
Abstract
Background:
Pain, reduced grip strength, loss of range of motion, and joint stiffness, leading to impaired hand function, and difficulty with daily activities are documented symptoms of first carpometacarpal joint osteoarthritis. Splinting is a common type of conservative treatment for this injury.
Objectives:
The aim of this study was to evaluate the effect of custom-made thumb splints on pain, function, grip strength, and key pinch in patients with first carpometacarpal joint osteoarthritis.
Study Design:
Quasi experimental.
Methods:
Patients with first carpometacarpal grade I and II osteoarthritis (n = 18) participated in a repeated measure study. The patients all wore custom-made thumb splints. All parameters were measured at baseline, and also after 30, 60, and 90 days from initial supply. A visual analogue scale, along with a disability of the arm, shoulder, and hand questionnaire, a dynamometer and pinch gauge were used to assess pain, function, grip strength, and pinch, respectively.
Results:
After 60 days of splint usage, grip strength was improved. However, a reduction in pain was demonstrated after only 30 days and this continued to improve with time. Function and pinch strength also increased significantly and continued to do so during the study period when compared to baseline.
Conclusions:
The use of a custom-made splint for patients with osteoarthritis of the first carpometacarpal joint produced decreased pain and increased grip strength, pinch strength, and hand function.
Clinical relevance
Custom-made splints may be recommended for the treatment of first carpometacarpal joint osteoarthritis.
Background
Osteoarthritis (OA) in the hand is a chronic joint disease which commonly affects one or more of the joints of the thumb and fingers in the upper extremity, 1 and is a major cause of disability and illness. 2 In the hand, after the distal interphalangeal joints, the most common site of OA is in the first carpometacarpal (CMC) joint (otherwise known as the trapeziometacarpal (TMC) or basilar joint). 3 Estimates of the prevalence of hand OA have been reported as being between 13% and 26% and are higher in women.1,4 Pain, reduced grip strength, loss of range of motion (ROM), and joint stiffness, leading to impaired hand function, and difficulty with daily activities are documented symptoms of first CMC joint OA.5,6 Laxity of the volar oblique ligament is the primary cause of OA in the first CMC joint. Subluxation occurs when this joint experience stressed situations, resulting in inflammation and joint destruction. A thenar muscle contraction moves the first metacarpal forward. The loosening of the posterior capsule with an activated pinch shifts the upper end of the metacarpal to a more posterior position. These joint changes cause stiffness, limited first CMC joint ROM, and pain associated with basilar arthritis. 7 Muscle atrophy and loss of power are commonly seen symptoms that cause reduced functional ability among patients, and 74% of patients with thumb CMC OA have difficulty in performing their activities of daily living.7,8 Different treatments offered for this disease include the use of drugs, surgery, or conservative approaches.9,10
The primary goals of conservative treatment are to reduce pain, to improve the joint space position and improve thumb performance, and to produce increased grip strength and pinch.11,12 An improvement in all of these objectives could therefore result in an increase in the ability to perform activities of daily living and an improvement in the quality of life of patients with OA of the first CMC joint. The use of splinting is one conservative method routinely used.9,10 The first aim of splinting is to stabilize the first CMC joint of the thumb and to prevent its movement during activities such as catching and pushing. 7 Previous studies which have investigated the efficacy of splints for treatment of symptoms associated with OA of the first CMC are scarce, but a number of researchers have reported that many rheumatologists recommend their use, although few studies have been published on the subject, especially when reporting the use of an orthosis for the first CMC joint OA. 13
This joint is the most common site upon which surgery is performed in the upper extremity, 14 but many patients also suffer from chronic pain and instability after surgery.15,16 However, conservative approaches appear to be more effective than surgery on treatment in the early stage of OA. McKee and Eason-Klatt 16 in their study demonstrated that wrist immobilization may cause both fatigue and over-use syndromes. Accordingly, the authors recommended the use of a custom-made short thumb splint manufactured from low-temperature molding material for the treatment of CMC joint OA.16,17
Patients with first CMC joint OA of the hand experience a loss of manual ability and grip strength. Freedom of movement and stability are two important functions of the first CMC joint, 18 and because 45% of activities of daily living involve this joint during upper limb activities, it is considered one of the most important hand joints. When pain relief is provided increased function may be expected. 3 This effect could be due to increased joint stability and proprioception. However, whereas in a randomized controlled trial by Carreira et al. 3 splints designed for patients with TMC OA did reduce pain levels, they did not alter function, grip strength, pinch strength, or dexterity. Previous studies in this field have demonstrated similar results.16,19 In addition, Weiss et al. 20 reported that a prefabricated splint demonstrated better performance than a custom-made splint in function improvement for this patient group. The study by Weiss et al., which compared the effects of two types of splint over a 1-week period only for each, did not use a valid score system to assess improvement in symptoms, and therefore, more evidence is needed as to their efficacy. The evidence in the literature therefore suggests that agreement on the most effective splint design does not yet exist for this condition.19,20 Based on the conservative nature and low cost of splinting, it has been recommended that patients with grade I and II OA of the first CMC joint, otherwise known as the TMC joint, use a specifically designed splint. 21
The objective of the present study was therefore to assess the effect of a low-temperature moldable thermoplastic custom-made thumb splint on pain, function, grip strength, and key pinch in patients with grade I and II OA of the TMC joint.
Methods
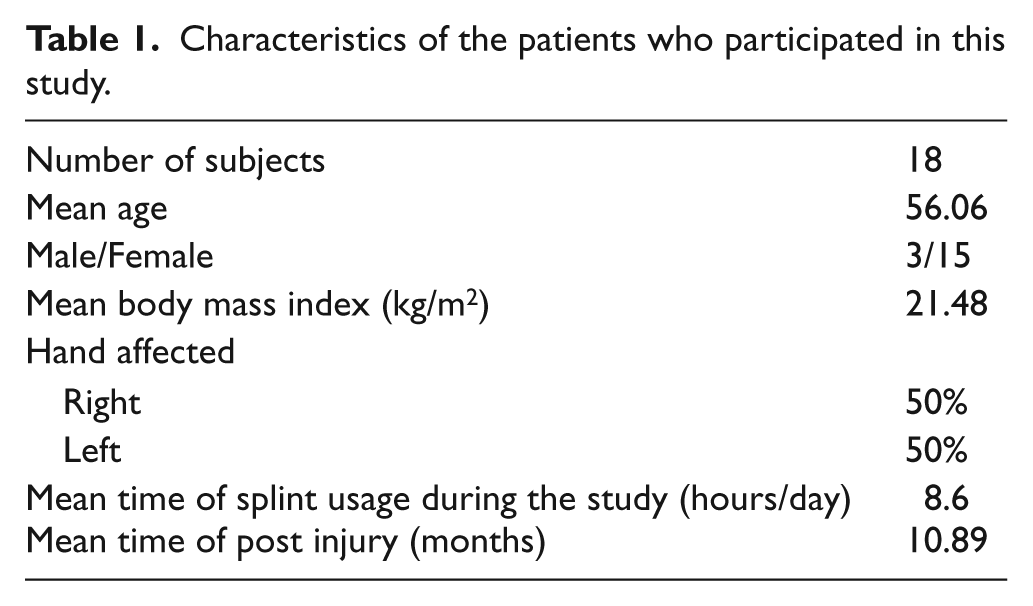
Volunteer patients who participated in the study (n = 18) were referred with a diagnosis of grade 1 and 2 thumb carpometacarpal joint OA by an orthopedic surgeon to the Orthotics and Prosthetics department of University of Social Welfare and Rehabilitation Sciences. Volunteer patient details are shown in Table 1.
Characteristics of the patients who participated in this study.
Inclusion/exclusion criteria
Inclusion criteria for this study included clinical and radiological diagnosis of thumb carpometacarpal joint OA grade 1 and 2, of either gender, with pain in the base of the thumb. Exclusion criteria included other deformities of the affected hand, deformities of the distal interphalangeal joint of the thumb, use of a splint on the affected thumb during the previous 6 months, surgery on the studied hand during the previous 6 months, potential allergy to the splint material, an inability to respond to a questionnaire due to communication difficulties or to perform the tests, evidence of injection therapy in the studied hand in the previous 6 months, and presence of additional disease affecting the ipsilateral upper limb (e.g. carpal tunnel syndrome, De Quatrains tendonitis, Dupuytren’s contracture, arthritis, and fifth and sixth cervical vertebral disk herniation). The present study was approved by the ethics committee of the University of Social Welfare and Rehabilitation Sciences. All patients signed consent forms.
Orthotic intervention
The orthosis was designed to stabilize the first CMC joint, while maintaining the pulp of the distal phalange of the index finger free for gripping with the other fingers and leaving the thumb in a functional position with the wrist free from restraint. The wrist was not immobilized as the splint was designed as a thumb spica type brace as recommended in the literature.14,15
A custom-made orthosis was constructed for each subject using 3.2 mm thick low-temperature moldable thermoplastic material (Aquafit NS Stiff—3.2 mm (1/8″), Orfit Company, Inc., Belgium) based on a pattern that matched the dimensions of the patient’s hand. After the splint had cooled, a 3 mm low density Plastazote lining was adhered to the shell, and the splint closed by Velcro® on the patients’ hand (Figure 1).

The custom-made thumb splint used in this study.
Patients received the splint one day following the initial evaluation. The patients were asked to use the splint during activities of daily living and remove them during sleeping, bathing, and in dangerous conditions which would be harmful for the splint material (e.g. when exposed to excessive heat). It was explained how to maintain splint cleanliness and how the splints should be used. Patients were advised to contact the rehabilitation team should they feel any discomfort with the splint.
Clinical test used in the study
All tests were conducted by an orthosist who had been previously trained to administer the tests at baseline, after 30, 60, and 90 days following initial supply of the splint. The primary outcome measures were pain, function, grip strength, and pinch strength.
A visual analogue scale (VAS) ranging from 0 (“no pain”) to 10 cm (“worst pain imaginable”) was also used for pain assessment. The VAS was chosen as it is an accepted method in the literature to measure pain levels of joints in the upper limbs.21–23 The patient announced his or her level of pain according to VAS score using the tip of a pen. In evaluation of pain without the splint, the average pain the patient felt in the previous week without the use of the splint was considered. In assessment of pain with the splint, average pain the patient felt using the splint during the assessment was considered.
Function was measured via completion of the disability of the arm, shoulder, and hand (DASH) questionnaire, which is a comprehensive assessment tool, and is validated to measure function in the upper limbs. It has 30 questions that assess function and symptoms. It includes the following: physical function (21 questions), symptoms of disease (6 questions), and social aspects (3 questions), and two optional modules (4 questions) for workers and athletes.
The DASH questionnaire was answered according to the patient’s experiences in the previous week. If the patient did not have the opportunity to perform one of the activities in the previous week, he or she was asked to estimate the most accurate response. The DASH questionnaire has points from 0 to 96 with the higher scores indicating worse functional capacity.
Grip strength was measured using a dynamometer (Jamar Hydraulic Hand Dynamometer—PC 5030 J1, Patterson Medical Holdings, Inc.). For assessment of patient’s grip, patients were seated with the elbow at 90° and wrist flexion in the neutral position between pronation and supination. Grip strength was considered in kilogram-force (kgf) and the mean results were used for analysis. The mean grip strength was taken from the mean of five tests for the affected hand.
Key pinch was measured using a Pinch Gauge (Jamar Hydraulic Pinch Gauge, model PC 7498-05, Patterson Medical Holdings, Inc.). For assessment of patients’ pinch strength, they were seated with the upper limb in the same position as that adopted for the grip strength test, and key pinch strength was again considered in kilogram-force, and the mean of results were used for analysis. The mean key pinch strength was taken from the mean of five tests for the affected hand.
Statistical analysis
To evaluate the effect of the splints on the primary outcome measures during the duration of the study period (i.e. pain, function, grip, and pinch strength), a repeated measures analysis of variance was used. SPSS 16 was used for data analysis. The significant level considered was α = 0.05. Each patient used themselves as a control.
Results
Based on age, disease duration, gender, and the degree of OA of the affected hand, the patients were homogenous at baseline. The mean of age of the participants was 56.06 years (3 males and 15 females) in the study group. All 18 patients who participated in the study completed all of the assessments. Demographic information of the sample (n = 18) are reported in Table 1.
Comparison of primary outcome measures between 30, 60, and 90 days after commencement of splint use
A reduction in the VAS pain scores when wearing the splints was shown in this study (Table 2). In the intragroup comparison, pain reduced in patients when wearing a splint between baseline and 30 days after splint using (p < 0.001) and continued to reduce up to 90 days after splint application (p < 0.001), demonstrating that the decrease in pain occurred in the first 30 days of treatment and was maintained for another 60 days. There were significant improvements in the DASH scores between baseline and 30 days after splint use (p < 0.001), 60 days after splint use (p < 0.001), and also 90 days after splint use (p < 0.001). There was significant difference noted in grip strengths after 60 days of splint use, but not after 30 days from baseline. Pinch strength when wearing the splint, produced significant intragroup improvements at all the measurement times (Table 3).
Mean (SD) of outcome measures in first CMC OA patients at baseline and also at 30, 60, and 90 days following application of a splint.
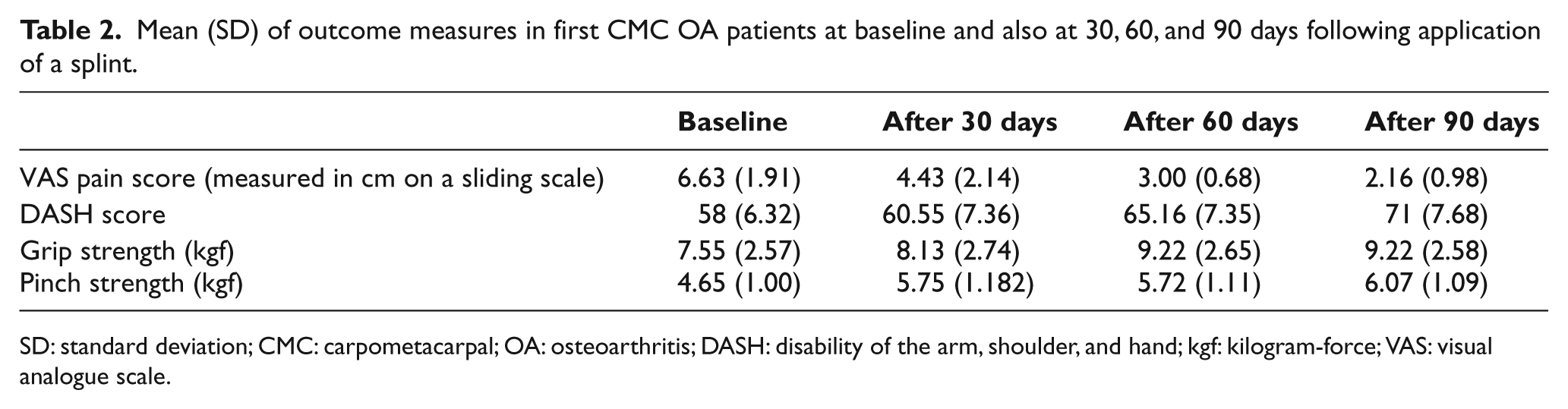
SD: standard deviation; CMC: carpometacarpal; OA: osteoarthritis; DASH: disability of the arm, shoulder, and hand; kgf: kilogram-force; VAS: visual analogue scale.
Statistical significance (p values) between baseline scores and those at 30, 60, and 90 days following splint application.
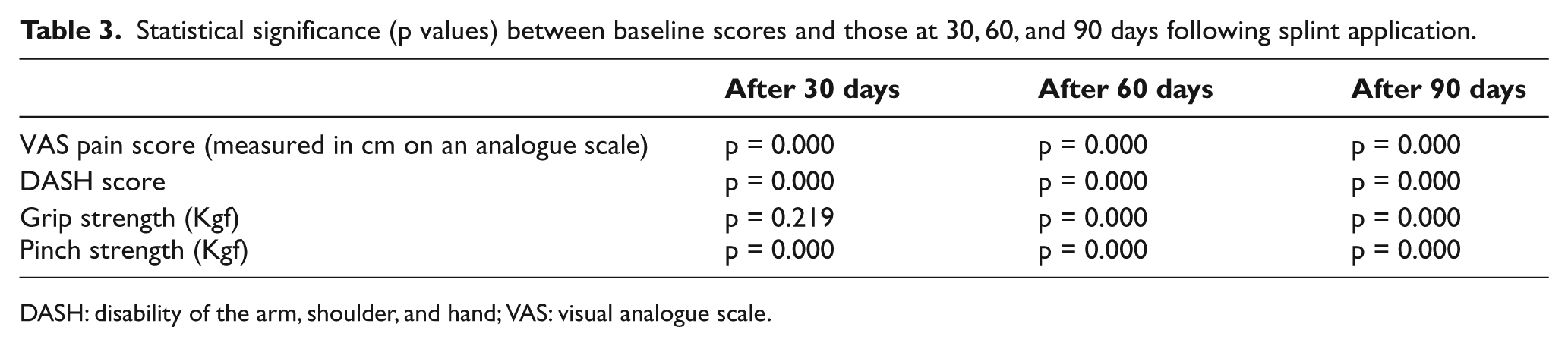
DASH: disability of the arm, shoulder, and hand; VAS: visual analogue scale.
Comparison between outcome measures at 30–60 and 60–90 days after splint use
In the comparison between initial splint application and 90 days after use, there were statistically significant differences in all parameters measured except pinch strength. These significant differences were maintained at 30–60 days after splint use with regard to pain, grip strength, and DASH scores (Table 4) and also at 60–90 days with regard to pain, pinch strength, and DASH scores. This demonstrated a continued improvement during the total measurement period regarding pain, grip strength, and function. However, pinch strength was not significantly increased at 30–60 days after splint application (p = 0.757).
Statistical significance (p values) between outcome measures at 30 and 60 days, 30 and 90 days, and between 60 and 90 days following splint application.
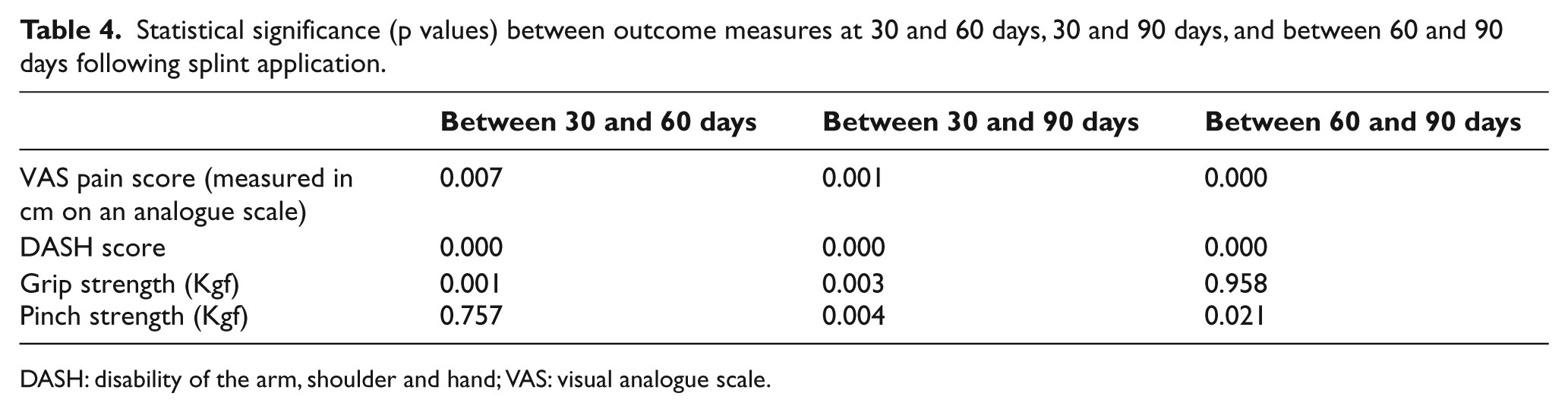
DASH: disability of the arm, shoulder and hand; VAS: visual analogue scale.
When comparing the period 60–90 days after splint use, there were statistically significant differences in pain, pinch strength, and function noted, but again no significant difference was observed in grip strength (p = 0.958) (Table 4).
Discussion
The main goal of this study was to assess the effect of custom-made thumb splints on the symptoms associated with carpometacarpal thumb joint OA over a predetermined period of splint usage. The existence of pain and the problem of experiencing reduced hand function due to lack of pinch and grip strength decreases the ability and increases the difficulty in performing daily living activities. The relevant parameters that were analyzed in this study were therefore pain, function, grip strength, and pinch strength.
In our study, the custom-made splints improved the pain experienced compared to when not previously wearing a splint. This improvement continued during the whole duration of the testing period. Their effect could be due to the corrected position of the osseous and ligamentous structures with the splint applied.
In addition, pain reduction may have occurred for several reasons when using the splint—such as immobilization of the encapsulated joint and decreased inflammation with splinting. Reducing pain has been thought to be an important factor for reducing symptoms of this disease. 10
Function in this study was measured using the DASH assessment, which is a comprehensive and a validated tool to measure function in the upper limbs, including when analyzing hand function.23–27 A DASH score change of 10–14 is considered clinically meaningful. 23 In this study, the mean improvement in the DASH score was 13, which therefore demonstrated clinical as well as statistical significance in this parameter. This parameter also continued to improve throughout the duration of the study. This demonstrates that a short custom-molded splint is capable of improving upper limb function over a 90-day period following initial application. However, an extended study is required over a longer period of time to confirm its longer term efficacy in improving function.
Comparison with other studies
Weiss et al. 20 and Sillem et al. 19 demonstrated similar results to this study regarding pain among patients with OA of the basilar joint. McKee et al. compared two types of CMC joint-stabilizing splints. One splint only covered the CMC joint and another covered both CMC and metacarpophalangeal (MCP) joints, but both reduced pain. 16 Wajon and Ada 22 compared and analyzed reduction of pain using either splintage or physiotherapy as interventions but found no differences between the two interventions.
However, in this study, we evaluated a custom-molded splint for CMC OA patients. The splint increased grip strength compared to the without-splint situation after 60 days of splint use. The splinting provided pain reduction, resulting in an increase in pinch and grip strength. On the other hand, splints can cause muscular atrophy and decrease these parameters. 3 When the splints were molded on the patient’s hand, care was taken to ensure that a corrective force was used to position the thumb in a position to prevent dislocation of the upper end of the metacarpal. However, Carreira et al. 3 announced no change in pinch and grip strength with their custom-made thumb splint on the first CMC joint OA patients. Weiss et al. 20 reported that both prefabricated and custom-made splints increased the ability of pinch strength. McKee and Eason-Klatt 16 reported that pinch strength was increased compared to baseline by two types of splinting, but no significant differences were shown between them.
The correct positioning of the first CMC joint within the splint was thought to be important in this study, but it is not well documented in previous studies investigating thumb splint efficacy in improving hand function. This needs to be investigated further.
Limitations
There were some limitations to the present study that should be reported. A control group was not utilized in this study. Instead, the volunteer subjects served as their own controls. The patients’ comments and perceptions of the effect on their quality of life were also not analyzed. It was not possible to utilize a blinded assessor. However, the results from this study have given the authors confidence to proceed to a future randomized controlled trial study planned over a protracted period in order to further quantify the longer term clinical benefits of custom-made shorthand splints for thumb CMC OA.
Conclusion
During the period of splint usage in this study, the use of a custom-made splint during activities of daily living for patients with OA of the first CMC joint decreased pain and increased grip strength, pinch strength, and function.
Footnotes
Funding
We thank the Research Deputy of University of Social Welfare and Rehabilitation Science for financial support of this research.