
Abstract
Background: Ankle-foot orthoses (AFO) have been used to improve the gait of individuals post stroke, but their use has come into question secondary to increased understanding of motor re-learning.
Objectives: The purpose of this study was to determine if there is a change in tibialis anterior muscle electromyography, ankle angle, or gait velocity when individuals post stroke walk with a posterior leaf-spring AFO (PLAFO) or a dynamic ankle orthosis (DAO).
Study Design: Repeated measures.
Methods: Fifteen participants post stroke walked without an orthosis, with a PLAFO, and with a DAO. Data were gathered using electromyography, force plates, and three-dimensional motion analysis cameras. A repeated measures ANOVA was used to test for statistical significance (p ≤ 0.05).
Results: Participants exhibited significantly less tibialis anterior muscle electromyography during the swing phase of gait with use of a DAO (p < 0.001). No change in velocity or ankle angle was exhibited with use of either orthosis.
Conclusions: The results support therapists’ notions that bracing can lead to a decline in tibialis anterior muscle activity during the swing phase of gait. The results also showed no improvement in gait velocity when either orthosis was used by participants who could walk without an orthosis.
Clinical relevance
First, the use of relatively flexible orthoses can cause a decline in tibialis anterior muscle activity during the swing phase of gait. Secondly, neither the posterior leaf-spring ankle-foot orthosis nor the dynamic ankle orthosis should be prescribed to improve gait velocity in individuals who are able to walk without bracing.
Introduction
Ankle-foot orthoses (AFO) including custom-moulded polypropylene and bilateral metal upright AFOs have traditionally been used to improve the gait of individuals post stroke, but their use has come into question in recent years.1–9 Impairments in ambulation post stroke stem from diminished dorsiflexion of the ankle with resulting sustained plantarflexion and inversion of the ankle during the swing phase of gait, a lack of eccentric control of ankle dorsiflexion during weight acceptance and a decrease in gait velocity.1,10–12 Multiple studies have demonstrated improved ankle kinematics, improved symmetry, and increased velocity when individuals post stroke walk with an orthosis.1–9
Secondary to the increased understanding of plasticity of the brain, healthcare providers are hesitant to use an AFO for individuals post stroke because they fear using an orthosis encourages disuse of the tibialis anterior (TA) muscle and decreases opportunity for motor relearning with the end result of permanent gait impairments, and a dependence upon bracing.7,13 Hesse et al. 7 investigated electromyography (EMG) of the TA muscle and recorded a decrease in activation when individuals post stroke walked with a rigid AFO compared to walking without an AFO. Mulroy et al. 14 found that a plantarflexion stop AFO reduces TA muscle activity in patients post stroke; however, they also demonstrated that a rigid AFO and a dorsiflexion assist/dorsiflexion stop (DA/DS) AFO did not reduce TA muscle activity. 14 The DA/DS orthosis was hinged with elastic bands to provide dorsiflexion assistance during swing and a posterior strap to limit dorsiflexion to five degrees. 14 Unlike the plantarflexion stop AFO, the DA/DS orthosis allowed subjects to plantarflex during the loading phase of gait which likely resulted in the continued TA activity. Geboers et al. 13 demonstrated an immediate decrease in TA muscle firing when a rigid AFO was used in subjects with peripheral paresis and healthy subjects. However, the authors also demonstrated the reduction in EMG did not accumulate over time when subjects were remeasured at a 6-week interval. 13 These studies lend support to therapists’ notions that use of certain AFOs may lead to a decreased use of the TA muscle.
In addition, orthoses have been designed for individuals with neurological impairments aimed at preventing a decline in muscle activity during gait. The dynamic ankle orthosis (DAO), also known as the Utley’s foot orthosis, is one such orthosis. It has been developed to provide ankle stability and dorsiflexion while minimizing the decrease in muscle recruitment during gait by allowing normal movement patterns. 15 The DAO theoretically provides a proper base of support for weight acceptance by maintaining the ankle joint in a subtalar neutral position, allows for normal tibial advancement during the stance phase of gait, and potentially provides assistance in foot clearance during the swing phase of gait. 15 However, to the best of our knowledge no published research exists investigating the effects of the DAO on gait.
The current study investigated participants 7 months or less post stroke walking without an AFO, walking with a posterior leaf-spring AFO (PLAFO), and walking with a DAO. The primary objective of the study was to investigate if there was a decline in TA muscle EMG during the swing or loading phases of gait when the two different orthoses were used compared to walking without an orthosis. The secondary objectives were to examine ankle angle and velocity during gait when the different orthoses were used.
Methods
Participants
Fifteen participants were recruited for the study based on an a priori power analysis with an estimated effect size of 0.5 with an acceptable power ≥0.8. Eight female and seven male individuals who were recently discharged from a rehabilitation hospital were recruited for this study. Participants were 7 months or less post stroke and had a diagnosis of stroke acquired hemiparesis. Inclusion criteria consisted of the ability to walk a minimum of 20 metres without assistance. Participants were not excluded if they typically wore an orthosis and were able to ambulate 20 metres without the orthosis. Two participants included in the study typically wore a custom-fit hinged polypropylene AFO. Ten individuals had paresis on the right and five on the left. Corrêa et al. 16 have demonstrated no difference in EMG or ground reaction forces for individuals post right-sided stroke compared to left-sided stroke. Therefore, we investigated subjects with both right and left paresis; however, an even distribution was not a requirement when recruiting participants. Additional participant characteristics can be seen in Table 1.
Descriptive data for subjects.
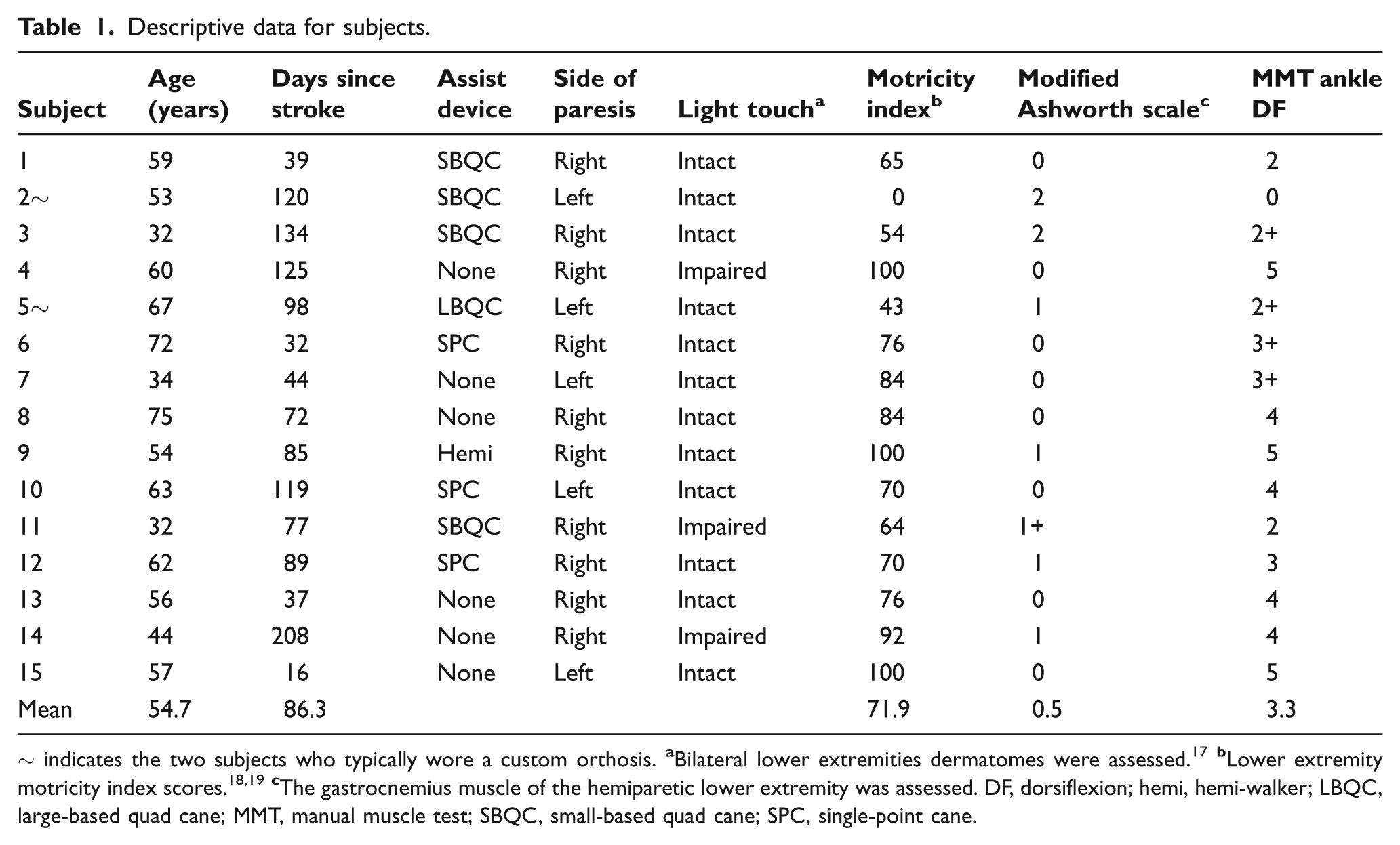
~ indicates the two subjects who typically wore a custom orthosis.
Instrumentation
Surface EMG data were collected at a rate of 1560 Hz using a Myopac EMG unit. a A VICON 460 Motion Analysis System b was used to acquire a three-dimensional moving image of subject’s lower extremities. Video recording from a JVC c colour video camera and video capture software d were acquired to allow an observational comparison of movements. Also, data were collected at a rate of 1560 Hz from embedded force plates e and were used for determining gait events. Data from the force plates, motion analysis cameras, video recordings, and EMG were synchronized and integrated using the VICON Datastation.
Orthotics
Prior to testing a pre-fabricated PLAFO f (Figure 1) was sized for each participant according to the manufacturer’s instructions. DAOs (Figure 2) were fabricated for the hemiparetic lower extremity for each participant following guidelines outlined in the course materials presented by Utley and Woll in ‘Orthotics used with the neurodevelopmental treatment approach to neurological patients. 20 (See Appendix A for details). The DAO were made from Polyflex II and consisted of a medial cuff and a short foot plate that extends from the posterior heel to the proximal end of the metatarsals. Additional instructions for the manufacturing process of the DAO can be seen in Appendix A.

Left posterior leaf-spring ankle-foot orthosis.
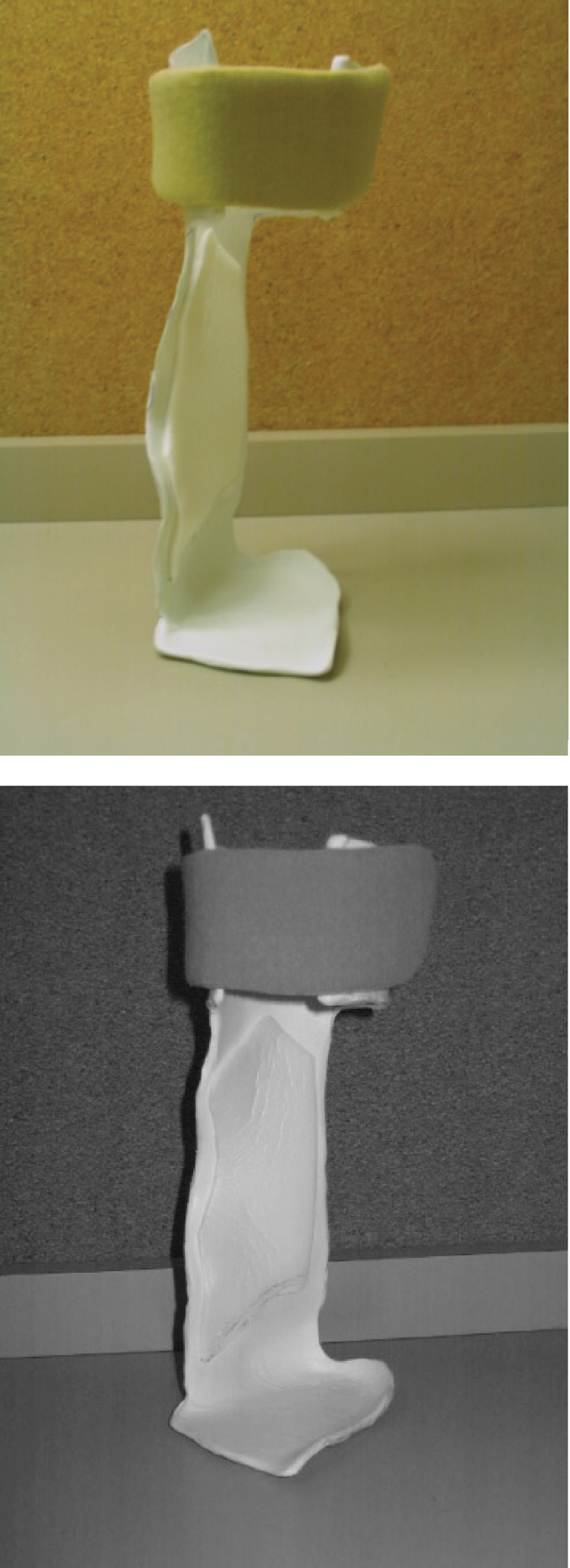
Left dynamic ankle orthoses.
Methodology
To assure human rights protection, the study was approved by a local Institutional Review Board. Participants also signed an informed consent form prior to participating in the study. Prior to data collection, a DAO was custom made for each participant and appropriate fitting PLAFO was selected. During testing, participants wore a comfortable pair of their own walking shoes without heels that could accommodate the orthosis and short athletic socks.
Electrodes (2 × 3 cm) were placed in a standardized position 2.5 cm apart running parallel to the muscle fibres for the TA muscle on the hemiparetic lower extremity. 21 Reflective markers (25 mm) were placed at the VICON Plug-In-Gait standardized anatomical positions including the anterior and posterior sacroiliac spines bilaterally, thighs, knees, tibia, ankles, heels, and toes. All EMG electrodes and reflective markers were placed on subjects by the same researcher. The researcher had previously established good intra-rater reliability with an intraclass correlation coefficient of >0.98 for all marker placements.
All trials were conducted on the same day and different orthoses were donned and doffed without altering the electrodes or reflective markers. All trials were randomized via a Latin square. 22
A repeated measures design was used such that participants were their own controls. Participants were instructed to walk at a comfortable speed to a cone that was 10 metres away. Data were collected over 4 metres in the middle portion of the distance to minimize the effects of acceleration and deceleration. Participants were asked to walk under three different conditions: (1) wearing shoes; (2) wearing a PLAFO and shoes; and (3) wearing a DAO and shoes. Prior to collecting data, participants were provided 5 minutes to become accustomed with each orthosis. Participants were allowed to use a cane for ambulation but were required to use the same device for all trials. Participants were asked to walk a minimum of 10 trials for each condition and were provided rest breaks for a minimum of 1 minute between each trial.
For each subject EMG data and velocity of gait were recorded and averaged from the first three strides where there was a clean foot strike on a force plate. 23 EMG data were filtered, enveloped, and area was computed using MatLab 6.1. A 10−500 Hz band pass filter was used to eliminate motion artifact. Root mean square (RMS) was used to create a linear envelope from the filtered EMG data making calculations from windows of 50 millisecond intervals. 24 RMS area was determined for the swing and loading phases of gait for the TA musculature for the hemiparetic lower extremity. Data from the EMG was segmented into phases of gait using vertical force measurements greater than zero from the force plates and visual confirmation from the VICON system. The loading phase of gait was defined as the time from initial contact of the hemiparetic foot until the sound limb was no longer in contact with the force plate. 25 The swing phase of gait was defined as the time when the hemiparetic lower extremity was no longer in contact with the floor until the hemiparetic lower extremity made initial contact with the floor. 25
Once the data was segmented, the area under the RMS envelope (RMS area) was calculated using the MatLab 6.1 trapezoidal numerical integration function. The RMS area calculations represent the power of the EMG signal over a percentage or phase of the gait cycle. All RMS integrals were normalized with the shoe-only trial so comparisons could be made across subjects. Figure 3 provides a representation of the EMG for one subject when walking with the different orthoses.
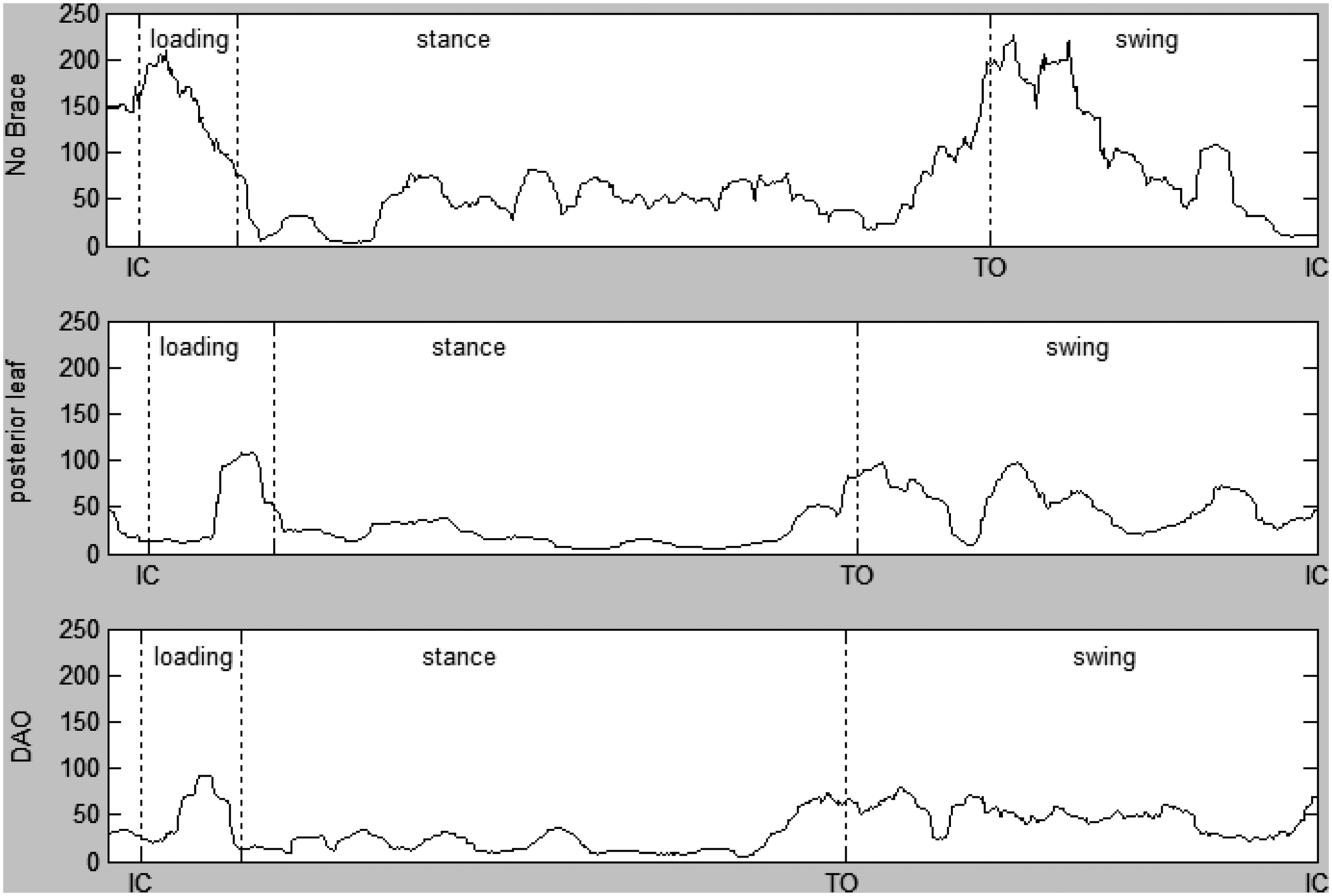
Example electromyography (EMG) for one subject. Measurements are in millivolts. Phases of gait are denoted by vertical lines. Stance includes the loading phase of gait. DAO, dynamic ankle orthosis; IC, initial contact; TO, toe off.
Kinematic data from the VICON were used to calculate sagittal ankle angles. The initial contact angle was taken at the point of initial contact of the hemiparetic lower extremity. The angle for midswing was calculated by determining the mean ankle angle from the middle one-third of the swing phase of gait.
Gait velocity was calculated by determining the time required to walk across the two force plates and dividing the time into the length of the force plates. Velocity measurements were averaged over the same three strides used for EMG calculations.
SPSS software was used for data analysis. The data were analysed using a repeated measures one-way ANOVA. Post hoc comparisons were conducted with a Tukey’s t-test with a Bonferroni adjustment of alpha. 22 A p-value of ≤ 0.05 was used to determine significance for all statistical tests.
Results
Tibialis anterior muscle EMG
A significant difference was observed in EMG during the swing phase of gait among the three conditions. Both orthoses demonstrated a decrease in EMG of the TA muscle during swing (Table 2). Post-hoc pair-wise comparisons revealed significantly less (p = 0.001) TA muscle EMG activity when participants walked with the DAO compared to walking without a brace (Table 3). A decline in EMG activity occurred when participants walked with the PLAFO compared to walking without a brace; however, the decline was not statistically significant (p = 0.089). No significant differences (p = 1.0) were observed when comparing the DAO and the PLAFO. There were no statistically significant differences in EMG during the loading phase of gait when comparing across the different braces (Tables 2 and 3).
Electromyography (EMG) descriptive statistics normalized to the shoe-only trial and p-values.

Values are mean percentages of milliamps as compared to the shoe-only trial ± standard deviation unless otherwise stated. DAO, dynamic ankle orthosis; PLAFO, posterior leaf-spring ankle-foot orthosis.
Repeated measures ANOVA table for electromyography (EMG).

Ankle angle
No significant differences were observed in ankle angle at initial contact or during midswing among the three conditions (Table 4).
Descriptive statistics and p-values for ankle angle.

Values are mean±standard deviation. DAO, dynamic ankle orthosis; PLAFO, posterior leaf-spring ankle-foot orthosis.
Gait velocity
No significant differences were observed in gait velocity among the three conditions (Table 5).
Descriptive statistics and p-values for velocity.

Values are mean±standard deviation. DAO, dynamic ankle orthosis; PLAFO, posterior leaf-spring ankle-foot orthosis.
Discussion
Tibialis anterior muscle EMG
The current research has shown a decrease in TA muscle EMG during the swing phase of gait with use of the DAO and a decline in EMG, although statistically insignificant, with use of a PLAFO. When comparing the DAO and the PLAFO, the normalized EMG were quite similar, at 80% and 82% respectively. However, a large variability was evident during PLAFO trials, as noted by the large standard deviation reported in Table 2. This variability likely accounts for the lack of statistical difference between the PLAFO and no brace conditions. The authors speculate the variability may have been a result of the inability to assure an optimal fit with the off-the-shelf PLAFO. A poor fit may have altered the gait and subsequently EMG secondary to pain or changes in spasticity. However, this issue is beyond the scope of this study and warrants further investigation.
The decrease in EMG during swing with use of a DAO suggests individuals 7 months or less post stroke may be limited in their ability to activate the TA muscle if they use a DAO during gait. However, use of an orthosis has been shown to increase walking. 13 An increase in walking could negate the decrease in TA muscle activity in a single gait cycle. Prior to making decisions about orthosis usage, one should consider the potential for an increase in the amount of walking when using an orthosis. An increase in amount of walking (steps taken) could offset a decrease in EMG during one step. Further longitudinal studies should be performed before definitive conclusions are made about use of the DAO or PLAFO post stroke.
Initially, it was hypothesized the DAO would exhibit more TA muscle EMG when compared to the PLAFO secondary to its less restrictive design. However, no significant differences were observed when comparing the DAO and the PLAFO EMG during the swing and loading phases of gait. The DAO is designed to allow more ankle motion in the sagittal plane than traditional AFOs. 15 However, like other AFOs, the DAO’s foot plate is functionally coupled with the shoe and thus provides sagittal plane stability during the swing phase of gait. This enhanced functional stability could potentially reduce the demand on the ankle dorsiflexors and result in the decreased EMG seen in the current study. Therefore, clinicians should not assume that use of a DAO or any other orthosis that is designed to allow freedom of sagittal plane movement will not decrease activity of the TA muscle. The less restrictive design does not translate into increased TA muscle activity. Therefore, use of a DAO instead of a PLAFO with the expectations of preventing a decrease in TA muscle EMG is unwarranted.
In contrast to EMG activity during swing, EMG of the TA muscle during loading was not decreased when either orthosis was worn. The plantarflexion moment at the ankle is elevated during the loading phase of gait with use of a PLAFO and during normal gait. 26 Resisting this plantarflexion moment requires maximal eccentric recruitment of the TA muscle to prevent foot slap. 26 Secondary to the less restrictive design of the DAO and PLAFO, continued recruitment of the TA muscle was required resulting in no significant differences in EMG during loading.
Ankle angle
Unlike previous studies 4,5,7,8 the current study demonstrated no difference in ankle dorsiflexion angle when comparing shoe-only ambulation to ambulation with a PLAFO or a DAO. These findings could be the result of methodological differences. One factor is previous studies used rigid orthoses or hinged orthoses with dorsiflexion assistance, whereas the current study investigated less rigid PLAFOs and DAOs. Another factor is the participants in the current study varied from having severe foot drop to having only minimal impairments during gait. If subjects with minimal impairment (manual muscle test score of 3+ or greater) are eliminated from the statistical analysis the remaining subjects exhibit improved ankle dorsiflexion during swing when wearing a PLAFO compared to using no brace. However, only six subjects met the aforementioned criteria, thus limiting the generalizations of this finding.
Gait velocity
In the current study, differences were not observed in velocity of gait when the different orthoses were compared to walking without a brace. Important to note, previous research with normal subjects has shown that an increase in TA muscle EMG is correlated with an increase in gait speed. 27 Since no difference in gait velocity occurred during the current research, the observed decline in TA muscle activity cannot be attributed to a slower velocity of gait.
Previous studies have shown increased gait velocity with use of articulated orthoses or rigid polypropylene orthoses.1–6,8,9,28 In contrast to previous studies, the current research found the PLAFO failed to significantly increase gait velocity. The current research has also shown no significant change in velocity with use of the DAO, indicating the DAO should not be used with individuals post stroke to improve gait speed. A study by Pohl and Mehrholz 29 and a study by Burdett et al. 30 have also revealed no change in gait velocity when orthoses of similar design were used.
Limitations
Only subjects who could walk without an orthosis or physical assistance were included in the current research. Yet, patients acutely post stroke are often unable to ambulate without physical assistance or without use of an orthosis. Therefore, future research should include subjects who are more impaired, but who have a good prognosis for regaining the ability to walk.
Subjects with plantarflexor spasticity require more TA muscle activity to dorsiflex the foot and overcome the resistance. Seven subjects with small degrees of plantarflexion spasticity were included in the current study. It would be prudent for future studies to investigate subjects with greater levels of spasticity.
Only short-term use of the orthoses was investigated. Geboers et al. 13 investigated the long-term effects on TA muscle EMG when a rigid AFO was used and found subjects’ EMG activity did not change with long-term use of the orthosis. Long-term effects on TA muscle EMG with use of different orthoses in patients post stroke should also be investigated.
Finally, nine subjects walked with some type of cane. It has been shown that use of a cane increases ankle dorsiflexion during swing 31 and causes a decrease in the burst duration for TA muscle EMG. 32 Both variables could affect the amplitude of EMG. However, using a repeated measures design and having subjects use the same assistive device throughout testing should control for any influence that using a cane may have had on TA muscle EMG.
Conclusion
Clinical significance from the current research is twofold. First, the use of relatively flexible DAO can cause a decline in TA muscle activity during the swing phase of gait. This supports therapists’ notions that bracing decreases TA muscle activity. Finally, neither the PLAFO nor the DAO should be prescribed to improve gait velocity for individuals who are able to walk without bracing.
Footnotes
Appendix A
Notes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.