
Abstract
Background and aim:
Microtia is one of the forms of ear loss and deformity. A prosthesis that is simple to apply, and which has adequate suspension and acceptable aesthetics, can be useful in the rehabilitation of patients with this deficit and can improve the social and psychological effects of patients with ear amputation. The aim of this article was to describe a novel technique for fabricating ear prosthesis in a patient with congenital ear deformity.
Technique:
This method involves a novel method to produce an ear prosthesis using clips that were located within the layers of the final silicone ear.
Discussion:
This study demonstrated ease of use and acceptance by the patient. Design and fabrication of silicone ear prosthesis via this new method of suspension could also be suitable for provision to children with ear microtia who are not yet suitable for surgery or would not be suited to other methods of suspension.
Clinical relevance
The new method of suspension demonstrated that this approach could be used to provide low cost and acceptable silicone ear prosthesis for patients with microtia and partial ear amputation.
Background and aim
Cosmetic prostheses combine the skills and knowledge of art and science in the reconstruction of defects and anomalies of the human body. 1 The human ear is in a prominent and nonprotected position on the head and is therefore vulnerable to injury. 2 Ear amputation occurs due to trauma or congenital diseases and can also occur following surgical removal of benign and malignant tumors.3,4 Cosmetic surgery is one of the therapeutic approaches. 4 The prevalence of a congenitally small ear has been quoted as being demonstrated in 1 in 12,500 births. 5 The facial defects that occur due to the treatment of malignancies, congenital deformity, and trauma may lead to functional and psychological problems for patients. Therefore, prosthetic rehabilitation for reconstruction of facial defects could prove useful and lead to improved levels of function, appearance, and confidence in patients. 6
There are various types of suspension methods traditionally used to hold ear prostheses in place. One common method is the use of adhesives, but this has certain disadvantages, because adhesive removal from the skin surface can cause damage to the prosthesis wall. 7 In addition, adhesive use may lead to the accumulation of microbes and possible subsequent infection. 8 Attention and skill are needed to position the prosthesis in the correct place. 9 The use of implants is not ideally suited for people with partial loss of the ear or those with microtia, and it is necessary to surgically remove residual tissue for implant techniques. 5 The use of a prosthesis is therefore a viable alternative for those patients who are reluctant to undergo surgery. 10 However, the prosthesis needs to have an aesthetic appearance and be effectively suspended while the residual ear is still retained. This article describes the fabrication of custom-made ear prosthesis in a patient with congenital amputated ear fabricated in silicone, which provided adequate suspension, was aesthetic, and proved easy for the patient to use.
Technique
Case report
The patient was a 13-year-old male child who had congenital microtia of the right ear. He was referred to the Department of Orthotics and Prosthetics in the University of Social Welfare and Rehabilitation Sciences. It was decided to use a silicone ear prosthesis because it was not appropriate to perform surgery or apply an implant. The patient gave informed consent to participate in this study. Approval was obtained from the Ethics Committee of the University of Social Welfare and Rehabilitation to undertake this study.
The fabrication of the ear prosthesis involved numerous stages. Initially, the stump and residuum were examined to confirm suitability of provision of a silicone ear prosthesis. The patient’s affected right ear (Figure 1) was lubricated with a thin layer of Vaseline to avoid adherence of the impression material to the skin or any localized hair. Cotton was placed in the ear cavity. A circular box was placed around the ear area, and alginate (tropicalgin; Zhermack, Italy) impression material was poured into the circular box. The alginate impression material permitted the negative cast to be removed from the residuum. The patient’s head was positioned so that the ear area was as near to the horizontal plane as possible to reduce leakage of alginate. Plaster of Paris was then poured into the negative cast to produce a positive cast. Following this, the two-snap adaptation was attached to positive cast of residual limb to provide a suspension method.

Patient with right microtia.
A positive cast of the healthy ear was then prepared by wax (modeling wax; Covex, The Netherlands) from negative cast for the replicated donor ear. A wax-positive impression was attached on the plaster of Paris positive cast of the affected ear to reconstruct the amputated ear using wax. A multipiece former was therefore prepared from a reconstructed model of the ear (Figure 2), which included two pin-type snaps. The number of pieces in this stage depends on the number of negative quadrants of the positive model of the healthy ear that need to be constructed on the stump.

Multipiece format and two pin-type snap positions.
The multiple pieces of the resulting former were kept together with a pincer manually. It was then placed in boiling water for 10 min, to enable the wax material in the reconstructed ear to melt. The multipiece former was then ready for silicone injection and designed to prevent tearing of the final silicone ear prosthesis.
According to patient’s skin, an appropriate background color was mixed with the silicone biomaterial (RTV 3040; Shimi Afsoon Company, Iran). The prepared silicone was poured in the multipiece former, which was then split apart to produce the final ear prosthesis. The two pin-type snaps were then attached.
The final step was placement of the prosthesis on the congenital ear deformity (Figure 3), following secondary painting of the prosthesis to closely match the coloration to that of the patient’s skin on the healthy ear.

The final prosthesis.
In this approach, two clips were used, which were located within the layers of the final silicone ear. These clips provided suspension when the prosthesis was pushed into position (Figure 4).
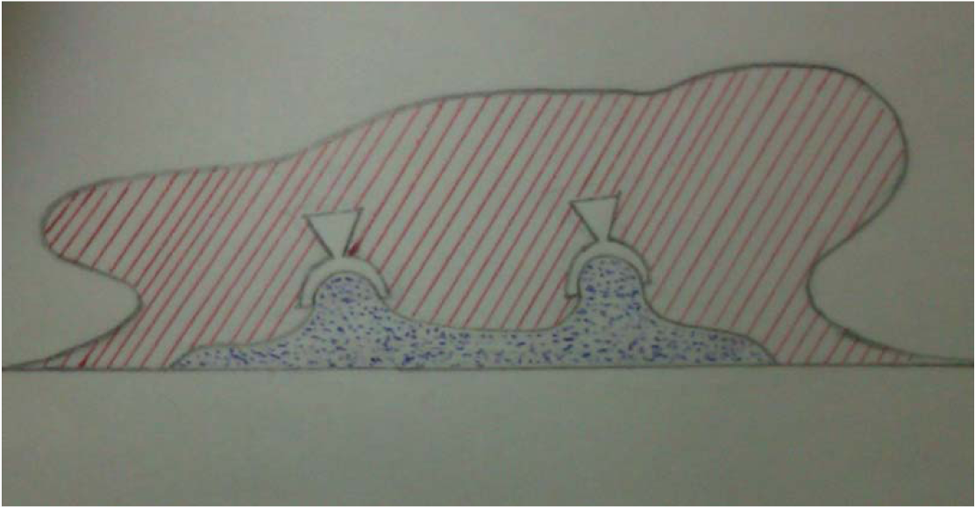
Details of the new method of suspension used in this study.
Discussion
An appropriate suspension method plus a user-friendly design is critical for use of this type of prosthesis.11,12 In this article, a new method of suspension based on simple application and use of biomedical material was proposed.
Adapted spectacles (glasses), adhesives, and surgical implantation are the general suspension methods currently applied for ear prostheses.7,10,13,14 In this study, use of a new method of suspension for ear prosthesis was provided by using two pin-type snaps. Previous studies in this field have demonstrated that the use of adhesives, implants, and mechanical suspension methods such as glasses are not successful approaches in providing suspension for ear prostheses in all cases.5,10,15 In situations where patients are unable to use such conventional methods of suspension, a new system such as the one designed in this study could prove useful. The new method was stable and easy to use with assistance from the two-snap system for suspension.
Deficiencies such as congenital ear deformity or amputation can provide unwanted cosmesis problems for patients and can negatively affect their self-body image. Ear prostheses can play an important role in restoring near-normal appearance in subjects with ear amputation. In those cases where adhesive types of suspension, surgery, or glass suspensions are not acceptable for patients, requests are often made for ear prosthesis. Silicone ear prostheses may have additional appearance benefits for such patients, as the use of silicone biomaterial permits copying of the natural ear in finite detail.
Prosthetic rehabilitation of patients with ear amputation or deformity is quick, user-friendly, acceptable, and allows the residual limb to be closely monitored. 7 Design and fabrication of a prosthesis that provides a cosmetic natural skin surface needs both artistic and prosthetic expertise in providing an appropriate skin color and requires great attention to detail. 1
In the particular case of the volunteer subject described in this article, 5 months following the receipt of the ear prosthesis, the patient announced his satisfaction with the cosmetic appearance of the prosthesis, its ease of use, and the fact that it was comfortable to wear and could be conveniently removed. He also reported improved confidence during social activities.
Evaluation of this type of prosthesis based on the new method articulated in this article regarding its efficacy, suitability, and cosmesis in a larger cohort of patients with ear amputation using verbal and written evaluations would be beneficial in a further study. In addition, evaluation of quality of life on persons with ear amputation using this new method of prosthetic treatment compared to other suspension methods by means of formative feedback will also be interesting in a further study in this field.
Key points
Congenital ear deformity involving structural loss of tissue is one type of facial defect seen in prosthetic practice.
Prosthetic rehabilitation for reconstruction of facial defects could prove useful and lead to improved levels of function, appearance, and confidence in patients.
To provide suspension in ear prosthesis, clips were used, which were located within the layers of the final silicone ear. These clips provided suspension when the prosthesis was pushed into position.
Footnotes
Acknowledgements
This article was a part of a PhD thesis in the Department of Orthotics and Prosthetics (O&P) in the University of Social Welfare and Rehabilitation Science. The authors would like gratefully acknowledge the help extended by members of the O&P department and the contributions from the patients in all stages of study.
Conflict of interest
The authors did not have any conflicts of interest with regards to the study presented in this paper.
Funding
This research received no specific grant from any funding in the public, commercial, or not-for-profit sectors.