
Abstract
Background:
Lumbopelvic injuries are often refractory to treatment and can limit return to sport. Research shows that 50 Newtons (N) of force applied transversely to the pelvis improves lumbopelvic stability and pain. This study applies transverse and diagonal forces to the pelvis in athletes with lumbopelvic pain, and investigates effects on pain and function.
Objective:
To investigate the effects of transverse and diagonal compressive forces applied to the pelvis of athletes with lumbopelvic pain
Study Design:
A randomized, repeated measures design using 20 athletes with lumbopelvic pain.
Methods:
No belt and four pelvic belt configurations (50 N force) were tested. Outcome measures were: resting pain, pain on active straight leg raise (ASLR), resisted hip adduction force and pain on 1-metre broad jump. Force on the adduction test was determined via load cell.
Results:
Data were analyzed using repeated measures ANOVA. Squeeze test showed significant effect of condition F (4, 76) = 2.7, P < 0.05. On ASLR ipsilateral to the side of pain, pain decreased across conditions (F (4, 76) = 2.5 P = 0.05).
Conclusion:
Results suggest application of diagonal forces towards the site of pain may have additional benefits in improving pain and function. Such information may inform the development of an orthosis.
Clinical relevance
The results may be used clinically to determine the effectiveness of different belt placements (with belts or straps) in managing athletic lumbopelvic pain. The results offer an alternative to the application of transverse belts, and may inform new approaches in the development of orthotics.
Keywords
Background
Athletic lumbopelvic pain is difficult to diagnose and manage, due to the close proximity of anatomical structures, and the common occurrence of more than one site of injury 1 . This can often result in the development of chronic pain through on-going dysfunction. A difficulty exists in defining groin and sacroiliac joint (SIJ) pain as separate entities. Prather and Hunt 2 highlight that while posterior pelvic pain (a more appropriate term for SIJ pain) is commonly located around the posterior superior iliac spine, such pain can also be experienced in the groin. They further acknowledge that if adaptive changes caused by conditions such as pubic symphysis can lead to SIJ pain, the reverse is possible. This equates with the acceptance that there is commonly more than one site of pain, 3 and an overlap in responses to pain provocation tests. Alterations in muscle recruitment and pelvic stability have been implicated in both pelvic and groin pain.4-6 Therefore, in this paper we will use the more appropriate term of lumbopelvic pain.
Current management of sports-related lumbopelvic pain involves a wide range of approaches from surgery, strengthening exercises, 7 pelvic belt application and stabilization exercises. 8 One specific intervention that has been investigated in sports-related groin pain is the application of pelvic belts, which have been shown to produce beneficial effects in both pain and function, as demonstrated by improved performance on clinical tests of active straight leg raise (ASLR) and resisted bilateral hip adduction. 9 This approach has focused upon the use of pelvic belts to address the force closure mechanism. A useful explanation proffered by Lee 8 discusses how belt placement (compression) may affect specific muscles associated with lumbopelvic stability. Placement of a belt at the level of the anterior superior iliac spine (ASIS) is thought to imitate a contraction of transversus abdominus, while action of the anterior pelvic floor is thought to be reinforced with placement of a belt at the level of the symphysis pubis. The finding that there is a delay in transversus abdominus activation in subjects with chronic groin pain 5 suggests that there may indeed be a link between altered force closure and pain that may be addressed with the application of pelvic belts.
Pelvic belts also have been researched and adopted clinically in the management of pelvic pain in other conditions, such as peri-partum and post-partum pelvic pain. Research has shown, for example, that such belts can decrease pain, and improve the stability of the SIJ where laxity (impaired force closure) is associated with pain.10, 11 More specifically, this research has demonstrated that the application of 50 N of force has the most beneficial effect upon pain; with higher forces (up to 200 N) not showing any further benefit. 12
Transverse belts are most commonly used in both athletes and in peri- and post-partum women. These belts are placed just below the level of the ASIS or at the level of the symphysis pubis or the greater trochanter. To date, other pelvic belt and strap combinations have not been examined. Diagonal configurations which may provide a compression force towards and/or away from the site of pain warrant investigation based on the notion that they may provide an alternative method of belt application which is more effective than those currently used. It is possible that an asymmetry caused by lumbopelvic pain presenting on one side of the body, could be addressed by an external force that rebalances the asymmetry in force closure and/or joint mobility.
The aim of this study was to establish if alternative applications of pelvic belts may decrease lumbopelvic pain and improve function in athletes. Improvements in lumbopelvic pain with particular directions of force application may inform new approaches in the development of orthotics, such as dynamic elastomeric fabric orthosis (DEFOs).13-16
Methods
Study design
A repeated measures experimental design was used, so that every subject could be tested under each condition, and therefore act as their own control.
Sample
A sample of 20 athletes with clinically ascertained lumbopelvic pain, as determined by the screening procedure is outlined below. Mens et al. 9 found a mean difference of 38 N (+/- 13.8 mean+/- standard deviation) in adduction force in subjects with groin pain with or without a pelvic belt. A sample size calculation was undertaken, for a +power of 0.99 and significance level of 5%, 11 participants were required in each group. However, given Jansen’s 7 finding of variability in adduction force between those with left-, compared with right-, sided groin pain the sample size was increased to 20 to minimize type II errors. The study was approved by the local ethics committee (Plymouth University) and people participated after informed written consent was obtained. The rights of the participants were protected at all times.
Eligibility criteria
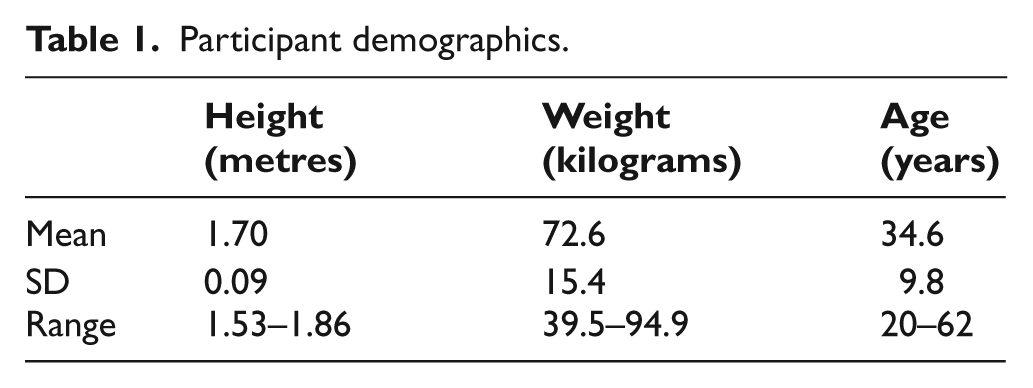
Potential subjects were over 18 years old, for consent reasons (see Table 1 for demographics), with a history of lumbopelvic pain occurring during sport or at rest. There was no time minimum or maximum on duration of pain, to allow for inclusion of both acute and chronic conditions.
Participant demographics.
Inclusion criteria
In line with European guidelines, the following battery of tests was used for screening purposes, 17 ensuring that the inclusion of tests to identify sacroiliac joint, symphysis pubis and adductor pain.
Active Straight Leg Raise (ASLR)
This has been shown to be a reliable measure of impaired load transfer through the lumbopelvic region, 18 and valid for use in athletes with groin pain. 5 Subjects were supine with their legs 20 cm apart and were asked to raise each leg 20 cm above the plinth. Subjects self-scored how difficult they found this task using a rating of 0 to 5 (where 0 refers to no difficulty, 2 to 4 represent increasing difficulty, and 5 indicates great difficulty). The final score was determined by adding scores from both legs (range 0–10). Scores 1 to 10 were defined as positive.
Faber/Patrick’s test
From a supine position the subject was asked to position their leg into flexion, abduction and external rotation, by placing one foot across the knee of their opposite leg. The therapist then applied pressure to the externally rotated knee, while stabilizing the opposite ASIS; a positive test was determined if pain was provocated with application of this pressure. 19
Resisted hip adduction
In line with other studies examining groin pain,9, 20 from a supine position the subject was asked to adduct their leg and maintain adduction against an external resistance. The test was positive when the subject’s lumbopelvic pain was reproduced.
Thigh thrust
Laslett et al. 21 identified this test, which is also known as the posterior pelvic pain provocation test, as the most sensitive test of sacroiliac pain. The subject was asked to lie in a supine position, while the therapist flexed their knee and hip, before applying a downwards force through the knee towards the pelvis. A positive test was determined if pain was provocated with application of pressure. 22
Gaenslens
From a supine position, the therapist flexed the knee and hip of the subject, while extending the opposite leg to lie off the plinth. Overpressure was applied to the flexed knee towards the pelvis, and to the iliac crest of the abducted/extended leg. A positive test was determined if pain was provocated with application of this pressure. 22
For inclusion, positive pain scores had to be determined on at least two of these five tests, as when used in isolation these tests are limited in terms of reliability, but when used together they provide a more conclusive approach 23 . The minimum number of positive responses to pain, was based upon the nature of the tests selected for this battery.
Exclusion criteria
The following exclusion critera were adopted:
Osteoporosis, to exclude risk of a pelvic fracture being responsible for lumbopelvic pain.
Anorexia, to exclude those at risk of osteoporosis.
Neurological signs, determined by clinical examination, which may influence pain perception, and to exclude lumbosacral radicular syndrome.
Pregnant at time of testing, to ensure the safety of the mother and foetus.
Co-morbidities, such as rheumatological, neurological or systemic disease which may impact upon the outcome measures.
Suspected fracture based on clinical examination (e.g. pain as measured by a numerical rating scale (NRS) >8/10, deformity, acute swelling, significant leg length discrepancy, and mechanism of injury).
Trochanteric bursitis.
Muscle or tendon rupture.
Inguinal herniation.
Previous pelvic fracture.
Instrumented pelvic belts and straps were constructed consisting of a horizontal pelvic belt (similar to that used in clinical practice with additional pelvic straps to traverse across the pelvis (right to left, and left to right). A low profile load cell (S250, SMDsensors, Bury St Edmonds, UK) was attached in series to allow the measurement of applied force of 50 N, in each strap signals from the load cell were AD converted (200 Hz, micro1401, CED, Cambridge, UK) and displayed (SPIKE2 software, CED,UK) to allow consistency of load application across participants. Figure 1 shows the pelvic belt configurations.

The pelvic belts with the strain gauges in situ.
Following the screening process, baseline data were gathered and then outcome measures undertaken in a standardized order across the five belt conditions. The order in which participants were tested under each of the belt conditions was randomized:
No belt.
A belt just below the ASIS. 9
A belt traversing right to left diagonally across the pelvis.
A belt moving left to right diagonally across the pelvis.
A combination of right and left diagonal belts.
Each of these positions (except no belt) were tested with an applied force of 50 N using the outcome measures detailed below.
Standardized instructions were given to each subject to ensure accuracy of the information given and to control confounding variables; such as verbal motivational cues delivered by the tester. A standardized ‘flush out’ period of three minutes between each intervention was used to avoid carryover effects, and to minimize irritation. 10 This involved a rest period, where the subject was asked to lie supine on the plinth. The duration of rest was accounted for by the effort taken to order the tests from least to most irritable, and those with a high pain score (8/10) being excluded from this study.
Outcome measures
Baseline measures
A standardized questionnaire was used to gather demographic data, training regime – frequency and type of training; injury and pain history, and sport specific information.
The following battery of clinically orientated tests and functional sporting measures was then undertaken for all conditions, as described below. The measures selected were chosen on the premise that they are not only tests used clinically and/or in the field, but in the cases of the ASLR and resisted adduction, are used as measures in pelvic belt research.
Primary outcome measure:
1) Force produced on bilateral hip adduction: With participants lying in supine a padded load cell (SGA, Applied Weighing, Reading, UK) was placed between the ankles at the level of the medial malleoli. Participants were asked to perform a bilateral contraction of the hip adductors against the strain gauge and to continue the contraction until they rated their pain as moderate (5/10 on the NRS) or they reached their maximum contraction. Subjects pressed a hand-held switch to indicate this point. The force at which this point occured was measured via the load cell. Force and switch signals were AD covereted at 200 Hz (Micro 1401, CED, Cambridge, UK) and recorded using Spike2 software. The applied force at the point of the switch press was directly measured via interactive cursors.
Secondary outcome measures:
2) Pain during ASLR: Subjects lying in supine were asked to lift their leg (keeping their knee in extension) up to a bar placed 20 cm above the plinth and 65 cm distal to the greater trochanter to ensure all subjects moved through an identical arc. Pain was measured by means of a 10-point NRS; where 0 represents no pain and 10 is the worst imaginable pain. Both legs were tested one at a time, commencing with the right leg.
3) Pain at rest while lying in supine: This was measured via a 10-point NRS scale.
4) Standardized broad jump: Subjects performed a standardized broad jump of 1 metre. Pain was rated using a 10-point NRS immediately pre- and post-jump.
Statistical analysis
Statistical analysis was performed using SPSS 19, for Windows. The control and each experimental condition were compared using a repeated measures ANOVA (five factors: control and belt position 2 to 5). The latter was selected as the assumptions for using a parametric test were met. A Greenhouse-Geisser correction was applied if assumptions of sphericity were violated. A priori contrasts were used to explore whether there was any difference between the no belt condition and the four belt configurations. Significance level was selected at P≤0.05.
For purposes of analysis and to correspond to clinical terminology, the right to left and left to right belt configurations were relabelled ipsilateral to contralateral (IPSI TO CONTRA), and contralateral to ipsilateral (CONTRA TO IPSI), relative to each subjects’ site of pain.
Results
Demographics
Twenty-two athletes from various sports/physical activity backgrounds and with lumbopelvic pain were assessed. After screening, 20 were eligible for inclusion (14 female), and provided written informed consent to partake in the testing process. Table 1 provides details of their demographic characteristics. There was a mixture of both chronic (n = 15) and acute (n = 5) conditions; location of pain is detailed in Table 2); some participants reporting more than one site of pain. Sports included rugby football, football, power walking, boxing, beach sprints, squash, running and cycling, with many participants citing their involvement in several sports. All subjects were training between three and five times per week undertaking a mixture of aerobic and anaerobic training. Nineteen of the participants were recreational level athletes (two of whom had previous experience of national level sport), and one athlete was competing at international level. Table 2 presents the pain location, history and responses to the pain provocation tests used in the screening process.
Injury history and participant responses to pain provocation tests.
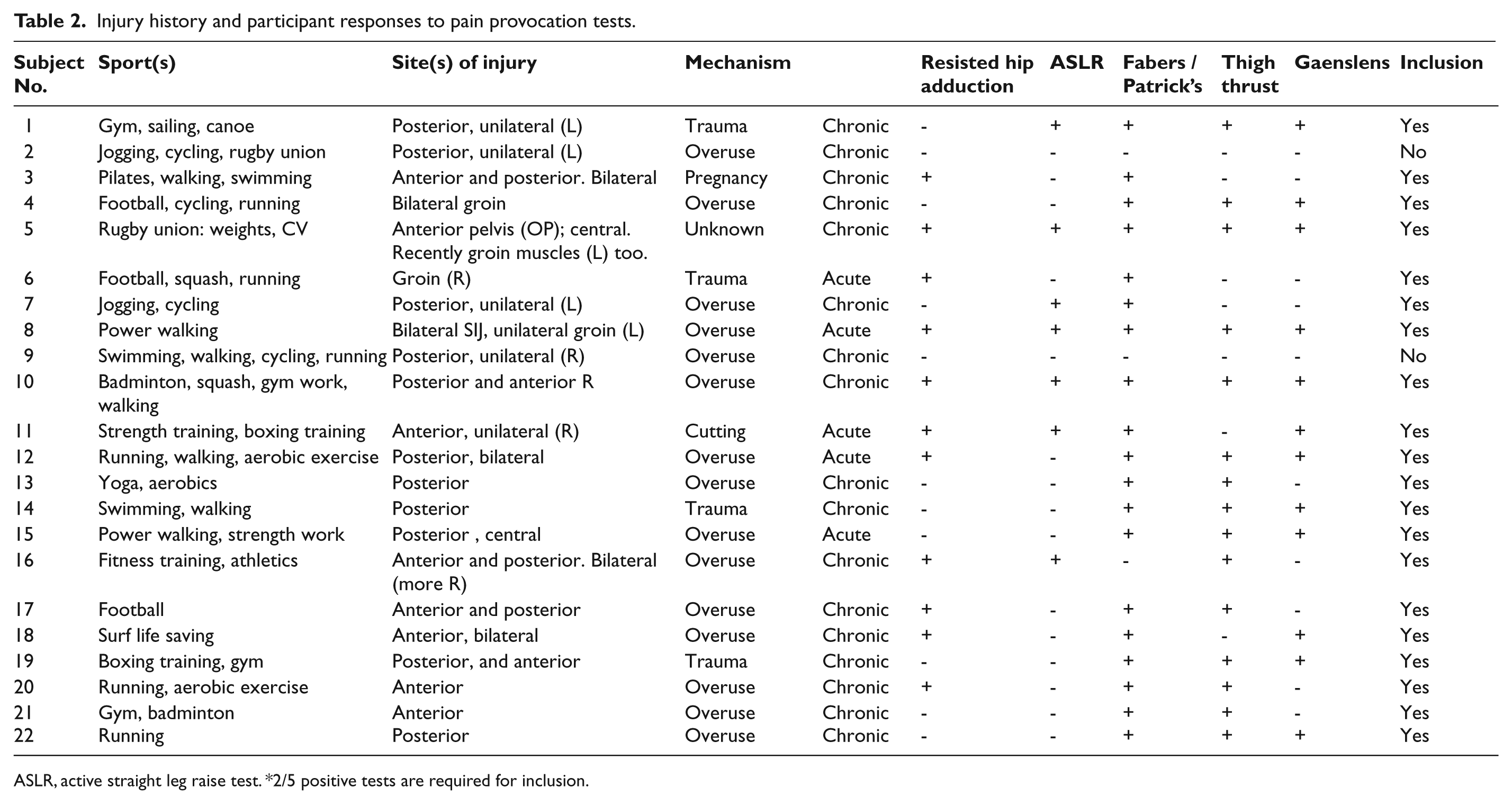
ASLR, active straight leg raise test. *2/5 positive tests are required for inclusion.
Outcome measures
Resisted bilateral hip adduction showed a significant effect of condition (F (4, 76) = 2.7 P < 0.05). Within subjects contrasts demonstrated that the adductor force produced was significantly lower in the ‘no belt’ condition compared to the ASIS condition (ASIS F (1, 19) = 9.3 P < 0.01), and a belt traversing towards the site of pain (CONTRA TO IPSI, F (1, 19) = 5.2 P < 0.05, Table 3).
Effects of pelvic belt configuration on applied force and pain. Mean ± standard deviation is indicated.
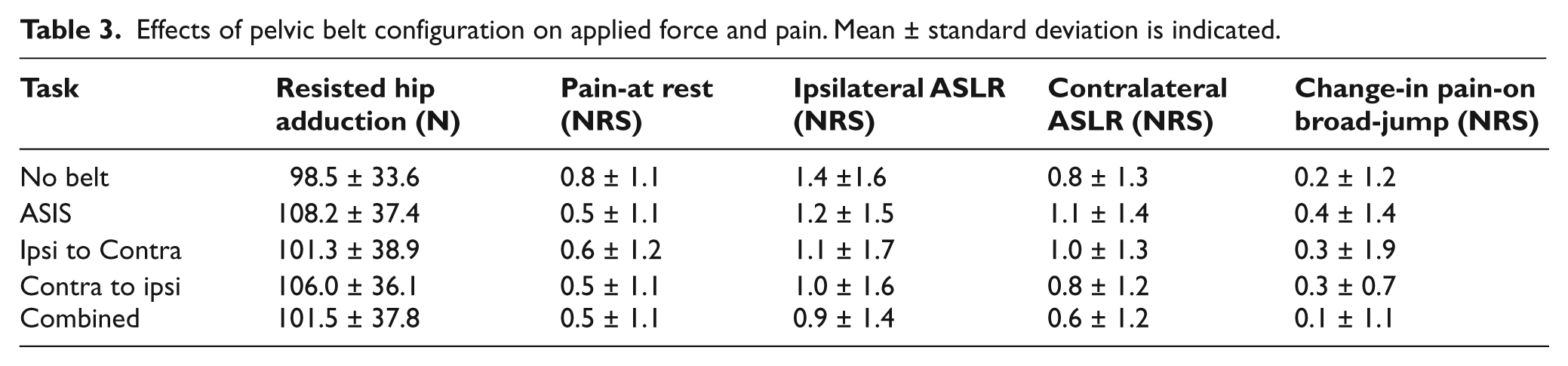
For the ipsilateral ASLR there was a tendency for the pain to decrease across conditions (F (4, 76) = 2.5 P = 0.05). Contrasts revealed that there was a significant reduction in pain in the CONTRA-IPSI (F (1, 19) = 8.2 P < 0.01) and ‘combined belt’ conditions (F (1, 19) = 8.6 P < 0.01) compared to the ‘no belt’ condition (Table 3).
There was no effect of belt condition on resting pain (F (4,76) = 1.9 P > 0.05); contralateral ASLR (F (4,76) = 2.2 P > 0.05) or the change in pain following a broad jump (F (4,76) = 0.34 P > 0.05).
Discussion
Pelvic belts providing compression towards the site of pain produced a decrease in pain experienced during ipsilateral ASLR. The traditional ASIS belt produced an improvement in ability to self-generate adduction force and the combined belt produced an improvement in ASLR-related pain, compared to ‘no belt.’
The improvement in pain and function may be caused by the belts enhancing joint stability and force closure. Other possible mechanisms are, however, also possible, since not all lumbopelvic dysfunction is associated with loss of force closure. 24 For example, activation of muscles, such as transversus abdominus, that are felt to play an important role in force closure have demonstrated significantly less resting thickness in longstanding groin pain patients, but do not always show changes in thickness or activation pattern following resolution of pain with rehabilitation. 6 It has also been suggested by Jansen 6 that pelvic belts provide an improvement in hip joint position awareness. Elaborating upon this, improved proprioception for example, has been reported in the trunk and limb following neoprene bracing25,26 and hypothesized to underlie some of the actions of taping. 27
It is also acknowledged that improvement in pain and function may have been the result of belts addressing the symptoms, rather than the cause of dysfunction. The fact that many athletes engaged in multiple sports could also confound the issue when it comes to understanding the very mechanism associated with their pain. However, as has been done, the literature should be used to inform any discussion of lumbopelvic pain and its proposed mechanisms, and the complex nature of lumbopelvic pain has been acknowledged. 7
The selection of outcome measures was designed to encompass both clinically used tests (e.g. ASLR, resisted hip adduction) and a sports-orientated measure (broad jump). What became apparent during the testing process was that these tests were often not reproducing the athlete’s pain, or that pain was at a level so low that it was difficult to measure the true effect of each belt.
From an ethical perspective, minimizing irritability with repeated measurement in one session was essential. Some athletes, who did not experience pain during testing, were still able to clearly identify sporting activities that exacerbated their pain tremendously e.g. pain during ‘cutting’ manoeuvres. 5 A consideration for further research may be to incorporate more stressful tests that may be able to recreate the stress placed upon the pelvis during sporting activities, while also ensuring that the testing procedure provides adequate recovery time to minimize irritability. One potential measure is the bilateral adduction test; patient’s knees in extension, and the hips raised to 30 degrees of flexion with 10 degrees internal rotation, and adducting against resistance. 28 This is often used to test adductor and/or osteitis pubis pain in athletic populations, alongside the tests used in this study, but is more stressful. While the results do appear to be in consensus with suggestions from the pelvic belt literature, inclusion of more stressful tests of both pelvic girdle and groin pain may enable differentiation between the ASIS and contralateral-ipsilateral belts in their ability to improve function and reduce pain.
Conclusion
The results support previous studies demonstrating that a circumferential belt at the level of ASIS improves pain and pain-free adduction force. The results further suggest that the application of diagonal forces towards the site of groin pain may have additional benefits in improving pain and function compared to no belt or a circumferential belt at the level of the ASIS. Such information may be used to inform the future development of DEFOs.
Footnotes
Conflict of interest
The results were used to aid the development of an athletic orthosis which has been registered by DM Orthotics Ltd.
Funding
This work was funded by the department of health and DM Orthotics Ltd, as a Knowledge Transfer Partnership.