
Abstract
Background:
Lower-limb prosthesis users typically experience residual limb volume losses over the course of the day that can detrimentally affect socket fit.
Objectives:
To determine whether temporarily doffing the prosthesis encouraged residual limb fluid volume recovery and whether the recovered fluid was maintained.
Study Design:
Experimental design.
Methods:
Residual limb fluid volume was monitored on 16 participants in three test sessions each. Participants conducted six cycles of resting/standing/walking. Between the third and fourth cycles, participants sat for 30 min with the prosthesis and liner: donned (ON), the prosthesis doffed but the liner donned (LINER), or the prosthesis and liner doffed (OFF).
Results:
Percentage fluid volume gain and retention were greatest for the OFF condition followed by the LINER condition. Participants experienced fluid volume losses for the ON condition.
Conclusion:
Doffing the prosthesis or both the prosthesis and liner during rest improved residual limb fluid volume retention compared with leaving the prosthesis and liner donned.
Clinical relevance
Practitioners should advise patients who undergo high daily limb volume losses to consider temporarily doffing their prosthesis. Fluid volume retention during subsequent activity will be highest if both the prosthesis and liner are doffed.
Background
For many people with lower limb loss, maintaining a stable and comfortable fit between the residual limb and prosthetic socket over the course of a day is challenging. Some amputees, especially individuals who have recently had their amputation, experience a reduction in residual limb volume over the course of a day as a result of mechanical pressures and shear stresses applied by the socket to the residual limb.1–3 Loss of volume may cause the socket to feel loose and promote pistoning, undesirable excessive motion of the residual limb up and down within the socket. 4 Limb volume changes alter the distribution of normal and shear stresses at the limb-socket interface and may put soft tissues at risk of injury.5,6
As a means to compensate for volume loss and thus reduce risk of injury, practitioners may recommend volume accommodation strategies for use inside the patient’s prosthetic socket. Socks, air-filled pads, liquid-filled bladders, and adjustable sockets, for example, are commercially available products intended to fill voids that result from limb volume loss. However, it was recently reported that reducing the size of the socket using socks or bladders can further accentuate limb fluid volume loss.7,8
In this study, a simple means for accommodation of fluid volume loss termed “socket release” was evaluated. Subjects performed socket release by temporarily doffing the prosthesis. No material was added or removed from inside the socket. Socket release was intended to facilitate fluid volume recovery by relieving socket interface stresses immediately after a period of activity. In this study, we investigated whether socket release encouraged fluid volume recovery and whether the recovered fluid was maintained during subsequent activity.
Methods
Participants
Human subject approval from an institutional review board at the University of Washington was obtained before test procedures were initiated. Trans-tibial amputee subject volunteers were recruited to participate in this study. Inclusion criteria were a trans-tibial amputation performed at least 1 year prior, use of a definitive prosthesis, capability to walk at least 5 min continuously on a treadmill, capability to stand 2 min continuously with equal weight-bearing, and a residual limb length that allowed at least 5.5 cm between voltage-sensing electrodes (necessary for proper bioimpedance measurement 9 ). Exclusion criteria were skin breakdown or presence of metal implants within the limb which can distort bioimpedance results. The research practitioner interviewed the subject and inspected the residual limb at the outset of each test session to ensure the subject met all inclusion criteria.
Instrumentation
A bioimpedance analyzer and custom electrodes constructed specifically for testing amputee residual limb fluid volume were used in this study. The system is described in detail elsewhere. 10 In brief, the instrument generated short packets of constant alternating electrical current (~300 µA). Each set of packets included 24 frequencies between 5 kHz and 1 MHz. Approximately 20 packets/s were transmitted via cable to electrodes positioned proximally on the thigh and distally on the inferior surface of the residual limb (Figure 1). Voltage was sensed via two channels, one from the anterior surface and another from the posterior surface. On each surface (anterior and posterior), one voltage-sensing electrode was positioned at the level of the patellar tendon and the other at the level of the distal tibia. The instrument collected and processed the current and voltage data and then stored results to disk. No filtering was performed on the signal.
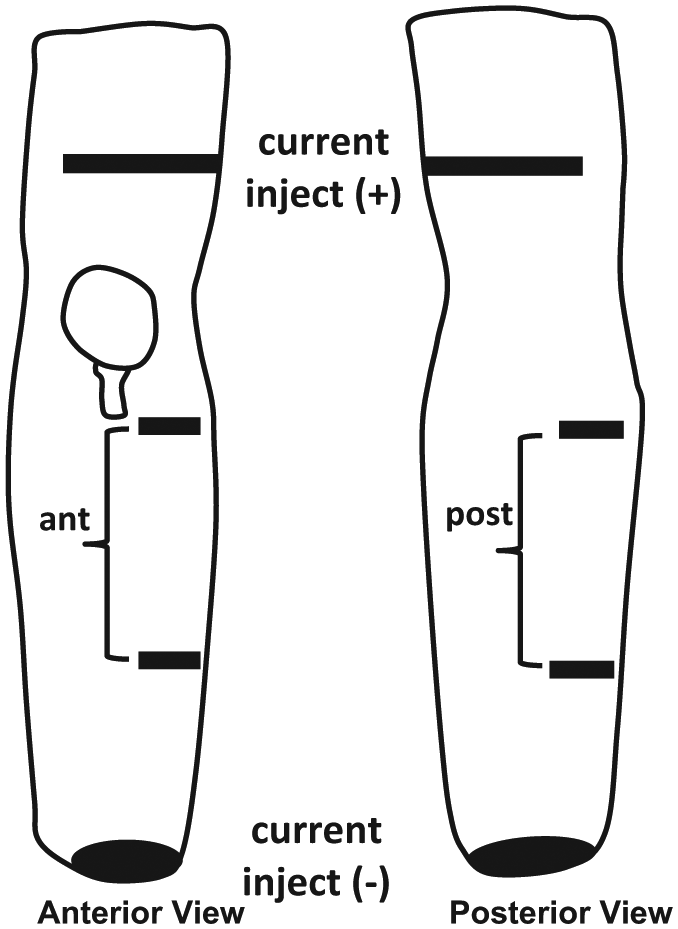
Electrode layout. Current injecting electrodes were placed on the thigh (one anterior, one posterior) and on the distal inferior residual limb. Two voltage-sensing electrodes were placed on the anterior lateral side for the anterior channel (ant) and two on the posterior side for the posterior channel (post).
The electrodes were constructed using a conductive polymer (ARCare 8881; Adhesives Research Inc., Glen Rock, PA, USA (thickness 0.09 mm), hydrogel (KM10B, Katecho; Des Moines, IA, USA (thickness 0.81 mm), and a very thin layer of coupling agent between the hydrogel and skin (ultrasonic coupling gel; GE Panametrics, West Chester, OH, USA). Multi-stranded silver-platedcopper wire with an aramid core and poly vinyl chloride insulation (32 AWG; New England Wire, Lisbon, NH, USA) (thickness: 0.76 mm) and a flattened gold crimp at the wire-insulation boundary was used for the electrode leads. The proximal current injecting electrodes were 1.5 × 15.0 cm, the distal current injecting electrode was of 3.5 cm diameter, and the voltage-sensing electro-des were 1.5 × 5.0 cm. Electrodes were covered with 0.03-mm-thickness Tegaderm Transparent Film Dressing ( 3M, St. Paul, MN, USA).
Test procedure
On each of three test days, the participant sat for 10 min after arrival to achieve a homeostatic condition. While sitting, participants answered questions about their health history and recent changes to their prosthesis. Temperature in the room was controlled via the building thermostat to 22°C. Medical history was recorded and medications that might affect residual limb volume identified. The subject’s body mass was measured. Participants then doffed their prosthesis, liner, and socks (if worn). The participant’s skin was cleaned (Red Dot Trace Prep; 3M) and electrodes were placed on the residual limb. If a participant had bilateral trans-tibial amputation, the limb expected to produce the strongest bioimpedance signal (i.e. longest length, least skin scarring near electrode sites) was selected for testing. Wires from the electrodes were extended proximally along the lateral aspect of the thigh. Care was taken to ensure wires were laid flat and covered with Tegaderm at the brim to avoid air gaps and ensure no loss of prosthetic suspension.
After the electrodes were placed on the limb, bioimpedance data collection was initiated. The participant donned the prosthesis and sat in a chair for 90 s. We reminded the participant to keep a proper sitting posture by avoiding excessive knee flexion that might occlude blood flow and by avoiding too much extension that might cause a slouching posture. Bioimpedance data were observed by the researchers on a computer monitor in approximately real time (~2-s delay) to ensure the instrumentation was performing properly. The participant stood for 90 s on a platform with an electronic scale embedded in the surface to monitor weight bearing on the prosthetic limb. If the prosthetic-side weight deviated by more than 10% of half the body weight, the participant was instructed to shift his or her weight to restore equal weight bearing. The 10% criteria was based on prior investigation where we found that this range of weight-bearing change did not typically induce changes in bioimpedance results and thus did not require continual instruction to the subject for weight shifting. 11 Next, the participant walked for 5 min on a treadmill at the self-selected walking speed established during subject inclusion/exclusion testing. This 5 min of treadmill walking was followed by standing briefly (5–10 s) on the platform with the embedded electronic scale. The participant repeated the sit (90 s)/stand (90 s)/walk (5 min)/brief stand (5–10 s) cycle two more times for a total of three cycles. The participant then sat down for 30 min with the prosthesis in one of three conditions (one condition was performed on each of the three test days): (1) ON: prosthesis and liner left donned; (2) LINER: prosthesis doffed but liner left donned; (3) OFF: prosthesis and liner doffed. After the 30-min period, the subject donned the prosthesis (if it was removed) and conducted three more sit (90 s)/stand (90 s)/walk (5 min)/brief stand (5–10 s) cycles as performed earlier in the test session. At the conclusion of the cycles, the subject doffed the prosthesis, bioimpedance data collection was terminated, and the electrodes were removed. The three test conditions (ON, LINER, OFF) were conducted on three different test days in a randomized order. We attempted to schedule test sessions at the same time of day for each subject and asked subjects to perform similar physical activities each day before coming to the lab.
Analysis
Collected bioimpedance data were post-processed using custom-written code in MATLAB (MathWorks, Natick, MA, USA) that performed de Lorenzo’s version of the Cole modeling strategy. 12 Data from the model were converted to extracellular fluid volume using a limb segment model. 13 No filtering of the signal was conducted.
Percentages limb fluid volume change during the 30-min rest period, short-term fluid volume response, and long-term fluid volume response for each test condition were calculated (Figure 2)
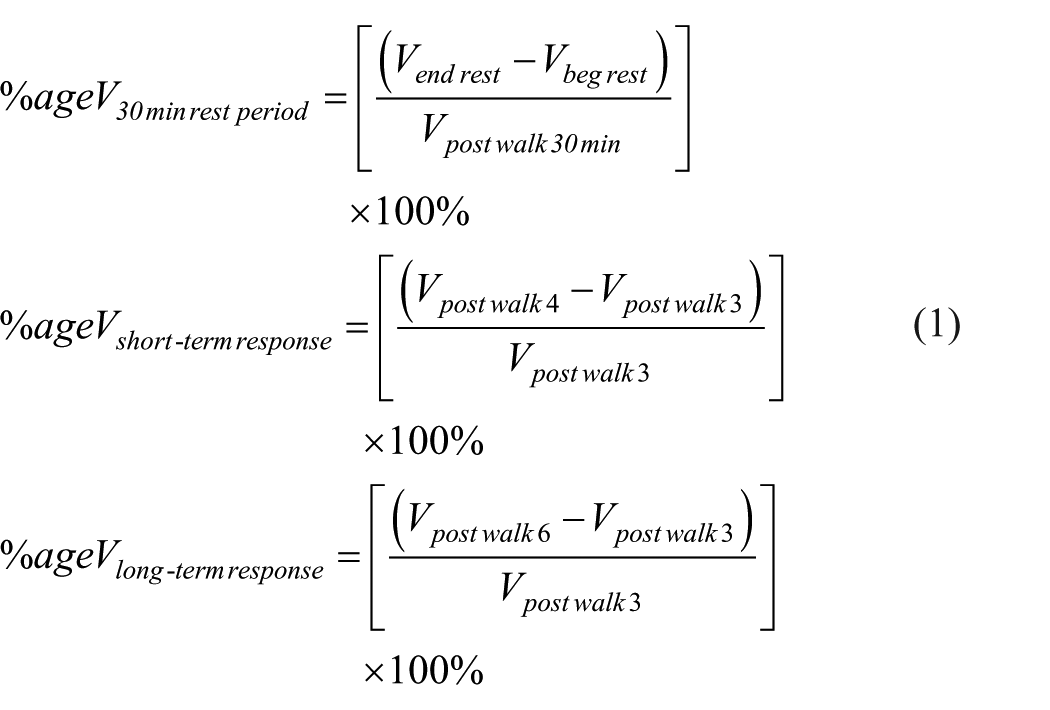
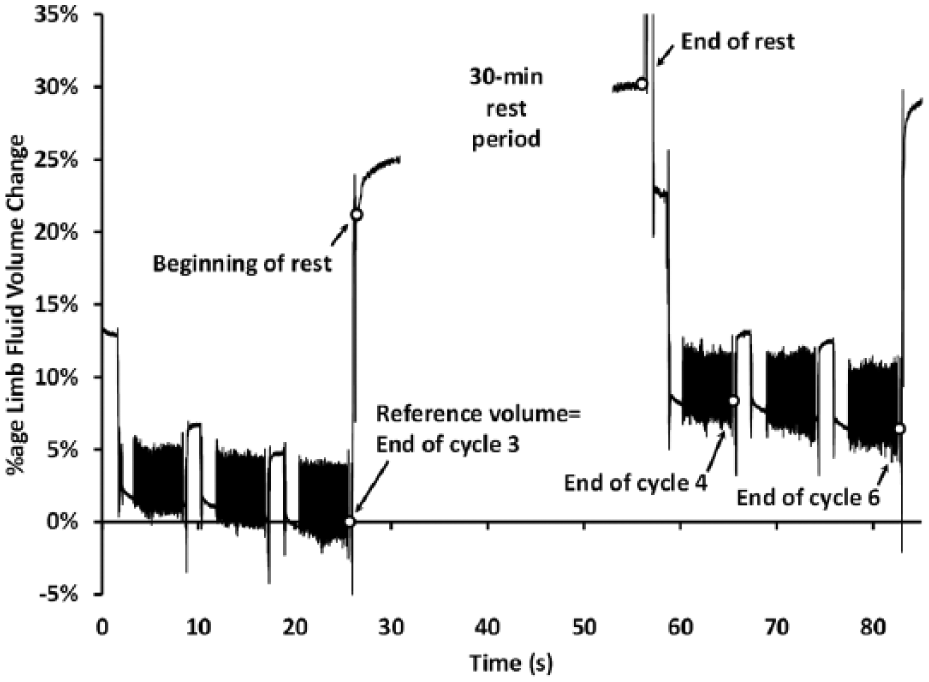
Data points used in analysis. Labeled points correspond to variables in equation (1).
We used the Vpost walk3 as the reference (denominator) for all three calculations because the experimental protocol was identical up to that point for all protocol conditions (ON, LINER, OFF). We were interested in effects of our intervention strategy (condition) relative to this point. Results are presented as percentage changes since subjects had different residual limb sizes.
We conducted a repeated-measures analysis of variance (ANOVA) with Greenhouse–Geisser adjustment for lack of sphericity, and Bonferroni adjustment for post hoc tests to assess whether there were differ-ences in
Results
A total of 16 individuals participated in the study. Subject and prosthesis characteristics are summarized in Table 1. No participants’ prosthesis was altered between sessions. The average time of day difference between the start of the latest session and the start of the earliest session averaged 1.7 h. Of these, 11 subjects were tested within 2 h of the same start time, 3 subjects between 2 and 3 h (#s 4, 8, 15), and 2 subjects more than 3 h (#s 10, 12). The number of months to complete all three test sessions averaged 69 days (±43). It was less than 3 months on 13 subjects and more than 3 months on 3 subjects. Subject absolute value mass changes over the course of testing (max mass–min mass) as assessed by measurements at the start of each test session averaged 2.3 kg (+1.4) and ranged from 0.1 to 6.0 kg.
Subject and prosthesis characteristics.
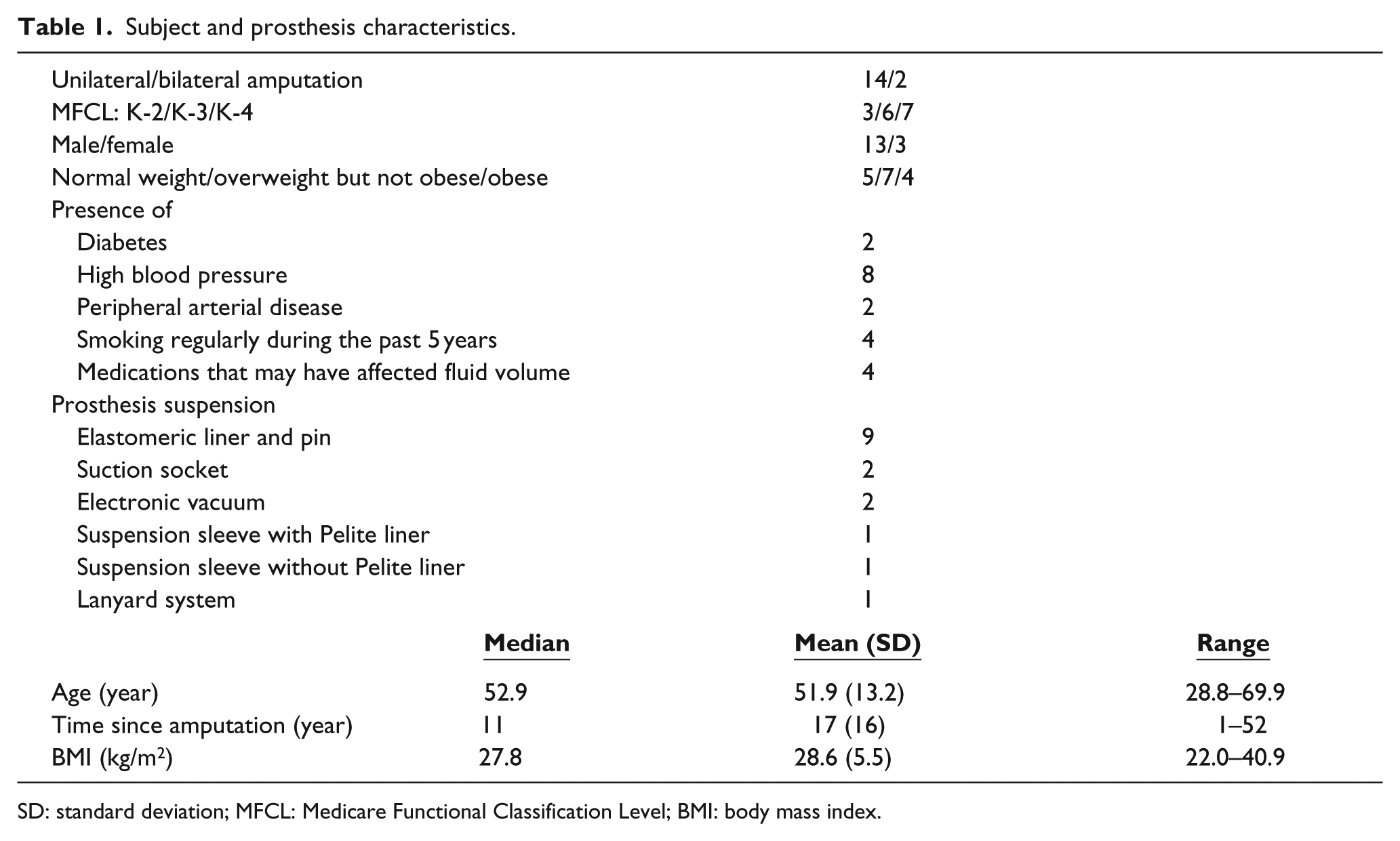
SD: standard deviation; MFCL: Medicare Functional Classification Level; BMI: body mass index.
Limb fluid volume reduced during the 30-min recovery period with the socket donned (ON) for all participants for both anterior and posterior regions with the exception of Subject 14 who showed a slight increase for the anterior region (Figure 3(a) and (b)). All 16 participants gained fluid volume during the recovery period when doffing the socket (OFF), both anteriorly and posteriorly. All participants gained limb fluid volume when the socket was doffed and liner donned (LINER) except Subject 15 who showed a slight reduction for the posterior region (Figure 3(b)). Mean percentage fluid volume changes are summarized in Table 2.
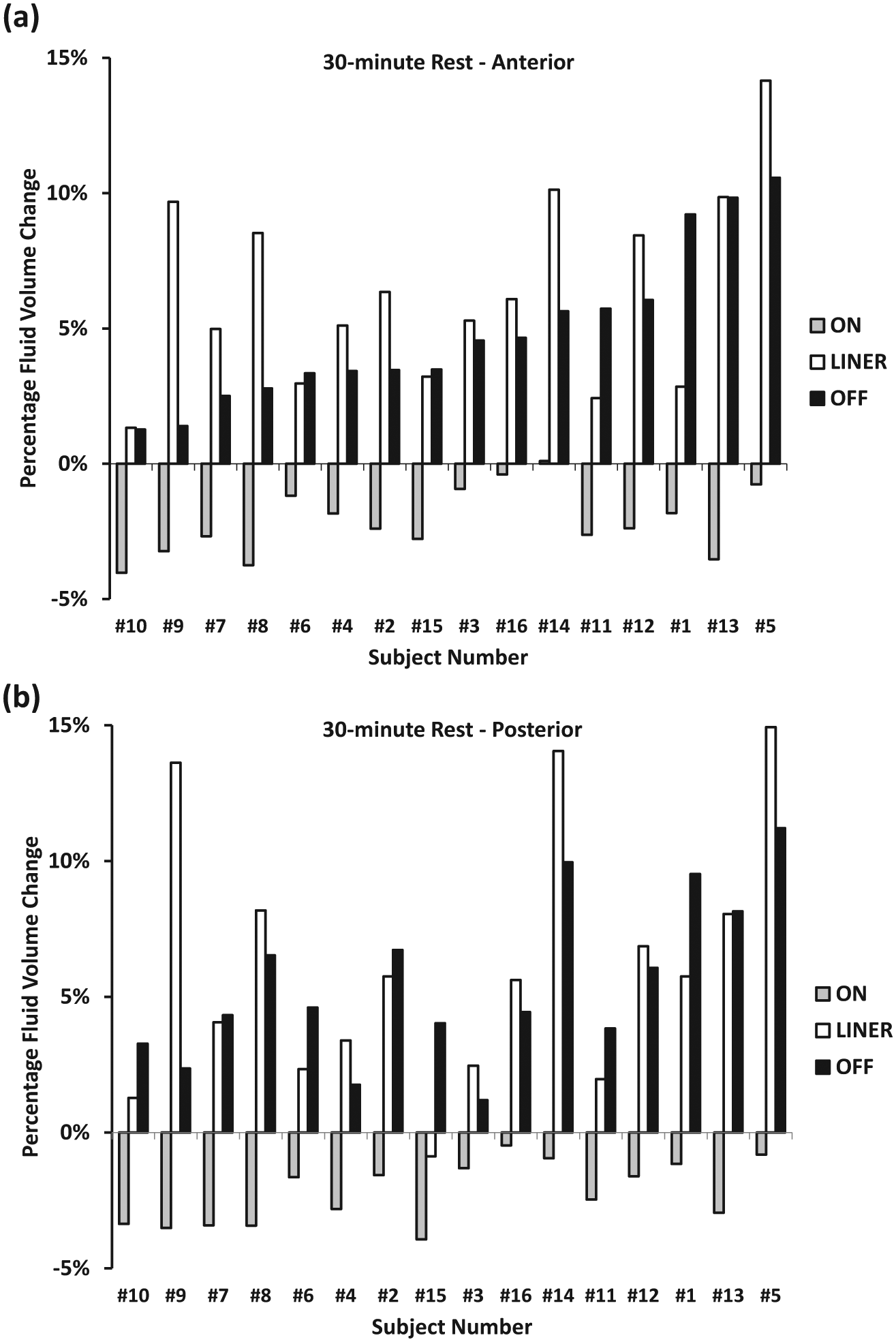
Rest period percentage fluid volume changes for all subjects: (a) anterior (top panel) and (b) posterior (bottom panel) changes are shown. Subjects ordered left to right from low to high anterior 30-min rest fluid volume change for the OFF condition.
Mean (SD) percentage fluid volume changes for all 16 participants.
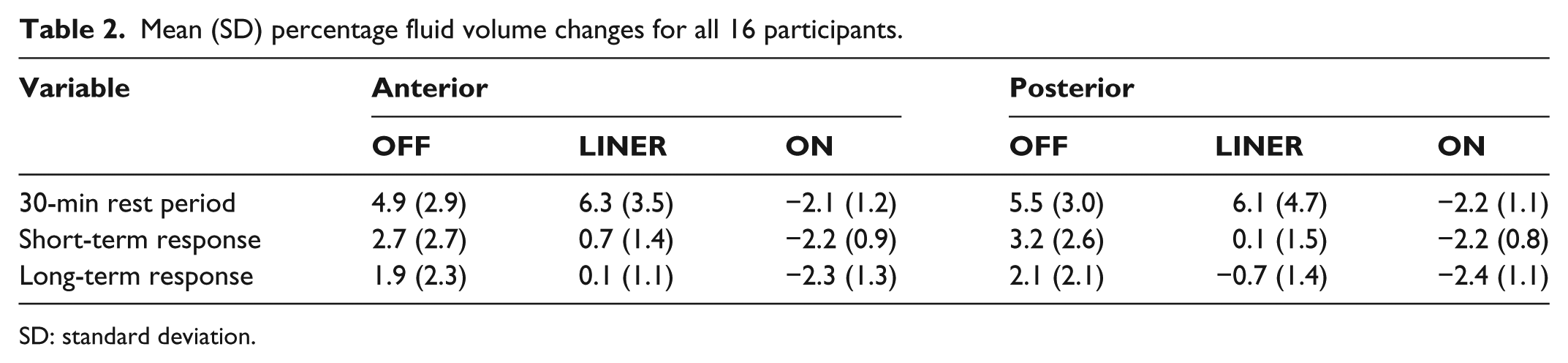
SD: standard deviation.
The repeated-measures ANOVA showed statistically significant differences between percentage fluid volume changes (p < 0.001 for both anterior and posterior) during the rest period for the three conditions (ON, LINER, OFF). Post hoc comparisons showed that percentage fluid volume changes were elevated for OFF compared to ON (p < 0.001 for both) and for LINER compared to ON (p < 0.001 for both), but not different between OFF and LINER (p = 0.33 for anterior and p = 1 for posterior).
All 16 participants lost fluid volume over the short term for the ON condition for both anterior and posterior regions (Figure 4(a) and (b)). Of 16, 13 participants showed fluid volume increases in percentage short-term fluid volume change for the OFF condition for anterior sites and 14 for posterior sites. For the LINER protocol, results were mixed.
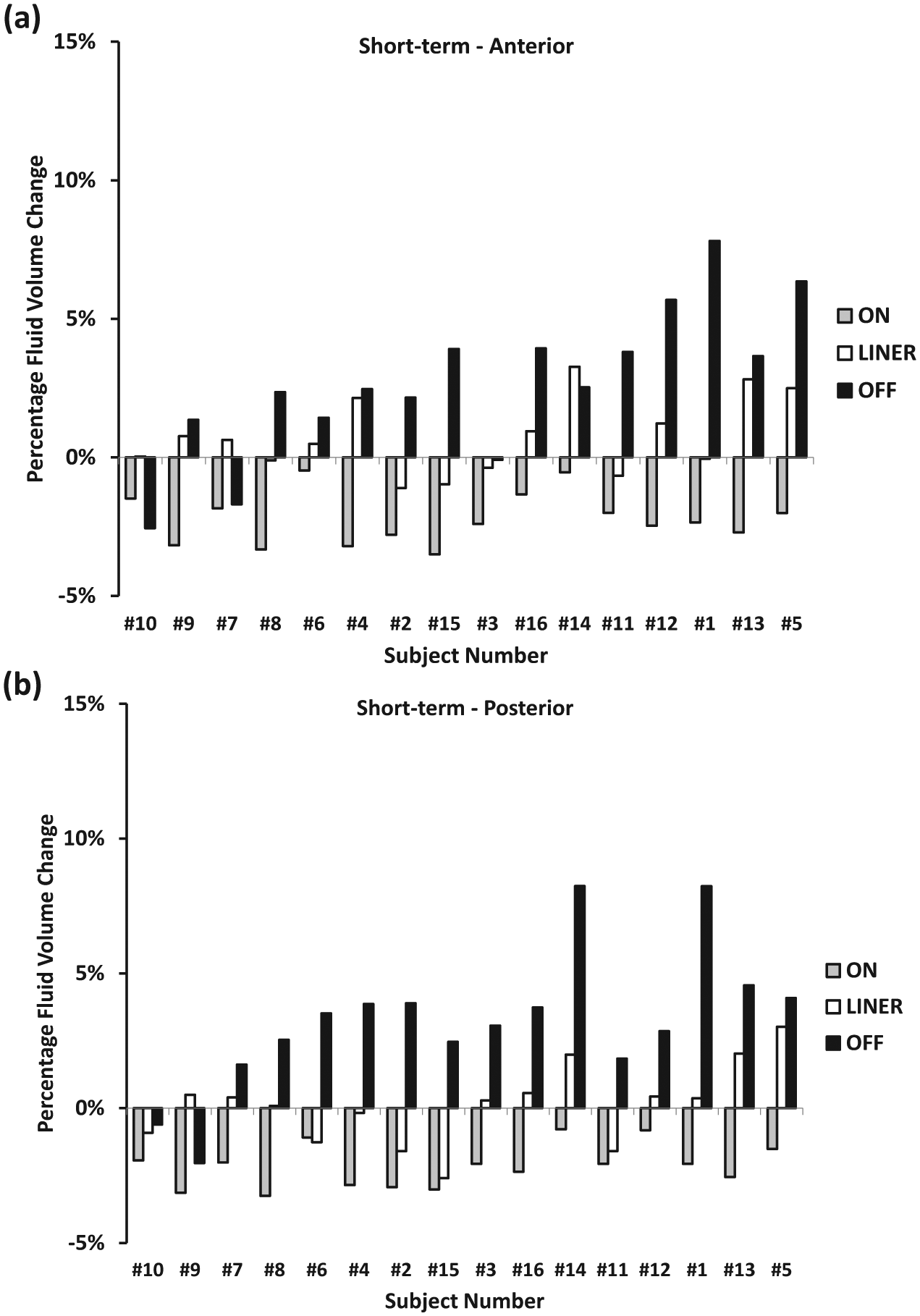
Short-term percentage fluid volume changes for all subjects: (a) anterior (top panel) and (b) posterior (bottom panel) changes are shown. Subject ordering same as for Figure 3(a) and (b).
The repeated-measures ANOVA of the percentage short-term fluid volume change data showed statistically significant differences between the three conditions (p < 0.001 for both anterior and posterior), and post hoc tests showed that differences between pairs of conditions were statistically significant (p ⩽ 0.04 in all cases). Therefore, the average change in percentage fluid volume between the cycle after the rest period (fourth cycle) and the cycle before the rest period (third cycle) depended on the recovery period condition (ON, LINER, OFF).
Percentage long-term fluid volume change for the ON condition was negative for all 16 participants for both the anterior region and posterior region with the exception of Subject 6 who experienced a slight increase for the anterior region (Figure 5(a) and (b)). For the OFF condition, 13 of 16 subjects experienced increases in the anterior region and 14 experienced increases in the posterior region. Results for the LINER condition were mixed.
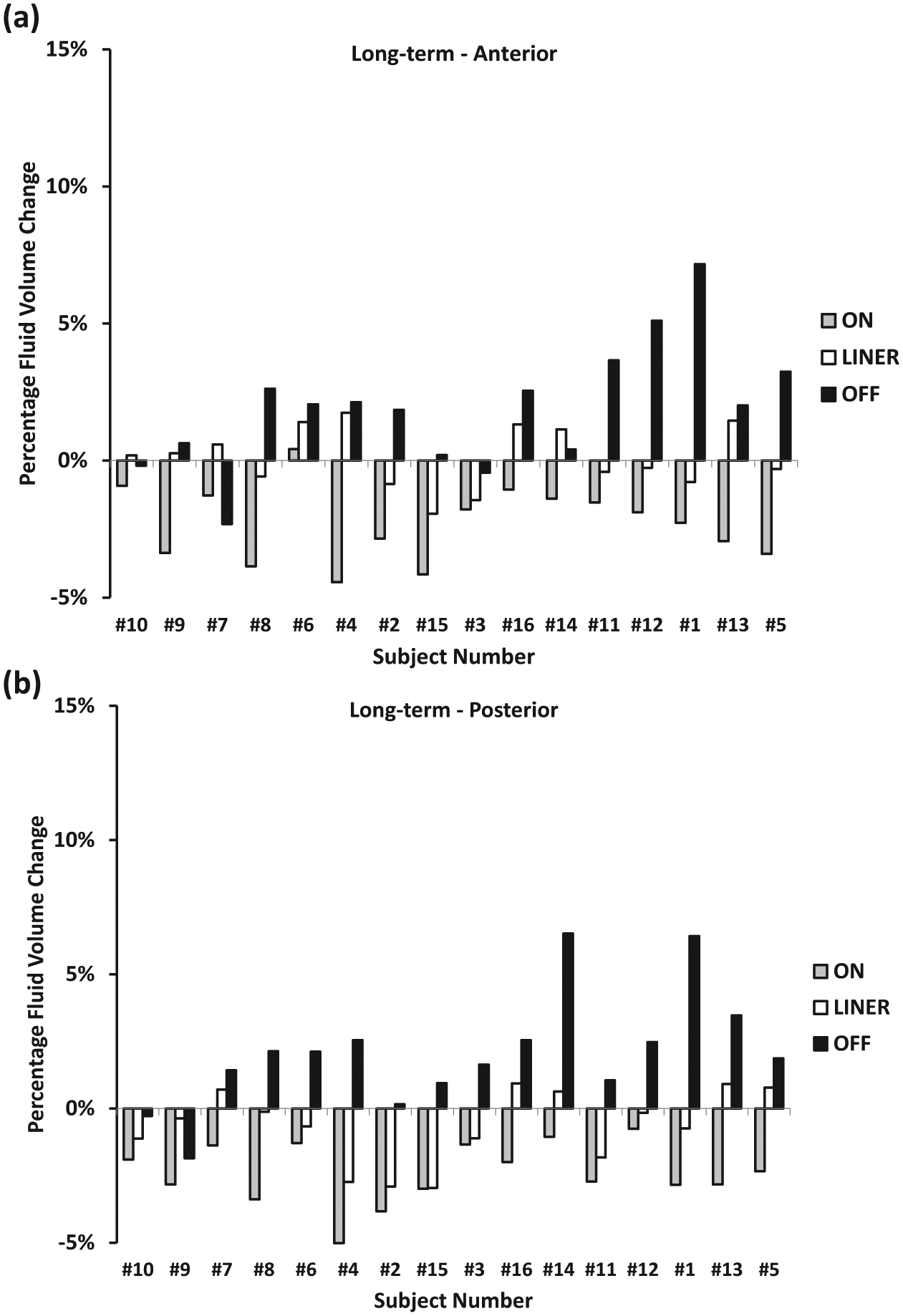
Long-term percentage fluid volume changes for all subjects: (a) anterior (top panel) and (b) posterior (bottom panel) changes are shown. Subject ordering same as for Figure 3(a) and (b).
The repeated-measures ANOVA for percentage long-term fluid volume changes showed statistical significance between each of the three conditions (ON, LINER, OFF) with p < 0.001 for both anterior and posterior. The post hoc analysis showed that differences between conditions were each statistically significant (p < 0.04 for all). Therefore, the average percentage long-term volume change depended on the recovery period condition (ON, LINER, OFF).
Anterior versus posterior regions
Anterior and posterior percentage fluid volume changes were similar for all comparisons for ON and OFF conditions and for the 30-min rest for the LINER condition (Figures 3(a) and (b), 4(a) and (b), and 5(a) and (b)); subjects are ordered the same in all figures, from low to high anterior 30-min rest fluid volume change).
For the LINER condition, measures of mean percentage fluid volume changes for both short and long term on the anterior side tended to be larger than those on the posterior side. However, repeated-measures ANOVA including side (anterior vs posterior) as a second factor showed that only condition was statistically significant (p < 0.001 for both short and long term); there was no statistically significant effect of side (p = 0.39), or interaction between condition and side (p = 0.24).
Formal subgroup analysis for this small sample size would not have meaningful interpretation. We considered exploratory analysis, but refrained from performing it because certain subgroups had so few observations that we could not obtain meaningful estimates of the mean and standard deviation for each subgroup (e.g. only two bilateral amputations, only three females, most of the suspension types observed in one or two individuals).
Discussion
Use of socket release to increase limb fluid volume and mitigate daily residual limb volume loss is an alternative strategy to adding socks. Advantages are that with socket release, no socks need to be added or removed, and the prosthesis user does not need to remember to carry socks or adjust settings on the prosthesis.
We postulate that limb fluid volume recovery was greater during the rest period for the OFF and LINER conditions compared with the ON condition for two reasons. First, doffing the prosthesis reduced interstitial fluid pressures and thus increased arterial-to-interstitial fluid transport relative to interstitial-to-venous transport within the residual limb. Second, the reduced socket pressures allowed blood vessels within the residual limb to enlarge, increasing volume of blood within the limb vasculature.
Because fluid recovered into the residual limb during the rest period was maintained for both short- and long-term intervals, it was unlikely that the recovered fluid was exclusively from venous pooling. If it had been only venous pooling, then that fluid would have quickly departed the residual limb upon subsequent donning and weight bearing. 3 We therefore suspect that the recovered fluid was primarily interstitial fluid.
The magnitude of fluid volume recovered during the 30-min rest period was comparable between the LINER and OFF conditions, but the short- and long-term fluid volume recoveries were much lower for the LINER condition than the OFF condition. We propose three possible reasons for this result: (1) because the liner compressed the distal end of the residual limb, for the LINER condition, fluid recovery was focused to the proximal portion of the residuum, a location from which it was subsequently expelled more quickly during activity; (2) pressure relief over the entire limb surface is a necessary condition for fluid to enter and remain trapped within the interstitial space during subsequent activity; (3) presence of the liner typically quickened the time to reach a residual limb fluid volume maxima (similar to a previous study 14 ); thus, the remainder of the rest period for the LINER condition may have caused fluid volume loss rather than recovery. In the OFF condition, limb fluid volume typically continued to increase at the end of the rest period. Further research is needed to determine whether one of these modes of action dominates over the others.
A reason the anterior region tended to maintain limb fluid volume better than the posterior region for the LINER condition in both the short and long term may be interface stress relief during sitting. The anterior limb surface is minimally loaded during resting with the liner donned on most amputees because the tibial crest tends to serve as an apex and pull the liner away from tibial flares. This result lends support to explanation (2) above, that pressure relief over the limb surface is a necessary condition to maintain recovered fluid during subsequent activity. High sensitivity of transcutaneous partial pressure of oxygen to interface pressure has been demonstrated; a pressure of 42–71 mmHg (5.6–9.4 kPa) was sufficient to reduce transcutaneous partial pressure of oxygen to zero over the anterior lower limb of able-bodied human subjects. 15 This result supports the hypothesis that even very low interface pressures restrict fluid volume recovery.
Clinical application
Socket release may be an effective strategy to reduce residual limb fluid volume loss over the day. A person with limb amputation may benefit by removing the prosthesis during periods of inactivity (e.g. a lunch break). Our previous results illustrate that the degree of fluid volume recovery is higher if the prosthesis is doffed right after activity compared with doffing after rest. 14 The optimal doffing duration to achieve daily limb fluid volume stabilization is unknown and may need to be customized for the individual patient.
The greater short-term and long-term fluid volume recovery for the OFF condition compared to the LINER condition supports the conclusion that the lower the interface pressure during rest, the longer the recovered fluid is retained during subsequent activity. Wearing a tight liner and keeping the liner on after doffing the prosthesis will likely not gain and retain as much fluid from socket release compared with wearing a less restrictive liner or removing the liner altogether during socket release.
One limitation of our study was that, due to the small sample size, we could not assess whether certain factors, such as sex, weight, unilateral or bilateral amputation, type of suspension, and comorbidities, influenced the change in limb fluid volume. Furthermore, test sessions were conducted over a relatively short time period (less than 2 h). Bioimpedance monitoring for longer durations will be needed to quantify duration recovered fluid volume is maintained within the residual limb and if/when a second socket release is needed.
Future research
We suspect that socket release intervals of less than 30 min will accomplish effective limb fluid volume recovery, although it is unclear at this point to what degree the magnitude of recovery and retention during subsequent walking is dependent upon the duration of doffing. A sensitivity analysis of the duration of socket release may serve to establish clinical guidelines for appropriate doffing intervals.
Although results from the present investigation suggest that even the relatively low interface pressure from a donned elastomeric liner can affect the duration of fluid retained from socket release, the mode of action of the liner on limb physiology is still not clear. Three possible modes of action include (1) the prosthetic liner restricts the volume of blood entering the residual limb, (2) the liner restricts transport of fluid across the arterial walls into the interstitium, and (3) the liner enhances transport of fluid from the interstitium into the veins and out of the residual limb. Identifying the dominant mode of action would help toward the design of effective socket release strategies and devices.
Automated socket release systems that adjust socket size at appropriate times rather than by user intervention should also be considered. Actuators that relieve the socket wall based on posture and/or activity (e.g. using accelerometers, inclinometers, and/or force sensors) may be effective, although such systems may need to accommodate for day-to-day differences in physiological fluid transport rates of the prosthesis user. Furthermore, it will be important for such systems to carefully re-tighten the socket upon subsequent donning so that the prosthesis user is stable during weight-bearing. Finally, a liner that is not excessively tight may be an important criterion for such systems to achieve effective socket release.
Conclusion
The impact of socket release, doffing the prosthesis right after periods of activity, on residual limb fluid volume was investigated. Results showed that doffing the socket and liner for 30 min tended to induce both short-term and long-term fluid volume recovery and retention, while not doffing the socket and liner tended to induce short-term and long-term fluid volume loss. Doffing the socket but leaving the liner donned tended to induce comparable fluid volume recovery but less retention than doffing both the socket and liner. Results suggest that subjects who experience large limb fluid volume losses during the day may benefit from temporary doffing the prosthesis during rest. To determine whether shorter doffing durations (<30 min) are effective, further research is needed to establish relationships of doffing duration to limb fluid volume recovery and to what degree they depend upon qualities of the subject, for example, health status and prosthesis design.
Footnotes
Author contribution
Sanders: study design, analysis, article preparation and editing; Hartley: study execution, analysis; Phillips: study execution, analysis; Ciol: statistical analysis; Hafner: analysis and article editing; Allyn: study execution, article editing; Harrison: study execution.
Declaration of conflicting interests
The authors declare no conflict of interest.
Funding
This work was funded by the National Institute of Child Health and Human Development at the National Institutes of Health (Grant/Award Number: “R01HD060585”) and the Department of Defense CDMRP Orthopaedic Research Program (Award Number: “W81XWH-10-1-1035”).