
Abstract
Background:
While the effectiveness of orthoses prescribed for tennis elbow has been reported in several studies, the effect of how they may limit movements which aggravate this condition has not yet been explored.
Objective:
The purpose of this study was to evaluate the effect of a new spiral hand-forearm splint that restricts the movement of the wrist and forearm, on grip strength, pain, and function in patients with tennis elbow.
Study design:
Quasi-experimental design.
Methods:
A total of 15 patients with tennis elbow (mean age 43 years) took part in this study. The amount of pain, grip force, and function were compared using a visual analog scale, Jamar dynamometer, and the Disability of the Arm, Shoulder, and Hand questionnaire, respectively. This was performed at baseline and repeated after 4 weeks of splint use. Active motion of the forearm was measured by a goniometer.
Results:
The spiral splint significantly relieved pain and improved function and grip force in patients after 4 weeks of application (P < 0.05).
Conclusion:
The new splint design had a positive effect on the treatment of tennis elbow symptoms which included pain, grip strength, and function. Restriction of rotational movement (e.g. reduction of the supination and pronation of forearm) may have played the main role in this.
Clinical relevance
This new splint design may be considered as a new approach in the conservative treatment and rehabilitation of patients with tennis elbow.
Background
Tennis elbow (otherwise known as lateral epicondylalgia) is also often referred to as epicondylitis or tendinopathy clinically. 1 The condition affects between 1% and 3% of the population 2 with an annual incidence of four to seven cases per 1000 patients. It typically presents in patients aged between 35 and 55 years. 3
Overuse of the extensor tendon due to excessive rotational movement of the forearm causes micro-tears in the origin of the common wrist extensor and extensor carpi radialis brevis (ECRB) and degeneration of the associated collagen. 4 Risk factors include repetitive manual tasks, and the handling of heavy loads (>20 kg) and/or heavy tools (>1 kg). 5 The risk is increased by postural positioning of the arms, whereby they are raised in front of the body. This is coupled with repetitive forearm twisting or rotating motions and by a high gripping force. 6 Tennis elbow is characterized by pain and tenderness on the lateral epicondyle and by a reduction in grip force. 7 The pain is aggravated by resisted wrist extension, 8 and also heavy duty hand function during work related activities, sporting, and daily activities. 9
Excessive loading of the common extensor origin, 8 the area where the maximum tensile forces occur during wrist movements, are linked as an underlying cause. 10 In particular, this excessive loading affects the ECRB tendon while gripping with forearm supination/pronation and wrist extension during daily activities. 11 Decreasing forces on the origin of the ECRB is perceived to be a general principle of treatment of lateral epicondylitis. 12 As far back as 1882, Morris 13 suggested that symptoms of tennis elbow would soon disappear if supination and pronation of forearm was restricted for a few weeks. Other treatment options for tennis elbow include rest, injection therapy, physical therapy, non-steroidal anti-inflammatory drugs, shock wave therapy, orthotic treatment, ultrasound, and surgery. 14
The use of wrist hand splints and forearm straps (otherwise commonly referred to as clasps) are two popular orthoses which are prescribed for the treatment of tennis elbow.15,16 The mechanism of action for current orthotic intervention in the treatment of lateral epicondylalgia is related to their effects on the restriction of forearm movement or relief of loads on the origin of the extensor muscles. Although different studies have demonstrated the effectiveness of these orthoses,15,16 none of them limit the rotational movement of the forearm. In addition, the use of a forearm strap or clasp is sometimes associated with problems such as pressure on the radial and interosseous nerves, edema, and venous congestion. 17
The concept of the new hand-forearm splint described in this study was based on restriction of movements of the wrist and forearm in association with relief of loads on the origin of the extensor muscles. When comparing a forearm strap and a new splint design composed of a wrist and below elbow counterforce strap connected by a non-flexible middle part, Forogh et al. 18 showed that the newly designed orthosis was more effective than a counterforce orthosis in reducing pain due to the limitation of forearm supination. This orthosis, however, only restricted supination of the forearm. When comparing the clinical outcomes of a wrist splint with that of a counterforce forearm strap, Garg et al. 19 observed no difference in total clinical outcome scores between two groups for the treatment of lateral epicondylitis of the elbow at 6 weeks in 44 patients. However, the wrist splint produced significantly better pain relief compared to the forearm strap brace.
The reason for the design and development of a new splint in this current study was therefore to clarify the best orthotic treatment option in this field. The purpose of this study was to evaluate a new hand-forearm splint that restricts movement of both the wrist and forearm on improvement in grip strength, pain, and function in patients with tennis elbow.
Methods
Design and concept of new splint
To design and construct the splint, the first step involved negative casting which was performed with the hand and forearm in a mid-point position. 20 After modification of the positive plaster molds, an orthosis was made for each participant.
The proximal end of the orthosis was trimmed 4 cm below the lateral epicondyle of the humerus and the orthosis maintained the wrist in 30° of extension. The proximal section of the splint was molded around the forearm using a spiral design. The splint was attached using a proximal strap plus two straps placed at the metacarpophalangeal and wrist joints areas. Polypropylene thermoplastic material (5 mm thickness) was used to fabricate the device. Figure 1 shows the new design of the splint.

New design of tennis elbow splint used in this study.
Subjects
Prior to the main part of the study, the intra-rater reliability of each measurement (within-day and between-days) using this new splint for restriction of supination and pronation of the forearm was undertaken on 13 healthy volunteer subjects (all females, 21.69 years old, 55.54 kg weight, and 169 cm height). The first two measurements were taken half an hour apart on the first occasion to assess the within-day reliability, and the third measurement was taken between 3 and 5 days afterwards to assess the between-day reliability.
This was followed by the main study, which was a quasi-experimental and recruited 15 patients with tennis elbow (5 men, 10 women; mean ± standard deviation (SD) age, 43 ± 7.69 years). All patients were referred by an orthopedic specialist. The following inclusion criteria were used: patients with pain on palpation at the lateral epicondyle and on resisted wrist extension 21 and aged between 30 and 55 years, with at least 3 weeks of history of symptoms. 22 Exclusion criteria included the following: patients with history of another treatment within the last month; 22 history of fracture, dislocation, and/or surgery; 23 and history of arthritis or limited range of motion (ROM). 18 Ethical approval was sought from the ethics committee of the University of Social Welfare and Rehabilitation Sciences. All patients were asked to wear the spiral splint 12 h a day, particularly during times when performing activities of daily living (ADLs) for 4 weeks. 18
Outcome measures
A visual analog scale (VAS) was used to evaluate pain intensity.24,25 The VAS included a 100-mm straight line (with 0 = no pain, 10 = the most severe pain). Patients were asked to report on their maximum pain experienced for the activities during the previous week as a baseline point of pain. Patients demonstrated the intensity of the sensation of pain experienced by placing a mark on the VAS line. The Disability of the Arm, Shoulder, and Hand (DASH) questionnaire was used to analyze function.24–26 The questionnaire was answered by the patients 1 day before beginning the orthotic intervention and again after 4 weeks of splint use. The DASH score has 30 questions that assess function and symptoms. It includes physical function (2 questions), symptoms of disease (6 questions), and social aspects (3 questions), and two optional modules (4 questions) for workers and athletes. Grip strength was measured using a dynamometer (Jamar Hydraulic Hand Dynamometer—PC 5030 J1). In order to measure grip strength, the test was repeated three times within a 15-min period. Active motion of the forearm was measured using an electronic digital goniometer. The goniometer was positioned on the stationary arm at the end of the forearm in line with the humerus, pointing either upward or downward. The moveable arm was aligned with a pencil that the subject held in his or her hand (Figure 2).

A goniometer was used to measure active motion of the forearm.
For assessment of grip strength and forearm motion, the subjects were seated with the elbow at 90°degrees of flexion and with the wrist in a neutral position between pronation and supination. Pain, function, and grip strength were measured at baseline and at 4 weeks. All tests were conducted by an orthotist who was trained to administer the tests. To prevent measurement bias, white paper was used to cover the goniometer dial so that the tester could not read it. 27
Data analysis
Pain, grip strength, and function were calculated for each patient/subject before and after splint use. The mean of these variables was computed for each of the two primary intervention points (baseline and after 4 weeks).
The normal distribution of the data was confirmed using the Kolmogorov–Smirnov test. The paired t-test as a parametric test and Wilcoxon test as nonparametric test were used to evaluate differences in parameters for all subjects. SPSS version 17 (JMP IN software, SAS Institute, Inc.) was used for data analysis. The significant level considered was α ⩽ 0.05.
Results
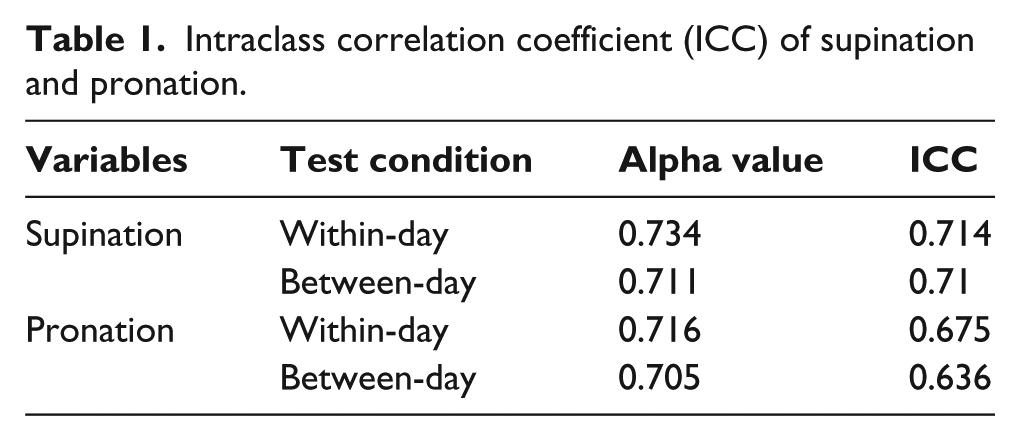
Within-day supination and pronation measurements using the new splint were shown to be acceptable, with good intraclass correlation coefficient (ICC) values of 71% and 67% for supination and pronation, respectively (Table 1). Between-day measurements also demonstrated acceptable reliability with ICC values of 71% and 63% for supination and pronation, respectively, in the healthy subjects group.
Intraclass correlation coefficient (ICC) of supination and pronation.
In the patient group, all variables (e.g. age, weight, height, time of splint use, dominant hand, affected hand, duration of injury, pain, function, and grip strength) had a normal distribution at baseline. All patients continued their use of the splint to the end of the study (100% compliance). The characteristics of the patients who participated in this study are provided in Table 2.
The characteristics of the patients in this study.
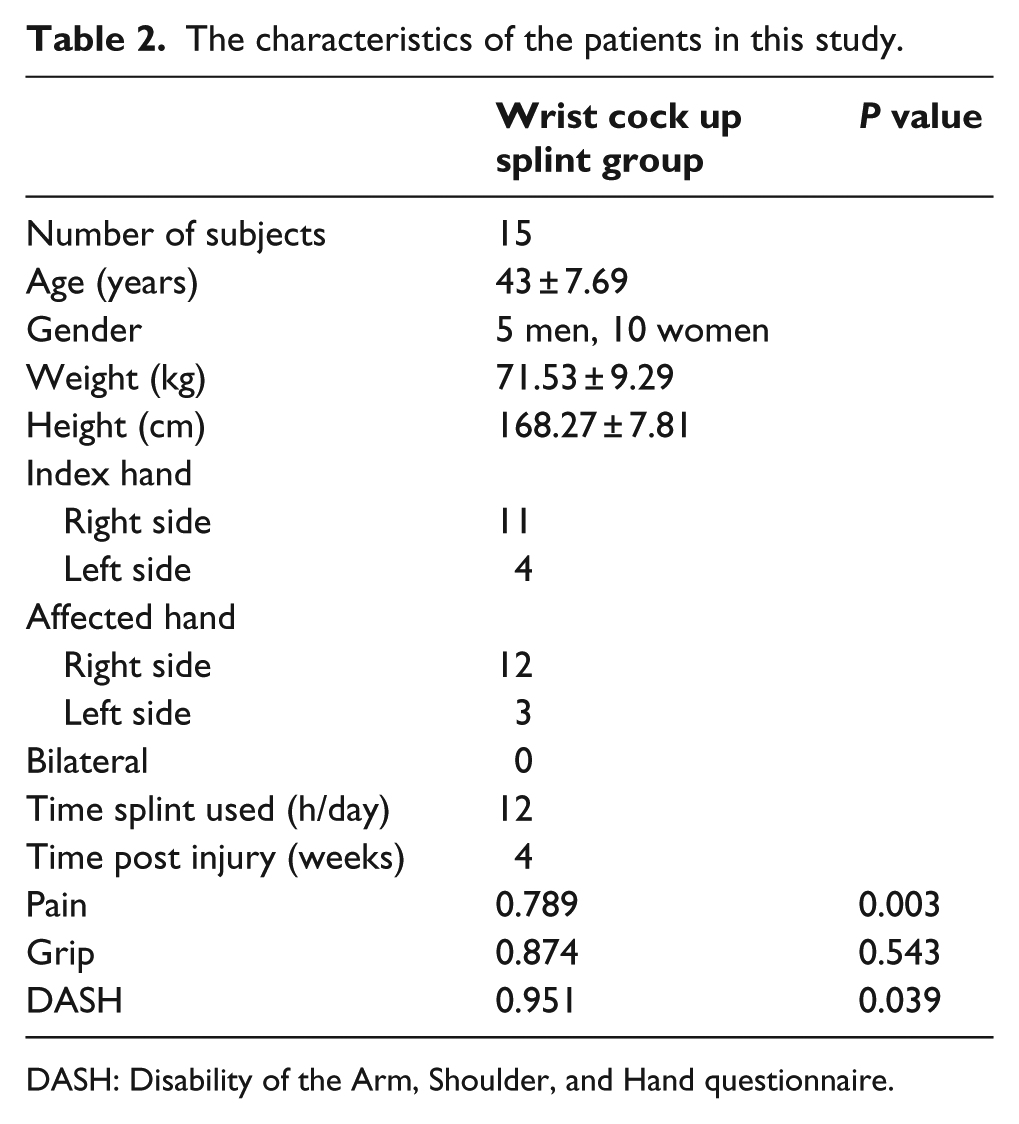
DASH: Disability of the Arm, Shoulder, and Hand questionnaire.
Comparison of restriction of forearm supination and pronation in subjects with tennis elbow and healthy subjects
Restriction of ROMs during supination and pronation are demonstrated in Table 3. There was a 59% and 53% reduction in supination and pronation, respectively, when using the spiral splint compared to the without-splint test condition in healthy subjects. In addition, using a spiral splint in the patient group also showed that there was a positive reduction in supination and pronation ROM with and without splint wear.
Supination and pronation ROM in the healthy and patient group with and without the splint being worn.
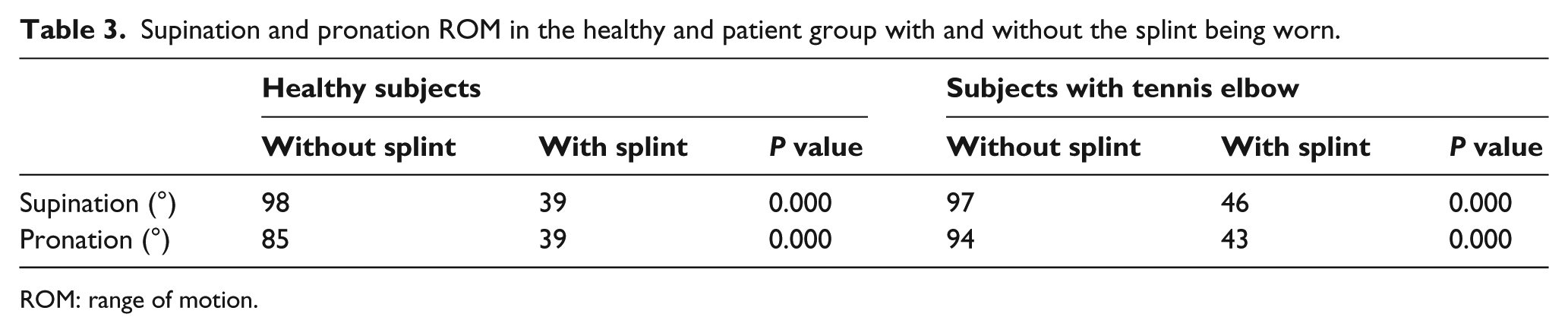
ROM: range of motion.
Comparison of parameters at the end of week 4
Using the new splint significantly decreased pain (P ⩽ 0.001) and increased grip strength (P ⩽ 0.001) compared to baseline at the end of the fourth week of splint use. Significant improvements in function based on the DASH score were also shown when using the new splint (P ⩽ 0.001) (Table 4).
Comparison of parameters at baseline and at the end of week 4.

Discussion
The aim of this present study was to introduce a new design of spiral splint that restricted wrist extension and limited supination and pronation of the forearm. The bespoke orthosis demonstrated a positive role in restriction of these objectives. The introduction of the orthosis by Forogh et al. only influenced supinator restriction in the forearm.
As with the wrist extensor muscles, the supinator muscles are responsible for forearm supination due to their origins from humeral lateral epicondyle. Therefore, these muscles have a common source in that they cause pain following forearm lateral rotation. The authors introduced a new orthosis to limit forearm supination. When compared to existing orthoses for the treatment of tennis elbow, the new orthosis provided limitation of supination, restriction of wrist motion, and counterforce pressure. The normal range of supination and pronation were 98° and 85°, but the new splint reduced these rates by 59% and 53%, respectively, compared to the without-splint condition in healthy subjects.
The results of the present study demonstrated that the new orthoses significantly relieved pain and improved function and grip strength of all patients after 4 weeks of use. This result is similar to previous studies regarding the effectiveness of orthoses in tennis elbow.15,28
The use of orthotic devices designed to relieve strain on the extensor muscles’ point of origin or using a forearm splint to restrict wrist movement has previously demonstrated positive effects on improvement of symptoms associated with tennis elbow.15,28 A combination of these two mechanisms was used in this study. Superiority of this mechanism compared to the separated mechanism must be further evaluated in future studies in this field. It seems that the restriction of supination movement associated with immobilization of the wrist extensor muscles may have caused the improvement of the clinical outcome in this study. Forogh et al. in the evaluation of a new orthosis that limited forearm supination showed that the supinator muscle rotates the forearm externally, and this has a common origin with wrist extensor muscles. In essence, this can produce pain following forearm supination. Forogh et al. 18 concluded that limitation of forearm supination can be effective for the treatment of tennis elbow. In addition, Grag et al. 19 concluded that immobilization of the wrist extensor muscles in resting position caused significant pain relief in patients after 4 weeks.
The lack of a control group is a significant weakness of this study and the improvement of tennis elbow patients may occur over time without any intervention. Active motion of the forearm was measured using an electronic digital goniometer. To help prevent measurement bias, white paper was used to cover the goniometer dial. 27 However, the assessor was not blinded to the measurements, so the possibility of bias cannot be ruled out. Further research in this area will be beneficial for the generalization of the findings presented. A further limitation relates to the short period of time (4 weeks) for the evaluation the new orthosis on patients with tennis elbow injury. Comparisons between the spiral splint and other types of orthoses over a longer period of time are required before definitive conclusions can be drawn.
Conclusion
The new splint design had a positive effect on the treatment of tennis elbow symptoms, and this included pain, grip strength, and function in patients with tennis elbow. Restriction of rotational movement (e.g. reduction of the supination and pronation of the forearm) may have been the main reason why the brace was effective in reducing symptoms.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.