed to influence changes in the residual limb volume over the course of a day. 7
To maintain an appropriate fit between a changing residual limb and rigid prosthetic socket, prosthetic users are encouraged to adopt one or more limb volume management strategies. There are a range of options available to prosthetic users, including the use of liners, socks, pads, and adjustable sockets. 4 Adding or removing prosthetic socks over the course of a day is a common and convenient means to accommodate for changes in limb volume. 8 Prosthetic socks are available in a variety of sizes, thicknesses, and materials. Socks can also be worn individually or stacked to achieve a desired thickness. Socks are relatively inexpensive, easy to maintain, and allow a wearer to add or remove them, as necessary, to compensate for volume loss over the course of a day. 4
Although prosthetic socks are commonly prescribed to persons with transtibial amputation, practitioners have an incomplete understanding about when and how socks are used by their patients. For example, some patients may don and doff prosthetic socks throughout the day to manage residual limb volume, while others may don socks with the prosthesis to enhance comfort, but not change socks over the course of a day. Patients may be able to generally inform a practitioner about their typical sock use, but specific details may be challenging for patients to recall. Practitioners can also inspect patients’ residual limbs for evidence of prosthetic sock use or misuse (e.g. redness, edema, skin breakdown), but the exact causes of observed issues may be challenging to diagnose.9,10 Information about how often different prosthetic users change socks, changes in number and thickness of socks worn, and the times of day in which socks are changed could enhance the limb volume management process and aide in troubleshooting poorly fitting sockets. Such information is presently unavailable to practitioners.
The purpose of this study was to quantify frequency and timing of sock changes and thicknesses of socks worn by persons with transtibial amputation. Of interest was how sock use differs between those who report use of socks for volume management (i.e. adding and removing socks to accommodate residual limb volume changes throughout the day) and those who report use of socks for comfort (i.e. donning socks with the prosthesis, but not changing socks throughout the day). The investigators hypothesized that, in general, prosthetic limb users who used socks for comfort would initially don relatively thin socks (e.g. less than 5 total sock ply) and not change socks throughout the day. The investigators hypothesized that those who used prosthetic socks to manage their residual limb volume fluctuations would also initially don thin socks, but would add socks over the course of the day. It was also believed that adding socks would regularly produce a total sock thickness in excess of 5 ply by the end of the day. Confirmation of these hypotheses would suggest that sock use is consistent with users’ self-report and that persons with transtibial amputation who experience substantial diurnal residual limb volume loss accommodate volume loss through the addition of one or more socks over the course of the day.
Methods
Subjects
Persons with transtibial amputation(s) were recruited for participation in the study. Candidate subjects were identified by posting flyers at local prosthetic offices, hospitals, and support group meeting sites. Inclusion criteria included 18 years of age or older, unilateral or bilateral transtibial amputation, date of amputation(s) at least 1 year prior to participation in the study, Medicare Functional Classification Level (K-level) 2 or higher 11 use of a prosthesis (or prostheses) for at least 4 h per day, and routine use of prosthetic socks for comfort or residual limb volume management. Time of amputation was set to a minimum of 12 months to mitigate the effects of large residual limb volume changes that typically occur after amputation surgery. Although minor changes in limb shape and size may take place for up to 18 months after amputation, the limb typically stabilizes in the first 6 months after surgery. 3 As recent studies have shown that residual limb volume change may be associated with activity, 12 persons classified as limited or unlimited community ambulators (i.e. K-level 2 or higher) were sought for inclusion in this study. A minimum of 4 h of typical daily prosthesis use was chosen to identify “regular” prosthesis wearers. We believed that regular users would likely experience different limb volume changes (and therefore use different forms of volume management) than occasional prosthesis users. Exclusion criteria included existing residual limb skin issues (e.g. skin breakdown or sores) that would prohibit daily use of a prosthesis for a period of 2 weeks.
Protocol
Interested candidates were screened by telephone to ascertain whether they met study selection criteria. Candidates were then asked to attend an in-person session to confirm candidacy and provide study investigators with basic demographic information (e.g. age, gender, height, weight, etc.). Subjects were interviewed and assessed by the study prosthetist to determine K-level, etiology of amputation, prosthetic componentry (i.e. socket style, suspension method, liner, and foot type), residual limb length, sock use, assistive device use, and socket comfort score (SCS). 13 Assignment of K-level was made through assessment of subjects’ self-report of typical activities and use of their prostheses, which is consistent with clinical practices. Residual limb length was measured to the nearest 1.0 mm using a standard clinical measuring tape. For reporting purposes, residual limb length was calculated as a percentage of the anatomical segment using the subjects’ height and standardized anthropometric tables. 14 Subjects were categorized into two subgroups based on their reported style of sock use. Subjects were each asked “do you add or change socks throughout the day?” Those who responded “yes” were categorized as subjects who used socks to manage daily residual limb volume (subgroup 1) and those who responded “no” were classified as subjects who used socks primarily for socket comfort (subgroup 2).
Subjects were provided with a sock log (described below) and a return envelope by the study investigators. Subjects were asked to read the instructions and provided an opportunity to ask questions about how to complete the log. Subjects were asked to complete the log daily for a period of 2 weeks (i.e. 14 days). Two weeks was selected as the investigators believed it was long enough to measure habitual weekly patterns in sock use, but not so long as it would place undue burden on the study subjects. Subjects with bilateral amputations were asked to complete a sock log for their dominant limb.
All study procedures were approved by a University of Washington Human Subjects Division Institutional Review Board. Informed consent was obtained from all subjects prior to their participation in the study.
Survey
A self-report “sock log” (Figure 1) was developed by the study investigators to gather information about subjects’ daily sock use. The sock log included instructions, an example that described how to complete the log, and 14 daily surveys. Each survey solicited the time when the prosthesis was donned, times when a sock change was made during the day, and the time when the prosthesis was doffed. At each time (e.g. donning, sock change, or doffing), the respondent was asked to provide the number and ply of socks being currently worn. Socks were described by standard plies (i.e. 1, 3, and 5) as well as by relative thickness (i.e. thin, medium, or thick). Subjects were verbally instructed to write in additional comments if the provided options did not match their situation (e.g. if the subject donned a ply other than what was specified in the form) or additional fields were needed (e.g. if more than three daily sock changes were performed). Finally, subjects were asked to identify whether the prosthesis was not worn so as to discriminate days with no sock use from an incomplete survey.
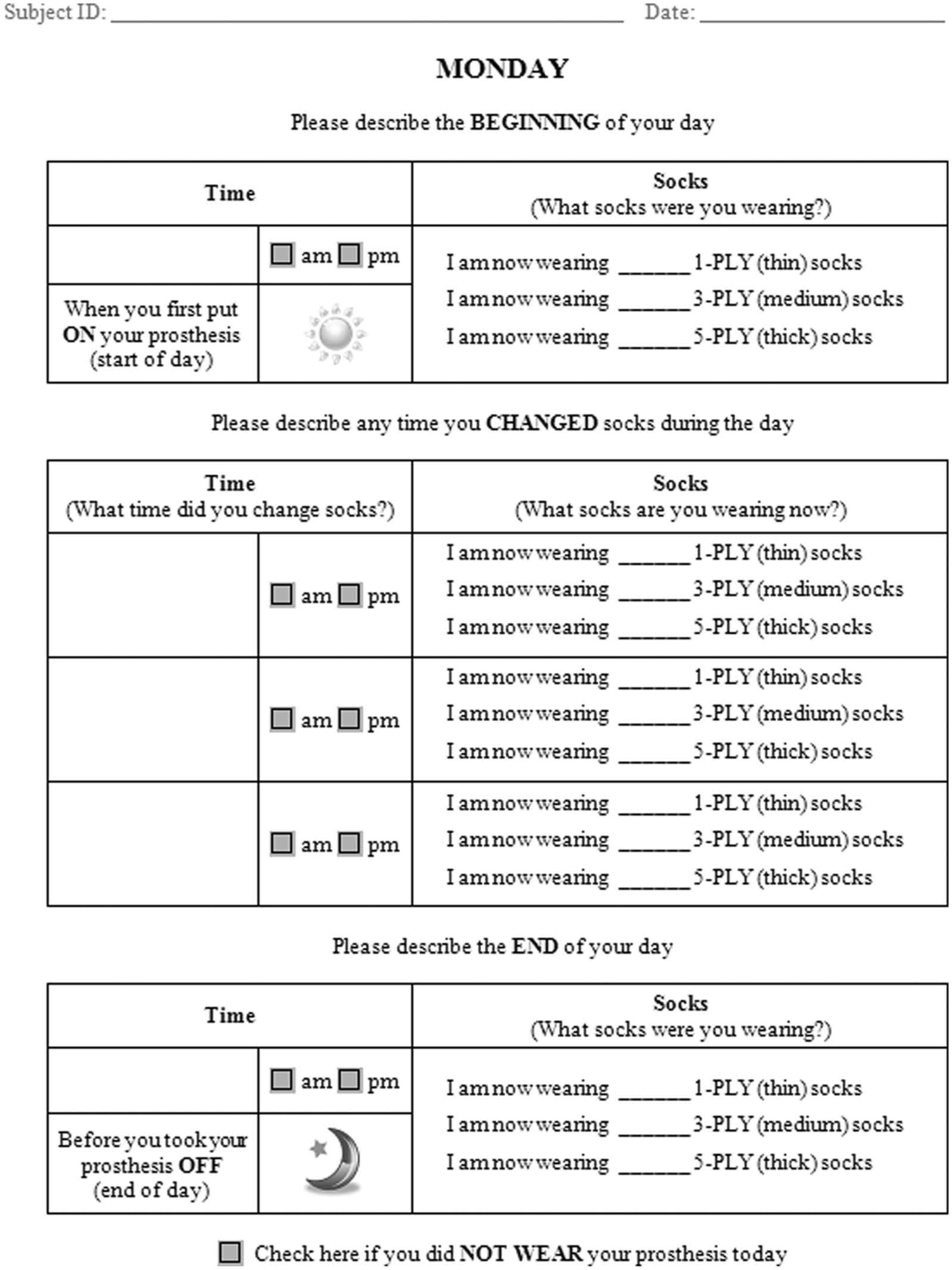
Self-report “sock log.” Two-week surveys were provided to all study subjects (1 day of the survey is shown). Instructions provided on a separate page informed subjects that they were free to use any of their usual prosthetic socks and to add/remove them throughout the day, as needed. An example of a completed survey (1 day) was also provided.
Analysis
Subjects’ survey responses were used to derive daily outcome variables (Table 1). Outcome variables were computed over a standardized, 24-h “day” that was individually determined for each subject. All 14 “days” in the study period were set to begin at the earliest donning time reported by the subject. Standardized periods were allowed to vary across subjects to account for variations in routines.
Descriptions of study outcome variables. Sock log data were used to calculate outcomes related to wear times, sock plies, and sock changes.
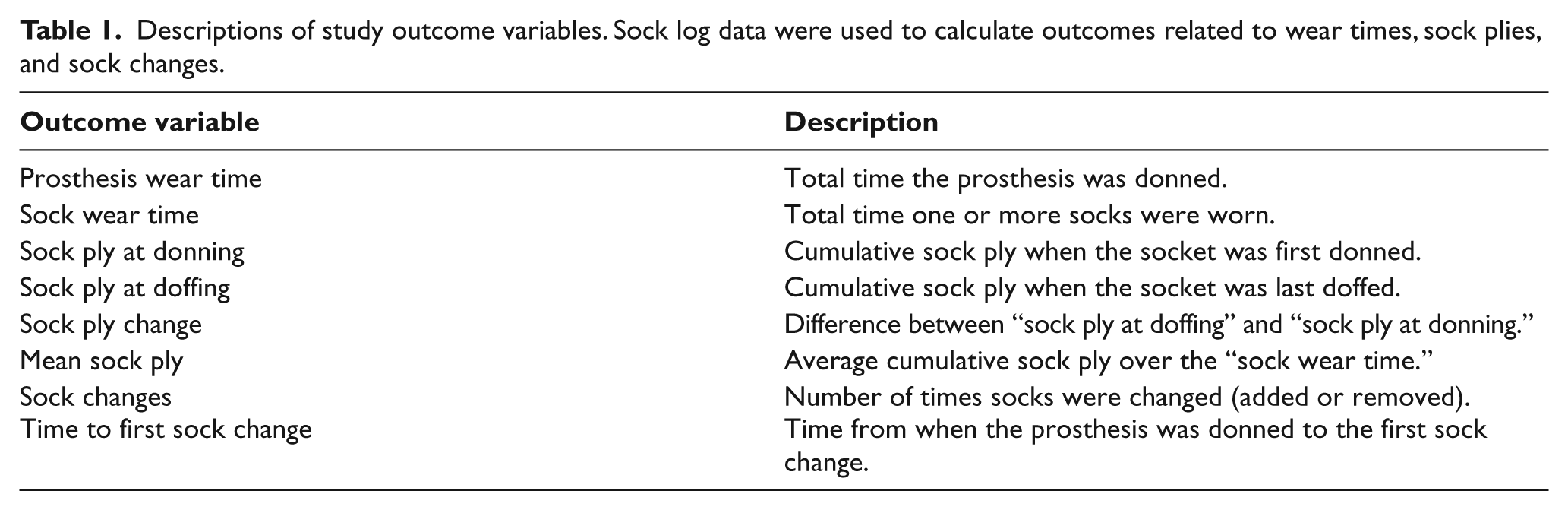
Daily outcomes variables for each subject were tabulated and averaged over three different time periods—weeks (i.e. Monday to Sunday), weekdays (i.e. Monday to Friday), and weekends (i.e. Saturday and Sunday). Data were also averaged across all subjects and across subgroups.
Descriptive analysis included calculation of minimums, maximums, and means of all variables. Data were assessed for normality using the Shapiro–Wilk test. Data were determined to be nonnormally distributed. Therefore, differences between subgroups were assessed with a Fisher Exact Test (categorical data) or Mann–Whitney U Test (continuous data). Differences in outcomes between weekdays and weekends were assessed with the Wilcoxon signed-rank test. The significance threshold was set at α = 0.05. Analyses were performed with IBM SPSS 17.0 (Armonk, New York).
Results
A total of 25 subjects were recruited to participate in the study. Data from individual subjects’ sock logs were extracted and graphed for visual analysis (Figure 2). Data from two subjects were removed based on review of the returned sock logs and visual analysis of the data. One subject reported an extended and irregular daily schedule that often exceeded the standardized 24-h period used in this study. The resultant data were deemed to be incomparable to the other study subjects. A second subject did not adhere to provided instructions and reported sock use over nonconsecutive days. These data were deemed to be similarly inconsistent with the remainder of the study subjects and was removed from this analysis. Data from the remaining 23 subjects (Table 2) were included in the computational analyses described here.
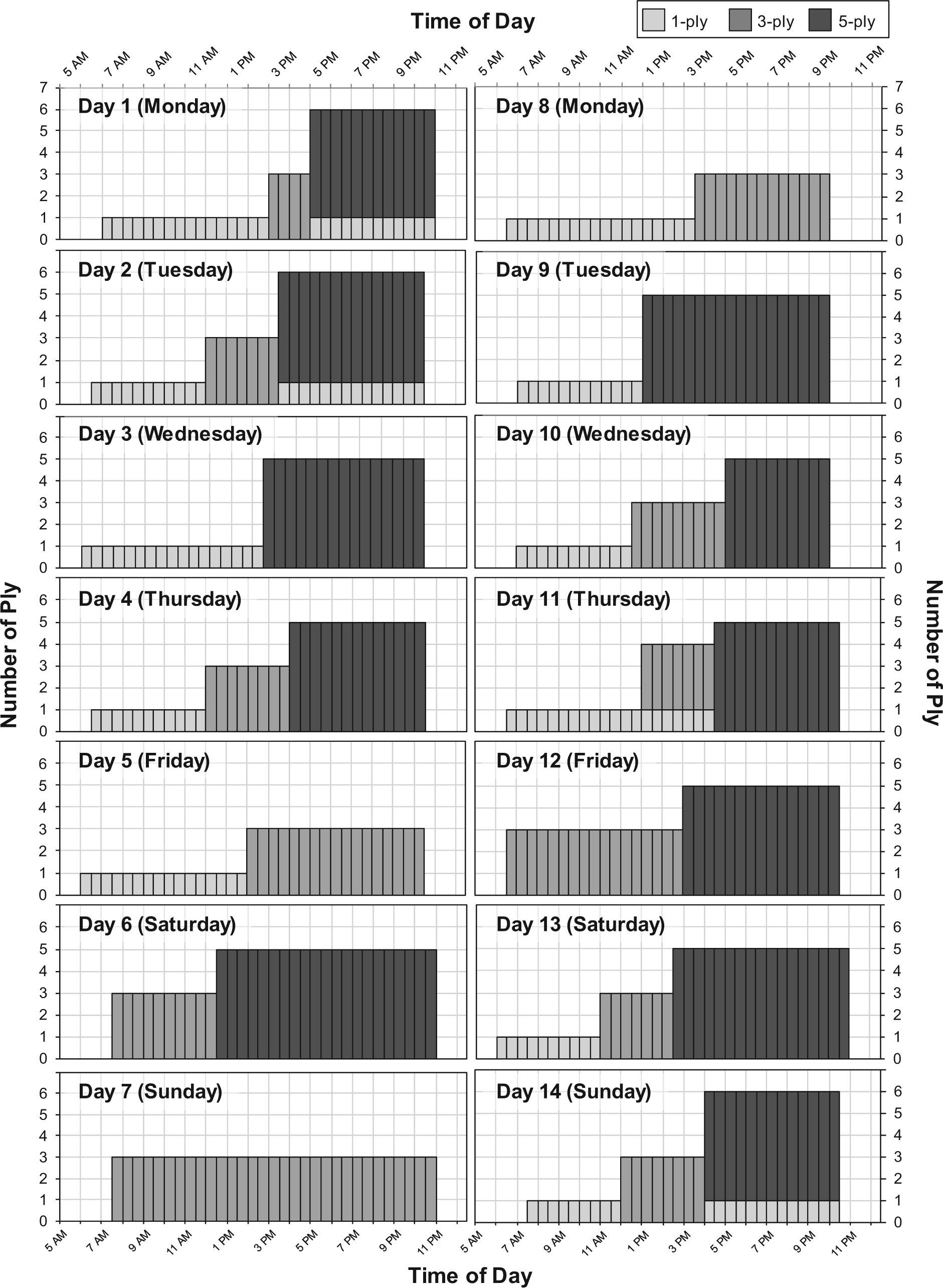
Daily sock use, as measured using the sock log. Two weeks of data for one subject are shown.
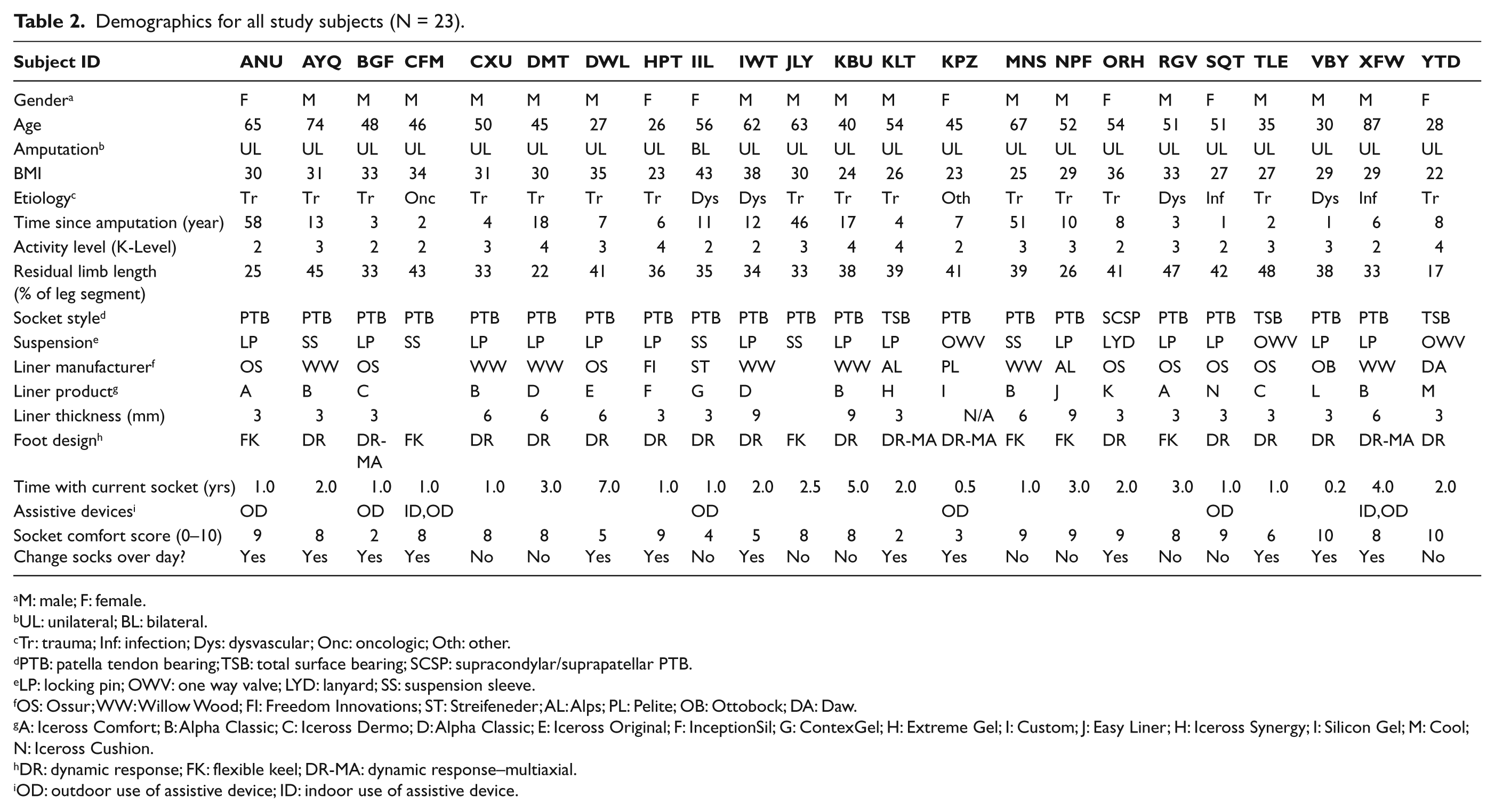
Demographics for all study subjects (N = 23).
M: male; F: female.
UL: unilateral; BL: bilateral.
Tr: trauma; Inf: infection; Dys: dysvascular; Onc: oncologic; Oth: other.
PTB: patella tendon bearing; TSB: total surface bearing; SCSP: supracondylar/suprapatellar PTB.
LP: locking pin; OWV: one way valve; LYD: lanyard; SS: suspension sleeve.
OS: Ossur; WW: Willow Wood; FI: Freedom Innovations; ST: Streifeneder; AL: Alps; PL: Pelite; OB: Ottobock; DA: Daw.
A: Iceross Comfort; B: Alpha Classic; C: Iceross Dermo; D: Alpha Classic; E: Iceross Original; F: InceptionSil; G: ContexGel; H: Extreme Gel; I: Custom; J: Easy Liner; H: Iceross Synergy; I: Silicon Gel; M: Cool; N: Iceross Cushion.
DR: dynamic response; FK: flexible keel; DR-MA: dynamic response–multiaxial.
OD: outdoor use of assistive device; ID: indoor use of assistive device.
Of the final 23 survey respondents, 16 were male and 7 were female. Subjects ranged in age from 26 to 87 years with a mean of 50 years (standard deviation (SD) = 15 years). A total of 22 subjects in the study had unilateral transtibial amputation, and one had bilateral transtibial amputations. Time since amputation ranged from 1 to 58 years, with an average of 13 years (SD = 16 years). Nine individuals were classified by the study prosthetist as K-level 2 (K2), nine as K-level 3 (K3), and five as K-level 4 (K4). Residual limb length ranged from 17% to 48% of anatomical tibial segment with a mean of 36% (SD = 8%). Body mass index (BMI) ranged from 22 to 43, with a mean of 31 (SD = 5) across all study subjects. Etiology of amputation varied across the study sample. A total of 16 individuals experienced their amputation as a result of a traumatic injury, 4 from dysvascular-related issues, 2 as a result of infection, 1 from cancer, and 1 from other causes (i.e. club foot). A total of 19 subjects used patellar tendon bearing (PTB) sockets, 3 used total surface bearing (TSB) sockets, and 1 used a supracondylar suprapatellar (SCSP) PTB socket. Of 23 subjects, 14 subjects used a locking pin suspension system, 1 a lanyard, 3 a one-way valve, and 5 used suspension sleeves. Subjects included in this study reported an average SCS of 7.2 (SD = 2.4).
A total of 13 subjects (9 males and 4 females) were categorized into subgroup 1 and 10 (7 males and 3 females) into subgroup 2. Groups were similar in age (50 years), BMI (29 and 30), residual limb length (38% and 33% of the anatomical tibial segment), and time with current socket (1.9 and 2.3 years). Each subgroup consisted of a similar proportion of men (69% and 70%), those who had experienced amputation due to trauma (62% and 70%), those who had experienced amputation due to dysvascular disease (15% and 20%), those with PTB socket designs (85% and 90%), and those who used a locking pin suspension (62% and 60%). Subjects in subgroup 1 had experienced their amputation, on average, more recently than those in subgroup 2 (10 and 17 years prior). Subjects in subgroup 1 were generally of a lower activity level, as the proportion of those classified as K2 (54% and 20%), K3 (31% and 50%), and K4 (15% and 30%) differed between groups. SCS was, on average, lower in subgroup 1 (6.5) as compared to subgroup 2 (8.1). There also seemed to be a higher portion of people within subgroup 1 who used assistive devices for outdoor walking (38% and 20%). However, no significant differences (p > 0.05) between subgroups according to subjects’ gender, age, BMI, time since amputation, residual limb length, time with current prosthesis, or SCS were found.
Subjects reported wearing their sockets 14.8 h per day (SD = 1.5 h) and prosthetic socks for 14.2 h per day (SD = 3.0 h) over the study period (Table 3 and online Appendix 1). Sock ply at the beginning and end of each day was 4.8 (SD = 3.9) and 5.5 (SD = 3.9), respectively. Subjects changed socks, on average, less than once per day (mean = 0.6, SD = 0.5). Sock changes typically were performed 2.4 h (SD = 2.2 h) after donning the prosthesis. No significant differences (p < 0.05) in the studied outcome variables (Table 1) were observed between subgroups 1 and 2. Study subjects reported significantly longer periods of socket use (p = 0.02) on weekdays (mean = 15.0 h, SD = 1.3 h) compared to weekends (mean = 14.1 h, SD = 2.5 h). Although the mean time of sock wear was similarly greater on weekdays (mean = 14.5 h, SD = 3.0 h) than on weekends (mean = 13.6 h, SD = 3.3 h), the difference was not significant (p = 0.06). No significant differences in sock ply at donning (mean = 4.8, SD = 3.9 on weekdays and mean = 5.5, SD = 3.8 on weekends), sock ply at doffing (mean = 4.8, SD = 3.9 on weekdays and mean = 5.4, SD = 4.2 on weekends), or mean sock ply (mean = 5.6, SD = 3.8 on weekdays and mean = 5.4, SD = 4.0 on weekends) were noted. However, subjects reported significantly more (p = 0.03) sock changes on weekdays (mean = 0.6, SD = 0.6) than on weekends (mean = 0.4, SD = 0.4). Time to first sock change was also significantly (p = 0.03) greater on weekdays (mean = 2.8 h, SD = 2.6 h) than on weekends (mean = 1.6 h, SD = 1.9 h).
Average daily sock use across the study sample and by subgroup. No significant differences between groups were observed. Subjects reported significantly greater wear time (p = 0.02), sock changes (p = 0.03), and time until first sock change (p = 0.03) on weekdays than on weekends.
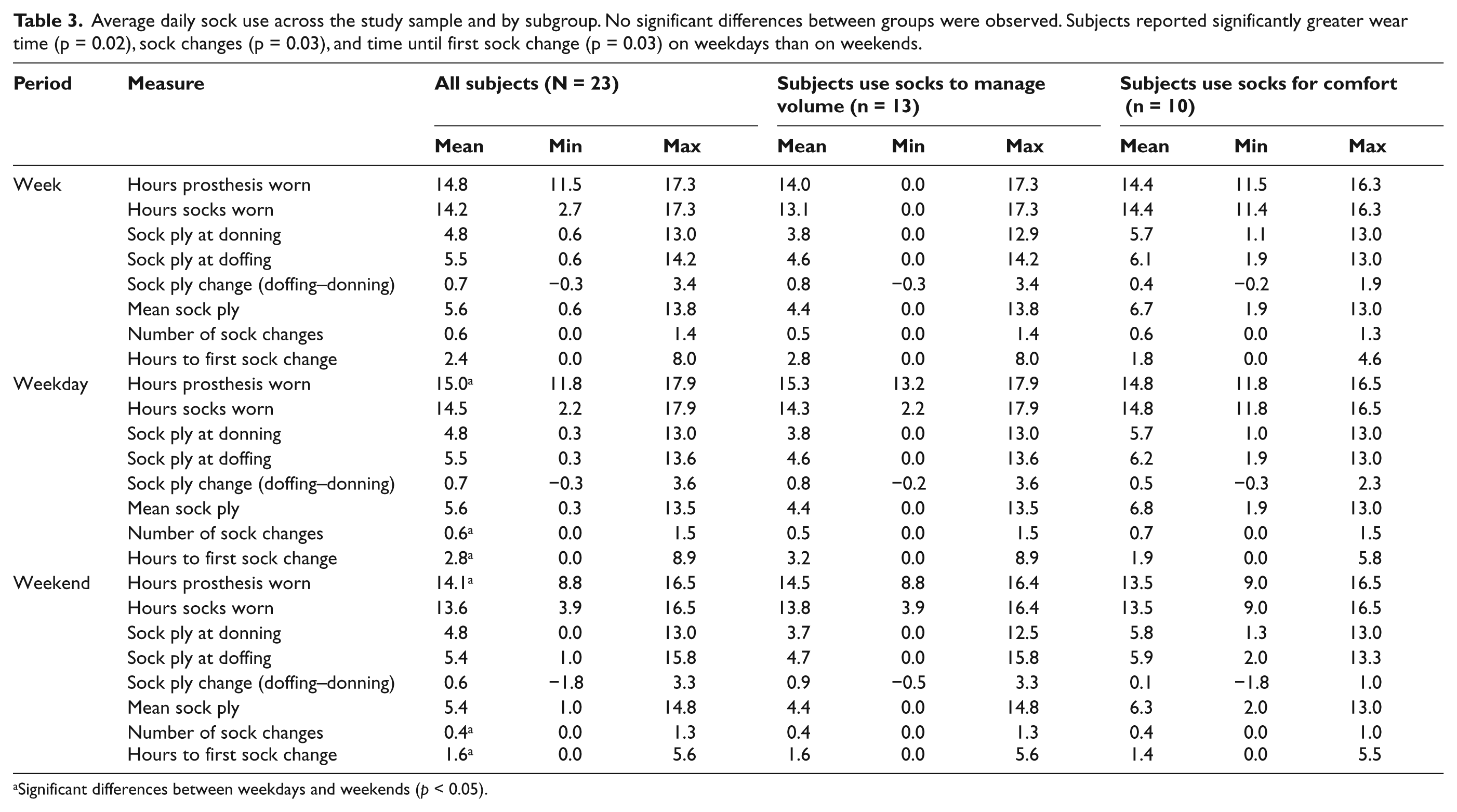
Significant differences between weekdays and weekends (p < 0.05).
Discussion
Proper fit between the socket and the residual limb is well recognized as a critical factor in overall comfort and security of a prosthesis.7,15–17 Although practitioners often discuss socket fit with patients, verbal questions posed at the clinic visit may not elicit a thorough understanding about the patients’ daily routines (or lack thereof) for managing residual limb volume fluctuations and comfort. A sock log was used in this study to quantify patterns of sock use among persons with transtibial amputation. More precise knowledge of sock use may help practitioners plan volume management strategies, justify socket replacement, or troubleshoot fitting issues, such as skin breakdown, discomfort, or pain. 9 Here, we used logs from persons with transtibial amputation to quantify the number of sock changes, sock thicknesses, and times when socks were changed each day.
Sock use varied, but showed interesting trends across our study population. Users donned their prostheses wearing a wide range of socks (i.e. less than 1 ply to 13 ply). While average sock ply at donning was slightly below 5 ply, 10 of 23 subjects started the day wearing more than 5 ply. As hypothesized, subjects in subgroup 1 generally started the day with less total ply than those in subgroup 2. However, subjects in subgroup 2 wore greater ply at doffing than did subjects in subgroup 1. Thus, subjects in subgroup 1 did not appear to add socks to account for volume loss to the extent we had hypothesized. Sock log data also showed that average cumulative ply in the evening was greater than 5 ply. However, only 10 of 23 subjects averaged above 5 ply at doffing (and 9 of these subjects started the day above 5 ply). While most subjects’ ply at doffing was less than the 10 ply limit associated with socket replacement,18–21 our experience suggests that socks in excess of 5 ply (particularly in addition to the 3- to 9-mm elastomeric liners used by many subjects in this study) may be deemed to be clinically unacceptable. If true, a large portion of the studied population may have been wearing sockets that could be deemed too large for optimal fit. Finally, of the 23 subjects included in this study, 12 added socks, 7 did not change socks, and 4 removed socks over the day, on average. Across the study population, subjects increased sock ply by 0.7 from the time of first donning to time of last doffing. This is consistent with our previous findings that suggest most, but not all, persons with transtibial amputation lose volume over the day. 12 Finally, we noted that study subjects, on average, changed socks less than once a day. This finding held true for both subgroups, suggesting prosthetic users rarely elect to change socks during the day. Failure to properly accommodate residual limb changes with socks could contribute to the multitude of skin issues reported among prosthetic users.9,10
Using data collected in this study, we also sought to assess the validity of a singular question (i.e. “do you add or change socks throughout the day?”) as an indicator of individuals’ sock-use routines by comparing sock log data from those who responded “yes” to those who responded “no.” Comparison of sock-use data, by subgroup, showed no significant differences among any of the measured outcomes. This may indicate that responses to questions about sock use are inconsistent with data collected with a daily log. This may mean that habits are being inaccurately reported to practitioners. However, as daily logs have also deviated from simultaneously collected performance data among prosthetic users, 22 more research is needed to determine which type of report (i.e. single-question or daily log) is more accurate.
We acknowledge several limitations to this study. First, this study included a relatively small sample (N = 23). Given the pilot nature of this study, this sample size was deemed appropriate. Although our sample population was limited, the ratios of gender and etiology of amputations in our sample population are consistent with larger studies of persons with limb loss. 23 Thus, we believe our sample to be representative of the target population. Another potential limitation is an assumption inherent to our analysis that ply and thickness are related by a fixed constant (e.g. 1 ply = 2 mm, 3 ply = 6 mm, 5 ply = 10 mm). Sock plies have traditionally been considered additive (e.g. two 1 ply are equivalent to one 2 ply).19,21,24 We initiated this study and analyzed the sock log data under this assumption. However, recent evidence suggests that thickness may vary across products of the same sock ply. 25 Thus, it may be warranted in future research to directly quantify or estimate the thickness of socks worn by limb users in lieu of assuming the relationship between ply and thickness. To assess the impact of our assumption, we compared sock ply and thickness for one subject (Figure 3). The thicknesses of the socks from one subject were measured using a technique described by Sanders et al. 8 As shown, the donning-to-doffing change was 20% (using plies relative to total ply at donning) and 50% (using measured thickness relative to sock thickness at donning). Thus, our analysis may underestimate the volume loss accommodated by socks over each day. While we acknowledge that ply outcomes (e.g. sock ply at donning, mean sock ply) in this study may be affected by our assumption, use of conservative (nonparametric) statistical analyses may mitigate the impact. Furthermore, data related to number and timing of sock changes should be unaffected by ply-thickness assumptions. Finally, the sock log used to collect data for this study was developed purposefully for this application and has not been validated. To our knowledge, no similar measures of sock use exist. Future efforts should seek to validate this log using direct observation or objective instrumentation. 26
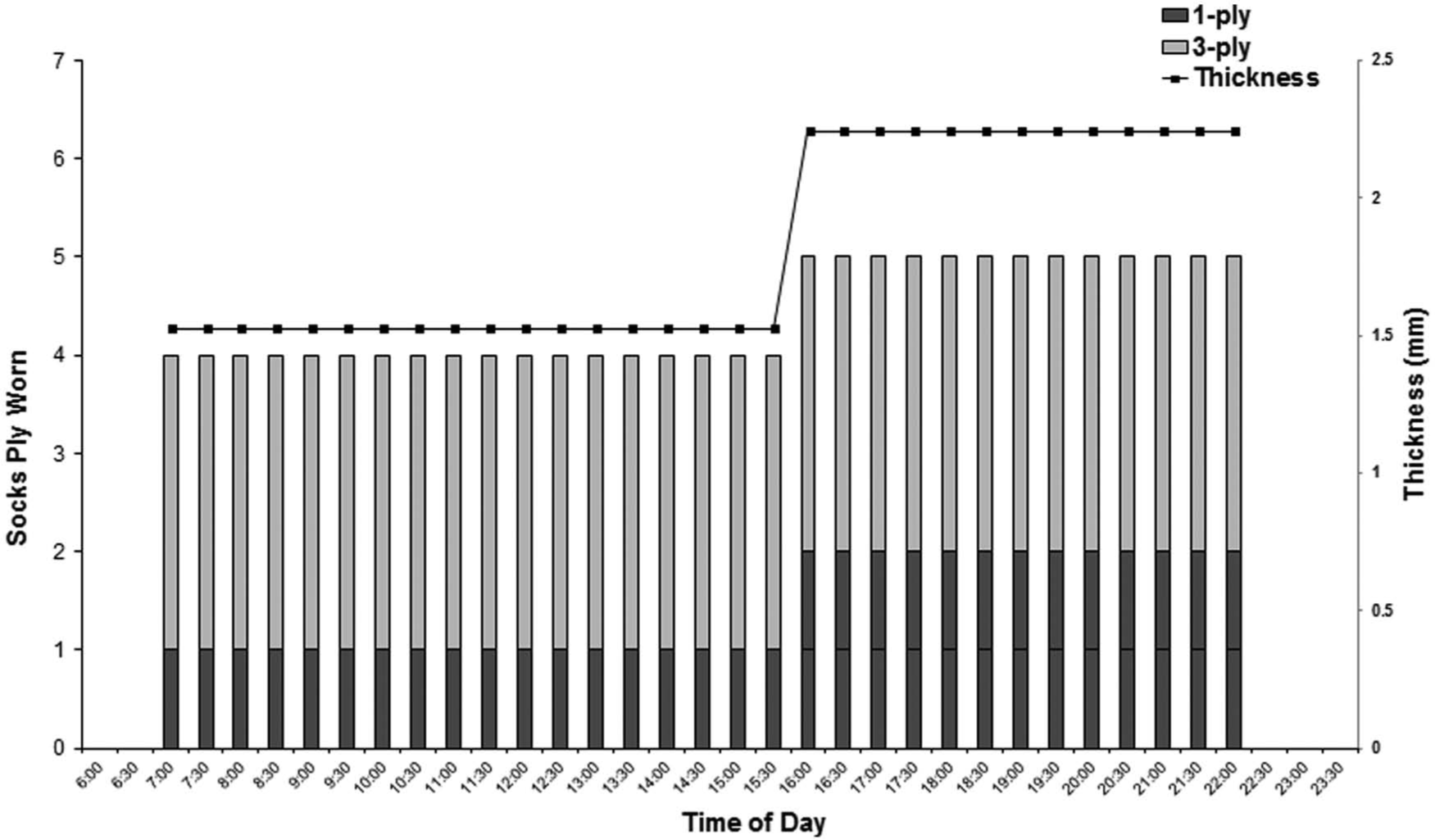
Comparison of sock thickness by distance units (right axis) and direct measurement (left axis). Data show that ply may underestimate relative changes in thickness when multiple prosthetic socks are used.
We believe sock logs, like that developed for this study, can be immediately useful to prosthetic clinicians and researchers. Clinicians could use this tool to better understand patients’ habits and select volume management strategies suited to the individual patient. Researchers could use the sock log developed here to assess the impact of prosthetic interventions on limb volume fluctuations over extended periods of time. Modifications to this log could also enhance its potential to address other questions of clinical or scientific importance. For example, it may be desirable to incorporate prosthetic liner use into the log. Knowledge of prosthetic liner type and thickness may help to assess overall volume accommodation. Fields could be added to allow respondents the ability to comment on reasons why socks were changed (e.g. socket too loose, pain distally, etc.). The log could also be modified to include the SCS 13 or other measures of residual limb health, such as the Prosthesis Evaluation Questionnaire. 27 Inclusion of standardized measures could facilitate study of factors that adversely affect or contribute to socket fit. Future study of volume management strategies and behaviors using tools such as these has the potential to greatly inform our understanding of the health of persons with limb loss. Large-scale administration of sock logs could be used to assess patterns of volume management in different patient populations (e.g. amputation due to trauma as compared to amputation from dysvascular disease), postamputation periods (e.g. recent as compared to established), climates (e.g. hot as compared to temperate), or healthcare systems (e.g. private as compared to public).
The data collected in this study represent sock-use strategies employed by a limited number of prosthetic users. However, they enhance our knowledge of volume management approaches used by people with limb loss. Our findings additionally raise questions that warrant consideration as we seek ways to enhance clinical care. For example, if patients advised to use socks to accommodate diurnal volume loss cannot or do not do so, then improved methods for achieving proper volume management are needed to maintain residual limb health. Creation of educational materials to facilitate sock use (e.g. take-home flyers), technologies to provide reminder notifications (e.g. text-messages), or development of self-adapting volume management strategies (e.g. automatically adjusting sockets) may be required to ensure users experience an optimal prosthetic fit. Through these and future efforts, it will be possible to create and maintain the intimate connection between a prosthetic user and their device.
Conclusion
Although lower limb prosthesis users add or remove socks to accommodate differences between the prosthetic socket and the residual limb, socks are rarely changed over the course of a day. In cases where changes are made, socks are generally (but not always) added over the day. Socks worn by prosthetic users often exceed 5 ply. There are no differences in sock-use patterns between those who claim to use socks for volume management and those who claim to use socks for comfort. These data suggest that socket fit may be suboptimal, and improved methods of volume management may be required to achieve an optimal fit. Future research should target improved strategies to manage limb volume and maintain a healthy residual limb.
Footnotes
Acknowledgements
The authors gratefully acknowledge Dan Harrison for subject scheduling and coordinating return of sock logs and Lee Organick for insight through the editorial process and analysis.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
Research reported in this publication was supported by the National Institute of Child and Human Development of the National Institutes of Health under award number R01HD069387. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.