
Abstract
Background:
Assistive devices that augment arm function were already introduced during the polio era. Devices are still being developed, but a review has not been performed thus far.
Objective:
To create an overview and categorize assistive devices facilitating arm function in activities of daily living for people with decreased arm function.
Study design:
Literature review.
Methods:
A systematic review in three scientific literature databases. Conference proceedings, assistive technology databases, and references were searched and experts consulted. This resulted in a database of dynamic arm supports. Product information was added, and the devices were categorized.
Results:
A total of 104 dynamic arm supports were found. These could be categorized as nonactuated devices (N = 39), passively actuated devices (N = 24), actively actuated devices (N = 34), or devices using the functional electrical stimulation principle (N = 7). Functionality analysis resulted in second-level categorization: tremor suppression, facilitation of anti-gravity movement, and assistance of specific joint motion.
Conclusion:
All devices could be ordered in a categorization of low complexity. Many have been developed; most have disappeared and have been succeeded by similar devices. Limitations of the devices found mainly concern interfacing and the range of motion facilitated. Future devices could make use of whatever residual strength is available in the users’ arm for control.
Clinical relevance
The provided overview of devices in this article and the classification developed is relevant for practitioners seeking assistive solutions for their clients as it makes the range of developed solutions both accessible and comprehensible.
Assistive devices augmenting arm functionality in the weak upper extremity were introduced extensively after the polio epidemic in the 1940s. Improved polio treatment resulted in large numbers of polio survivors with arms too weak to bring their hands to their mouths to feed themselves. 1 Assistive devices designed for this population allowed movement in the horizontal and vertical planes using gravity compensation to support the lower arm. These devices enhanced the users’ ability to eat and were therefore called feeders. Over time, these devices were used for different activities of daily living (ADL) and by people with different causes of upper extremity weakness. As a result, they became known as (mobile) arm supports 2 or orthotic devices. 1
Technological advances since the 1940s resulted in a steady development of new devices assisting persons with upper extremity limitations in ADL. Given such a rich history of developments, any new development initiative should take into account previously developed devices and their functionalities. While several articles refer to prior developments,2,3 no comprehensive overview of devices could be found in the literature, let alone an overview based on scientific publications. That is the aim of this article: to create an overview of orthotic devices and arm supports that have been developed in the past decades and to better understand the current status of this family of devices. This understanding is required to identify the functional abilities and limitations in current designs, which could point out potential for future developments.
Arm supports and orthotic devices are both classified in the assistive device classification of the International Organization for Standardization 4 (ISO 9999) as forearm support to permit manual activities, defined as: “delivery of forearm support during manual activities.” This categorization contains devices that follow the user’s movements, but also static devices that do not follow the user’s motion. Orthoses are defined in the ISO classification as: “externally applied devices used to modify the structure and functional characteristics of the neuromuscular or skeletal system.” This category of devices contains products such as splints, bandages, and functional electrical stimulators (FES). The problem is, however, that terms from the ISO classification are applied differently in the literature. On the one hand, the literature reports on different names being used for devices that are functionally the same, as noted by Landsberger et al. 2 On the other hand, different functions can be fulfilled with one kind of device, for example, with devices called orthotics: these may support feeding, but may also prevent a joint from moving. Practically, this inconsistent use of terms means that the name of a device does not always reflect its function correctly. Since the arm’s main function is bringing the hand to places where it can manipulate objects, a static device that does not follow the arm while this is moving cannot facilitate arm function to any great extend during the performance of many ADL tasks. Since these devices are less interesting for ADL, this article will focus solely on dynamic devices that facilitate arm function during the performance of ADL tasks. These will be called dynamic arm supports for the purpose of this article.
Rahman 5 and Cardoso 6 distinguished between two categories of dynamic arm supports from a technical perspective: nonpowered (or passive or body-powered devices) and powered devices. This distinction gives insight into the main differences between the two types of dynamic arm supports, but not much into the different functionalities and underlying working principles, of which knowledge is needed to provide a basis for future developments. This article gives an overview and categorization of dynamic arm supports, primarily with a view on possible new developments in this field.
Methods
Several methods were used to collate information on dynamic arm supports. These included a literature search and a search into assistive technology databases and conference proceedings. Additionally, the Internet was searched, references to studies mentioning a dynamic arm support were read, and experts were consulted.
A literature search was conducted in PubMed and CINAHL and the IEEE database in March 2012. The following combinations of key words and Medical Subject Headings (MeSH) were used in this search: neuromuscular diseases, muscular dystrophies, muscular disease, muscle weakness, cerebrovascular disorders, multiple sclerosis, arm dysfunction, stroke, spinal cord injury, hemiparesis, arm, upper extremity, upper limb, forearm, robot*, arm support, exoskelet*, orthotic device, and self-help device (for a complete list of search terms, see Appendix 1). Quality assessment of the publications retrieved was not part of the publication evaluation. There were no criteria regarding the date of publication. The search strategy was validated by checking the output of the search command for 4–7 titles for each database. These titles were relevant articles recommended by experts prior to the search.
Three reviewers scored the retrieved titles of references independently according to the following inclusion criteria: titles had to refer to any device that assists in activity or movement of the upper extremity and to people with limited arm function. References were excluded if they referred to training or therapy, had been developed to assist hand function only, or mentioned a static device. Articles not meeting the inclusion criteria obtained 0 points, meeting the inclusion criteria resulted in 2 points, and when in doubt, the publications were given 1 point.
When the sum of the scores appointed by the three reviewers equaled 2 or more, the abstracts were assessed. However, if the abstract was not written in English, the abstract was excluded. Two reviewers scored the abstracts independently using the same inclusion and exclusion criteria as for the titles. When the total score equaled two or more, one reviewer then scanned the full text. If the full text was not written in English, the article was excluded. The text was scanned for devices that could facilitate arm function in ADL. If a name or direct reference to a device appeared in the text, the name of this potentially relevant device was added to a database. Cohen’s kappa was calculated to determine the agreement between the three reviewers in title assessment and between the two reviewers in abstract assessment.
Records in the following Internet databases of assistive technology were inspected: Abledata, Eastin, Handywijzer, and VilansHulpmiddelenwijzer. The conference proceedings of Rehabilitation Engineering and Assistive Technology Society of North America (RESNA), Association for the Advancement of Assistive Technology in Europe (AAATE), Australian Rehabilitation & Assistive Technology Association (ARATA), and Rehabilitation Engineering Society of Japan (RESJA) were searched manually, and Google and GoogleScholar were searched using text words. References to dynamic arm supports encountered in the different searches were also searched and the following experts consulted: manufacturers, distributors, and an occupational therapist.
Names of potentially relevant devices from the different sources were added to the database, and the database developed was checked for devices not meeting the inclusion criteria. Inclusion of the devices in the database was discussed by two researchers for each device. Devices were excluded if they were static devices, were intended to be used therapeutically, or were exclusively designed to train arm function, or if they facilitated hand function only or were used as manipulators (Figure 1). Articles, installation guides, catalogues, and web pages of distributors and manufacturers were used to extract information about those devices identified. The following information was entered into the database:
Name of the device
Year of development
Intended use (generic/dedicated use: activity)
Mounting (to an immovable object/to a movable object/body-worn/on a base)
Actuation
Functionalities
Interface
Manufacturer/developer
Availability
Picture
Commercial availability (October 2012)
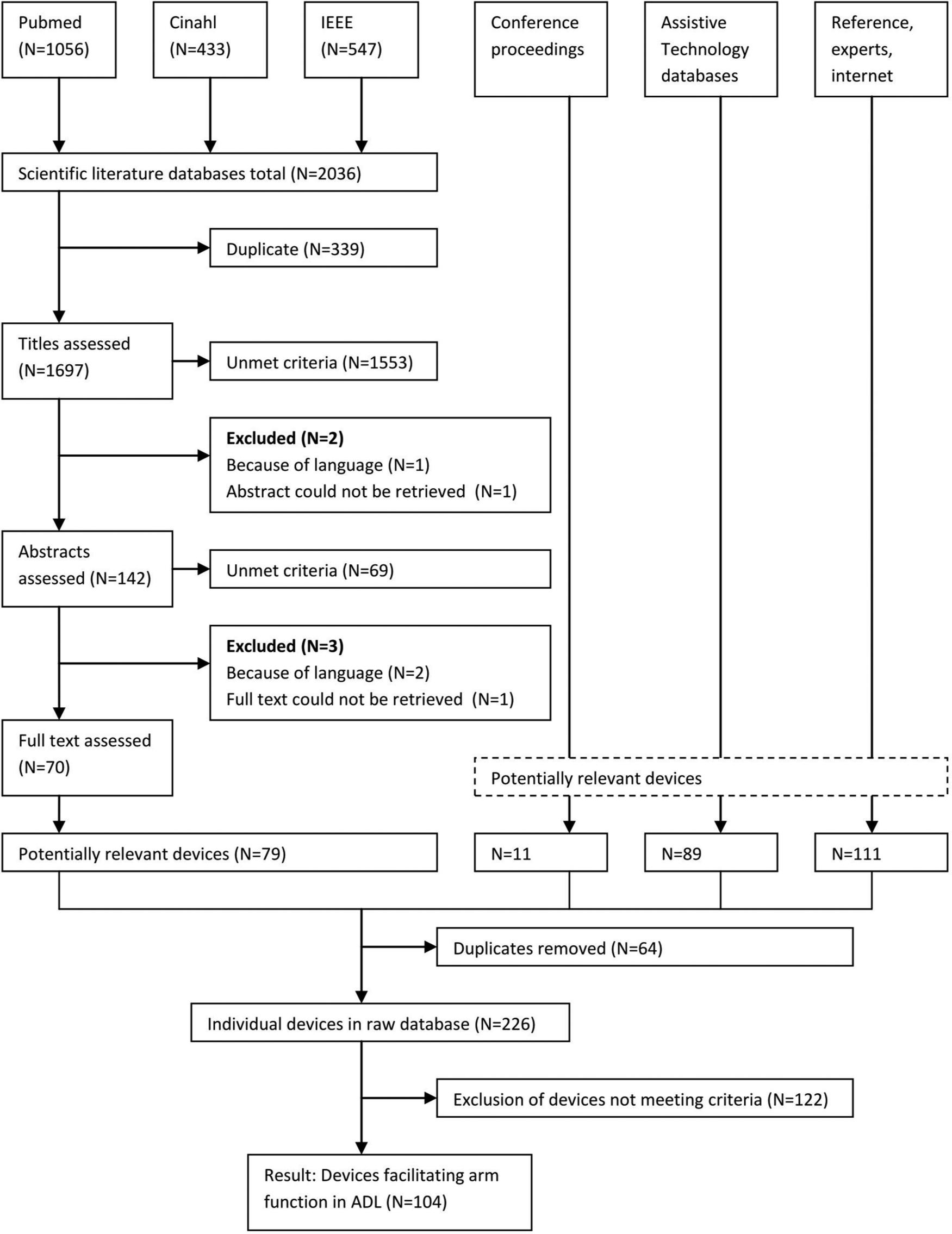
The process of selecting dynamic arm supports.
Devices were regarded as being commercially available if the device appeared on a website of a distributor or manufacturer. In successive rounds, dynamic arm supports were divided up on the basis of differentiating characteristics and functionalities. Categorization was regarded to be successfully completed when all dynamic arm supports without exception could be divided into a limited number of categories and when consensus was reached on categorization between all experts in the panel. The panel consisted of an occupational therapist, a psychologist, a physician, a movement scientist, an electrical engineer, and a biomechanical engineer.
Results
The scientific literature databases yielded 1697 singular references. Cohen’s kappa for agreement regarding the title selection was 0.439 for reviewers L.H. and G.G., 0.248 between M.S. and L.H., and 0.171 between G.G. and M.S. Cohen’s kappa regarding the abstract selection was 0.462 between G.G. and L.H. Seventy articles were read, and 79 devices in total were mentioned or referred to directly in the articles. The raw database of devices consisted of 226 entries, and after screening for the exclusion criteria, 104 devices were regarded as dynamic arm supports (Figure 1). The first known year of development was 1936, and the latest reported development was from 2011.
A two-level categorization of identified dynamic arm supports was based first upon a technical perspective and second upon a functional perspective. The technical categorization elaborates on the categories identified by Cardoso 6 and Rahman 5 and is based upon the external energy required to operate the device. Analysis of the method of actuation of these 104 dynamic arm supports revealed three major groups: nonactuated devices (39 products) that do not require external energy input to function and do not have the ability to store energy but must be powered by the user; passively actuated devices (24 products) that do not require external energy input but have the ability to store potential energy and need to be powered by the user to a lesser extent; actively actuated devices (34 products) require external energy input and can have the ability to store energy. These devices do not need to be powered by the user for operation, or only minimally so. A fourth and distinct category of devices is those using the functional electrical stimulation principle (seven products). These are regarded as a separate group because the working principle is completely distinct from the other devices.
Further categorization based upon functionalities resulted in three groups: facilitation of arm function by tremor suppression, facilitation of anti-gravity movements, and assistance of specific joint motion. For the functionality assistance of specific joint motion, it is important to distinguish between two types of devices, the exoskeletons and end-effectors. Exoskeletons are devices that resemble the structure of the human upper limb. Joints of the exoskeleton are aligned to the user’s joint and are attached to at least two segments. This offers the possibility to control each joint separately. End-effectors can be recognized as devices attached to the upper limb at one single point, which is often the lower arm in dynamic arm supports. The joints of these devices are not aligned with the joints of the upper extremity. Isolated motion at a specific joint is not easy to generate, since motion of the end-effector can cause a combination of movements in the elbow and shoulder. 7 Therefore, the functionality assistance of specific joint motion is only applicable to exoskeletons (Table 1).
Categorization and functionalities of dynamic arm supports.

ADL: activities of daily living; gray: functionality met by the device; *: no information available. For assistance of specific joint motion—P: passively actuated; N: nonactuated, only indicated if actuation of that joint is not in accordance with the device’s classification.
Commercial availability was determined in October 2012.
Possibly the Case Orthosis and the Case Research Aid, Mark I are the same device, but since they are described differently,27,28 they are regarded as different devices.
Provides the possibility to passively suppress tremor.
The four main categories (nonactuated, passively actuated, actively actuated, and FES), the different functionalities, the actual devices, and the underlying working principles will now be described in more detail. Devices are either developed for a specific activity, for example, devices that help in eating or devices that are developed for general ADL task performance. These are called generic devices (Table 1).
Nonactuated devices
Nonactuated devices are simple devices that can improve arm function during ADL (Figure 2). They fulfill the following functionalities: tremor suppression, anti-gravity support (enabling horizontal movement), and facilitation of flexion and/or extension of the elbow. Anti-gravity support for movements in the horizontal plane is provided by enabling low-friction movement in combination with physical support of the lower arm. This is the case in 30 of the 39 nonactuated devices.

A nonactuated dynamic arm support. The Standard Mobile Arm Support (MAS) (JAECO Orthopedic).
Except for one device, all devices in the group of nonactuated devices are end-effectors attached mostly to the forearm. A forearm through acting as a seesaw is a mechanism often encountered within the nonactuated devices. This mechanism enables either elbow flexion or extension. As these devices are end-effectors, changing the position of the forearm results in movements in the shoulder as well. Application of this mechanism could be seen among the earliest devices such as the Balanced Forearm Orthosis, 9 developed around 1965, the C-clamp feeder, the Barker feeder, the foot-operated feeder, and the corset-based feeder. Apart from the first example, all of these were developed by the Georgia Warm Springs Foundation. 1 Several of the devices which are currently available still apply this mechanical principle, such as the M.A.G. horizontal orthosis (Proteor) and the Jamie (Focal Meditech). For devices having a similar design as the Balanced Forearm Orthosis, which is among others described by Chyatte, it has been reported that the design and adjustments on the device can bring about movements in the shoulder by supporting shoulder flexion, abduction, adduction, and internal and external rotations. 9
The Stanmore flail arm orthosis (Liberating Technologies) is regarded as a nonactuated exoskeleton that enables the user to perform elbow movements. The devices need to be operated by the sound hand. The Thomas steady arm and the action arm (RT Machined Specialties) are devices that aim to suppress the tremor during upper extremity movement. This is accomplished by increasing the resistance of motion.
Many nonactuated devices are dedicated to specific activities such as tabletop activities, for example, the Zonco Arm Support (ZoncoArm) and the Ergorest (Ergorest), or to feeding assistance, as in the case of the Foot-operated feeder. 1 The Corset-based feeder is an example of a body-worn device, 1 but most nonactuated devices are intended to be fixed to a mobile object such as a wheelchair or to be fixed to an immovable object.
Passively actuated devices
Twenty-four of the 104 devices are passively actuated devices featuring mechanisms to store potential energy within the device (Figure 3). Again, they may facilitate arm function during ADL tasks by providing three functionalities: manipulation of specific joints, support of anti-gravity movements, and tremor suppression.

A passively actuated dynamic arm support. The TOP/HELP (Focal Meditech).
Adding counterweights, springs, or elastic bands can passively compensate for the impact of gravity on the arm and results in a balanced arm if these are properly adjusted. Counterweights are frequently applied in suspension-type devices, of which the Musgrave orthosis (1984) 15 is one of the earlier examples. This mechanical concept is still used, for example, in the Mobility Arm (Nitzbon). In addition to counterweights, springs or elastics can be used to generate a vertical force to balance the arm, a mechanism which is used in the WREX (JAECO Orthopedic) and the Armon Edero (Microgravity Products) among others. The devices listed here that compensate for the effects of gravity are all end-effectors, implying that forearm movements generated by this compensation result in a combination of movements in the shoulder and the elbow.
Joint motion of the elbow and pronation/supination can be accomplished with passively actuated exoskeletons. For example, elbow motion can be achieved passively by springs, which is the case in the Wilmer Elbow Orthosis (Ambroise) where an abduction or anteflexion angle of 30° results in full elbow flexion. The Constant Elbow Torque Orthosis assists in pronation. 14
Three devices passively suppress tremor by damping involuntary (e.g. spastic) movements. The Comfy Feeder II (Comfy Splints) uses a spring which results in an automatic rise of the lever in the direction of the mouth after depression of the spoon. The Nelson (Focal Meditech) uses viscous fluid to absorb energy and consequently smoothens out high-frequency and spastic movements. The Neater Eater (Neater Solutions) uses both principles. These tremor-suppression devices were all developed to assist in feeding and are fixed on a base to be placed on the table while eating.
Apart from the three tremor-suppression devices, none of the other passively actuated devices are designed to assist in specific activities. Additionally, the majority is designed for fixation to an immovable object or a movable object and only four can be attached to the user.
Actively actuated devices
Actively actuated devices have the same functionalities as the other two categories but differ in the sense that, due to external energy, they are not dependent on pre-stored mechanical energy and are thus able to exert greater forces or control movements more precisely (Figure 4). Actively actuated devices are more difficult to categorize further according to their functionalities, because their energy supply allows them to provide more than one function. Actuation mechanisms of these devices can be, for example, pneumatic, electric, or hybrid.

An actively actuated dynamic arm support. The Armon Ayura (Microgravity Products).
A relatively high number of exoskeletons was encountered in the group of actively actuated devices (N = 17), and these devices are able to control many joints of the upper limb directly, that is, the shoulder, elbow, wrist, and hand, as well as pronation and supination. An early attempt to control individual joints actively was made with the Rancho electric arm, 24 which allowed the user to manipulate the shoulder, elbow, and wrist independently as well as enabling pronation and supination and hand motion. In order to move joints independently and actively, joint motion needs to be controlled. The Rancho electric arm therefore uses seven tongue switches. The PODEUM made use of myo-electrical input from the eyebrows to allow amyotrophic lateral sclerosis patients to open and close the hand and to control elbow extension. 33 More recent developments involving direct joint motion are the Exorob-7 22 and the SUEFUL-7. 18 Control by electromyography (EMG) is planned for both of these, whereby the SUEFUL-7 will have force sensors as additional controls. However, neither development is commercially available at the moment.
Additionally, actively actuated devices can support anti-gravity movements while allowing horizontal movement, a solution encountered in the end-effector devices. This can be achieved in two different ways. One way is the combination of passive designs with external energy, which can be achieved, for example, by actively adjusting springs. This results in the possibility of adjusting the balance as in the case of the Armon Ayura (Microgravity Products) and the recently developed Darwing (Focal Meditech), both of which are commercially available. Operation of these devices can often be accomplished with one switch.
The second mechanism for providing active gravity compensation is to simply elevate the forearm. One of the earliest applications was the Musgrave orthosis (1984); a suspension dynamic arm support in which the counterweight was substituted by a 12-V motor. 15 This mechanism is still applied, for example, in the TOP/HELP electric (Focal Meditech) and the electric variant of the Neater Arm Support (Neater Solutions). Both devices are commercially available. Elevation of the forearm is often carried out with just one switch control. As for the nonactuated and passively actuated end-effectors, also in these devices, a combination of motions in the shoulder and elbow occur, due to the changing position of the forearm.
Actively actuated devices that aim to suppress tremor are the Controlled Energy Dissipation Orthosis 36 and the WOTAS. 37 The WOTAS is able to suppress tremor in the elbow and wrist and in pronation and supination.
FES
The final category of dynamic arm supports is those that use functional electrical stimulation. During this review, seven devices were encountered that provide this specific function. In general, FES are applied to restore neurological function. Compared with the three previously mentioned categories, FES are mostly applied to upper motor neuron disorders. These devices can make use of a commercially available device such as the Freehand or the FESMate, expanded with elbow extension, shoulder flexion, wrist extension, and/or pronation and supination.45–47,52 When the contractile force of the muscles is insufficient, a Balanced Forearm Orthosis, suspension devices, or splints are used.45,47,50
Discussion
The aim of this review was to investigate dynamic arm supports which have been developed and to categorize these in order to provide a basis for future developments. The overview provided gives insight into the devices developed and those available on the market. The number of devices identified was much higher than expected and it appeared to be possible to divide them into a relevant categorization. This categorization is of limited complexity while the devices could be categorized without difficulty. Striking is the limited diversity in the functioning principles of the devices.
Three groups differing in actuation method were identified as well as one FES group. The intended target population of FES is different from the other three categories in respect of the affected function that causes the decreased upper limb function. The implications of this research will therefore not be directed at FES. In contrast to the classification applied by Rahman 5 and Cardoso, 6 this study divided the group which they defined as passively actuated or body-powered into two groups: nonactuated and passively actuated dynamic arm supports. The nonactuated devices are mostly simple devices but they do support arm function in ADL.
Within the actuation categories, the devices could be categorized functionally, and technical solutions related to functionality could be distinguished. The devices developed only have a limited number of functionalities related to a limited set of technical designs, for example, the seesaw that assists in the flexion and extension of the elbow in nonactuated devices. Springs and counterbalancing suspension devices are extensively used in passive devices to facilitate vertical movement. Only a few devices were encountered that tried to solve the problem with a different mechanism, such as the Mobile Arm Support developed by Radulovic. Radulovic developed an active, body-worn, pneumatic system that counterbalances the weight of the arm and features passive elbow flexion as the result of active shoulder abduction. The idea behind this was that, in everyday life, abduction of the shoulder and flexion of the elbow are generally performed together. 44
The minority of devices, 23 out of the 104 (7 FES), are devised to be mounted onto the human torso. Because the human arm is fixed to the torso, it seems ideal to develop a body-worn dynamic arm support, but considering the weight of the devices developed, especially of active dynamic arm supports, these are mostly too heavy to be worn by the user, who is often already in a weakened state.
All of the commercially available active devices in this study are end-effectors. These devices can be controlled mostly with one switch to elevate the arm or to adjust the tension in a spring. A manual switch control is standard in many of these devices. However, virtually all body movements can be used as inputs for operation, for example, eye or finger control, although these interfaces are not intuitive. Additionally, residual arm function does not need to be used to operate the device, although in devices that actively adjust spring tension, choosing the amount of gravity compensation allows a choice regarding exploitation of the user’s own arm function. Recent research has identified the importance of using residual arm function in order to prevent muscle deterioration. 53 Using residual arm function to control future designs would increase the amount of movement of the upper extremity on the one hand, and the intuitiveness of the interface on the other; movement intention would result directly in arm movement. The application of sensor technology has already been explored by Rahman et al. 19 among others, although this device is not currently commercially available.
Exoskeletons offer the possibility to control different joints directly as well as more precise control of motion. However, as they need to mimic the complete arm, they are mostly more conspicuous, and historically, they have required more complex interfaces because every joint has to be controlled manually. Nevertheless, recent developments have tried to make dynamic arm support control easier by developing advanced control systems to make the interfaces more intuitive. EMG control has been implemented, for example, in the SUEFUL-7, but EMG control is difficult to achieve due to interference from the motion of other joints, retrieving signals, intra-personal differences, and connection of the device. 54 To result in successful use, these devices need to have intuitive interfaces such as force sensors, EMG, or other smart solutions, since controlling different joints manually is too complex for the user. Some active exoskeletons for training purposes are commercially available, and while these devices might be beneficial for this purpose, 7 these devices are not ready to be used as assistive devices in the home situation yet or exoskeletons might be less suitable than end-effectors when used as assistive technology.
It appears that the balance between the functional benefit of a device and the burden of use is still not ideal. No device will be as efficient as the healthy human arm, but it seems there is still potential for improving this balance. Nevertheless, the efforts of past developers deserve credit and future developments should build on the legacy of these earlier devices rather than reinvent the wheel. However, for developments to become effective, they have to be introduced on the market first. The majority of the devices developed since 2000 have never been used in daily life by the target population for whom they were developed. Particularly in comparison with the nonactuated and passively actuated devices, a low percentage of the actively actuated devices were commercially available in October 2012. Possible explanations might be that their production costs are higher, they cannot be used in the home situation yet, due to safety issues or their size, or these devices still have an unfavorable cost–benefit ratio in terms of functional gains, and effort and appearance. Maybe more effort should be put into actually bringing devices to the market alongside new innovative developments.
The burden of the devices mentioned in this review was not measured but derived from the different interfaces that were used and the size of the devices. Nor does this review provide insight into the actual use of devices, their effectiveness, or side-effects. This study gives insight into the device’s functionalities, which are mainly derived from technical descriptions of devices. This study, however, does not give insight into the functional benefits for the patients, which is reported as an indicator for successful use.55,56 Therefore, it would be useful for future developments to gain more knowledge regarding those factors that lead to successful or unsuccessful use of the devices. To the best of our knowledge, no systematic review has been performed on this so far. This is remarkable in light of the studies performed on the effectiveness of upper extremity rehabilitation robotics.57–59
The results of this study can primarily be used for future developments by developers and researchers, but also by clinicians such as occupational therapists to increase their awareness of the number and possibilities of currently available devices. Due to the different names devices have been given, their function might not always be clear. It is not the case that devices with different names are different in, for example, function or structure. Why devices are called orthoses, arm supports, or exoskeletons did not become clear from the results of this study but may be due to geographical differences or different fields of development. The terminology could be clarified by developers and manufacturers by giving the device the correct name. Retrievability in databases as well as recognition by clinicians would be improved by the use of the term “dynamic arm support” to describe these devices.
Study limitations
Different sources were examined in order to collect the results presented in this article. Databases on assistive technology yielded those devices available on the market, whereas scientific literature focused on new developments. Devices developed many years ago were found through reference retrieval. Some devices may have been missed in this review but consultation with many sources gave a wide range of products, enabling them to be classified, and therefore, missing some products would probably not have led to a different classification. The agreement between the reviewers was calculated for title assessment and abstract assessment. Agreement was low in all cases, which could imply that some relevant articles were missed. However, the total score of 2 necessary for inclusion, meaning one reviewer was sure or that two reviewers were in doubt, implies a rather high acceptance rate, which gives more certainty that only a few relevant titles were excluded. For some devices, especially older devices, little information could be found, and product information sometimes had to be retrieved from just a few sentences of text and a picture. Commercial availability was extracted from websites of distributors and manufacturers. Due to information that may not be up to date on websites or could not be found, devices might have been listed in this article as being commercially available, while in fact they were not and the other way around.
Conclusion
Many attempts have been made to help people with upper extremity limitations in daily life by means of dynamic arm supports. It was possible to categorize these devices into a categorization of low complexity. Although many devices have been developed, those that disappeared were succeeded by similar devices in functionality and technical design. There is still need for new devices since new devices are currently being developed and there is also room for improvement. Interfaces could be more intuitive; devices either have many functionalities and are big or difficult to control or are easy to control, but not very functional in the performance of ADL tasks. Ultimately, developments should aim to improve the balance between the functional benefit of a device and its burden of use as well as stimulating use of residual muscle strength in the user.
Footnotes
Appendix 1
Acknowledgements
We would like to acknowledge M. Spreeuwenberg for her contribution to the scoring of the titles retrieved from scientific literature databases.
Declaration of conflicting interests
Of the authors, only D. van der Pijl has a commercial interest in the devices mentioned in the article as he is an employee of Focal Meditech, the SME of which several devices are discussed in the manuscript. He offered his valuable insights to strengthen the content of this article and has, by no means, influenced the content of this article for the benefit of his company.
Funding
This work was supported by the national innovation program Pieken in de Delta. Agentschap NL (grant no. PID 102055), the provinces of Limburg and Brabant.