
Abstract
Study Design
Ambispective study.
Objectives
To determine the long-term natural history of non-surgically treated patients with myopathy and spinal deformity.
Methods
Data were analyzed from 118 files from a children’s rehabilitation hospital. Seventeen patients were operated on; the remaining 101 patients (86%) were managed conservatively. Retrospective data included demographics, medical history, respiratory and mobility status, Cobb angle (CA), and pelvic obliquity (PO). Prospective data were obtained via telephone interviews and included the Scoliosis Research Society (SRS-22r), World Health Organization Quality of Life (QoL) (WHO-QoL) and Functional Independence Measure for Children (WeeFIM).
Results
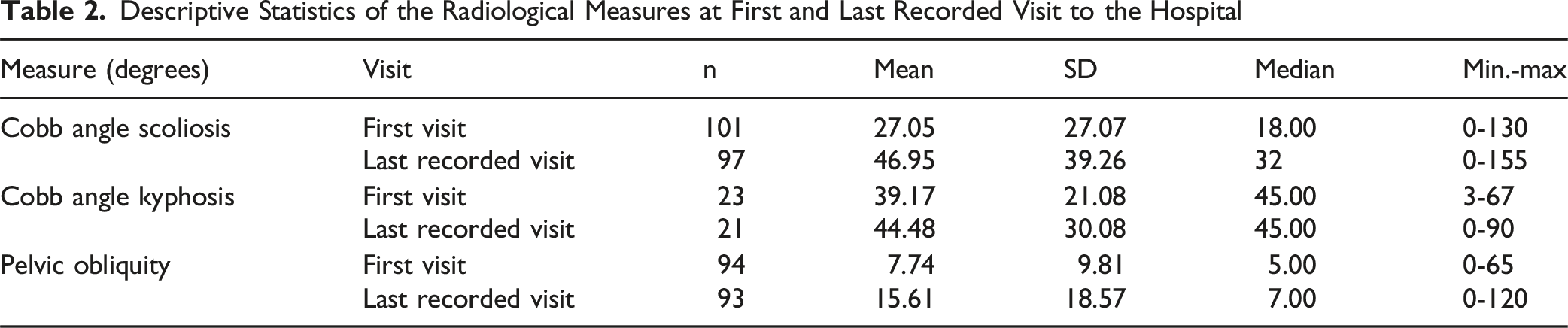
One hundred and one patients with myopathy and scoliosis did not have surgery and were followed for up to 33 years. Their mean age at first visit was 5.45 ± 5.27 years. CA and PO at the first visit were 27.05 ± 27.07 and 7.74 ± 9.81°, worsening to 46.95 ± 39.26 and 15.61 ± 8.57° at last visit. Respiratory data for 67 patients showed 45 who remained stable and 14 who worsened moderately and 5 severely. Mobility status worsened but not significantly. Of the 24 participants who responded to the survey (mean age 17.41 ± 10.84 years), 92% are single or divorced. They reported being generally satisfied with their QoL, although their functional scores indicated limited independence.
Conclusions
Despite worsening of scoliosis and limited independence, participants were generally satisfied with their QoL.
Introduction
The term myopathy refers to a large group of diseases affecting the voluntary muscles (limbs, pelvis, back, face and breathing). These diseases can be divided into acquired diseases or hereditary (genetic) such as congenital muscular dystrophy, Nemaline myopathy, fiber-type disproportion congenital myopathy. The main symptom of myopathy is weakness and wasting of muscles. The large muscles are usually affected although any voluntary muscle may be, depending on the type of myopathy. Muscle weakness is manifested by difficulty and weakness in a range of functional activities. 1 As the disease progresses, patients lose head control, and trunk imbalance develops together with discoordination. 2 At this stage, the neuromuscular scoliotic deformity increases, presenting as a long C-shaped curve in the coronal plane including the sacrum leading to pelvic obliquity. The compromise in muscular support of the vertebrae leads to a collapsing deformity, and the scoliosis becomes structural over time.
Prevalence of scoliosis in myopathy is up to 90%, with rapid worsening of 16-24° per year during the peak growth period.3,4 This is associated with a reduction in lung function of 4-8% of vital capacity for every 10% Cobb angle.4,5 Additionally, people with neuromuscular scoliosis typically have an impaired ability to perform activities of daily living (ADL). Progressive disease may lead to reliance on a wheelchair for mobility. As the deformity worsens, loss of sitting ability makes treatment of these children extremely difficult.3,6 The loss of the ability to walk and sit in a wheelchair accelerates the development of scoliosis, although the reasons for this are not completely clear.3,6
Treatment options of scoliosis in myopathic patients are very limited. Development of disease modifying drug treatment such as steroid treatment for Duchenne MD resulted in the preservation of mobility, improvement in muscular strength and respiratory functions. Maintaining mobility over time resulted in a significant reduction in the progression of scoliosis and the age of its development, and thus steroids are considered to be a modifier for the course of the scoliosis.4,5 The use of a corset has been proven to be effective in idiopathic scoliosis.3,7 This treatment has not been proven to prevent or delay the development of scoliosis and is not considered effective in myopathic scoliosis.4,5 When scoliosis progresses and pelvic obliquity is present, surgery is considered. At this stage patients are usually confined to a wheelchair, so the purpose of surgery is to improve the ability to sit, and prevent further deterioration of scoliosis and respiratory volume secondary to the worsening of scoliosis. 8
Due to the low prevalence of myopathy 9 few studies have examined the questions related to optimal treatment options, function and quality of life. The aim of the current study was to characterize the long-term course of scoliosis in patients diagnosed with various myopathies who did not undergo surgery, and determine their daily functioning, pain, satisfaction and quality of life. A preliminary version of the results was presented at the 2023 Global Spine Congress. 10
Materials and Methods
Study Design
The study used an ambispective design. As indicated in Figure 1, retrospective data were retrieved from the hospital database (1990-2022) as well as archived files. These data were supplemented by survey data obtained during a telephone interview during September to October 2022, including SRS-22r Quality of Life (QoL), WHO-QoL and Functional Independence Measure for Children (WeeFIM). The research protocol was approved by the ALYN Hospital Ethics Committee in accordance with the provisions of the World Medical Association Declaration of Helsinki (approval number 054-22). Informed consent has been obtained from participants of the telephone survey. Number of Participants in All Stages of Analysis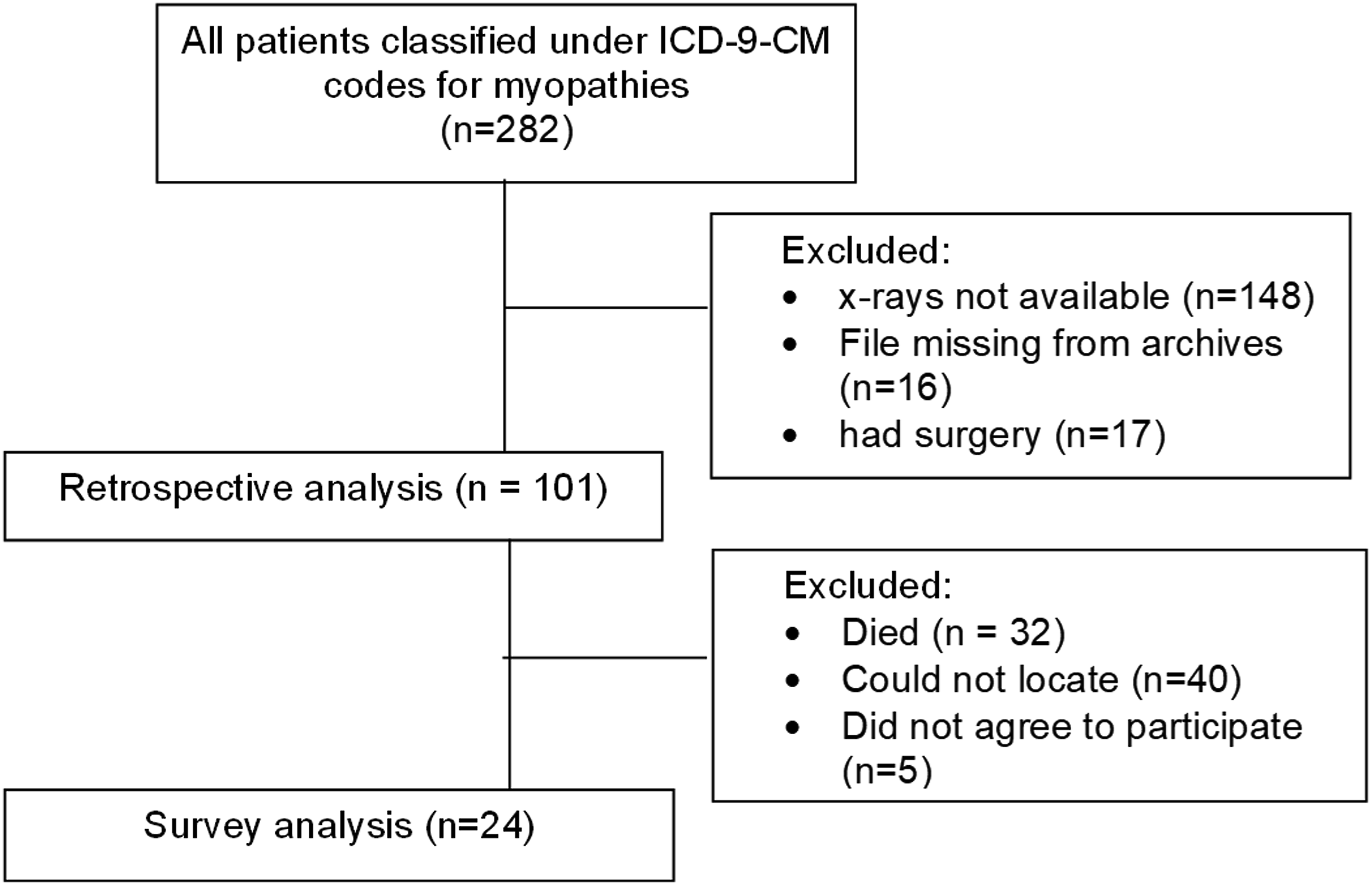
Patients and Research Team
Patients were included in the study if they were classified under the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes for myopathies. 11 The general diagnosis for myopathy was uniform and included all subgroups. Patients whose x-rays could not be retrieved were excluded from the study. Conservative treatment for our patients includes physical therapy, wheelchair adjustment for upright sitting, and for most patients, TLSO are used to support trunk position while sitting. During rehabilitation periods patients receive respiratory physical therapy and occupational therapy regularly, as well as dietitian evaluation. Emotional support is provided for both patients and caregivers. These treatment strategies were consistent throughout the study period.
One-hundred and eighteen patient files (55% males, 45% females) that met the study inclusion and exclusion criteria were retrieved from the hospital’s electronic medical records. Seventeen patients were operated on; the remaining 101 patients (86%) were managed conservatively and are the focus of the current analysis. These patients attended outpatient clinics for a minimum of 3 visits over a period that spanned up to 33 years. The mean and median time between the first and last recorded clinical visit were 11.63 (SD: 6.85) and 11.67 years.
While collecting the ICD-9-CM diagnoses, each of the files was reviewed manually by the researchers to confirm the diagnosis (AS, SE), updated to the latest diagnosis in patients who underwent Axom exam. The mean ± SD length of follow-up between the first and last recorded visits was 11.63 ± 6.85 years. The team included 1 pediatric orthopedic rehabilitation specialist (SE), 2 pediatric spine orthopedic surgeons (JES, AS), 1 medical student (RH) and 2 research methodology experts (AR, PLW). One of the pediatric spine orthopedic surgeons (AS) performed all the radiological measurements. Treatment protocols have been consistent over the years.
Context
The study took place at ALYN Hospital, a Pediatric & Adolescent Rehabilitation Center that serves children with physical medical and complex challenges, providing a wide array of rehabilitation services with the goal of promoting healthy, independent lives as adults. It is a 120-bed hospital, with twice as many children receiving care on an ambulatory basis. Due to our rehabilitation hospitals’ role as a referral center, treatment protocols were determined by other clinicians.
Instruments
Demographic and Medical Questionnaire
Data included general demographics, medical history, respiratory and mobility status.
Cobb angle
Cobb Angle is used to determine scoliosis severity and progression. It is measured by drawing lines parallel to the upper and lower boundaries of the upper and lowest vertebrae of the structural curves of the spine. Then, erecting perpendiculars from these lines to cross each other creates the Cobb Angle. 12 The Cobb Angle, assessed using a standing coronal radiograph of the entire spine, is considered the gold standard assessment for scoliosis. 13
Pelvic Obliquity
Pelvic obliquity is a misalignment of the pelvis, defined by the rotation of the pelvis in the coronal plane. It was measured using the Maloney Method; a first line was drawn across the superior aspects of the iliac crests, and a second line was placed perpendicularly to that line. A third line was drawn between the centers of T1 and S1. The pelvic obliquity was defined as the angle formed by the intersection of the second and third lines. The Maloney Method was found to be highly reliable (ICC = 0.96).14,15
The following questionnaires were completed via the telephone survey
World Health Organization Quality of Life (WHOQOL)-BREF
The WHOQOL-BREF is a 26-item questionnaire designed to measure self-reported quality of life. It was found to have high internal consistency reliability (α = 0.92), good test-retest reliability (r = 0.66-0.72) and good concurrent validity. 16
Scoliosis Research Society-22 revised (SRS-22r Quality of Life)
The SRS-22r is a questionnaire designed to assess health-related quality of life among young adults with adolescent idiopathic scoliosis. It was found to have high reliability (ICC = 0.61-0.9) and good concurrent validity for most domains (Cronbach α = 0.71-0.85). Activity\function and satisfaction with management domains had lower concurrent validity (Cronbach α = 0.44-0.58).17,18
Functional Independence Measure for Children (WeeFIM)
The WeeFIM is an 18-item instrument aimed to evaluate disability in children. It was found to be reliable (ICC 0.80-0.99),19,20 and to have high concurrent validity in self-care, transportation/ locomotion, and communication/social function domains (r > 0.88). 21
Data Retrieval and Analysis
No correlations between diagnostic subgroups and the primary research outcomes were found and so in all subsequent analyses they were treated as a single group. Data were described by frequencies and percentages for the categorical and ordinal variables and by means, medians and standard deviations for the numerical variables. The Wilcoxon signed rank test was used to determine significant differences of change over time for scoliosis, kyphosis and pelvic obliquity; the McNemar-Bowker test was used to determine significant differences of change over time of the mobility and respiratory state of the patients. Spearman’s r and Pearson’s chi-square tests were used to assess magnitude and significance of associations between variables of interest. Analyses were carried out using SPSS V26 and R V4.3.1 software. Results were considered to be statistically significant at P ≤ 0.05.
Results
The mean age and median at the participants’ first visit were 5.45 years (SD: 5.27) and 3.10 years (Min.-Max.: 0.27-18.60). Their mean and median current age were 31.22 years (SD: 16.64) and 34.25 (Min.-Max.: 5.07-72.00).
Distribution of Diagnoses in Accordance with ICD-9-CM Guidelines
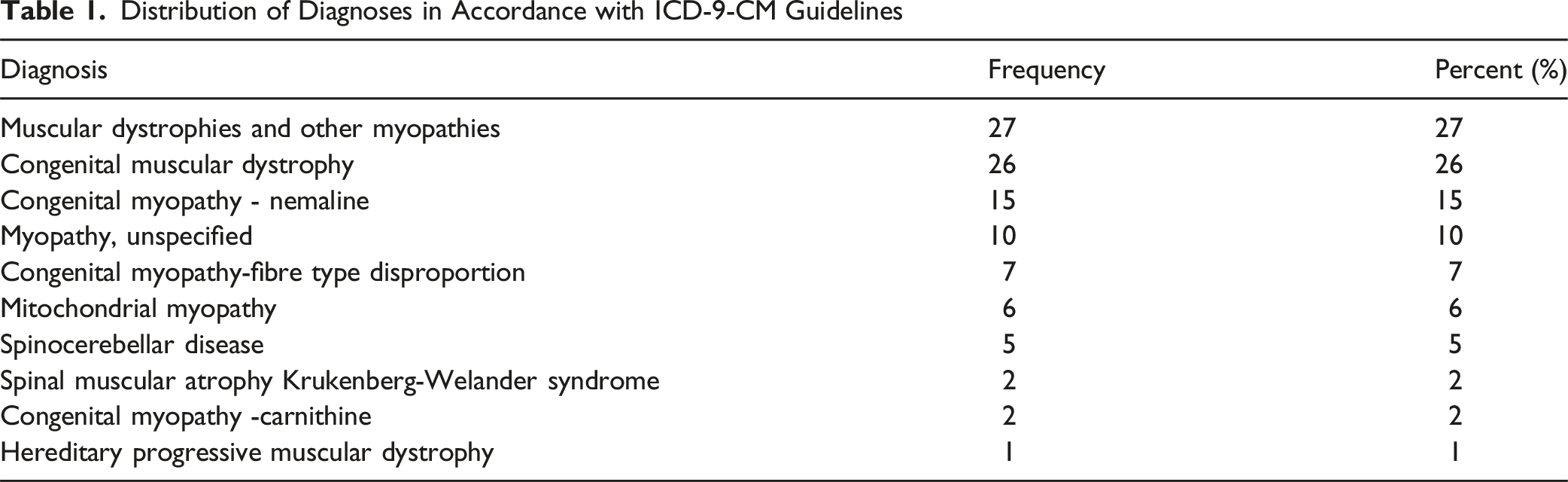
Sixty-seven (66%) of the patients had involvement of the limbs including contractures, ataxia, waddling gait, Gower’s sign or difficulty with head control, hip dislocation, calf hypertrophy, hyper-flexibility and spasticity. Eighteen patients (18%) had surgeries to the limbs including hip tenotomies, Achilles tenotomies, acetabular and/or hip osteotomy. Nine patients (9%) had a gastrostomy for feeding.
Spinal Deformity
Radiological data were recorded over a time span of 32 years. Patients’ mean age ±SD at the time of the first radiology recording was 8.18 ± 6.38 years (Median = 6.34, Minimum = 0.27, Maximum = 35.42). At the time of the last radiology recording, it was 15.19 ± 8.61 years (Median = 13.98, Minimum = 1.35, Maximum = 46.44). Mean duration between these visits was 7.28 ± 6.70 years (Median = 5.14, Minimum = 0.42, Maximum = 32.41). A bi-modular distribution of the initial Cobb angle was observed; the first peak had a mean of 25° in the early monitored group, and the second peak had a mean 55° in the late monitored group (ie, patients who likely started their follow-up monitoring at a stage where their scoliosis had already progressed).
Descriptive Statistics of the Radiological Measures at First and Last Recorded Visit to the Hospital
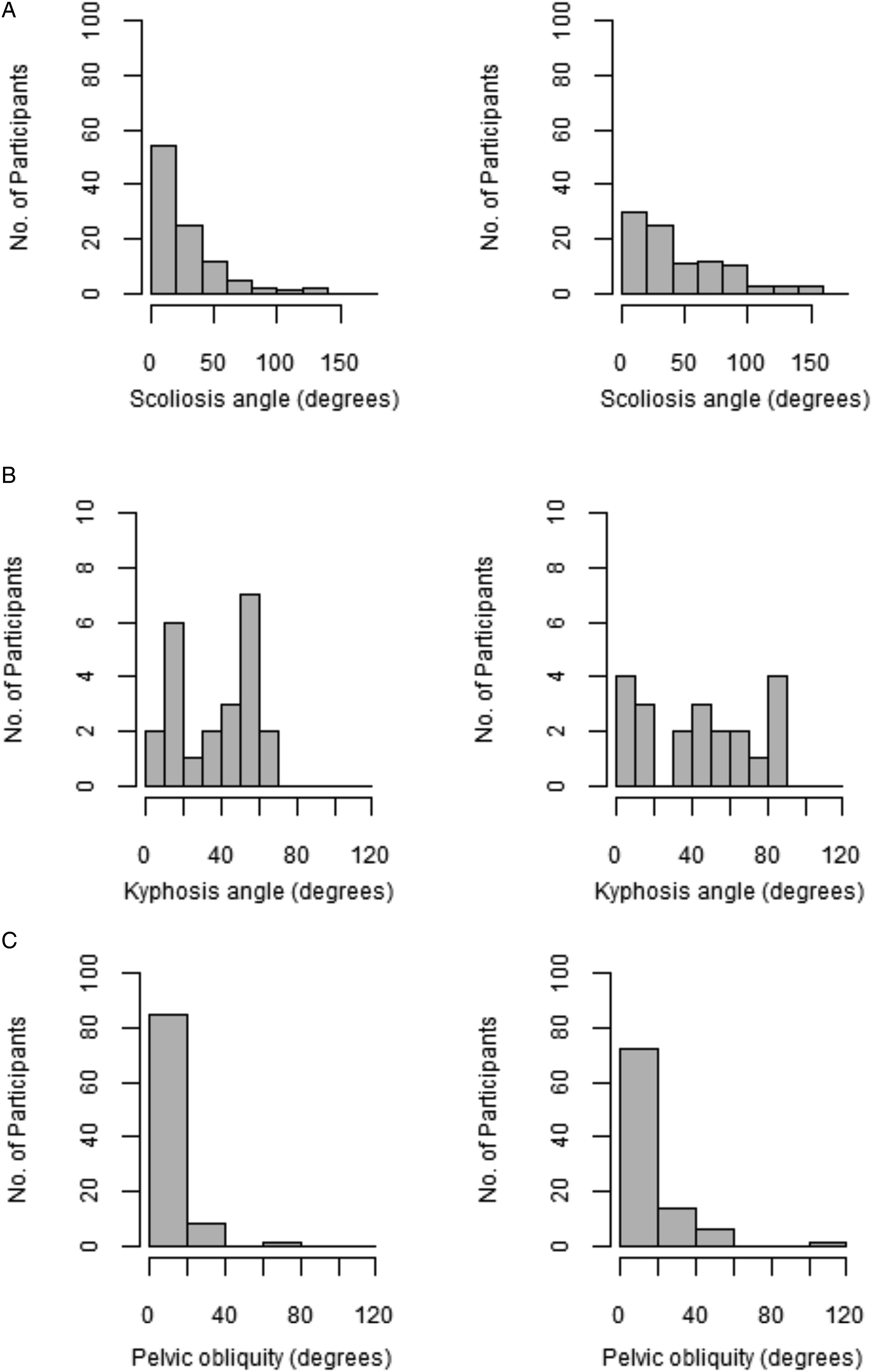
(a) Distributions of Cobb Angle Scoliosis at First (Left Graph) and Last (Right Graph) Visits (b) Distributions of Kyphosis Angle at First (Left Graph) and Last (Right Graph) Visits (c) Distributions of Pelvic Obliquity at First (left graph) and Last (Right Graph) Visits
In 37 patients (37%) the scoliosis angle did not change between the visits (change of less than 5°), in 57 patients (56%) the scoliosis got worse (ie, the angle increased) and in 3 patients (3%) the scoliosis got better (ie, that angle decreased). Regarding the latter patients, the improvement across time was not large (∼10°); in 1 patient there was a substantial worsening of the kyphotic angle which may ‘compensate’ for the worsening in the scoliotic angle. In 4 patients (4%) these data were missing. A greater proportion of female scoliosis angles worsened (31, 71%) compared to males (26, 52%); however, this difference was not significant (Χ2(1) = 3.34, P = 0.07).
Out of the 101 patients with scoliosis who were treated conservatively, only 28% were recommended to be treated with a corset. Data concerning the use of the corsets and their effectiveness were not available.
Respiratory Status
During the first visit 67 (66%) patients breathed independently, 5 (5%) used a bi-pap (bilevel positive airway pressure) ventilator or a respirator at night and 6 (6%) had a tracheostomy; these data were missing in 23% of participants. At the last recorded visit, 40 (40%) patients breathed independently, 17 (17%) used bi-pap ventilator or a respirator at night and 10 (10%) had a tracheostomy; these data were missing in 33% of participants.
The respiratory status (Figure 3) for 45 (45%) patients remained the same between the first and last recorded visit; it worsened moderately for 14 (14%) patients (ie, they changed from breathing independently to using a bi-pap ventilator or from using a bi-pap ventilator to a tracheostomy). Breathing status worsened severely for 5 (5%) patients (ie, they changed from breathing independent to using a tracheostomy). The respiratory status of 2 (2%) patients improved between the first and final visits; whether this improvement was maintained or their status declined at a later stage was not reported. Patients’ respiratory status worsened with time; the percentage of bi-pap ventilation was more than 4 times higher, and the use of tracheostomy was 1.5 times higher. These changes were statistically significant (McNemar-Bowker test = 22.00, df = 6, P = 0.001). Percentage of Participants for Each Breathing Status at First Visit (Black Columns) and at Last Visit (Grey Columns)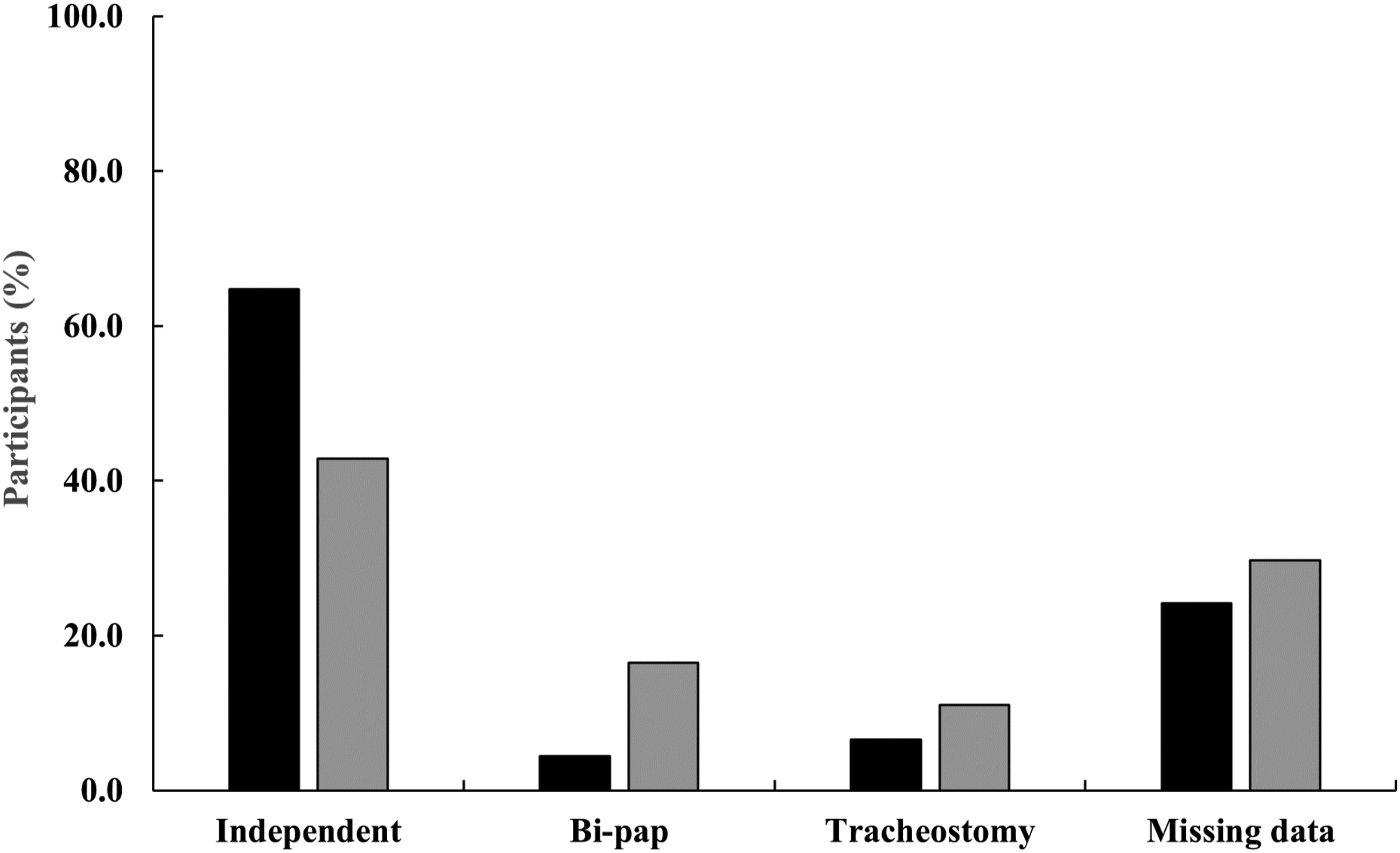
Looking at the change in respiration in concordance with the change in scoliosis the results demonstrated a greater proportion of patients whose scoliosis angle deteriorated for patients whose breathing status worsened moderately (9, 64%; 4, 31%) or severely (4, 80%, 1, 20%). This association did not reach statistical significance probably due to the small number of patients in each category.
ADL and Mobility
During the first visit, 2 patients (2%) were independent in ADL, 10 (10%) occasionally required help, 16 (16%) required help daily and 48 (48%) were completely dependent; these data were missing in 26% of participants. Eighteen (18%) patients were independent in mobility, 21 (21%) used mobility accessories, 36 (36%) were not mobile (1 of them was very young at his first visit, hence could not walk by definition); these data were missing in 25% of participants. At the last recorded visit, 12 (12%) were independent in mobility, 10 (10%) used mobility accessories and 51 (51%) were not independently mobile; these data were missing in 27% of participants.
Mobility status did not change for 33 (33%) patients between the first and last visits; it worsened moderately for 19 (19%) patients (ie, from independent to using assistive devices or from using assistive devices to not independently mobile) (Figure 4). Mobility worsened severely for 7 (7%) patients (ie, from independent to not independently mobile). Interestingly, the mobility status of 10 (10%) patients improved over time. Overall, their mobility status worsened with the percentage of patients who were not independently mobile increasing by about 1.4 times, although the differences were not statistically significant (McNemar-Bowker test = 8.52, df = 6, P = 0.20). Percentage of Participants in Each Mobility Status at First Visit (Black Columns) and at Last Visit (Grey Columns)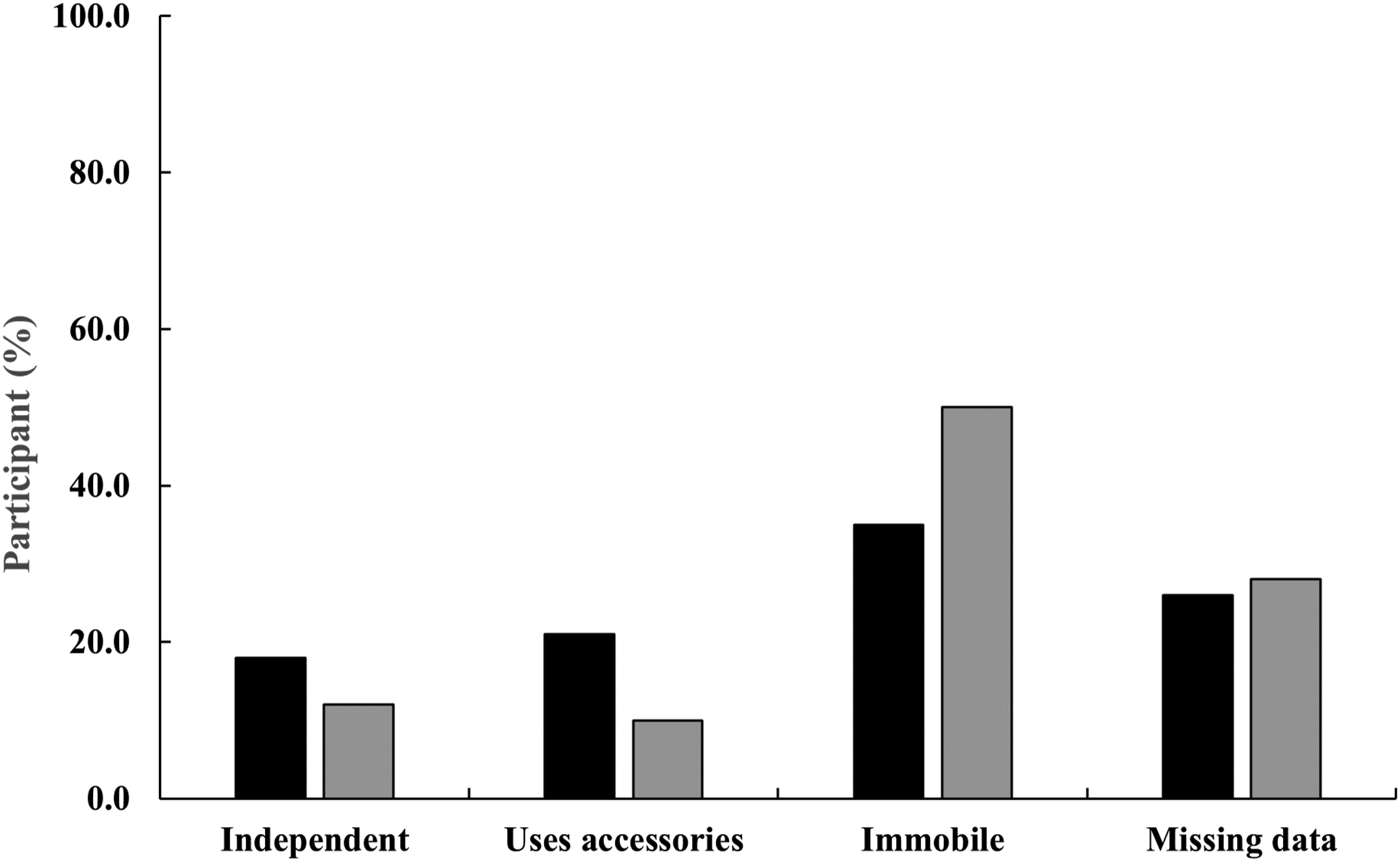
Looking at the change in mobility related to the change in scoliosis, the results were mixed without any significant correlation between the two.
Survey Data
Of the 101 patients in the cohort, 32 (32%) died by the time the survey took place. Mean and median age of death (from the available data) were 24.88 years (SD: 15.68) and 23.50 (Min.-Max.: 4.13-52.73). Out of the 69 patients who, to the best of our knowledge, still lived at the time of the survey, 29 (42%) were reached by telephone and 24/29 (83%) completed the survey (questionnaire respondents); ie, 40/69 (58%) were lost to follow-up. The mean age of the respondents was 17.41 (SD = 10.84), 67% (n = 16) females, most of them single or divorced (92%, n = 22). Twenty-one (88%) indicated good to moderate socio-economic status and 17 (71%) indicated that their general health is good. Limb involvement, other than the spine, was reported by all the participants. Twenty-one (88%) reported that they receive physical therapy (21/24) and hydrotherapy (11/24). Most of them reported using orthotics in the past (92%, n = 22) and most of them (75%, n = 18) reported of limited mobility, ie, using wheelchair operated by another person. Other surgeries were also very common (71%, n = 17). The mean reported height of the questionnaire respondents was 142 cm (SD = 19), mean reported weight was 33 kg (SD = 23) and their mean BMI was 16.95 (SD = 5.81).
Their median WHO-QOL BREF score was 3.74 (Q1-Q3: 3.14-4.15), indicating that, overall, the participants are satisfied with their quality of life, although their median FIM score was 2.89 (Q1-Q3:2.50-3.89), which indicates limited independence. Regarding the SRS, lowest scores were found in the function activity domain (M = 2.23, SD = 1.12); while the other domains received approximately equal levels of satisfaction (General function: M = 3.68, SD = 0.48; General self-image: M = 3.81, SD = 0.84; Pain: M = 3.81, SD = 0.67). The association between the change of scoliosis angle and these measures was negative for most measures indicating that a greater angle change (ie, worsening of the scoliosis) was associated with lower scores regarding QOL and functioning. Since the sample was small, these correlations did not reach statistical significance; however, 2 were medium in their magnitude: pain (rs = −0.35, P = 0.10) and function activity (rs = −0.32, P = 0.14).
Discussion
Myopathy is a rare condition but those who reach adulthood face multiple daily life challenges. 22 A common characteristic of people with myopathy is a C-shaped scoliosis. The curve progresses with a decline in mobility, leading to deterioration in respiratory status.
In the current study, progression in scoliosis magnitude was observed as measured by the Cobb angle and pelvic obliquity. Early and long-term follow-up enabled detection of scoliosis at young ages, with a bi-modular distribution. Patient gender was the only factor associated with scoliosis progression. Since female gender is a known risk factor for other scoliotic deformities, especially during their adolescent growth spurt, this finding is not surprising. 23
Concerning respiratory function, the literature reports both relative weakness of intercostal and diaphragmatic muscles and scoliosis progression may contribute to deterioration in respiratory status, 5 resulting in lung infections and bronchial secretions. 24 No statistical association was found between the respiratory deterioration and the scoliotic deterioration. About 50% of the patients did not deteriorate in their respiratory function, of these most continued to be independent breathers. That is, there is no support for the need to operate on the scoliosis in order to maintain respiratory status. This may be attributed to tailor-made conservative respiratory treatment (e.g., physical therapy). With regard to the natural course of mobility status in myopathic patients we found no specific dependence on the progression of the scoliosis. This may be explained by the heterogeneity of myopathic pathologies as described.2,25
Of the 69 living patients whose data were analysed retrospectively, 24 patients responded to questionnaires. This 35% response rate may be attributed to the long-term follow-up of these patients. The patients reported overall satisfaction with their quality of life despite dissatisfaction with their overall function. Correlations between scoliosis progression and decreased ratings of QoL and the function domains (especially pain and function activity) were found, although they did not reach statistical significance. Due to the relatively small number of respondents, it is not possible to account for the unexpectedly good QoL, but it may be related to the local socially-based medical and welfare support systems that ensure a reasonable socio-economic lifestyle. 26
Limitations
There are several limitations to this study. First, only patients with myopathies who had documented scoliosis were included; the relatively small number of patients who did not have a documented radiological scoliotic deformity were not studied. Second, the retrospective studies tend to result in less-than-optimal uniformity in their databases. In the current study there was remarkable long-term stability of the clinical staff resulting in a good uniformity of recorded data outcomes. Third, patients with partial radiographic data could not be analyzed, leading to some bias in the final results. Fourth, because of the rare nature of these disorders, the overall number of patients is small and did not permit subdividing the cohort into subtypes of myopathy. Nevertheless, to date, this is the largest report of non-operated patients with myopathic scoliosis. Fifth, recent studies show relatively low response rates (33%-65%) to follow-up phone calls post-discharge, particularly for patients who were treated many years prior to the survey.27,28 A higher response percentage would have allowed for additional statistical analysis. Finally, we fully acknowledge that the use of instruments such as the SRS-22r, WHO-QOL BREF, and WeeFIM introduces the potential for recall bias and response bias, particularly in a population with long-standing, progressive conditions.
Conclusion
A comprehensive study was conducted of the long-term follow-up of patients with myopathic scoliosis who were treated without surgical intervention in their childhood. Several trends were observed of non-progression in respiratory and mobility status independent of scoliosis progression. We found that even without surgical treatment, these patients maintain an inclusive and relatively active lifestyle including quality of life and satisfaction. These findings should be considered when discussing scoliosis with patients and their family members. A companion study comparing patients who underwent surgery to the current cohort will be presented in a subsequent paper. This will help to understand the impact of the natural history relative to surgery.
Footnotes
Ethical Consideration
The research protocol was approved by the ALYN Hospital Ethics Committee in accordance with the provisions of the World Medical Association Declaration of Helsinki (approval number 054-22).
Informed Consent
Informed consent has been verbally obtained from participants of the telephone survey.
Author Contributions
Conceptualization, S.E., J.E.S. and A.S; methodology, S.E., R.H. and A.S.; formal analysis, A.R.; investigation, S.E., R.H. and A.S.; writing—original draft preparation, S.E., P.L.W., A.S.; writing—review and editing, S.E., J.E.S., A.S, A.R., P.L.W. and R.H.; visualization, A.R. and P.L.W.; supervision, S.E.; project administration, S.E.; funding acquisition, S.E. and P.L.W. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Leona M. and Harry B. Helmsley Charitable Trust (grant no. 2207-05386).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.