
Abstract
Background:
Historically, the orthotic treatment in progressive myopathic scoliosis has not been as effective as expected. The purpose of this study was to investigate the effect of a spinal orthosis on scoliotic curve correction, alignment of altered posture and cardio-respiratory functions.
Case Description and Methods:
An 11 year-old girl diagnosed with myopathy was fitted with a custom molded thoraco-lumbo-sacral orthosis to enhance the sitting ability. The cardio-respiratory tests were performed by a COSMED K4 b2; metabolic analyzer. The anterior posterior radiographs were analyzed for measuring Cobb angle and Ferguson angle. A plumb line test was used to assess the postural improvements.
Findings and Outcomes:
No significant difference was observed for variables such as O2 consumption level, PaO2, tidal volume, heart rate and energy expenditure/min. The improved posture was evident by shifting of the plumb line 18 mm towards the mid line with the use of orthosis. Very minor improvements in both angles were observed with the use of the brace.
Conclusion:
The brace treatment cannot be expected to have a lasting corrective effect although it can be used as a sitting support and for maintaining posture
Clinical relevance
This case study provides an objective prescription of thoraco-lumbo-sacral orthosis as a sitting support and for improving posture in progressive myopathic scoliosis if suitably designed and properly fitted.
Background
Progressive scoliosis is frequently seen in myopathy due to weakness of the supportive musculature of the spine. A severe scoliosis compromises respiratory function and makes sitting more difficult. 1 The goal of treatment in myopathy is to balance the spine and the pelvis, generally for the purpose of sitting and to improve the alignment of altered posture. 2 An orthosis should be prescribed in case of a progressive scoliosis with a Cobb angle of more than 20° if both patients and parents reject a surgical intervention or if the general condition of health does not allow a surgical stabilization of the spine. 3 The orthoses used are generally considered as containment devices to control the idiopathic and acquired scoliosis. 4 Historically, the orthotic treatment has been said to be ineffective in stopping the progression of scoliosis,5,6 secondarily it is uncomfortable, not well tolerated6,7 and may cause some respiratory compromise from the brace pressure.6,8 This clinical report shows an 11 year- old Indian girl presenting with progressive myopathic scoliosis for rehabilitation of postural problem. Muscle biopsy enabled the definitive diagnosis of myopathy. This report emphasizes the effect of considering orthotic rehabilitation combined with physical therapy in myopathy, as it may negate the need for surgery in earlier stages.
Case Description and Method
An 11 year-old Indian girl was referred to the National Institute for the Orthopedically Handicapped (NIOH), with a history of muscle weakness and delayed developmental milestones (e.g. sitting at eight months, standing at 29 months and walking at 36 months of age). She was able to walk before seven years of age but there after due to gradual weakness of all four limbs the girl was unable to stand and walk. The child’s cognitive functions were normal, and she was interactive. Laboratory examination and electro diagnosis confirmed muscular disease or myopathy. There was no family history of neuromuscular disease.
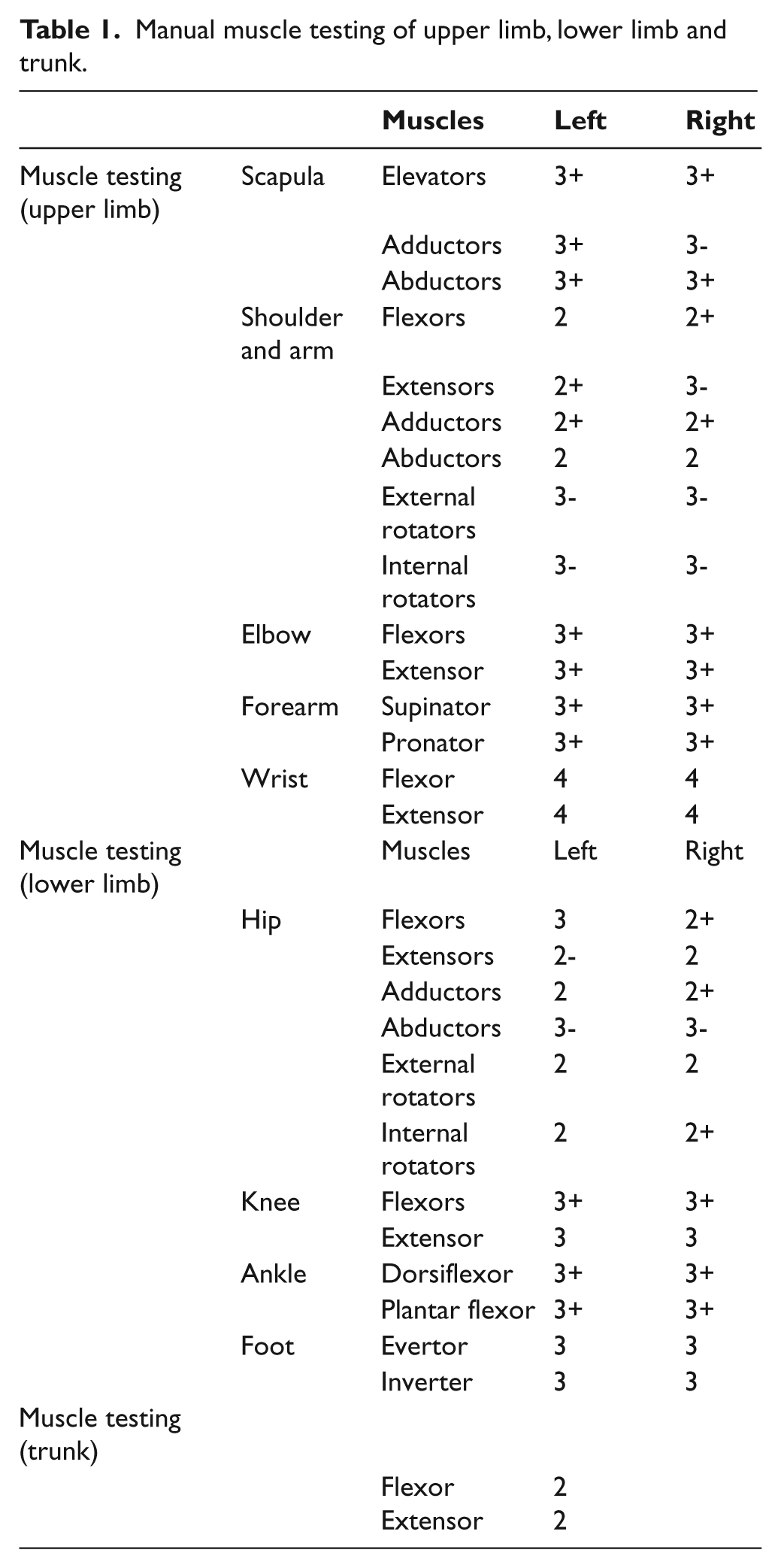
Prior to assessment and prescription the subject and her mother gave written consent to participate in this study. At presentation, the girl showed an elevated left pelvis and right shoulder, dorsal scoliosis, increased lumbar lordosis, thoracic hypokyphosis, bilateral flexed knees and plantar-flexed ankles in a sitting position (Figure 1). On examination, tightness in the hip extensors, hamstrings, gastrocnemius and left lateral trunk flexors were observed. Sensory examination results were normal. Manual muscle testing of upper limb, lower limb and trunk revealed proximal and symmetric weakness of muscles of both the upper and lower limbs (Table 1). Her tone was near to normal. A reduction in bulk of muscles was observed. Superficial reflexes like abdominal and plantar response were diminished and flexor type respectively. No elicitation in deep reflex for bilateral biceps, triceps, supinator, knee and ankle were observed. She was dependent in most activities of daily living for example feeding, eating, grooming, oral hygiene, etc. Hand functions evaluation revealed right hand dominancy with fair reach and good release ability. Chest expansion at axillary level, nipple and xiphoid process were 2.5 cm, 1 cm and 1.5 cm respectively. A pulse rate of 80 per minute and respiratory rate of 26 per minute were recorded.

Impaired posture with shoulder asymmetry and elevated pelvis.
Manual muscle testing of upper limb, lower limb and trunk.
Problems identified were poor sitting balance, inability to maintain the upright posture due to progressive dorsal scoliosis (Cobb angle 60 degrees), poor bed mobility and difficulty in overhead activities. The management planned was to continue physiotherapy utilising respiratory exercises, strengthening exercises for all four limbs and also including the trunk, stretching exercises for tight muscles, standing balance and bed mobility training. We planned for occupational therapy for enhancing hand functions by adaptive devices to make her independent and improve ranges of motion. A custom moulded bivalved thoraco-lumbo-sacral orthosis (TLSO) with an anterior abdominal opening (Figure 2) was planned and fabricated to maintain the good posture during sitting, to prevent the further progression of scoliotic curve, to support the weakened trunk musculature and to enhance the sitting ability. To maintain the level of pelvis, the wheelchair seating modifications were incorporated.

Anterior, lateral and posterior view of TLSO showing different trimlines.
General description of orthosis
Materials: The module consists of a bivalve copolymer polypropylene shell (4 mm thickness) with a soft liner of polyethylene foam.
Trimlines:
Anterior-Superior: up to sterna notch
Anterior-Inferior: 13 mm above pubic symphysis to just below ASIS providing sufficient clearance for sitting
Lateral-Superior: up to axilla level, not interfering with comfort.
Lateral-Inferior: 13 mm above greater trochanter
Posterior-Superior: up to scapular spine
Posterior-Inferior: as low as possible, not interfering with sitting clearance.
No additional pressure pads were provided in the orthosis, rather suitable modifications were done to make the orthosis as symmetric as possible (Figure 2).
The radiographic examinations were analysed with and without bracing conditions and the Cobb angle and Ferguson angle were compared. The spinal compensation and decompensation was measured by using plumb line from the middle point of occipital protuberance. The breath by breath analysis of the subject was carried out for cardio-respiratory functions with Cosmed k4b2 metabolic analyzer system (COSMED Srl – Italy) for the measurement of O2 consumption level (ml/min/Kg), PaO2 (mm Hg), tidal volume (TV) (ml), heart rate (HR) (beats/min) and energy expenditure (EE) per minute (Kcal/min) both in brace on and brace off conditions (Figure 3). The subject was psychologically normal during the test with no anxiety, stress or fear. Prior to the test, there was a five-minute rest period in order for her to get used to the system. Data were taken at normal room temperature whil in the sitting position.

Subject with k4 b2 metabolic analyzer system for cardio-respiratory functions test.
Findings and Outcomes
The summary of results for cardio-respiratory function tests is presented in Table 2. Data were acquired for four minutes (72 breaths), out of which the intermittent 30 breaths were used to produce the means. No difference was observed for variables such as O2 consumption level, PaO2, TV, HR and EE/Min in cardio-respiratory functions tests in brace on and brace off conditions. It was noticed that, the parameters like O2 consumption level, TV and EE/Min varied linearly where as PaO2 varied inversely to oxygen consumption rate (Figures 4 and 5).
Comparison of mean of cardio-respiratory function parameters in brace on and off conditions.

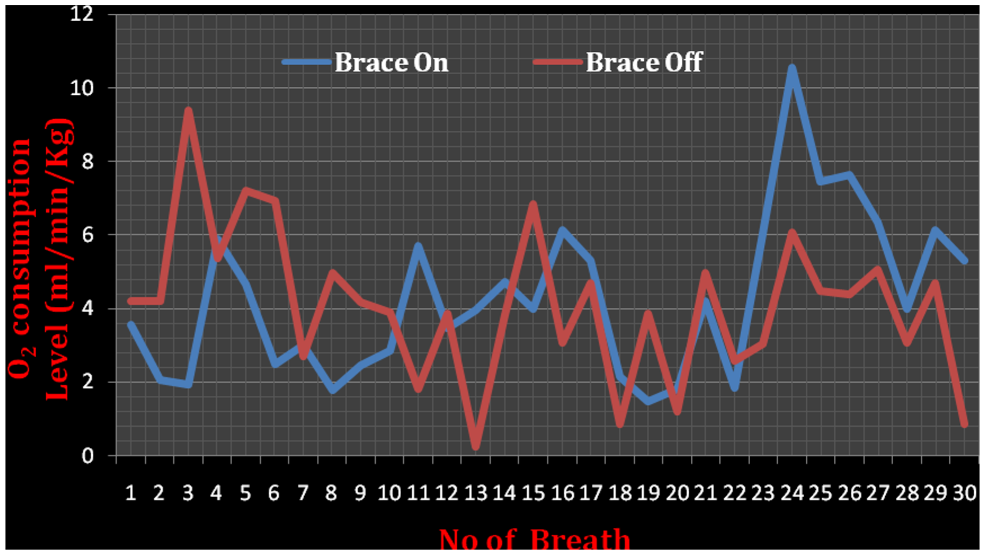
Line chart of oxygen consumption level with brace on and off.
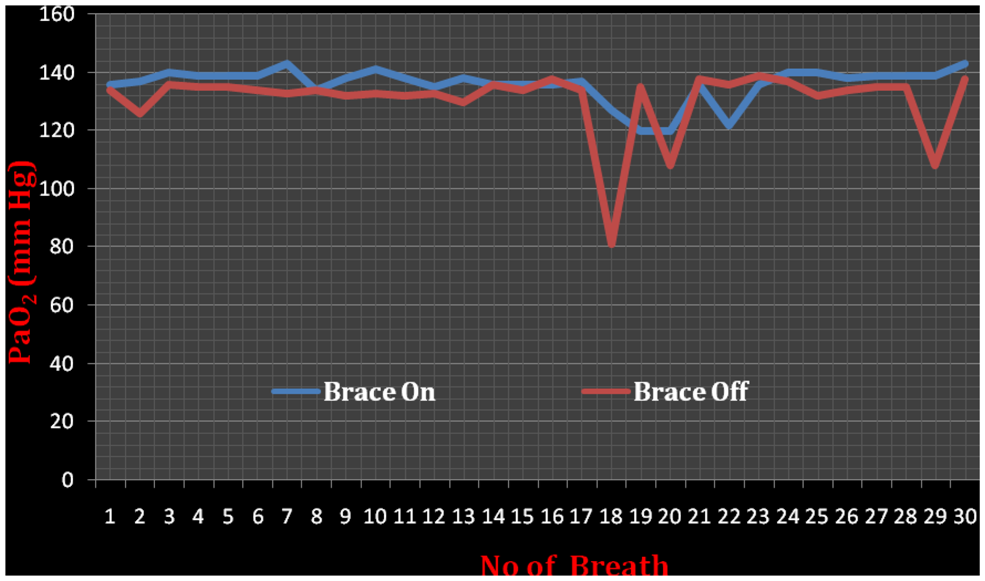
Line chart of PaO2 with brace on and off.
Postural improvements with plumb line test revealed that, the plumb line was shifted 18 mm towards the midline with the use of orthosis and vice versa. With improved posture, shoulder symmetry was achieved with brace on condition (Figure 6). It also improved the subject’s sitting ability and tolerance. She was able to sit for a period of two hours or more with brace on after three months of orthosis use. Regarding the main curvature (Cobb angle of 60 degrees) of the subject showed a c-shaped thoracolumbar scoliosis with its convex side to the right, a very minor improvement of 5 degrees and 3 degrees for Cobb angle and Ferguson angle was noticed for bracing and non bracing conditions respectively in A-P radiogram findings.

Improved posture with shoulder symmetry of the subject with TLSO.
Discussion
The purpose of this study was to determine the effect of spinal orthosis on scoliotic curve correction, alignment of altered posture, cardio-respiratory functions and balance of spine and pelvis in a subject with progressive myopathic scoliosis. Patients with myopathic scoliosis typically suffer from a host of pulmonary complications or restricted lung functions secondary to neuromuscular weakness. In our results, no difference was observed for variables like O2 consumption level, PaO2, TV, HR and EE/Min in cardio-respiratory functions tests in brace on and brace off conditions. It suggests that the subject was comfortable with brace on, though a minor decrease in O2 consumption level (0.016 ml/kg/min), TV (0.019 liter), HR (2.4 beats /min) and EE/Min (0.006 Kcal/min) was observed. The subject did not report worsening of any subjective symptoms of the respiratory discomfort while sitting in the orthosis. This may be due to the provision of anterior abdominal cutout provided in the TLSO so as to limit the extent of respiratory excursion. Earlier reports also emphasized the orthosis construction to improve the patients function in neuromuscular scoliosis. The inverse relation between O2 consumption rate and PaO2 is due to the fact that, the response to an increase in oxygen consumption is restricted to the patient’s ability to extract more of the available oxygen, thus decreasing PaO2.
Though reports have shown a temporal improvement of pelvic tilt, Cobb angle and comfort in sitting, trunk balance and of cosmetic appearance with improved posture, some results are contradictory. Gibson and Wilkins (1975) emphasized the importance of an early intervention using orthotic devices at the beginning of the wheelchair phase before the development of scoliosis. 3 However, Rideau and colleagues (1984) in spite of these measures concluded that in the progressive clinical situation the development of severe spinal deformation could not be avoided by an orthotic treatment. 9 In contrast, Letts and colleagues (1992) used a soft Boston orthosis in the management of neuromuscular scoliosis and noticed an improvement in the scoliosis with an average of 15 degrees, while the major advantage was a marked improvement in sitting stability in 80% of patients. 10 In another study, Olafsson et al. (1999) observed that mean brace-induced Cobb-angle correction was 60% with <10° curve progression during the observation time and a good brace compliance. 11 However, Mullender et al. (2008) did not recommend the use of orthosis to prevent the development or progression of scoliosis in myopathic patients. They advocated the use of a sitting type orthosis for patients who reject surgery for improvement of sitting comfort. 1 In contrast, Kotwicki et al. (2008) observed that a correctly designed orthosis was able to partially correct the spinal curvature and pelvic obliquity, provide a stable sitting position, balance the trunk, facilitate breathing, discharge the abdomen, and unload soft tissues of the buttocks. 12 In the present study, an improvement of 5 degrees in Cobb angle and 3 degree in Ferguson angle was observed in A-P radiogram analysis for brace on and brace off conditions. The same improvement was observed in the 15 week follow-up period. By supporting weakened trunk musculature, an improvement in sitting posture was achieved with good shoulder symmetry and improved sitting tolerance. The black points marked in the anterior part of the shoulder girdle clearly revealed the stable sitting position and cosmetic appearance (Figures 1 and 6). The subject was encouraged to continue the exercises and to actively keep her head straight, along with the orthosis which improved the sitting posture. A shifting of plumb line towards medial side by 18 mm was observed with brace on. Presently, the subject is continuing standing balance and other exercises which have led to gradual increase in muscle strength. Hence a knee ankle foot orthosis (KAFO) can now be planned.
The subject was wheelchair bound and had a very low sitting tolerance. To combat this, the ideal orthosis needed to work while the patient was in a seated position. The primary focus in this orthosis design was therefore to maintain a horizontal pelvis and a hyper-extended posture with the orthosis donned. Since orthotic management for this patient group involves provision of a containment device for limited correction of the spinal curvatures, the following objectives should be met when treating subjects with myopathic scoliosis, so that the orthosis:
avoids the further progression of scoliotic curvature
facilitates comfortable sitting position
facilitates unrestricted respiratory function by suitable orthotic modifications
improves the cosmetic appearance by improved posture.
In addition, it should not interfere with activities of daily living and should be easy to don and doff. However, the regular assessment of lung function is desirable to get the valuable information regarding the effect of orthosis and its tolerance and the time for spinal surgery, the last resort.
Conclusion
Controversy exists in the prescription and effect of spinal orthosis in myopathic scoliosis. Surgical intervention has been the most successful option. However, orthoses may be regarded as a temporary compromise for subjects who reject an operation or for patients who are inoperable because of their poor general condition. Thus it may be concluded that, a correctly designed and fitted TLSO can markedly increase patient’s acceptance, improve the sitting posture without cardio-respiratory discomfort in progressive myopathic scoliosis.
Footnotes
Acknowledgements
The authors would like to thank Dr. Asis Goswami, Mr. Durbadal Biswas, Mrs. Anuradha Ganguly, Mr. Arup Mukherjee & all staffs and students of MPO Training section, NIOH, Kolkata. Special thanks to our institute & the subject who cooperated us through out the study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
There is no conflict of interest.