
Abstract
Background and aim:
Patients with mild to moderate first carpometacarpal joint osteoarthritis report pain, a reduction in pinch and grip strength and hand function. The purpose of this study was to analyze the effect of a custom-made neoprene thumb carpometacarpal orthosis with thermoplastic stabilization on pain, function, grip strength, and key pinch in these patients.
Technique:
A total of 11 volunteer patients participated in this study. All the above-mentioned parameters were evaluated at baseline and also 30, 60, and 90 days after using the splint.
Discussion:
A decrease in pain was observed after 30 days, and this continued to improve during treatment with the splint. After 90 days of using the splint, grip strength was improved. Function and pinch strength also increased significantly and was maintained during the study period compared to baseline.
Clinical relevance
A custom-made neoprene thumb carpometacarpal orthosis with thermoplastic stabilization may be a suitable conservative approach for the treatment of first carpometacarpal joint osteoarthritis.
Keywords
Background and aim
The thumb is responsible for 45%–60% of function of the total hand, with much of this function dependent on the mobility of the first carpometacarpal joint (CMCJ),1–3 and this joint is therefore predisposed to the risk of developing osteoarthritis (OA). 2 Approximately 25%–40% people aged above 55 years have radiologic evidence of OA in this joint,4,5 and patients commonly report of experiencing pain, swelling and joint disorientation, instability, tenderness, stiffness, reduced pinch and grip strength, and compromised hand function.5,6 Surgery is the main approach for management of severe basilar joint OA, whereas physiotherapy, exercise, and splinting are the preferred approach in mild and moderate stages of OA. 7
Splinting or bracing is the main conservative method for improving symptoms in the first CMCJ.8–11 Long thermoplastic splints that cover the wrist and the metacarpophalangeal (MCP) joints significantly limit hand function. 12 Prefabricated shorter neoprene splints have been developed, 13 but long neoprene prefabricated thumb splints have been shown to be more effective in function. 11 Reduced trimlines in splints have also been tried.9,13 According to the literature, neoprene thumb splints are preferred by patients,7,11 but custom-made splints are more suitable.7,13 Therefore the aim of this study was to evaluate a neoprene thumb CMCJ orthosis incorporating a bespoke thermoplastic supportive insert on pain, hand function, grip strength, and pinch strength in patients with mild to moderate CMCJ OA.
Technique
Patients with grade 1 and 2 first CMCJ OA in the basilar joint, who felt pain in this joint, were considered for the study. Inclusion criteria consisted of the following: no deformity in the affected hand, no previous surgery or croton injection during the preceding 6 months, no allergy to splint materials, no existence of other disease that might cause similar pain such as carpal tunnel syndrome (CTS), De Quervain syndrome, Dupuytren’s contracture, arthritis, or fifth and sixth cervical vertebral disk herniation, and no pain or stiffness in the shoulder and glenohumeral joint. All patients who participated in this study signed consent forms. The present study was approved by the ethics committee of University of Social Welfare and Rehabilitation Sciences.
A short neoprene thumb CMCJ orthosis with thermoplastic stabilization was fabricated with neoprene material reinforced with a thermoplastic component (Aquafit NS Stiff—3.2 mm (1/8″), Belgium, Orfit Company) formed in a “U” shape around the CMCJ for stabilization of the joint (Figure 1).

A short neoprene thumb CMCJ orthosis with thermo-plastic stabilization was fabricated with neoprene material reinforced with a thermoplastic component.
The wrist and MCP joints were left free in this new orthosis, which only covered the CMCJ. The thermoplastic component was custom-molded to the patient’s hand and placed into a pocket in the neoprene, which was subsequently sewn and closed. The neoprene orthosis was constructed in 4 sizes and included a VELCRO® closure. The thermoplastic component was placed in the specific area in the neoprene splint (Figure 2). Patients were instructed to use orthosis when they experienced symptoms and for activities of daily living. The patients used this orthosis for a maximum of 3 months.

The completed splint.
An experienced orthotist performed all the tests outlined in this study, which were measured at baseline and after 30, 60, and 90 days. Pain, function, grip strength, and pinch strength were the selected outcome measures. A 100-mm Visual Analogue Scale (VAS) was used to measure pain in this study. The Disability of the Arm, Shoulder and Hand (DASH) questionnaire was used to evaluate function in this study. Grip strength and pinch strength were evaluated using a dynamometer (Jamar Hydraulic Hand Dynamometer model; PC 5030 J1) and pinch gauge (Jamar Hydraulic Pinch Gauge model; PC 7498-05). The mean of three tests of both grip and pinch strength of the affected hand was used for analysis. There was a short period of rest allowed between each test.
Statistical analysis
A repeated measures analysis of variance was used for intergroup comparison over time in 30, 60, and 90 days to evaluate the effect of using the orthosis on the primary outcome measures during the duration of the study period (i.e. pain, function, grip strength, and pinch strength). SPSS 16 was used for data analysis. The significant level considered was α = 0.05.
Results
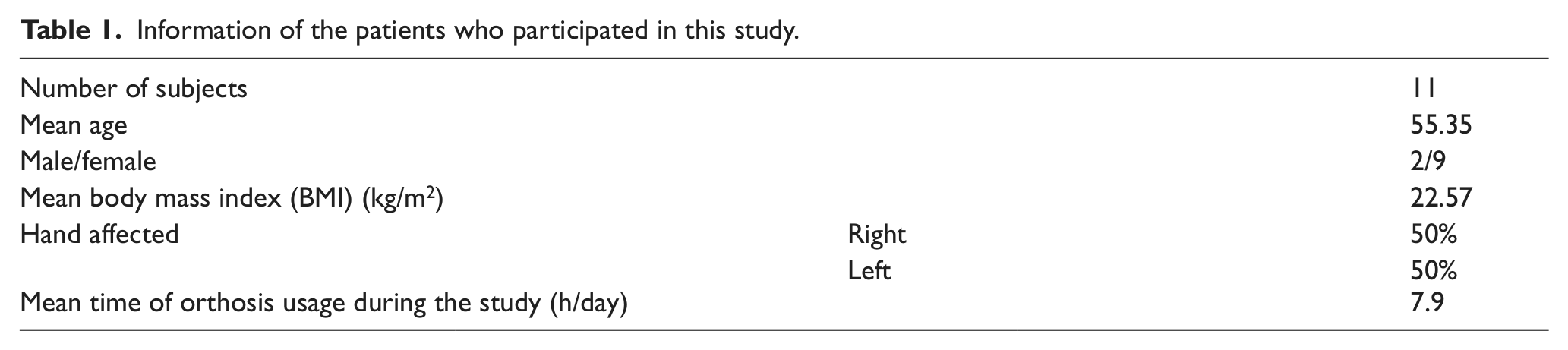
Eleven patients with grade 1 and 2 of first CMCJ OA participated in this study (Table 1).
Information of the patients who participated in this study.
A reduction in the VAS pain scores was demonstrated (Table 2). In the intragroup comparison, using an orthosis decreased pain in patients 30 days after orthosis provision compared to baseline (p = 0.003), and this reduction was maintained up to 90 days after wearing of orthosis commenced (p < 0.001). There was also significant improvement in DASH scores between baseline and 30, 60, and 90 days after wearing orthosis. A similar result was observed in grip and pinch strength after 30, 60, and 90 days of orthosis use from baseline (Table 3).
Mean (SD) of outcome measures in first CMC OA patients at baseline and also at 30, 60, and 90 days following application of an orthosis.
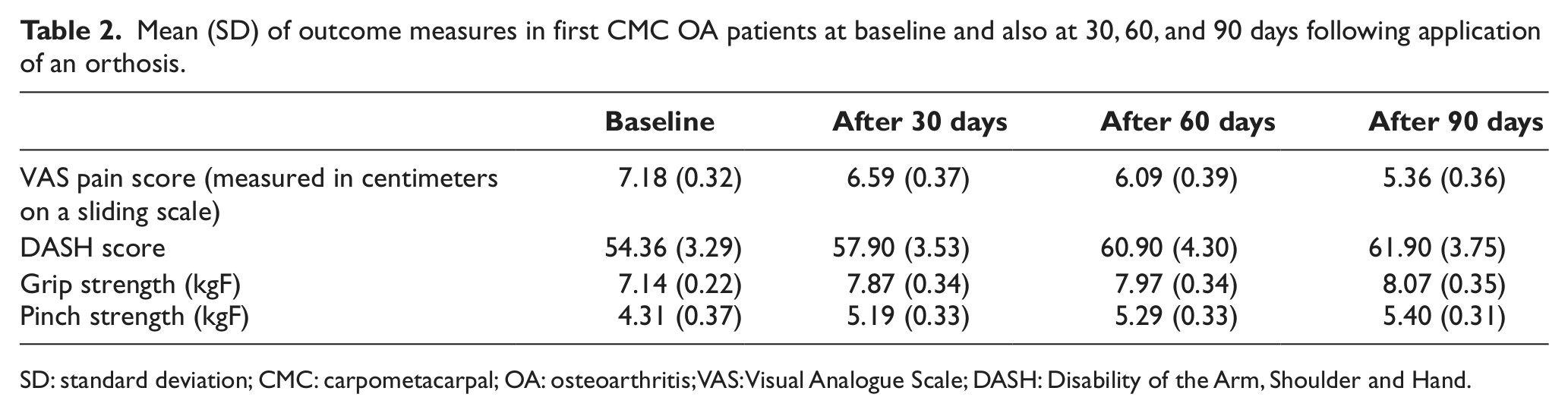
SD: standard deviation; CMC: carpometacarpal; OA: osteoarthritis; VAS: Visual Analogue Scale; DASH: Disability of the Arm, Shoulder and Hand.
Statistical significance (p values) between baseline scores and those at 30, 60, and 90 days following orthosis use.
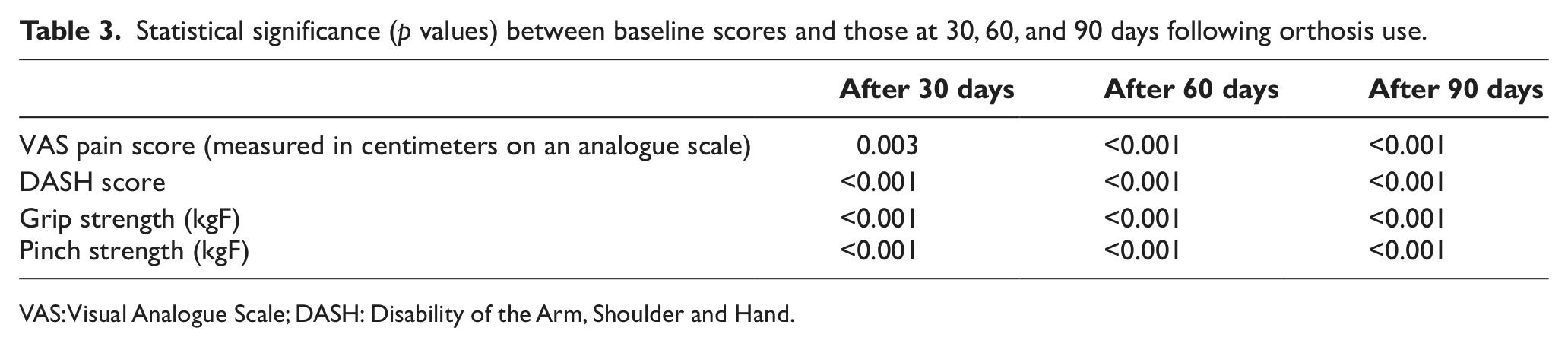
VAS: Visual Analogue Scale; DASH: Disability of the Arm, Shoulder and Hand.
The significant differences were maintained between 30 and 60 days after wearing orthosis according to pain, function, and pinch strength (Table 4) and also between 60 and 90 days during orthosis use. However, grip strength demonstrated no significant difference for the duration of orthosis use, although it was initially improved.
Statistical significance (p values) between outcome measures between 30 and 60 days, 30 and 90 days, and 60 and 90 days following orthosis use.
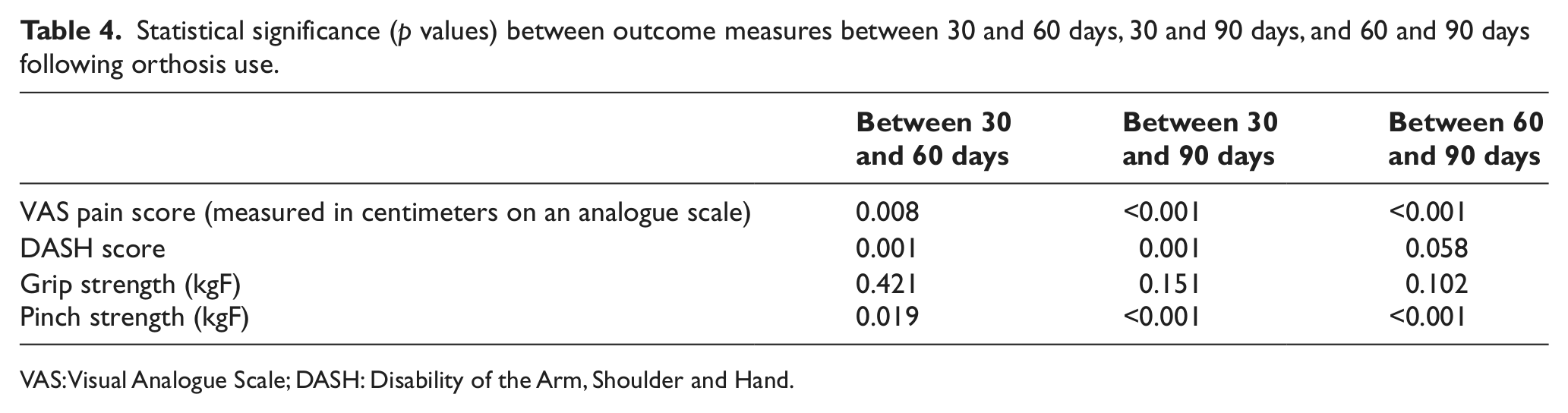
VAS: Visual Analogue Scale; DASH: Disability of the Arm, Shoulder and Hand.
In comparison of orthosis intervention on pain, pinch strength, function, and grip strength in the period 60–90 days after orthosis use, there were statistically significant differences observed in pain and pinch strength (Table 4).
Discussion
The results of this study showed that the orthosis could produce a decrease in pain and an increase in function, grip strength, and pinch strength. The orthosis improved pain as compared to baseline after 30, 60, and 90 days after treatment started. Pain may be reduced by stabilization of the joint and/or decreasing inflammation of joint as a consequence of the warmth created by the orthosis. In addition, the neoprene structure of the orthosis may have increased proprioception for the patient.
The improvement in pain levels associated with using the custom-made neoprene thumb CMCJ orthosis with thermoplastic stabilization can therefore result in improvement of function in patients with first CMCJ OA. When the thermoplastic component of the orthosis was molded on a patient’s thumb, a theoretical corrective force was performed to position the thumb in a more anatomical position and to help prevent dislocation of the first CMCJ.
Carreira et al. 2 reported no change in pinch and grip strength with a custom-made thumb orthosis on the first CMCJ OA patients. On the contrary, Weiss et al. 11 reported that both a prefabricated orthosis and custom-made orthosis increased the pinch strength. McKee et al. 13 demonstrated that pinch strength was increased compared to baseline by using two types of orthoses in patients with first CMCJ OA.
The main limitations for this research were lack of any questionnaire that assesses only hand function and the small number of subjects included in the study. Muscle atrophy was not evaluated along with any contraindications, which may become apparent in a larger and longer study. In this study, we evaluated only the new orthosis compared to baseline. Comparison between the new orthosis and conventional prefabricated and custom-molded thumb splints are now required to give clear treatment recommendations for OA of the first CMCJ.
Key points
Using the custom-made neoprene thumb CMCJ orthosis with thermoplastic stabilization demonstrated reduction in pain and increased function, grip strength, and pinch strength in patients with mild to moderate first CMCJ OA during activities of daily living.
A short splint still provided relief in symptoms and would not have restricted fingers of MCP joints.
It is important to manufacture the thermoplastic component to fit individually to each patient.
This technique may be easily replicated to the benefit of patients with CMCJ OA.
Footnotes
Acknowledgements
Essential materials and resources were provided by the Department of Orthotics and Prosthetics of University of Social Welfare and Rehabilitation Sciences.
Conflict of interest
The authors did not have any conflicts of interest with regard to the study presented in this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.