
Abstract
Background:
It is difficult for the lower limb amputee patients to adapt to their new lifestyles.
Objective:
To compare the life quality and functionality of patients with bilateral vs. unilateral lower extremity amputations.
Study Design:
Cross-sectional study.
Methods:
Fifteen bilateral and 15 unilateral lower extremity amputee patients were enrolled. Demographics, cause and level of amputations, frequency and duration of prosthesis use were evaluated. SF-36, Satisfaction with Prosthesis Questionnaire (SAT-PRO), Amputee Body Image Scale.
(ABIS), Houghton Scale (HS), six-minute walk test (6MWT), and 10-metre walk test (10 MWT) were performed.
Results:
Physical function, physical and emotional role scores of SF-36 were significantly lower in the bilateral amputee group in comparison with the unilateral group. SAT-PRO and ABIS total scores were similar between the groups. There was a positive correlation between the frequency of prosthetic use and SF-36 subgroups (except pain). The unilateral amputee group had significantly better scores than the bilateral amputee group in terms of HS, 6MWT and 10 MWT.
Conclusion:
Physical capacity of bilateral lower extremity amputee patients is lower than the unilateral amputee patients; satisfaction with prosthesis and body image are not related with the amputation level; and the life quality and satisfaction with prostheses are increased in parallel with the use of the prostheses.
Clinical relevance
Although differences exist between the groups, in terms of quality of life and functionality, patients can reach an acceptable life standard with good rehabilitation and a suitable prosthesis.
Background
Patients with lower limb traumatic amputations are exposed to several physical and psychosocial problems regarding body image, self-care activities, mobility, occupational or non-occupational activities. 1 Likewise, previous studies have focused on the comparison either between amputee vs. healthy/salvage subjects2-4 or between amputees with different amputation levels. However, sufficient data do not exist on the comparison between uni- vs. bilateral amputations.
In this study we aim to comparatively assess the prosthesis usage, life quality and functional ambulation of unilateral vs. bilateral lower extremity amputee patients.
Materials and methods
Participants
This study was performed among 15 bilateral and 15 unilateral lower extremity amputee patients (aged 21–43 years) who had been under follow-up at Turkish Armed Forces (TAF) Rehabilitation and Care Center. The patients were recruited from a sample of consecutive patients attending the clinic during a six-month period in 2010. Thirteen above knee amputee extremity had prosthesis with ischial containment socket, hydraulic joint and solid ankle cushion heel (SACH) foot. All of the 22 below knee amputees had endosceletal (modular), with patellar tendon bearing socket and SACH foot prosthesis. Fourteen below knee amputee extremity had pelite liner and the other eight had silicon liner socket. Subjects were enrolled if they had completed primary wound healing (a period of at least six months after amputation) and a previous rehabilitation program. Those who had open wounds or concomitant problems that would impede gait patterns, i.e. traumatic brain injury, spinal cord injury, neurological, vascular, pulmonary and psychological/mental disorders were excluded. All subjects were informed about the study procedure and they gave written consent to participate. The study protocol was approved by Gülhane Medical Academy Ethics Committee.
Quality of life and functional assessment
After noting the patients’ medical history, cause and level of amputations, we used the Turkish-validated version of the Short Form 36 (SF-36)-health survey version 25 for assessing quality of life (QoL), 6 Satisfaction with Prosthesis Questionnaire (SAT-PRO), a self-administrated questionnaire for evaluating the satisfaction of subjects towards their prosthesis, 7 and the Turkish-validated version of Amputee Body Image Scale (ABIS),8,9 a questionnaire for assessing an individual’s feelings and perceptions about their body experience.
The Houghton Scale (HS) was applied to all subjects for the evaluation of prosthetic use with respect to proportional duration, places (in-/outdoors), supportive device use (wheelchair, walker, crutches) and outdoor balance on various types of ground (plain, slope, broken).10,11
Functionality was assessed with the six-minute walk test (6MWT) and the 10-meter walk test (10MWT). The two tests were performed consecutively with a sufficient resting time interval. All subjects were asked to walk for six minutes in their regular walking rhythm (without any encouragement) in the corridor (50 m). At the end of the test, the total distance was recorded in meters. 12 During the 10MWT, subjects were asked to walk 10 m on a straight line at a speed similar to their daily activities. A chronometer was used and the average speed (m/s) was taken after two consecutive measurements. 13
The questionnaires were completed face to face at the clinic. All of the functional tests were performed by an experienced physiotherapist on the same day.
Statistical analysis
All data were analyzed by SPSS version 15.0 for Windows. Mann-Whitney U and Chi-square tests were used for group comparisons. Spearman rank test was used for correlation analyses. Statistical significance was set at p < 0.05.
Results
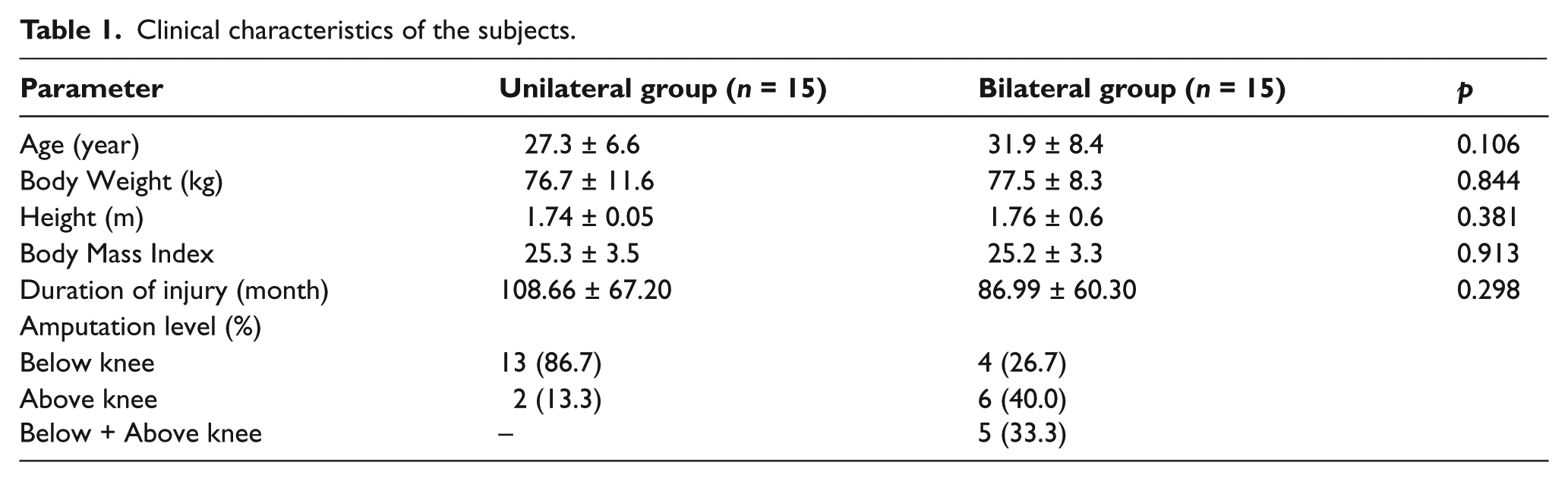
Clinical characteristics of the subjects are summarized in Table 1. The causes of amputations were as follows: high-energy land mine explosion (12), close gunshot injury (3) in the bilateral group, and high-energy land mine explosion (14) and close gun shot injury (1) in the unilateral group. The groups were similar in this regard (p > 0.05).
Clinical characteristics of the subjects.
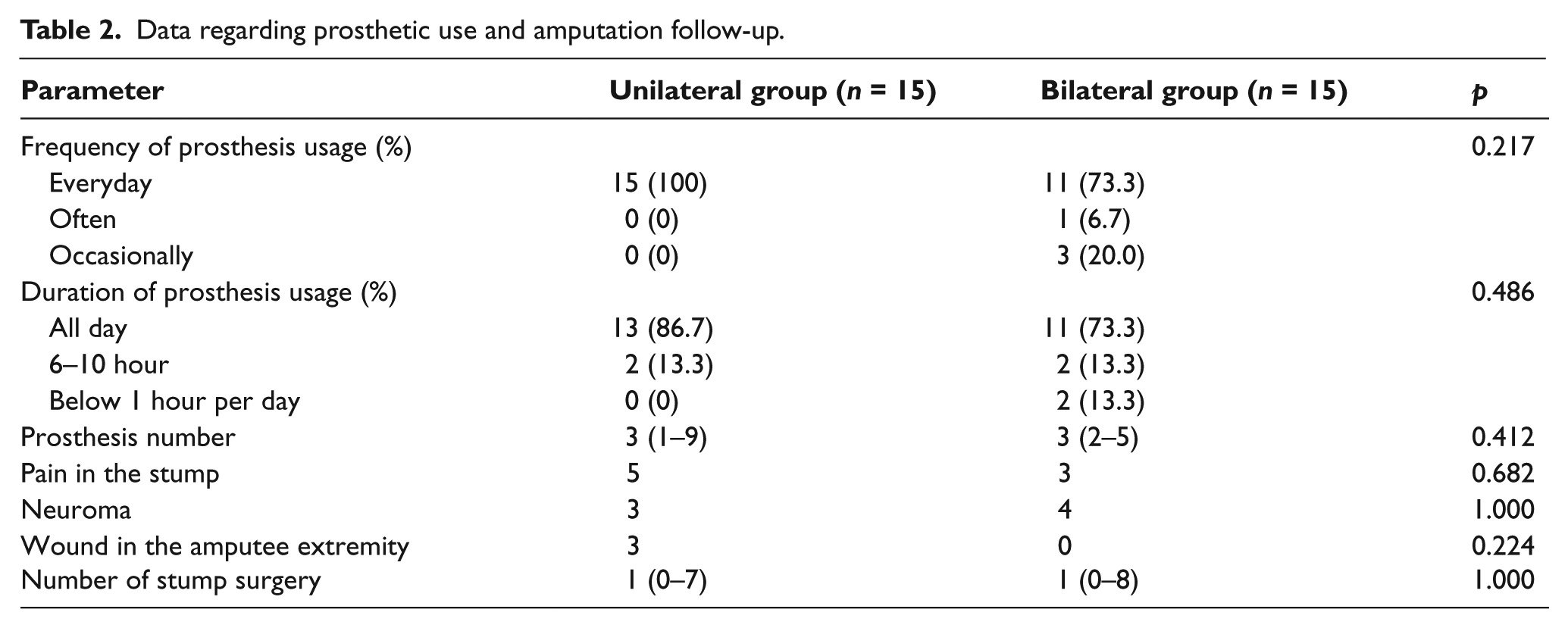
Concerning the prosthetic use (frequency, duration and the number of prosthesis) and relevant medical history (stump pain, presence of neuroma, wound or stump surgery), the groups were again similar (Table 2).
Data regarding prosthetic use and amputation follow-up.
QoL assessment scores are given in Table 3. Other than physical function, physical and emotional role scores being higher in the unilateral group (indicating better life quality), all parameters were similar between the two groups. Further, the frequency of prosthesis usage was found to be positively correlated with scores of SF-36 subgroups (except pain) (all p < 0.05), SAT-PRO (p < 0.05), but not of ABIS.
Quality of life assessment scores and functional ambulation measurement of the subjects.
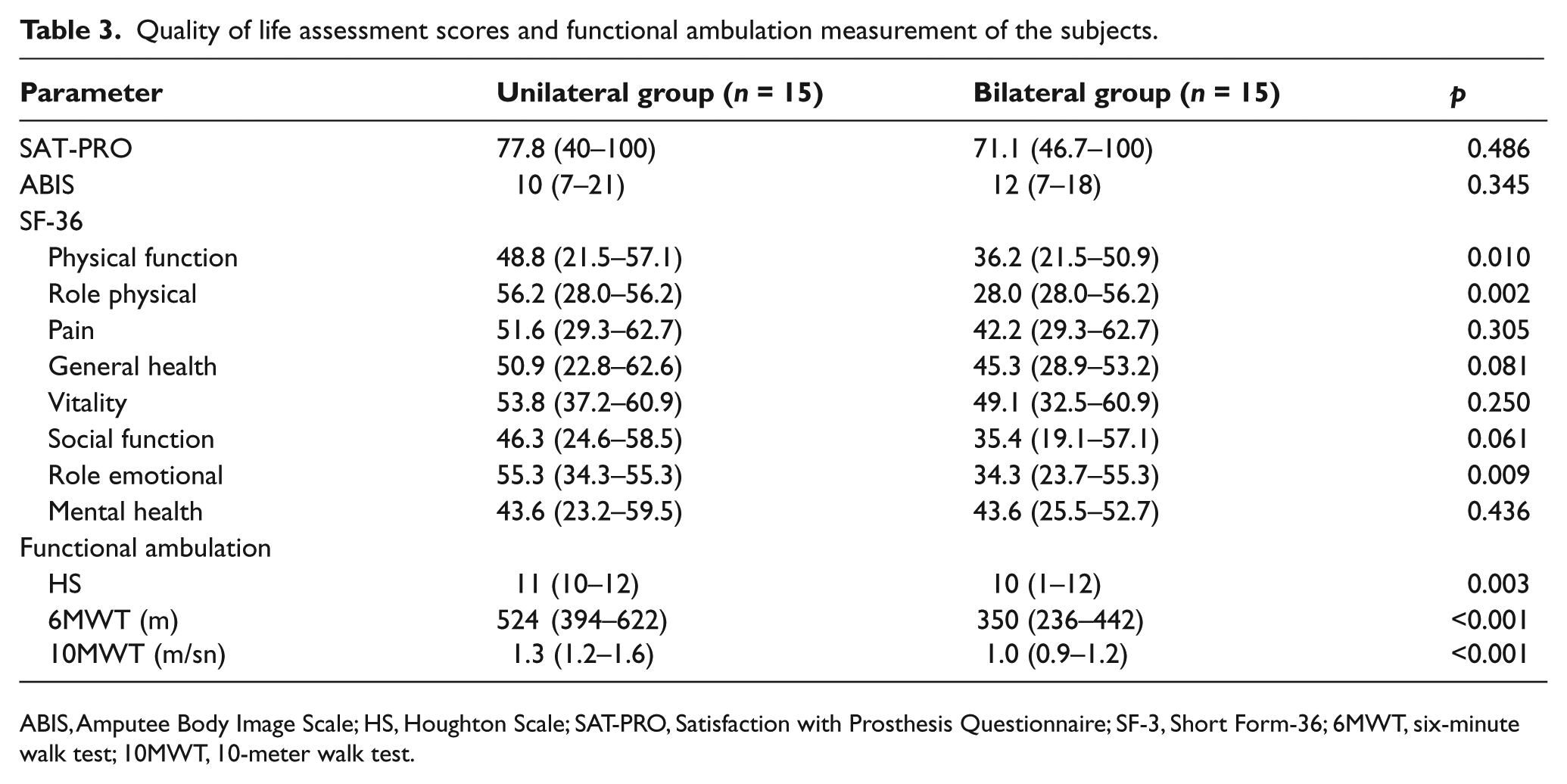
ABIS, Amputee Body Image Scale; HS, Houghton Scale; SAT-PRO, Satisfaction with Prosthesis Questionnaire; SF-3, Short Form-36; 6MWT, six-minute walk test; 10MWT, 10-meter walk test.
HS scores were higher in the unilateral group (Table 3). While none of the unilateral amputee patients needed additional supportive devices, two of the bilateral amputee subjects needed a wheelchair, five needed a single crutch and eight needed no additional supportive device for ambulation.
Although subjects in both groups had functional ambulation, 6MWT and 10MWT measurements were significantly higher in the unilateral group (Table 3).
Discussion
In this study, unilateral and bilateral amputee patients were compared with regard to their prosthesis usage, QoL, independent ambulation capacity and gait parameters to the best knowledge of the authors’ for the first time in the literature. Although prosthetic use was found to be similar between the groups, the rest of the assessment parameters were better in the unilateral amputee group.
Several factors like comfort, appearance, weight and usefulness are important regarding the use of prosthesis in an amputee patient.14,15 Prostheses also improve the QoL by providing normal body image and by increasing the physical abilities. 7 In our study, both groups obtained high scores according to SAT-PRO and ABIS. On the other hand, as the patient groups comprised only war veterans, our results may not be extrapolated to the other amputees for whom social security systems may assert financial limitations in some countries.
Subjects with lower limb amputations are exposed to several physical, psychological and social problems. Accordingly, we have used SF-36 to assess QoL in our patient groups. We found that the physical function, role physical and role emotional scores were significantly higher in the unilateral group. We believe that these differences stem from the fact that the majority of the subjects in the unilateral group are much more active and motivated in their lives when compared with the bilateral amputee subjects. Herewith, as previous reports mention only worse SF-36 scores of amputee (vs. normal) subjects in general 12,13,16; our results (being even worse in bilateral amputees) would be noteworthy as well. Further, as QoL scores positively correlated with prosthetic use of the subjects (being more frequent in the unilateral group), we believe that prosthetics may have also contributed to the difference between the QoL scores of the two groups (being higher in the unilateral group).
The basis of the rehabilitation program for lower extremity amputee patients comprises recovery of the best locomotor function and mobility possible. Therefore, evaluation of these functions (with self-rated scales or various performance tests) is necessary during the follow-up period. In our study, HS scores of bilateral amputee patients were found to be lower (worse) than those of unilateral amputees. According to the scale, while the subjects who had bilateral (above knee) amputation used wheelchair and crutches, those with bilateral (below knee) amputation did not need supportive devices for independent ambulation. Further, the additional supportive device use increased if subjects had bilateral and above-knee amputations.
The mean distance required for ‘functional ambulation’ and the mean walking speed have been reported (respectively) as 300 m and 1.33 m/sec (range 1.0–1.67 m/sec) by previous studies in the literature.17,18 According to our results, unilateral amputee patients had better walking distance and gait speed; but their mean values were within the aforementioned normal limits in both groups (Table 2). Therefore, these results may also imply that both groups of patients had undergone successful surgery and postoperative rehabilitation. Moreover, it is well known that a patient’s age has a significant effect on the prognosis of traumatic lower extremity injuries 4 and the majority of our patients were previously healthy young military personnel who had high physical functions. Accordingly, we believe that these premorbid features also had a favorable effect on the functional outcome of our patients in each group.
Conclusions
To conclude, in the light of our first and preliminary findings, we imply that physical abilities of bilateral amputee patients are lower than those of unilateral amputees. Further, prosthesis satisfaction and body image do not seem to change with the amputation level but the QoL and satisfaction with prostheses do increase in parallel with the use of prostheses. Lastly, we believe that future studies with a larger group of patients are needed to compare other parameters such as energy expenditure index or social statues of uni- vs. bilateral amputee patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.